
Prehabilitation in Cardiovascular Surgery: The Effect of Neuromuscular Electrical Stimulation (Randomized Clinical Trial)

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Methodology
2.3. Intervention
2.4. Statistical Analysis
3. Results
CONSORT 2010 Flow Diagram
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HS | handgrip strength |
| NMES | neuro-muscle electrical stimulation |
| ICU | intensive care unit |
| KES | knee extensor strength |
| KFS | knee flexor strength |
| 6MWT | six-minute walk test |
| FC | functional class |
| GFR | glomerular filtration rate |
| PCI | percutaneous coronary intervention |
| COPD | chronic obstructive pulmonary disease |
References
- Furukawa, H.; Tanemoto, K. Frailty in cardiothoracic surgery: Systematic review of the literature. Gen. Thorac. Cardiovasc. Surg. 2015, 63, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Afilalo, J.; Lauck, S.; Kim, D.H.; Lefèvre, T.; Piazza, N.; Lachapelle, K.; Martucci, G.; Lamy, A.; Labinaz, M.; Peterson, M.D.; et al. Frailty in Older Adults Undergoing Aortic Valve Replacement: The FRAILTY-AVR Study. J. Am. Coll. Cardiol. 2017, 70, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Graham, A.; Brown, C.H., IV. Frailty, Aging, and Cardiovascular Surgery. Anesth. Analg. 2017, 124, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.K.; Marques, A.; Lobo, D.M.L.; Umeda, I.I.K.; Oliveira, M.F. Pre-Frailty Increases the Risk of Adverse Events in Older Patients Undergoing Cardiovascular Surgery. Arq. Bras. Cardiol. 2017, 109, 299–306. [Google Scholar] [CrossRef]
- Sepehri, A.; Beggs, T.; Hassan, A.; Rigatto, C.; Shaw-Daigle, C.; Tangri, N.; Arora, R.C. The impact of frailty on outcomes after cardiac surgery: A systematic review. J. Thorac. Cardiovasc. Surg. 2014, 148, 3110–3117. [Google Scholar] [CrossRef]
- Sohn, B.; Choi, J.W.; Hwang, H.Y.; Jang, M.-J.; Kim, K.H.; Kim, K.-B. Frailty Index is Associated with Adverse Outcomes after Aortic Valve Replacement in Elderly Patients. J. Korean Med. Sci. 2019, 34, e205. [Google Scholar] [CrossRef]
- Hawkins, R.B.; Mehaffey, J.H.; Charles, E.J.; Kern, J.A.; Lim, D.S.; Teman, N.R.; Ailawadi, G. Psoas Muscle Size Predicts Risk-Adjusted Outcomes After Surgical Aortic Valve Replacement. Ann. Thorac. Surg. 2018, 106, 39–45. [Google Scholar] [CrossRef]
- Koter, S.; Cohnert, T.U.; Hindermayr, K.B.; Lindenmann, J.; Brückner, M.; Oswald, W.K.; Werkgartner, G.; Wagner, D. Increased hospital costs are associated with low skeletal muscle mass in patients undergoing elective open aortic surgery. J. Vasc. Surg. 2018, 69, 1227–1232. [Google Scholar] [CrossRef]
- Taniguchi, N.; Hosono, M.; Kuwauchi, S.; Yasumoto, H.; Kawazoe, K. Trunk Muscle Cross-Sectional Area as a Predictive Factor for Length of Postoperative Hospitalization after Surgical Aortic Valve Replacement. Ann. Thorac. Cardiovasc. Surg. 2020, 26, 151–157. [Google Scholar] [CrossRef]
- O’Neill, D.E.; Knudtson, M.L.; Kieser, T.M.; Graham, M.M. Considerations in Cardiac Revascularization for the Elderly Patient: Age Isn’t Everything. Can. J. Cardiol. 2016, 32, 1132–1139. [Google Scholar] [CrossRef]
- Ko, F.C. Preoperative Frailty Evaluation: A Promising Risk-stratification Tool in Older Adults Undergoing General Surgery. Clin. Ther. 2019, 41, 387–399. [Google Scholar] [CrossRef]
- Mihalj, M.; Carrel, T.; Urman, R.D.; Stueber, F.; Luedi, M.M. Recommendations for Preoperative Assessment and Shared Decision-Making in Cardiac Surgery. Curr. Anesthesiol. Rep. 2020, 10, 185–195. [Google Scholar] [CrossRef]
- Hulzebos, E.H.; Smit, Y.; Helders, P.P.; van Meeteren, N.L. Preoperative physical therapy for elective cardiac surgery patients. Cochrane Database Syst. Rev. 2012, 2012, CD010118. [Google Scholar] [CrossRef]
- Zheng, Y.T.; Zhang, J.X. Preoperative exercise and recovery after cardiac surgery: A metaanalysis. BMC Cardiovasc. Disord. 2020, 20, 2. [Google Scholar] [CrossRef]
- Iwatsu, K.; Yamada, S.; Iida, Y.; Sampei, H.; Kobayashi, K.; Kainuma, M.; Usui, A. Feasibility of neuromuscular electrical stimulation immediately after cardiovascular surgery. Arch. Phys. Med. Rehabil. 2015, 96, 63–68. [Google Scholar] [CrossRef]
- Iwatsu, K.; Iida, Y.; Kono, Y.; Yamazaki, T.; Usui, A.; Yamada, S. Neuromuscular electrical stimulation may attenuate muscle proteolysis after cardiovascular surgery: A preliminary study. J. Thorac. Cardiovasc. Surg. 2016, 153, 373–379.e1. [Google Scholar] [CrossRef]
- Kitamura, H.; Yamada, S.; Adachi, T.; Shibata, K.; Tamaki, M.; Okawa, Y.; Usui, A. Effect of Perioperative Neuromuscular Electrical Stimulation in Patients Undergoing Cardiovascular Surgery: A Pilot Randomized Controlled Trial. Semin. Thorac. Cardiovasc. Surg. 2019, 31, 361–367. [Google Scholar] [CrossRef]
- Sumin, A.N.M.; Oleinik, P.A.; Bezdenezhnykh, A.V.; Ivanova, A.V. Neuromuscular electrical stimulation in early rehabilitation of patients with postoperative complications after cardiovascular surgery. Medicine 2020, 99, e22769. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Medrinal, C.; Combret, Y.; Prieur, G.; Quesada, A.R.; Bonnevie, T.; Gravier, F.E.; Lozeron, E.D.; Frenoy, E.; Contal, O.; Lamia, B. Comparison of exercise intensity during four early rehabilitation techniques in sedated and ventilated patients in ICU: A randomised cross-over trial. Crit. Care 2018, 22, 110. [Google Scholar] [CrossRef] [Green Version]
- Paillard, T. Training based on electrical stimulation superimposed onto voluntary contraction would be relevant only as part of submaximal contractions in healthy subjects. Front. Physiol. 2018, 9, 1428. [Google Scholar] [CrossRef] [PubMed]
- Da Cunha, R.A.; Pinfildi, C.E.; Pochini, A.D.C.; Cohen, M. Photobiomodulation therapy and NMES improve muscle strength and jumping performance in young volleyball athletes: A randomized controlled trial study in Brazil. Lasers Med. Sci. 2019, 35, 621–631. [Google Scholar] [CrossRef] [PubMed]
- Adams, G.R.; Harris, R.T.; Woodard, D.; Dudley, G.A. Mapping of electrical muscle stimulation using MRI. J. Appl. Physiol. 1993, 74, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Mancinelli, R.; Toniolo, L.; Di Filippo, E.S.; Doria, C.; Marrone, M.; Maroni, C.R.; Verratti, V.; Bondi, D.; Maccatrozzo, L.; Pietrangelo, T.; et al. Neuromuscular electrical stimulation induces skeletal muscle fiber remodeling and specific gene expression profile in healthy elderly. Front. Physiol. 2019, 10, 1459. [Google Scholar] [CrossRef]
- Maffiuletti, N.A.; Zory, R.; Miotti, D.; Pellegrino, M.A.; Jubeau, M.; Bottinelli, R. Neuromuscular adaptations to electrostimulation resistance training. Am. J. Phys. Med. Rehabil. 2006, 85, 167–175. [Google Scholar] [CrossRef]
- Natsume, T.; Ozaki, H.; Kakigi, R.; Kobayashi, H.; Naito, H. Effects of training intensity in electromyostimulation on human skeletal muscle. Eur. J. Appl. Physiol. 2018, 118, 1339–1347. [Google Scholar] [CrossRef]
- Cerqueira, T.C.F.; Neto, M.L.D.C.; Cacau, L.D.A.P.; Oliveira, G.U.; Júnior, W.M.D.S.; Carvalho, V.O.; de Mendonça, J.T.; Filho, V.J.D.S. Ambulation capacity and functional outcome in patients undergoing neuromuscular electrical stimulation after cardiac valve surgery: A randomised clinical trial. Medicine 2018, 97, e13012. [Google Scholar] [CrossRef]
- Fischer, A.; Spiegl, M.; Altmann, K.; Winkler, A.; Salamon, A.; Themessl-Huber, M.; Mouhieddine, M.; Strasser, E.M.; Schiferer, A.; Paternostro-Sluga, T.; et al. Muscle mass, strength and functional outcomes in critically ill patients after cardiothoracic surgery: Does neuromuscular electrical stimulation help? The Catastim 2 randomized controlled trial. Crit. Care 2016, 20, 30. [Google Scholar] [CrossRef]
- Chen, X.; Hou, L.; Zhang, Y.; Liu, X.; Shao, B.; Yuan, B.; Li, J.; Li, M.; Cheng, H.; Teng, L.; et al. The effects of five days of intensive preoperative inspiratory muscle training on postoperative complications and outcome in patients having cardiac surgery: A randomized controlled trial. Clin. Rehabil. 2019, 33, 913–922. [Google Scholar] [CrossRef]
- Snowdon, D.; Haines, T.; Skinner, E.H. Preoperative intervention reduces postoperative pulmonary complications but not length of stay in cardiac surgical patients: A systematic review. J. Physiother. 2014, 60, 66–77. [Google Scholar] [CrossRef] [Green Version]
- Steinmetz, C.; Bjarnason-Wehrens, B.; Baumgarten, H.; Walther, T.; Mengden, T.; Walther, C. Prehabilitation in patients awaiting elective coronary artery bypass graft surgery—Effects on functional capacity and quality of life: A randomized controlled trial. Clin. Rehabil. 2020, 34, 1256–1267. [Google Scholar] [CrossRef]
- Yau, D.K.W.; Wong, M.K.H.; Wong, W.-T.; Gin, T.; Underwood, M.J.; Joynt, G.M.; Lee, A. PREhabilitation for improving QUality of recovery after ELective cardiac surgery (PREQUEL) study: Protocol of a randomised controlled trial. BMJ Open 2019, 9, e027974. [Google Scholar] [CrossRef]
- Boreskie, K.F.; Hay, J.L.; Kehler, D.S.; Johnston, N.M.; Rose, A.V.; Oldfield, C.J.; Kumar, K.; Toleva, O.; Arora, R.C.; Duhamel, T.A. Prehabilitation: The Right Medicine for Older Frail Adults Anticipating Transcatheter Aortic Valve Replacement, Coronary Artery Bypass Graft, and Other Cardiovascular Care. Clin. Geriatr. Med. 2019, 35, 571–585. [Google Scholar] [CrossRef]
- Neto, M.G.; Oliveira, F.A.; dos Reis, H.F.C.; Rodrigues, E.D.S.; Bittencourt, H.S.; Carvalho, V.O. Effects of Neuromuscular Electrical Stimulation on Physiologic and Functional Measurements in Patients with Heart Failure: A systematic review with meta-analysis. J. Cardiopulm. Rehabil. Prev. 2016, 36, 157–166. [Google Scholar] [CrossRef]
- Katsura, M.; Kuriyama, A.; Takeshima, T.; Fukuhara, S.; Furukawa, T.A. Preoperative inspiratory muscle training for postoperative pulmonary complications in adults undergoing cardiac and major abdominal surgery. Cochrane Database Syst. Rev. 2015, 2015, CD010356. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NMES Group (n = 62) | Control Group (n = 60) | p Value | |
|---|---|---|---|
| Men (n, %) | 44 (71.0) | 39 (65.0) | 0.339 |
| Age (years) | 62.0 [57.5; 66.6] | 63.5 [59.0; 69.0] | 0.131 |
| Body mass index (kg/m2) | 27.4 [25.4; 31.5] | 28.7 [25.9; 33.3] | 0.198 |
| FC angina pectoris ≥ 3 (n, %) | 16 (25.8) | 20 (33.33) | 0.337 |
| Myocardial infarction history (n, %) | 31 (50.0) | 30 (50.0) | 0.485 |
| GFR (mL/min/1.73 m2) | 84.5 [65.5; 94.5] | 78.0 [64.0; 97.0] | 0.778 |
| Hypertension (n, %) | 53 (85.5) | 47 (78.3) | 0.654 |
| PCI history (n, %) | 6 (9.7) | 7 (11.7) | 0.709 |
| Stroke history (n, %) | 5 (8.1) | 8 (13.3) | 0.313 |
| Permanent atrial fibrillation (n, %) | 10 (16.1) | 8 (13.3) | 0.748 |
| Diabetes mellitus (n, %) | 22 (35.5) | 15 (25.0) | 0.280 |
| Peripheral arterial disease (n, %) | 10 (16.1) | 10 (16.7) | 0.840 |
| COPD (n, %) | 10 (16.1) | 5 (8.3) | 0.214 |
| NMES Group (n = 62) | Control Group (n = 60) | p Value | |
|---|---|---|---|
| Left Atrial Diameter (cm) | 4.5 [4.2; 5.0] | 4.6 [4.2; 5.2] | 0.387 |
| Left Ventricle End-Systolic Volume (mL) | 74.0 [47.0; 113.0] | 64.0 [47.0; 97.0] | 0.245 |
| Left Ventricle End-Diastolic Volume (mL) | 180.0 [135.0; 231.0] | 173.0 [141.0;209.0] | 0.636 |
| Interventricular Septal Thickness (mm) | 1.0 [1.0; 1.2] | 1.0 [1.0; 1.3] | 0.378 |
| Posterior wall thickness (mm) | 1.0 [1.0; 1.2] | 1.0 [1.0; 1.2] | 0.657 |
| Aorta (cm) | 3.5 [3.4; 3.8] | 3.5 [3.3; 3.7] | 0.221 |
| Left ventricular ejection fraction (%) | 60.0 [48.0; 66.0] | 63.0 [48.0; 67.0] | 0.142 |
| Pulmonary artery systolic pressure(mmHg) | 29.5 [23.0; 35.0] | 32.0 [24.0; 45.0] | 0.308 |
| E/A ratio | 0.69 [0.62; 1.06] | 0.77 [0.66; 1.02] | 0.306 |
| Mitral regurgitation ≥ grade 3 (n, %) | 8 (12.9) | 6 (10.0) | 0.686 |
| Mitral stenosis (n, %) | 3 (4.8) | 8 (13.3) | 0.084 |
| Aortic valve regurgitation ≥ 3 grade (n, %) | 4 (6.5) | 1 (1.7) | 0.202 |
| Aortic stenosis (n, %) | 8 (12.9) | 9 (15.0) | 0.656 |
| Tricuspid regurgitation ≥ grade 3 (n, %) | 4 (6.5) | 7 (11.7) | 0.274 |
| Internal carotid artery stenosis ≥50% (n, %) | 10 (16.1) | 19 (31.7) | 0.035 |
| Chronic lower limb ischemia (n, %) | 12 (19.4) | 9 (15.0) | 0.529 |
| Glucose (mmol/L) | 5.8 [5.3; 6.5] | 5.8 [5.4; 6.3] | 0.619 |
| Creatinine (μmol/L) | 81.0 [71.0; 93.0] | 82.0 [70.0; 97.0] | 0.934 |
| NMES Group (n = 62) | Control Group (n = 60) | ||
|---|---|---|---|
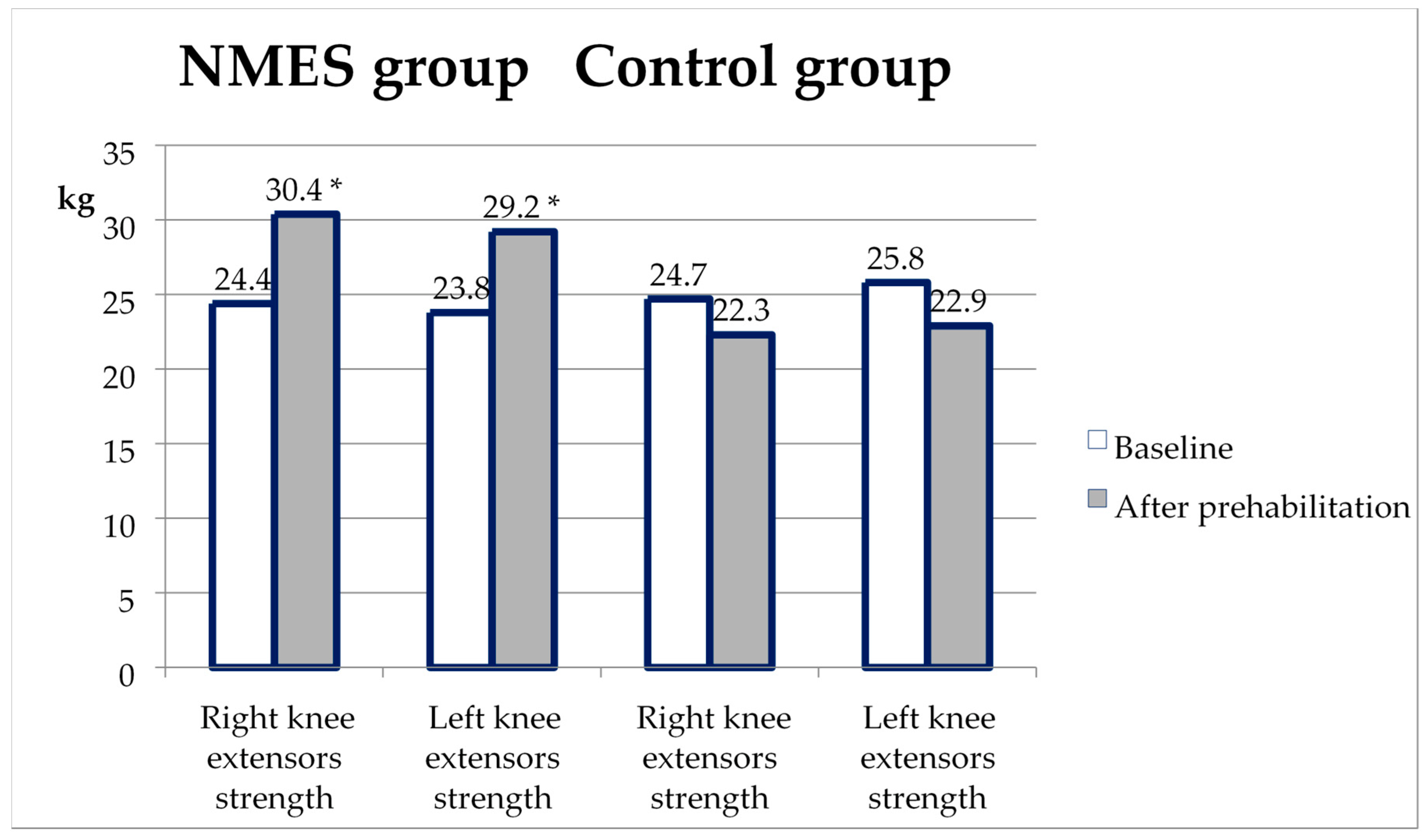
| Right knee extensors strength (kg) | Baseline | 24.4 [18.3; 31.4] | 24.7 [20.1; 33.2] |
| After prehabilitation | 30.4 [23.8; 36.2] b | 22.3 [18.9; 30.4] b | |
| Left knee extensors strength (kg) | Baseline | 23.8 [19.3; 31.3] | 25.8 [19.2; 31.3] |
| After prehabilitation | 29.2 [23.6; 35.4] b | 22.9 [18.9; 27.8] b | |
| Right knee flexors strength (kg) | Baseline | 18.9 [13.3; 24.0] | 19.6 [13.1; 26.0] |
| After prehabilitation | 21.7 [16.6; 25.1] a | 16.7 [12.1; 23.3] a | |
| Left knee flexors strength (kg) | Baseline | 19.3 [14.3; 24.5] | 19.5 [13.0; 24.3] |
| After prehabilitation | 21.9 [17.3; 26.7] a | 18.2 [13.4; 22.2] a | |
| Right handgrip strength (kg) | Baseline | 28.5 [20.5; 34.0] | 29.0 [19.0; 34.0] |
| After prehabilitation | 31.5 [22.0; 34.0] | 27.0 [19.0; 33.0] | |
| Left handgrip strength (kg) | Baseline | 25.0 [18.0; 31.0] | 24.0 [15.0; 31.0] |
| After prehabilitation | 25.0 [18.0; 32.0] | 22.0 [14.0; 28.0] | |
| 6MWT distance (m) | Baseline | 300.0 [261,0;371,0] | 304.5 [253.0; 380.0] |
| After prehabilitation | 331.0 [280,0;375,0] a | 285.5 [246.0; 342.0] a |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sumin, A.N.; Oleinik, P.A.; Bezdenezhnykh, A.V.; Bezdenezhnykh, N.A. Prehabilitation in Cardiovascular Surgery: The Effect of Neuromuscular Electrical Stimulation (Randomized Clinical Trial). Int. J. Environ. Res. Public Health 2023, 20, 2678. https://doi.org/10.3390/ijerph20032678
Sumin AN, Oleinik PA, Bezdenezhnykh AV, Bezdenezhnykh NA. Prehabilitation in Cardiovascular Surgery: The Effect of Neuromuscular Electrical Stimulation (Randomized Clinical Trial). International Journal of Environmental Research and Public Health. 2023; 20(3):2678. https://doi.org/10.3390/ijerph20032678
Chicago/Turabian StyleSumin, Alexey N., Pavel A. Oleinik, Andrey V. Bezdenezhnykh, and Natalia A. Bezdenezhnykh. 2023. "Prehabilitation in Cardiovascular Surgery: The Effect of Neuromuscular Electrical Stimulation (Randomized Clinical Trial)" International Journal of Environmental Research and Public Health 20, no. 3: 2678. https://doi.org/10.3390/ijerph20032678