
Enhancing Cross-Cultural Competence of Medical and Healthcare Students with the Use of Simulated Patients—A Systematic Review

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
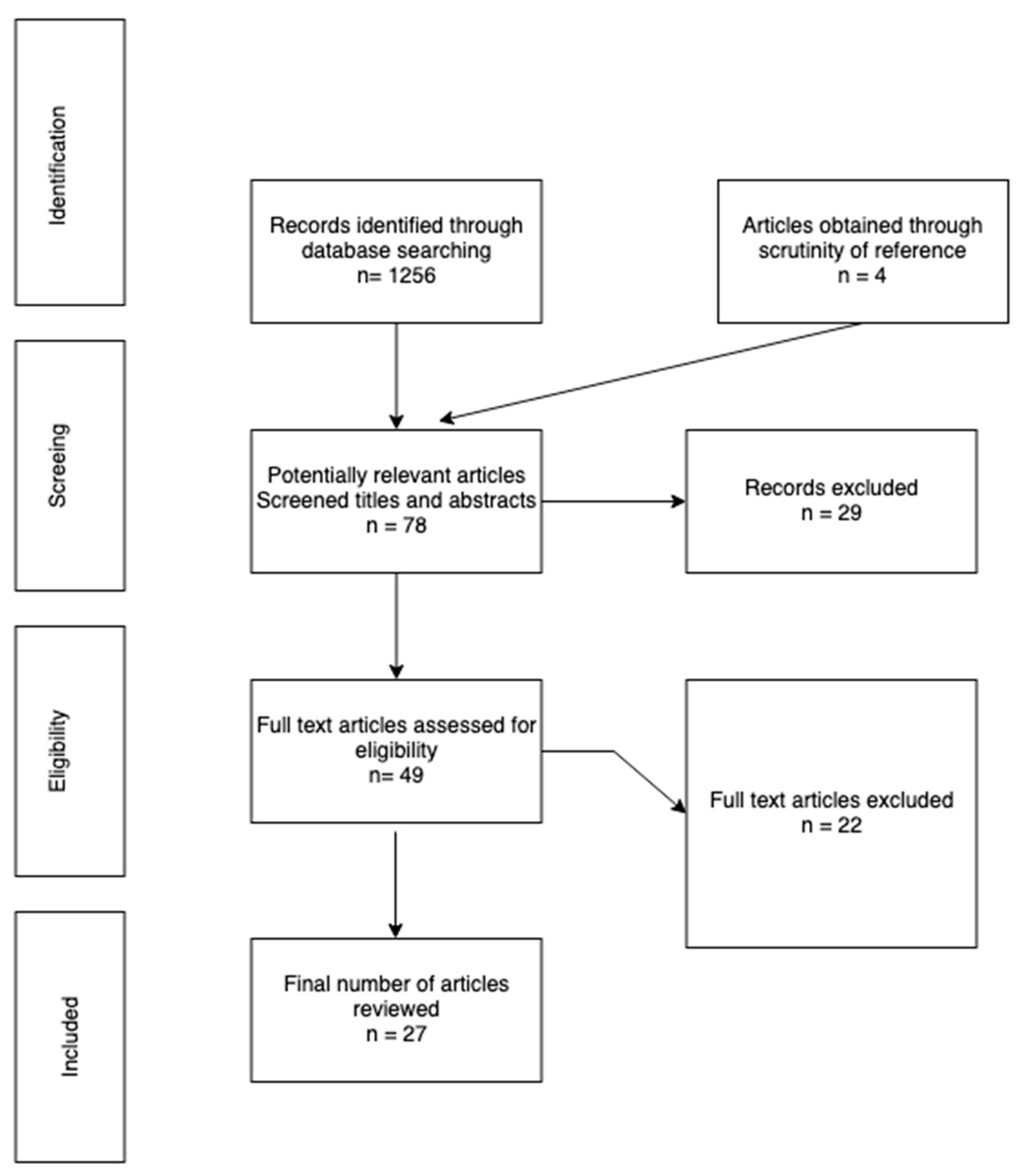
2.1. Study Selection and Inclusion Process
2.2. Inclusion/Exclusion Criteria
3. Results
3.1. Participants of Studies
3.2. Studies on Medical Students
3.3. Studies on Nursing Students
3.4. Studies on Students from Other Faculties
3.5. Studies Conducted on Interprofessional Groups of Students
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cai, D.Y. A Concept Analysis of Cultural Competence. Int. J. Nurs. Sci. 2016, 3, 268–273. [Google Scholar] [CrossRef] [Green Version]
- Musolino, G.M.; Babitz, M.; Burkhalter, S.T.; Thompson, C.; Harris, R.; Ward, R.S.; Chase-Cantarini, S. Mutual Respect in Healthcare: Assessing Cultural Competence for the University of Utah Interdisciplinary Health Sciences. J. Allied Health 2009, 38, 54E–62E. [Google Scholar]
- Panzarella, K.J. Beginning with the End in Mind: Evaluating Outcomes of Cultural Competence Instruction in a Doctor of Physical Therapy Programme. Disabil. Rehabil. 2009, 31, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Wagner, J.; Arteaga, S.; D’Ambrosio, J.; Hodge, C.E.; Ioannidou, E.; Pfeiffer, C.A.; Yong, L.; Reisine, S. A Patient-Instructor Program to Promote Dental Students’ Communication Skills with Diverse Patients. J. Dent. Educ. 2007, 71, 1554–1560. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.; Green, A.R. Student Reflections on Learning Cross-Cultural Skills through a “cultural Competence” OSCE. Med. Teach. 2007, 29, e76–e84. [Google Scholar] [CrossRef]
- Turkelson, C.; Cooper, D.; Creech, C.; Schellenberg, K.; Behnke, L. Using Simulation to Enhance Nurse Practitioner Students Cultural Sensitivity, Communication, and Empathy with Vulnerable Populations. Clin. Simul. Nurs. 2021, 56, 108–116. [Google Scholar] [CrossRef]
- Byrne, D. Evaluating Cultural Competence in Undergraduate Nursing Students Using Standardized Patients. Teach. Learn. Nurs. 2020, 15, 57–60. [Google Scholar] [CrossRef]
- Fitzgerald, S.N.; Leslie, K.F.; Simpson, R.; Jones, V.F.; Barnes, E.T. Culturally Effective Care for Refugee Populations: Interprofessional, Interactive Case Studies. MedEdPORTAL 2018, 14, 10668. [Google Scholar] [CrossRef]
- Min-Yu Lau, P.; Woodward-Kron, R.; Livesay, K.; Elliott, K.; Nicholson, P. Cultural Respect Encompassing Simulation Training: Being Heard about Health through Broadband. J. Public Health Res. 2016, 5, jphr.2016.657. [Google Scholar] [CrossRef] [Green Version]
- Claramita, M.; Tuah, R.; Riskione, P.; Prabandari, Y.S.; Effendy, C. Comparison of Communication Skills between Trained and Untrained Students Using a Culturally Sensitive Nurse-Client Communication Guideline in Indonesia. Nurse Educ. Today 2016, 36, 236–241. [Google Scholar] [CrossRef]
- Ndiwane, A.N.; Baker, N.C.; Makosky, A.; Reidy, P.; Guarino, A.J. Use of Simulation to Integrate Cultural Humility into Advanced Health Assessment for Nurse Practitioner Students. J. Nurs. Educ. 2017, 56, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Nimmo, C.; Behnke, L.; Creech, C.; Schellenberg, K.; Turkelson, C.; Cooper, D. Using Simulation to Educate Rural NP Students About Cultural Congruence. J. Nurse Pract. 2021, 17, 476–480. [Google Scholar] [CrossRef]
- Duke, P.S.; Brunger, F.; Ohle, E. Morning in Refugee Health: An Introduction for Medical Students. Int. J. Migr. Health Soc. Care 2015, 11, 86–94. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services, OPHS. National Standards for Culturally and Linguistically Appropriate Services in Health Care. Final Report. Available online: https://minorityhealth.hhs.gov/assets/pdf/checked/finalreport.pdf (accessed on 26 September 2022).
- International Council of Nurses Position Statement. Cultural and Linguistic Competence. Available online: www.icn.ch/sites/default/files/inline-files/B03_Cultural_Linguistic_Competence.pdf (accessed on 26 September 2022).
- Rozporządzenie Ministra Nauki i Szkolnictwa Wyższego z dnia 26 lipca 2019 r. w sprawie standardów kształcenia przygotowującego do wykonywania zawodu lekarza, lekarza dentysty, farmaceuty, pielęgniarki, położnej, diagnosty laboratoryjnego, fizjoterapeuty i ratownika medycznego. Available online: https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU20190001573/O/D20191573.pdf (accessed on 26 September 2022).
- Wehbe-Alamah, H.B. Leininger’s Culture Care Diversity and Universality Theory: Classic and New Contributions. Annu. Rev. Nurs. Res. Transcult. Soc. Res. 2018, 37, 1–23. [Google Scholar] [CrossRef]
- Shirazi, M.; Ponzer, S.; Zarghi, N.; Keshmiri, F.; Karbasi Motlagh, M.; Khorasani Zavareh, D.; Khankeh, H.R. Inter-Cultural and Cross-Cultural Communication through Physicians’ Lens: Perceptions and Experiences. Int. J. Med. Educ. 2020, 11, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, N.K.; Lam, P.; Castillo, E.G.; Weiss, M.G.; Diaz, E.; Alarcón, R.D.; van Dijk, R.; Rohlof, H.; Ndetei, D.M.; Scalco, M.; et al. How Do Clinicians Prefer Cultural Competence Training? Findings from the DSM-5 Cultural Formulation Interview Field Trial. Acad. Psychiatry 2016, 40, 584–591. [Google Scholar] [CrossRef]
- Tosun, B.; Yava, A.; Dirgar, E.; Şahin, E.B.; Yılmaz, E.B.; Papp, K.; Tóthova, V.; Hellerova, V.; Prosen, M.; Licen, S.; et al. Addressing the Effects of Transcultural Nursing Education on Nursing Students’ Cultural Competence: A Systematic Review. Nurse Educ. Pract. 2021, 55, 103171. [Google Scholar] [CrossRef]
- Ozkara San, E. Using Clinical Simulation to Enhance Culturally Competent Nursing Care: A Review of the Literature. Clin. Simul. Nurs. 2015, 11, 228–243. [Google Scholar] [CrossRef]
- Maran, N.J.; Glavin, R.J. Low- to High-Fidelity Simulation—A Continuum of Medical Education? Med. Educ. 2003, 37, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Jones, F.; Passos-Neto, C.; Melro Braghiroli, O. Simulation in Medical Education: Brief History and Methodology. Princ. Pract. Clin. Res. J. 2015, 1, 56–63. [Google Scholar] [CrossRef]
- Yudkowsky, R. Should We Use Standardized Patients Instead of Real Patients for High-Stakes Exams in Psychiatry? Acad. Psychiatry 2002, 26, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.J.; Tortorella, R.A.W. Hybrid Medical Simulation—A Systematic Literature Review. Smart Learn. Environ. 2020, 7, 16. [Google Scholar] [CrossRef]
- Churchouse, C.; McCafferty, C. Standardized Patients Versus Simulated Patients: Is There a Difference? Clin. Simul. Nurs. 2012, 8, e363–e365. [Google Scholar] [CrossRef]
- Cerbin-Koczorowska, M.; Przymuszała, P.; Waszyk- Nowaczyk, M.; Plewka, B.; Marciniak, R. The Need for Simulated Patient Method Implementation in Pharmaceutical Education in Poland. Indian J. Pharm. Educ. Res. 2020, 54, 875–880. [Google Scholar] [CrossRef]
- Beigzadeh, A.; Bahmanbijari, B.; Sharifpoor, E.; Rahimi, M. Standardized Patients versus Simulated Patients in Medical Education: Are They the Same or Different. J. Emerg. Pract. Trauma 2015, 2, 25–28. [Google Scholar] [CrossRef]
- Barrows, H.S. An Overview of the Uses of Standardized Patients for Teaching and Evaluating Clinical Skills. Acad. Med. 1993, 68, 443–451. [Google Scholar] [CrossRef]
- Collins, J.P.; Harden, R.M. AMEE Medical Education Guide No. 13: Real Patients, Simulated Patients and Simulators in Clinical Examinations. Med. Teach. 1998, 20, 508–521. [Google Scholar] [CrossRef]
- Przymuszała, P.; Marciniak-Stępak, P.; Cerbin-Koczorowska, M.; Borowczyk, M.; Cieślak, K.; Szlanga, L.; Zielińska-Tomczak, Ł.; Marciniak, R. ‘Difficult Conversations with Patients’—A Modified Group Objective Structured Clinical Experience for Medical Students. Int. J. Environ. Res. Public Health 2021, 18, 5772. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.G.; Warda, M.; Garbutt, S.; Curry, K. The Use of High-Fidelity Simulation to Teach Cultural Competence in the Nursing Curriculum. J. Prof. Nurs. 2014, 30, 259–265. [Google Scholar] [CrossRef]
- Grossman, S.; Mager, D.; Opheim, H.M.; Torbjornsen, A. A Bi-National Simulation Study to Improve Cultural Awareness in Nursing Students. Clin. Simul. Nurs. 2012, 8, e341–e346. [Google Scholar] [CrossRef]
- Ignacio, J.; Dolmans, D.; Scherpbier, A.; Rethans, J.J.; Chan, S.; Liaw, S.Y. Comparison of Standardized Patients with High-Fidelity Simulators for Managing Stress and Improving Performance in Clinical Deterioration: A Mixed Methods Study. Nurse Educ. Today 2015, 35, 1161–1168. [Google Scholar] [CrossRef] [PubMed]
- Wagner, J.; Arteaga, S.; D’Ambrosio, J.; Hodge, C.; Ioannidou, E.; Pfeiffer, C.A.; Reisine, S. Dental Students’ Attitudes toward Treating Diverse Patients: Effects of a Cross-Cultural Patient-Instructor Program. J. Dent. Educ. 2008, 72, 1128–1134. [Google Scholar] [CrossRef] [PubMed]
- Rutledge, C.M.; Garzon, L.; Scott, M.; Karlowicz, K. Using Standardized Patients to Teach and Evaluate Nurse Practitioner Students on Cultural Competency. Int. J. Nurs. Educ. Sch. 2004, 1, 17. [Google Scholar] [CrossRef] [Green Version]
- Dobbie, A.E.; Medrano, M.; Tysinger, J.; Olney, C. The BELIEF Instrument: A Preclinical Teaching Tool to Elicit Patients’ Health Beliefs. Fam. Med. 2003, 35, 316–319. [Google Scholar] [PubMed]
- Rosen, J.; Spatz, E.S.; Gaaserud, A.M.J.; Abramovitch, H.; Weinreb, B.; Wenger, N.S.; Margolis, C.Z. A New Approach to Developing Cross-Cultural Communication Skills. Med. Teach. 2004, 26, 126–132. [Google Scholar] [CrossRef]
- Green, A.R.; Miller, E.; Krupat, E.; White, A.; Taylor, W.C.; Hirsh, D.A.; Wilson, R.P.; Betancourt, J.R. Designing and Implementing a Cultural Competence OSCE: Lessons Learned from Interviews with Medical Students. Ethn. Dis. 2007, 17, 344–350. [Google Scholar]
- Bertelsen, N.S.; DallaPiazza, M.; Hopkins, M.A.; Ogedegbe, G. Teaching Global Health with Simulations and Case Discussions in a Medical Student Selective. Glob. Health 2015, 11, 28. [Google Scholar] [CrossRef] [Green Version]
- Ruth-Sahd, L.A.; Schneider, M.A.; Strouse, A. Fostering Cultural and Interdisciplinary Awareness with “Low-Tech” Simulation in a Fundamentals Nursing Course to Prepare Student Nurses for Critical Care Clinical Rotations. Dimens. Crit. Care Nurs. 2011, 30, 263–268. [Google Scholar] [CrossRef]
- Ndiwane, A.; Koul, O.; Theroux, R. Implementing Standardized Patients to Teach Cultural Competency to Graduate Nursing Students. Clin. Simul. Nurs. 2014, 10, e87–e94. [Google Scholar] [CrossRef]
- Plaza del Pino, F.J.; Arrogante, O.; Simonelli-Muñoz, A.J.; Gallego-Gómez, J.I.; Jiménez-Rodríguez, D. Use of High-Fidelity Clinical Simulation for the Development of Cultural Competence of Nursing Students. Nurse Educ. Today 2022, 116, 105465. [Google Scholar] [CrossRef] [PubMed]
- Quick, K.K.; Selameab, T.; Woll, A.; Mazzei, C.; Miller, J.L. Creating and Evaluating Skills-Based Training in Working with Spoken-Language Interpreters for Oral Health Professions Students. J. Dent. Educ. 2019, 83, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Woll, A.; Quick, K.K.; Mazzei, C.; Selameab, T.; Miller, J.L. Working With Interpreters as a Team in Health Care (WITH Care) Curriculum Tool Kit for Oral Health Professions. MedEdPORTAL 2020, 16, 10894. [Google Scholar] [CrossRef]
- Broder, H.L.; Janal, M. Promoting Interpersonal Skills and Cultural Sensitivity among Dental Students. J. Dent. Educ. 2006, 70, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Sales, I.; Jonkman, L.; Connor, S.; Hall, D. A Comparison of Educational Interventions to Enhance Cultural Competency in Pharmacy Students. Am. J. Pharm. Educ. 2013, 77, 76. [Google Scholar] [CrossRef] [Green Version]
- Paparella-Pitzel, S.; Eubanks, R.; Kaplan, S.L. Comparison of Teaching Strategies for Cultural Humility in Physical Therapy. J. Allied Health 2016, 45, 139–146. [Google Scholar] [PubMed]
- Chung, S.; Jarvill, M. Improving Nursing Student Cultural Competence: Comparing Simulation to Case-Based Learning. J. Nurs. Educ. Pract. 2019, 9, 128–132. [Google Scholar] [CrossRef]
- Ozkara San, E. Effect of the Diverse Standardized Patient Simulation (DSPS) Cultural Competence Education Strategy on Nursing Students’ Transcultural Self-Efficacy Perceptions. J. Transcult. Nurs. 2019, 30, 291–302. [Google Scholar] [CrossRef] [Green Version]
- Garvey, L.; Mackelprang, J.L.; Bhowmik, J.; Cassar, N.; Delbridge, R.; El-Ansary, D.; Willetts, G.; Williams, A. Enhancing Cultural Capabilities Amongst Health Professions Students: A Pilot Study of Interprofessional Tag Team Simulation. Clin. Simul. Nurs. 2022, 62, 83–91. [Google Scholar] [CrossRef]
- Guvenc, G.; Unver, V.; Basak, T.; Yuksel, C.; Ayhan, H.; Kok, G.; Konukbay, D.; Kose, G.; Aslan, O.; Tastan, S.; et al. Turkish Senior Nursing Students’ Communication Experience with English Speaking Patients. J. Nurs. Educ. 2016, 55, 73–81. [Google Scholar] [CrossRef]
- Unver, V.; Uslu, Y.; Kocatepe, V.; Kuguoglu, S. Evaluation of Cultural Sensitivity in Healthcare Service among Nursing Students. Eur. J. Educ. Res. 2019, 8, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Maar, M.; Bessette, N.; McGregor, L.; Lovelace, A.; Reade, M. Co-Creating Simulated Cultural Communication Scenarios with Indigenous Animators: An Evaluation of Innovative Clinical Cultural Safety Curriculum. J. Med. Educ. Curric. Dev. 2020, 7, 238212052098048. [Google Scholar] [CrossRef]
- Morell, V.W.; Sharp, P.C.; Crandall, S.J. Creating Student Awareness to Improve Cultural Competence: Creating the Critical Incident. Med. Teach. 2002, 24, 532–534. [Google Scholar] [CrossRef] [PubMed]
- Jeffreys, M.R. Teaching Cultural Competence in Nursing and Health Care; Springer Publishing Company: New York, NY, USA, 2016; ISBN 978-0-8261-1996-4. [Google Scholar]
- Welch, M. Teaching Diversity and Cross-Cultural Competence in Health Care: A Trainer’s Guide; Perspectives of Differences Diversity Training and Consultation Services for Health Professionals (PODSDT): San Francisco, CA, USA, 2003. [Google Scholar]
- Campinha-Bacote, J. The Process of Cultural Competence in the Delivery of Healthcare Services: A Model of Care. J. Transcult. Nurs. 2002, 13, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Tervalon, M.; Murray-García, J. Cultural Humility versus Cultural Competence: A Critical Distinction in Defining Physician Training Outcomes in Multicultural Education. J. Health Care Poor Underserved 1998, 9, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Zielińska-Tomczak, Ł.; Cerbin-Koczorowska, M.; Przymuszała, P.; Marciniak, R. How to Effectively Promote Interprofessional Collaboration?—A Qualitative Study on Physicians’ and Pharmacists’ Perspectives Driven by the Theory of Planned Behavior. BMC Health Serv. Res. 2021, 21, 903. [Google Scholar] [CrossRef]
- Cerbin-Koczorowska, M.; Przymuszała, P.; Michalak, M.; Piotrowska-Brudnicka, S.E.; Kant, P.; Skowron, A. Comparison of Medical and Pharmacy Students’ Readiness for Interprofessional Learning—A Cross-Sectional Study. Farmacia 2020, 68, 1166–1172. [Google Scholar] [CrossRef]


{kind=link}
| PICOS Terms | Applied Inclusion and Exclusion Criteria |
|---|---|
| Population | Inclusion: Undergraduate students of medical and healthcare faculties Exclusion: Other participant groups, including postgraduate students or residency programs |
| Intervention | Inclusion: Studies describing and evaluating educational interventions with the implementation of the simulated patient method Exclusion: Interventions using methods other than simulated patients (e.g., simulations with mannequins, student (peer) role-plays, pre-recorded videos, virtual reality, or simulation games), non-interventional studies (e.g., tool validation only), and studies where simulated patients were used only to assess students’ pre-existing skills and not as part of the evaluated intervention involving SPs |
| Comparison | Any comparator interventions |
| Outcomes | Inclusion: Participating students’ levels of cultural competencies, cultural sensitivity or cultural humility, confidence, empathy, interviewing skills, also during interpreter-supported interviews, overcoming language barriers, adapting care to cultural needs of patients, participants’ satisfaction Exclusion: Not relevant to cultural competence, cultural sensitivity, or cultural humility |
| Study type | Inclusion: Original articles published in English matching the above-mentioned inclusion criteria Exclusion: Articles published in languages other than English |
| Author, Year | Participants | Methods and Tools | Scenario Outline | Relevant Findings Related to Cultural Competences |
|---|---|---|---|---|
| Dobbie et al. 2003, [37] | 200 first-year medical students (197 students participated in the interview with SP). | A description of the BELIEF teaching tool and a study assessing the interviewing skills. Before the simulation, the students participated in a course on health beliefs and group discussions as well as sessions with standardized patients. | A Hispanic female with reflux and abdominal pain who believes the pain is the result of a curse and tried traditional healing remedies unsuccessfully. | The results following a series of interventions, including sessions with standardized patients, were as follows: Belief: 97% Explain: 95% Learn: 92% Impact: 97% Empathy: 90% (assessed by SP) Feelings: 94% |
| Rosen et al., 2004 [38] | 32 third-year medical students (24 completed the satisfaction survey). | A pre–post evaluation of a workshop, including a theoretical introduction and tOSCE sessions with SPs. Surveys assessing students’ attitudes and skills were filled out before and six weeks after the intervention. Students also filled out a self-evaluation survey immediately after the intervention. | 1. A Japanese patient with stomach cancer and his daughter demanding to speak with a doctor about her father’s diagnosis. 2. An Ethiopian immigrant to Israel diagnosed with HIV. 3. A Chinese woman who, after trying traditional Chinese healing methods without success, wants treatment from a Western doctor. 4. An Orthodox Jewish woman with symptoms possibly related to sexual abuse by a family member in the past. 5. A Bedouin man with asthma refusing to quit smoking. 6. An illegal Bulgarian laborer with asthma. | Significant improvement in regard to health-belief assessment, sexual history taking, biopsychosocial interviewing skills, breaking bad news, and approach to treatment. No significant changes were observed in communication with family members and working with an interpreter. Overall satisfaction with the course in the post-intervention survey: 96% considered the course effective, 96% noticed improvements in their ability to elicit treatment expectations, 92% understood patient’s perception of illness, 83% inquired about cultural issues, and 71% understood their cultural bias. |
| Green et al., 2007 [39] | 22 second-year medical students | Post-intervention semi-structured interviews with students on their perspectives on the SP encounter during a cultural competence OSCE station. | A Dominican woman with poorly controlled hypertension. | Identified themes covered learning goals, logistical issues, faculty feedback, and SPs. The overall students’ reception was positive. Some students pointed out that the separated format of the station posed a risk of promoting stereotypes and marginalizing the topic. SPs’ performance was mostly regarded as realistic and the feedback good, although sometimes too little specific. |
| Miller and Green, 2007 [5] | 22 second-year medical students | Post-intervention semi-structured interviews with students on their perspectives on the SP encounter during a cultural competence OSCE station. | A Dominican woman with poorly controlled hypertension. | 6 students (27%) were satisfied with their performance, 13 students (59%) realized gaps in knowledge and skills, 3 students (14%) were dissatisfied. Students’ reflections focused, among others, on inquiring about the reasons for non-adherence, patient’s perspective on the illness and social context, and exploring social and cultural factors associated with non-adherence. |
| Bertelsen et al., 2015 [40] | 33 medical students | Analysis and evaluation of a 4-week Global Health selective course. Assessment of students’ performance mostly using direct faculty observation and feedback. Evaluation of the curriculum using surveys with closed and open questions. | 1. A woman from rural Liberia in an obstetrical emergency. 2. A patient from Peru needing TB management. 3. A patient from Ghana and/or the Democratic Republic of Congo with hypertension. 4. A Chinese patient requiring counseling on smoking cessation. 5. An Ecuadorian diabetic patient. 6. A patient from the Democratic Republic of Congo with physical and psychological trauma. 7. A LEP patient needing the assistance of an interpreter. | Positive faculty and student feedback from the course, with 86% of students rating it as excellent. Highest ratings received by case discussion and experiential learning simulation. Increased students’ cross-cultural communication skills, ethical issues understanding in working with underserved populations, and appreciation of socio-cultural determinants of health-related needs and behavior, among others. |
| Maar et al., 2020 [54] | 39 first-year medical students | Pilot evaluation study of 9 Simulated Cultural Communication Scenarios using Likert scale questions and open-ended questions on faculty and students’ experiences and perceptions. | 1. A non-compliant female Indigenous diabetic patient uncomfortable with a male physician. 2. A male Indigenous patient with diabetes. 3. A male Indigenous patient with diabetes living under a lot of stress. 4. Tribal Indigenous police officer with frostbitten ears. 5. A male Indigenous patient who developed frostbite on his left hand, reluctant to receive help. 6. A male Indigenous patient with frostbitten fingers. 7. A male Indigenous patient recovering from addiction and living under a lot of stress needs a BP check-up. 8. A male Indigenous patient who is a single parent living with his sick mother and needs a BP check. 9. An Indigenous patient who travels a lot and needs a BP checked. | Improvements in students’ knowledge, skills, and understanding were believed to occur both by students and the faculty. Identified themes from qualitative data show the intervention’s potential to acquire culturally safe clinical skills due to the rich-in-context, authentic, safe dialogue with the patient. |
| Author, Year | Participants | Methods and Tools | Scenario Outline | Relevant Findings Related to Cultural Competences |
|---|---|---|---|---|
| Ruth-Sahd et al., 2011 [41] | 73 nursing students | Pre-simulation inquiry with open-ended questions on students’ feelings about it. Post-simulation Likert scale survey on students’ feelings about its value. | Two simulated patient scenarios: 1. A Hispanic woman after abdominal surgery. 2. A Haitian Jehovah’s Witness patient after limb surgery. | Improved cultural awareness and sensitivity according to 87% of students. |
| Grossman et al., 2012 [33] | 73 nursing students (48 Americans and 25 Norwegians) | Pre–post study using the Transcultural Self Efficacy Tool (TSET) measuring self-efficacy with subscales relating to cognitive, practical, and affective scores. | Two scenarios: 1. Somalian and Muslim patients for Norwegian students 2. Muslim and Italian Catholic patients for American students. | Increased self-efficacy in three TSET subscales and the total score (not significant only for the Practical subscale in the case of Norwegian students). |
| Ndiwane et al., 2014 [42] | 29 nursing students | Pre–post study in the OSCE context using the Cultural Assessment Survey with questions on students’ awareness and knowledge. Additionally, adapted Student Satisfaction Survey was used after the intervention to measure students’ satisfaction, self-confidence, and the intervention’s effect on critical thinking. Pre-OSCE didactic presentations were held for students on cultural assessment and practices of selected populations. Post-OSCE video recordings of their own and reference performances were provided to students for comparison. | Two scenarios for each student: 1. A pregnant Latina patient or a Latina patient with diabetes 2. An African-American patient with hypertension. | Significantly increased knowledge in 5 out of 7 variables of the Cultural Assessment Survey. No changes observed in regard to the opinion variables. No change in knowledge about the language. Mean scores of Student Satisfaction Survey (Likert scale 1–5): - Satisfaction—4.22 - Self-confidence—4.28 - Critical thinking—4.45 |
| Guvenc et al., 2016 [52] | 104 fourth-year nursing students | Mixed-methods study: - Qualitative data collected during semi-structured debriefing interviews - Quantitative data collected with authorial surveys administered after debriefing. | A non-Turkish-speaking pregnant woman with severe preeclampsia. | Raised awareness of the possibility of providing care to a patient who speaks English in 95.2% of students. Recognition of the need to improve their English by 98.1% and the need to learn about different cultures by 81.7% of students. Language use, cultural differences, and patient safety gains reported in the qualitative part. |
| Ndiwane et al., 2017 [11] | 63 nursing students (51 completed surveys) | Pre–post intervention using the Cultural Assessment Survey with pre-test used to assess cultural competency knowledge, followed by cultural sensitivity presentation and an OSCE module with an SP that was video recorded and then given to the student along with a reference video for comparison. After that, a debriefing session was held, and later, students completed the post-test and Student Satisfaction Survey. | A male African American patient with hypertension. | Statistically significant increase in knowledge. Generally good reception by students with highest satisfaction scores, followed by critical thinking and self-confidence. |
| Chung et al., 2019 [49] | 80 nursing students (38 simulation-based learning and 42 case-based learning) | Pre–post two-group study using the Cultural Competence Assessment Survey CCA, involving Cultural Awareness and Sensitivity scale CAS and Cultural Competence Behaviors CCB—(only pre-intervention). | A 60-year-old female Muslim needing a dressing change after hip surgery. | Improvement of CCA. Case-based learning group: 3.73 to 4.14; Simulation group: 3.98–4.02 Improvement of CAS. Case-based learning group: 5.94–6.09; Simulation group: 5.97–6.22 |
| Ozkara, 2019 [50] | 53 nursing students | Longitudinal pre–post intervention using the Transcultural Self-Efficacy Tool (TSET) and two other authorial tools: Simulation Survey and Simulation Participation Survey. | 1. A 65-year-old female Muslim patient from Turkey after surgery. 2. A 55-year-old American patient of Irish and Italian origin who is a Methodist and self- identifies with the LGBTQ population, suffering from diabetes. | Overall increase in transcultural self-efficacy (TSE) in all 3 learning domains. Significant changes in the cognitive learning subscale followed by the practical and affective ones. |
| Unver et al., 2019 [53] | 34 final-year nursing students | Pre–post model study with Intercultural Sensitivity Scale (ISS) and Intercultural Sensitivity Assessment Checklist aimed at evaluation of cultural sensitivity and communication barriers. | 1. A Muslim Arabic- Palestinian male with diabetes, an immigrant to Turkey, fleeing the civil war in Syria, strictly following Ramadan principles and refusing to eat and take medicines, requesting a male nurse, speaks little Turkish. 2. A catholic White-American female patient with asthma and migraine, holidaying in Turkey, presenting at the emergency unit, speaks only English. | No significant change on Intercultural Sensitivity Scale (ISS). Intercultural Sensitivity Assessment Checklist revealed: Less than 15% were fully happy with the experience, half never collected information about diverse cultures, 41.18 did not feel confident, and 52.94% respected patients’ opinions. All students respect cultural values, 88.2% considered themselves open-minded nearly all (97.05%) respect different cultural behaviors. |
| Byrne, 2020 [7] | 38 nursing students | Quasi-experimental mixed method study with the IAPCCSV© used for pre–post and an open-ended survey for qualitative part on students’ perception of the intervention’s effectiveness. Comparison of two educational strategies—lecture only and lecture plus simulation with SPs groups. | A patient from a culturally diverse background seeking nutritional assessment and advice (including the use of cultural terms related to diet unknown to the students). | No significant differences between the lecture group and the lecture plus simulation group were observed. However, the students describe the interaction with SP as valuable, helpful, and highly recommended. |
| Nimmo et al., 2021 [12] | 25 nursing students (results analyzed for 23 students) | Pre–post study using the Transcultural Self-Efficacy Tool (TSET). Qualitative data from student self-reflection assessments were also analyzed. Online learning modules with cultural content and basic Spanish lessons were offered before the simulation. | A Spanish-speaking patient from a rural Hispanic population. Focus of the simulation on the management of chronic disease, e.g., diabetes mellitus type 2 | Significantly higher post-test results on all 3 TSET subscales. Positive reception by students describing the simulation experience as ‘helpful’ and ‘enjoyable’ and acknowledging its role in identifying their knowledge weaknesses. |
| Turkelson et al., 2021 [6] | 26 nursing students (results analyzed for 23 students) | Quasi-experimental pre–post study using the Transcultural Self-Efficacy Tool (TSET), the Jefferson Scale of Empathy, and the Rural Characteristics Tool. Additionally, online modules dealing with culture, language, and communication strategies were introduced as pre-simulation education. | A Spanish-speaking Hispanic patient in a rural primary healthcare setting accompanied by a family member fluent in both Spanish and English. Three scenarios were developed, and they portrayed problems such as lack of insurance, lack of previous medical records, etc. | Significantly higher post-test results for all 3 TSET subscales. Substantially higher pre-test and post-test mean scores for the affective subscale in comparison with other scales. No significant pre–post changes were observed on the Jefferson Scale of Empathy. |
| Plaza del Pino et al., 2022 [43] | 63 fourth-year nursing students (56 completed the interviews) | A pre–post qualitative descriptive study aimed at the evaluation of cultural competences when caring for a migrant patient. Semi-structured interviews were conducted before and after simulations. Instructions about the scenario were given to the students. Following the simulations, the students engaged in discussions and feedback from the professors. | A Moroccan Muslim patient admitted with hyperglycemia understands Spanish. | Satisfaction with the ability to communicate in a language-discordant situation, satisfaction with the use of various communication strategies, e.g., drawings. Students felt new skills and knowledge about different cultures were gained. Students were able to show empathy to the patient. They had difficulties adapting their actions to different cultures and customs. Realization of the importance of cultural competence training. |
| Author, Year | Participants | Methods and Tools | Scenario Outline | Relevant Findings Related to Cultural Competences |
|---|---|---|---|---|
| Broder and Janal, 2006 [46] | 143 third and fourth-year dental students | Two-part clinical communication program—CC1 and CC2—with CC2 containing cultural and mental health sensitivity issues. Arizona Clinical Interviewing Rating Scale (ACIR) was used to rate students’ performance after each scenario. Additionally, a course evaluation survey was filled out by students. | Four scenario rounds were completed in each part. Exemplar CC2 scenario focused on cultural aspects: A 35-year-old Muslim female with osteogenic sarcoma. | Improvements in the ratings of students’ clinical communication were observed between training rounds. Positive ratings of the training sessions by students (mean item scores between 4.4 and 4.6 on a 1–5 scale). |
| Wagner et al., 2007 [4] | 118 dental students (79 completed a third rotation) | Three rotations extended over junior and senior years involving clinical interviews assessed with the use of standardized rating scales and content checklists. Before the rotations, a lecture and seminar were presented to students on cultural aspects, among others. | The second and third rotations contain cross-cultural aspects, which involve such issues as language and religious differences, immigration status, culture-based beliefs about oral health, culture-based trust in alternative treatment, etc. Examples include: 1. A non-compliant patient with a heart murmur. 2. A smoking cessation case. | The overall performance was good, with improvements between encounters on a given day. Most frequently passed cultural items involved: patient confusion on insurance coverage and related financial concerns. The most frequently missed cultural items involved: language barriers, alternative healing strategies, access to care, and support systems. |
| Wagner et al., 2008 [35] | 155 dental students | Retrospective pre–post evaluation study aiming at assessing students’ changes in attitudes and behaviors towards diversity was carried out during two cross-cultural rotations with SPs. A cross-cultural training evaluation measure developed by Welch was used to capture students’ diversity-related attitudes and behaviors. The students’ satisfaction was also assessed with a separate survey developed by one of the authors. | Patients from Central and South America, Eastern Europe, Africa, India, and Asia presenting challenging cultural contents such as belief in alternative healing methods, different worldviews and religious values, different attitudes towards health and healthcare, language barriers, issues related to insurance and immigration status, etc. | Retrospectively reported improvement in diversity-related behaviors and attitudes across the two rotations. Students’ high satisfaction with the course in terms of both usefulness and enjoyableness. |
| Sales et al., 2013 [47] | 84 second-year pharmacy students (26 lecture-based learning, 30 case-based learning, 28 simulation-based learning) | Pre–post comparison study using cultural assessment surveys before and after three separate interventions—a 50-min lecture, case-scenario with a brief 10-min lecture, and simulation with SP with a brief 10-min lecture. The cultural assessment tool was used, supplemented with questions developed by authors. | Two SP encounters (students assigned into groups of 6) 1. A 72-Indian patient discharged from the hospital where he received treatment for DVT. In a hospital pharmacy, he refuses to pick up some of the medicines prescribed by a physician and admits to not planning to go to a follow-up cardiology unit appointment. 2. An anxious Muslim patient at the hospital refill clinic refusing to speak to a pharmacist who is of the opposite gender. | No activity managed to raise survey scores in all domains. Significantly bigger improvement in the cultural skills involving modifying communication style, demeanor, and interviewing questions among students from simulation and lecture than in the case-scenario group. After the intervention, simulation group students were more likely to express the desire to learn about the health beliefs and practices of different cultures and ethnic groups. |
| Paparella-Pitzel et al., 2016 [48] | 37 second-year physical therapy students (25 standard lecture, 6 case-based enriched learning, 6 simulation-enriched learning) | Longitudinal, 2-year pre–post study comparing students’ levels of cultural competence at three time points in three different educational strategies—standard lecture, additional lecture along with a role-play session, or Teaching OSCE (TOSCE) with SP. The Inventory for Assessing the Process of Cultural Competence Among Health Care Professionals-Revised (IAPCC-R) scale was used. | Culturally diverse scenarios with SPs—no further information available. | No significant differences were observed between the educational interventions. In the total sample, significant score improvement was noticed between the pre-test and first post-test, and the pre-test to the second post-test, with a significant deterioration between the first post-test and the second post-test. |
| Author, Year | Participants | Methods and Tools | Scenario Outline | Relevant Findings Related to Cultural Competences |
|---|---|---|---|---|
| Min-Yu Lau et al., 2016 [9] | 45 nursing and medical students and junior practitioners | Mixed-methods evaluative study with cultural competency being measured before and after Cultural Respect Encompassing Simulation Training (CREST) videoconference sessions using a survey covering 5 domains of cultural competency and assessment of learning experience by the participants. | SPs from different ethnic groups, including Asia, Africa, the Middle East, Europe, and Aboriginal Australians. | Significant improvement was noticed in 4 out of 5 cultural competency domains—cultural skills, encounters, knowledge, and awareness. Increase in understanding of non-verbal behavior, respect for diverse cultures, and effectiveness of work with interpreters. Teaching quality and learning experience highly rated by students. |
| Quick et al., 2019 [44] | 89 dental, dental hygiene, and dental therapy students (49 completed the surveys) | Pre–post study on students’ confidence and familiarity with best practices and talking to a limited English proficient patient and a patient with an interpreter. Qualitative data were collected during focus groups with participants. Comparison group involved data from 245 dental, dental hygiene, and dental therapy students who did not participate in the intervention. | 41 translating and interpreting students served as SPs with scenarios focused on a limited English proficient patient and a patient with an interpreter. | Significant pre–post differences in participants’ self-ratings for all 7 survey items. Usefulness and relevance of the training concepts stated by students in focus groups. |
| Woll et al., 2020 [45] | 175 dental, dental hygiene, and dental therapy students | Pre–post study on students’ confidence and familiarity with best practices and talking to a limited English proficient patient and a patient with an interpreter. | 41 translating and interpreting students served as SPs with scenarios focused on a limited English proficient patient and a patient with an interpreter. | Significant pre–post improvements in all survey parameters, including respondents’ familiarity with provider and interpreter best practices, legal protections, safety issues, and health disparities experienced by LEP patients and their confidence with talking to a LEP patient and employing best practices. |
| Garvey et al., 2022 [51] | 72 nursing, occupational therapy, and dietetics students (55 completed qualitative survey) | Pre–post study using the Cultural Capability Measurement Tool (CCMT) and Interprofessional Attitude Scale (IPAS). Post-simulation students also were asked open-ended questions on the experience and its impact. | An Aboriginal woman after limb amputation accompanied by her daughter and an Aboriginal health worker during hospital discharge. | Significantly higher post-simulation of the overall CCMT score and the respect, communication, safety, and quality subscales. Changes for advocacy and reflection subscales were not significant. More than 50% of students described the simulation experience in relation to their cultural capability learning and interprofessional education as ‘extremely’ and ‘very useful’. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walkowska, A.; Przymuszała, P.; Marciniak-Stępak, P.; Nowosadko, M.; Baum, E. Enhancing Cross-Cultural Competence of Medical and Healthcare Students with the Use of Simulated Patients—A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 2505. https://doi.org/10.3390/ijerph20032505
Walkowska A, Przymuszała P, Marciniak-Stępak P, Nowosadko M, Baum E. Enhancing Cross-Cultural Competence of Medical and Healthcare Students with the Use of Simulated Patients—A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(3):2505. https://doi.org/10.3390/ijerph20032505
Chicago/Turabian StyleWalkowska, Aleksandra, Piotr Przymuszała, Patrycja Marciniak-Stępak, Maria Nowosadko, and Ewa Baum. 2023. "Enhancing Cross-Cultural Competence of Medical and Healthcare Students with the Use of Simulated Patients—A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 3: 2505. https://doi.org/10.3390/ijerph20032505
APA StyleWalkowska, A., Przymuszała, P., Marciniak-Stępak, P., Nowosadko, M., & Baum, E. (2023). Enhancing Cross-Cultural Competence of Medical and Healthcare Students with the Use of Simulated Patients—A Systematic Review. International Journal of Environmental Research and Public Health, 20(3), 2505. https://doi.org/10.3390/ijerph20032505