
Evaluation of a Group Therapy for Work-Related Mental Disorders

Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Data Collection
2.3. Intervention
2.4. Measures
2.4.1. Diagnosis
2.4.2. Sociodemographic and Occupational Variables
2.4.3. Depression, Anxiety and Somatization
2.4.4. Burnout Dimensions
2.5. Statistical Analysis
3. Results
3.1. Response Rate
3.2. Sociodemographic and Occupational Variables
3.3. Diagnoses
3.4. Mental and Work-Related Distress at T1
3.5. Mental and Occupational Distress at T2
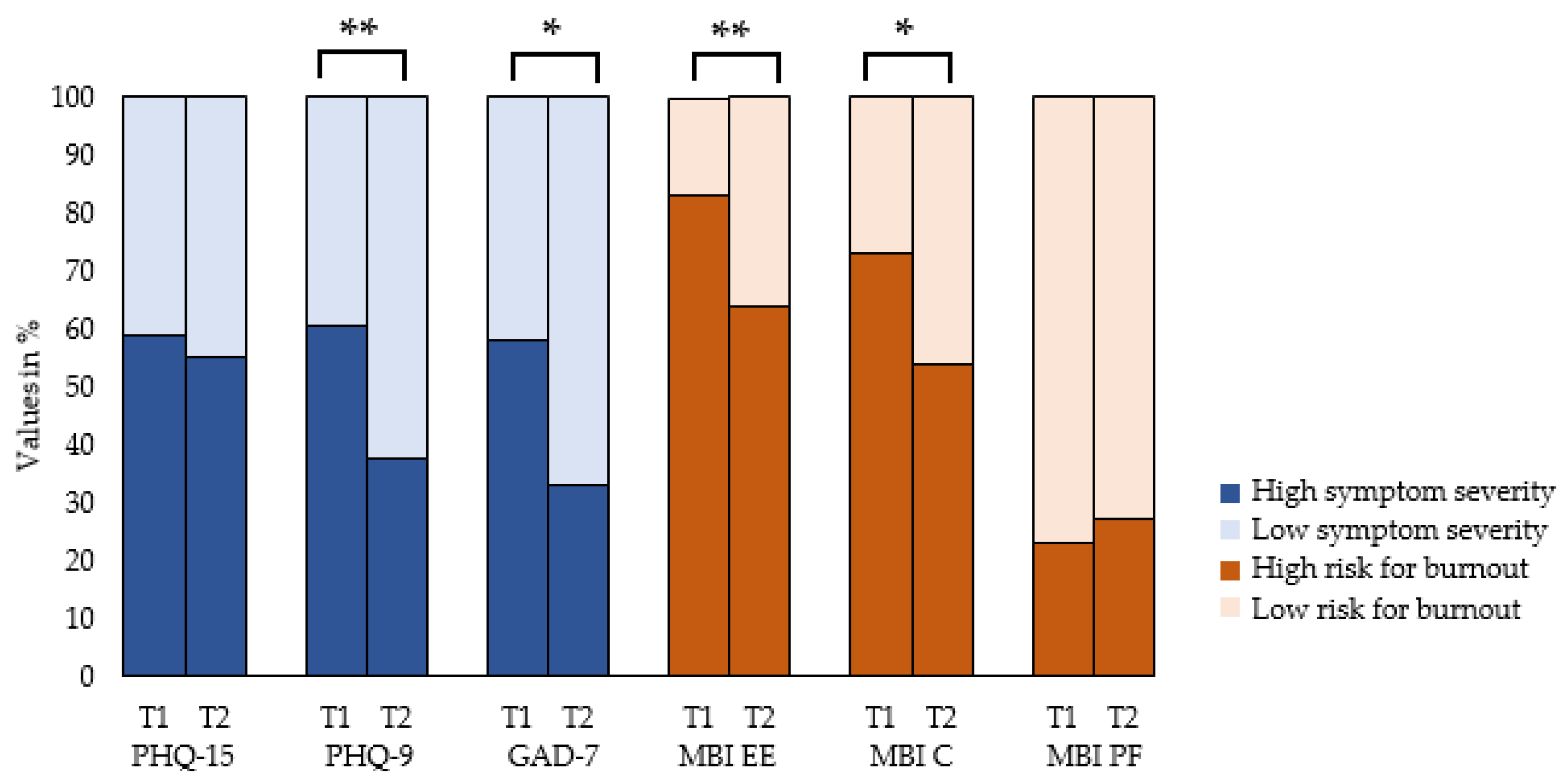
3.6. Changes of Mental Distress Measured in Prevalence
3.7. Changes of Mental Distress Measured in Symptom Manifestation
3.8. Gender Differences
4. Discussion
4.1. Reduction in Symptoms of Work-Related Mental Disorders and Burnout Dimensions
4.2. Gender Differences
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Braun, S.; Kessemeier, F.; Balint, E.; Schwarz, E.; Hölzer, M.; Gündel, H.; Rothermund, E. Psychische Erkrankungen im Arbeitskontext–eine Verortung im Versorgungssystem. PPmP 2019, 69, 505–516. [Google Scholar]
- OECD; European Union. Health at a Glance: Europe 2018: State of Health in the EU Cycle; OECD Publishing: Paris, France; European Union: Brussels, Belgium, 2018. [Google Scholar] [CrossRef]
- Harvey, S.B.; Modini, M.; Joyce, S.; Milligan-Saville, J.S.; Tan, L.; Mykletun, A.; Bryant, R.A.; Christensen, H.; Mitchell, P.B. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occup. Environ. Med. 2017, 74, 301–310. [Google Scholar] [CrossRef]
- Dewa, C.S. Les coûts des troubles mentaux en milieu de travail peuvent-ils être réduits ? [The Costs of Mental Disorders in the Workplace: Can They Be Decreased?]. Sante Ment. Que. 2017, 42, 31–38. [Google Scholar] [CrossRef]
- Aronsson, G.; Theorell, T.; Grape, T.; Hammarström, A.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Träskman-Bendz, L.; Hall, C. A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health 2017, 17, 264. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C. Burnout and engagement in the workplace: New perspectives. Eur. Health Psychol. 2011, 13, 44–47. [Google Scholar]
- WHO. ICD-11: International Classification of Diseases, 11th ed.; WHO: Geneva, Switzerland, 2019. Available online: https://icd.who.int (accessed on 31 January 2023).
- Guillaumie, L.; Boiral, O.; Champagne, J. A mixed-methods systematic review of the effects of mindfulness on nurses. J. Adv. Nurs. 2017, 73, 1017–1034. [Google Scholar] [CrossRef]
- Lomas, T.; Medina, J.C.; Ivtzan, I.; Rupprecht, S.; Eiroa-Orosa, F.J. A systematic review of the impact of mindfulness on the well-being of healthcare professionals. J. Clin. Psychol. 2018, 74, 319–355. [Google Scholar] [CrossRef]
- Stanulewicz, N.; Knox, E.; Narayanasamy, M.; Shivji, N.; Khunti, K.; Blake, H. Effectiveness of Lifestyle Health Promotion Interventions for Nurses: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 17, 17. [Google Scholar] [CrossRef] [PubMed]
- Niedermoser, D.W.; Kalak, N.; Kiyhankhadiv, A.; Brand, S.; Walter, C.; Schweinfurth, N.; Lang, U.E. Workplace-Related Interpersonal Group Psychotherapy to Improve Life at Work in Individuals With Major Depressive Disorders: A Randomized Interventional Pilot Study. Front. Psychiatry 2020, 11, 168. [Google Scholar] [CrossRef]
- Schramm, E.; Mack, S.; Thiel, N.; Jenkner, C.; Elsaesser, M.; Fangmeier, T. Interpersonal Psychotherapy vs. Treatment as Usual for Major Depression Related to Work Stress: A Pilot Randomized Controlled Study. Front. Psychiatry 2020, 11, 193. [Google Scholar] [CrossRef]
- Muschalla, B.; Linden, M.; Jobges, M. Work-Anxiety and Sickness Absence After a Short Inpatient Cognitive Behavioral Group Intervention in Comparison to a Recreational Group Meeting. J. Occup. Environ. Med. 2016, 58, 398–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, J.; Angerer, P.; Brenner, L.; Brezinski, J.; Chrysanthou, S.; Erim, Y.; Feißt, M.; Hansmann, M.; Hondong, S.; Kessemeier, F.M. Early intervention, treatment and rehabilitation of employees with common mental disorders by using psychotherapeutic consultation at work: Study protocol of a randomised controlled multicentre trial (friaa project). BMC Public Health 2021, 21, 1187. [Google Scholar] [CrossRef] [PubMed]
- Steinert, C.; Heim, N.; Leichsenring, F. Procrastination, Perfectionism, and Other Work-Related Mental Problems: Prevalence, Types, Assessment, and Treatment-A Scoping Review. Front. Psychiatry 2021, 12, 736776. [Google Scholar] [CrossRef] [PubMed]
- Schuster, N.; Haun, S.; Hiller, W. Psychische Belastungen im Arbeitsalltag: Trainingsmanual zur Stärkung persönlicher Ressourcen. Mit Online-Materialien; Beltz: Weinheim, Germany, 2011. [Google Scholar]
- Padkapayeva, K.; Gilbert-Ouimet, M.; Bielecky, A.; Ibrahim, S.; Mustard, C.; Brisson, C.; Smith, P. Gender/Sex Differences in the Relationship between Psychosocial Work Exposures and Work and Life Stress. Ann. Work Expo. Health 2018, 62, 416–425. [Google Scholar] [CrossRef]
- Vermeulen, M.; Mustard, C. Gender differences in job strain, social support at work, and psychological distress. J. Occup. Health Psychol. 2000, 5, 428–440. [Google Scholar] [CrossRef]
- Viertio, S.; Kiviruusu, O.; Piirtola, M.; Kaprio, J.; Korhonen, T.; Marttunen, M.; Suvisaari, J. Factors contributing to psychological distress in the working population, with a special reference to gender difference. BMC Public Health 2021, 21, 611. [Google Scholar] [CrossRef]
- Federal Statistical Office [Statistisches Bundesamt]. Population with a migration background. Results of the Microcensus 2014; Federal Statistical Office: Wiesbaden, Germany, 2015. Available online: https://www.destatis.de/DE/Publikationen/Thematisch/Bevoelkerung/MigrationIntegration/Migrationshintergrund2010220147004.pdf?__blob=publicationFile (accessed on 6 May 2022).
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-15: Validity of a new measure for evaluating the severity of somatic symptoms. Psychosom. Med. 2002, 64, 258–266. [Google Scholar] [CrossRef]
- Williams, N. The GAD-7 questionnaire. Occup. Med. 2014, 64, 224. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory Manual, 3rd ed.; Consulting Psychologists Press: Palo Alto, CA, USA, 1996. [Google Scholar]
- Büssing, A.; Glaser, J. Managerial Stress und Burnout. A Collaborative International Study (CISMS). The German Study; Technical University: Munich, Germany, 1998. [Google Scholar]
- Arnold, S. Kohärenzgefühl und Burnout bei Hochbegabten-Eine Querschnittstudie; Interuniversitären Kolleg für Gesundheit und Entwicklung Graz/Schloss Seggau: Seggauberg, Austria, 2011. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: Abingdon-on-Thames, UK, 1988. [Google Scholar] [CrossRef]
- Brenninkmeijer, V.; Lagerveld, S.E.; Blonk RW, B.; Schaufeli, W.B.; Wijngaards-de Meij, L. Predicting the Effectiveness of Work-Focused CBT for Common Mental Disorders: The Influence of Baseline Self-Efficacy, Depression and Anxiety. J. Occup. Rehabil. 2019, 29, 31–41. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, J.K.; Andrews, L.A.; Witcraft, S.M.; Powers, M.B.; Smits JA, J.; Hofmann, S.G. Cognitive behavioral therapy for anxiety and related disorders: A meta-analysis of randomized placebo-controlled trials. Depress. Anxiety 2018, 35, 502–514. [Google Scholar] [CrossRef]
- Leaviss, J.; Davis, S.; Ren, S.; Hamilton, J.; Scope, A.; Booth, A.; Sutton, A.; Parry, G.; Buszewicz, M.; Moss-Morris, R.; et al. Behavioural modification interventions for medically unexplained symptoms in primary care: Systematic reviews and economic evaluation. Health Technol. Assess. 2020, 24, 1–490. [Google Scholar] [CrossRef] [PubMed]
- Bakker, A.B.; Demerouti, E.; Verbeke, W. Using the Job Demands-Resources Model to Predict Burnout and Performance. In Human Resource Management: Published in Cooperation with the School of Business Administration, The University of Michigan and in Alliance with the Society of Human Resources Management; Wiley Online Library: Hoboken, NJ, USA, 2004; Volume 43, pp. 83–104. [Google Scholar]
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. The job demands-resources model of burnout. J. Appl. Psychol. 2001, 86, 499. [Google Scholar] [CrossRef] [PubMed]
- Leiter, M.P.; Maslach, C. Nurse turnover: The mediating role of burnout. J. Nurs. Manag. 2009, 17, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Employment Agency Germany. Payment Atlas; Employment Agency Germany: Nuremberg, Germany, 2020. Available online: https://web.arbeitsagentur.de/entgeldatlas/ (accessed on 31 January 2023).
- Weissman, M.M.; Bland, R.; Joyce, P.R.; Newman, S.; Wells, J.E.; Wittchen, H.-U. Sex differences in rates of depression: Cross-national perspectives. J. Affect. Disord. 1993, 29, 77–84. [Google Scholar] [CrossRef]
- Riffer, F.; Knopp, M.; Burghardt, J.; Sprung, M. Geschlechtsspezifische Unterschiede in der psychotherapeutischen Versorgung. Psychotherapeut 2021, 66, 511–517. [Google Scholar] [CrossRef]


{kind=link}
| Total Sample N = 48 | |
|---|---|
| Gender, n (%) | |
| Women | 23 (47.9) |
| Men | 25 (52.1) |
| Age, years, n (%) | |
| 26–40 | 8 (16.7) |
| 41–50 | 16 (33.3) |
| 51–60 | 24 (50.0) |
| Marital status, n (%) | |
| Single | 11 (22.9) |
| Married | 23 (47.9) |
| Divorced | 11 (22.9) |
| Separated | 2 (4.2) |
| Missing | 1 (2.1) |
| Children, n (%) | |
| Yes | 30 (62.5) |
| No | 18 (37.5) |
| Migration background, n (%) | |
| Yes | 5 (10.4) |
| No | 43 (89.6) |
| Education | |
| Primary School | 3 (6.3) |
| Middle School | 19 (39.6) |
| Secondary school | 26 (54.2) |
| Professional qualification | |
| Apprenticeship | 18 (37.5) |
| Master (craftsmen) | 7 (14.6) |
| University | 19 (39.6) |
| None | 1 (2.1) |
| Other | 3 (6.3) |
| Professional group | |
| Skilled worker | 2 (4.2) |
| Employee with basic tasks | 2 (4.2) |
| Employee with qualified tasks | 24 (50.0) |
| Employee with high qualified tasks/ leadership | 14 (29.2) |
| Employee with extensive management and decision-making authority | 5 (10.4) |
| Other | 1 (2.1) |
| Employment status | |
| Full-time | 36 (75.0) |
| Part-time | 12 (25.0) |
| Total Sample N = 48 | |
|---|---|
| Number of mental and behavioral disorders, n (%) | |
| One | 32 (66.7) |
| Two | 12 (25.0) |
| Three | 4 (8.3) |
| Main ICD-10 diagnoses, n (%) | |
| Mood (affective) disorders (F3) | 30 (62.5) |
| Mild depressive episode (F32.0) | 5 (10.4) |
| Moderate depressive episode (F32.1) | 10 (20.8) |
| Recurrent depressive disorder, current episode mild (F33.0) | 4 (8.3) |
| Recurrent depressive disorder, current episode moderate (F33.1) | 10 (20.8) |
| Recurrent depressive disorder, current episode severe without psychotic symptoms (F33.2) | 1 (2.1) |
| Neurotic, stress-related and somatoform disorders (F4) | 13 (56.3) |
| Panic disorder (F41.0) | 1 (2.1) |
| Generalized anxiety disorder (F41.1) | 1 (2.1) |
| Mixed anxiety and depressive disorder (F41.2) | 1 (2.1) |
| Adjustment disorders (F43.2) | 5 (10.4) |
| Other reactions to severe stress (F43.8) | 2 (4.2) |
| Undifferentiated somatoform disorder (F45.1) | 2 (4.2) |
| Somatoform autonomic dysfunction (F45.3) | 1 (2.1) |
| Behavioral syndromes associated with physiological disturbances and physical factors (F5) | 3 (6.3) |
| Eating disorder, unspecified (F50.9) | 1 (2.1) |
| Psychological and behavioral factors associated with disorders or diseases classified elsewhere (F54) | 2 (4.2) |
| Disorders of adult personality and behavior (F6) | 2 (4.2) |
| Other specified disorders of adult personality and behavior (F68.8) | 2 (4.2) |
| Total number of ICD-10 diagnoses, n (%) | |
| Mood (affective) disorders (F3) | 39 (60.9) |
| Neurotic, stress-related and somatoform disorders (F4) | 17 (26.5) |
| Behavioral syndromes associated with physiological disturbances and physical factors (F5) | 4 (6.3) |
| Disorders of adult personality and behavior (F6) | 4 (6.3) |
| T1 ** | T2 ** | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Sample (n = 48) M (SD) | Women (n = 23) M (SD) | Men (n = 25) M (SD) | Comparison between Men and Women at T1 | Total Sample (n = 48) M (SD) | Women (n = 23) M (SD) | Men (n = 25) M (SD | Comparison between Men and Women at T2 | |||||
| t | p | d | t | p | d | |||||||
| PHQ-15 | 10.81 (5.61) | 12.74 (5.43) | 9.04 (5.27) | −3.99 | <0.001 | −0.95 | 9.85 (6.19) | 10.30 (5.80) | 9.44 (6.62) | −2.00 | <0.05 | −0.48 |
| PHQ-15 * | 10.73 (5.56) | 12.57 (5.38) | 9.04 (5.27) | −3.68 | <0.001 | −0.88 | 9.73 (6.12) | 10.04 (5.67) | 9.44 (6.62) | −1.7 | 0.09 | −0.41 |
| PHQ-9 | 11.06 (6.19) | 12.25 (5.97) | 9.96 (5.50) | −1.20 | 0.23 | −0.29 | 8.29 (6.27) | 8.17 (5.75) | 8.40 (6.83) | 0.28 | 0.78 | 0.07 |
| GAD-7 | 9.94 (5.18) | 10.74 (4.85) | 9.20 (5.45) | −1.65 | 0.10 | −0.39 | 7.13 (5.69) | 6.17 (4.50) | 8.00 (6.57) | 0.33 | 0.74 | 0.08 |
| MBI EE | 4.63 (0.95) | 4.87 (0.77) | 4.42 (1.07) | −2.31 | <0.05 | −0.55 | 4.05 (1.35) | 4.14 (1.16) | 3.97 (1.52) | −0.89 | 0.38 | −0.21 |
| MBI Z | 3.93 (0.99) | 4.00 (0.86) | 3.86 (1.11) | −0.17 | 0.87 | −0.04 | 3.70 (1.32) | 3.70 (1.19) | 3.72 (1.44) | 1.11 | 0.28 | 0.27 |
| MBI PF | 4.30 (0.83) | 4.31 (0.74) | 4.27 (0.93) | 0.69 | 0.49 | 0.16 | 4.41 (0.94) | 4.62 (0.71) | 4.23 (1.09) | −0.66 | 0.51 | −0.16 |
| Total Sample T1–T2 | Women T1–T2 | Men T1–T2 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| t | p | d | t | p | d | t | p | d | |
| PHQ-15 | 1.57 | 0.12 | 0.23 | 3.65 | <0.001 | 0.76 | −0.43 | 0.67 | −0.09 |
| PHQ-15 * | 1.61 | 0.11 | 0.23 | 3.59 | <0.05 | 0.75 | −0.43 | 0.67 | −0.09 |
| PHQ-9 | 3.6 | <0.001 | 0.53 | 4.62 | <0.001 | 0.96 | 1.32 | 0.20 | 0.26 |
| GAD-7 | 3.4 | 0.001 | 0.49 | 4.36 | <0.001 | 0.91 | 1.02 | 0.32 | 0.20 |
| MBI EE | 3.8 | <0.001 | 0.55 | 3.26 | <0.05 | 0.68 | 2.13 | <0.05 | 0.43 |
| MBI C | 1.50 | 0.14 | 0.22 | 1.51 | 0.15 | 0.32 | 0.65 | 0.52 | 0.13 |
| MBI PF | −1.20 | 0.24 | −0.17 | −2.70 | <0.05 | −0.56 | 0.41 | 0.68 | 0.08 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hondong, S.; Morawa, E.; Kastel-Hoffmann, S.; Kandler, A.; Erim, Y. Evaluation of a Group Therapy for Work-Related Mental Disorders. Int. J. Environ. Res. Public Health 2023, 20, 2673. https://doi.org/10.3390/ijerph20032673
Hondong S, Morawa E, Kastel-Hoffmann S, Kandler A, Erim Y. Evaluation of a Group Therapy for Work-Related Mental Disorders. International Journal of Environmental Research and Public Health. 2023; 20(3):2673. https://doi.org/10.3390/ijerph20032673
Chicago/Turabian StyleHondong, Sinja, Eva Morawa, Silke Kastel-Hoffmann, Anja Kandler, and Yesim Erim. 2023. "Evaluation of a Group Therapy for Work-Related Mental Disorders" International Journal of Environmental Research and Public Health 20, no. 3: 2673. https://doi.org/10.3390/ijerph20032673
APA StyleHondong, S., Morawa, E., Kastel-Hoffmann, S., Kandler, A., & Erim, Y. (2023). Evaluation of a Group Therapy for Work-Related Mental Disorders. International Journal of Environmental Research and Public Health, 20(3), 2673. https://doi.org/10.3390/ijerph20032673