
I Don’t Want to Be Thin! Fear of Weight Change Is Not Just a Fear of Obesity: Research on the Body Mass Anxiety Scale


Abstract
:1. Introduction
2. Study 1—Scale Design
2.1. Procedure for Developing Scale Items
“…, I have a problem, I recently finished a job (I was on the move) which made me lose a bit of weight by eating less, now I have been out of work for a few days (for now) and I am practically not active at all, just sometimes I clean up, go out with the dogs, I eat relatively little and I am very afraid of getting fat (I have a mental problem with this), if I limit my food will I not get fat? The thought of getting fat in a few weeks scares me.”“… I can’t gain weight I am 174 cm tall and 55 kg how can I help myself? I avoid meeting people because they keep asking me why I’m so skinny. I hate it, I’m afraid I’ll never get fat …”“I overeat and I can’t control it, when I try to limit food, I get the fear that I’m going to lose weight and yet I already weigh too much …”
2.2. Participants and Procedure
2.3. Results and Discussion
3. Study 2—Translation and Validation of EN-BMAS-20 English Version
3.1. Scale Translation Procedure
3.2. Participants and Procedure
3.3. Results and Discussion
4. Study 3—Characteristics of Anxiety Related to Weight Change
4.1. Participants and Procedure
4.2. Methods
4.2.1. Body Mass Index (BMI)
4.2.2. Self-Weight Status Perception (SWSP)
4.2.3. Personality
4.2.4. Perceived Stress Level
4.2.5. Anxiety and Depression
4.2.6. Impulsiveness
4.2.7. Sensitivity to Punishment and Reward
4.2.8. Self-Control
4.2.9. Body Image
4.2.10. Data Analysis Procedure
4.3. Results and Discussion
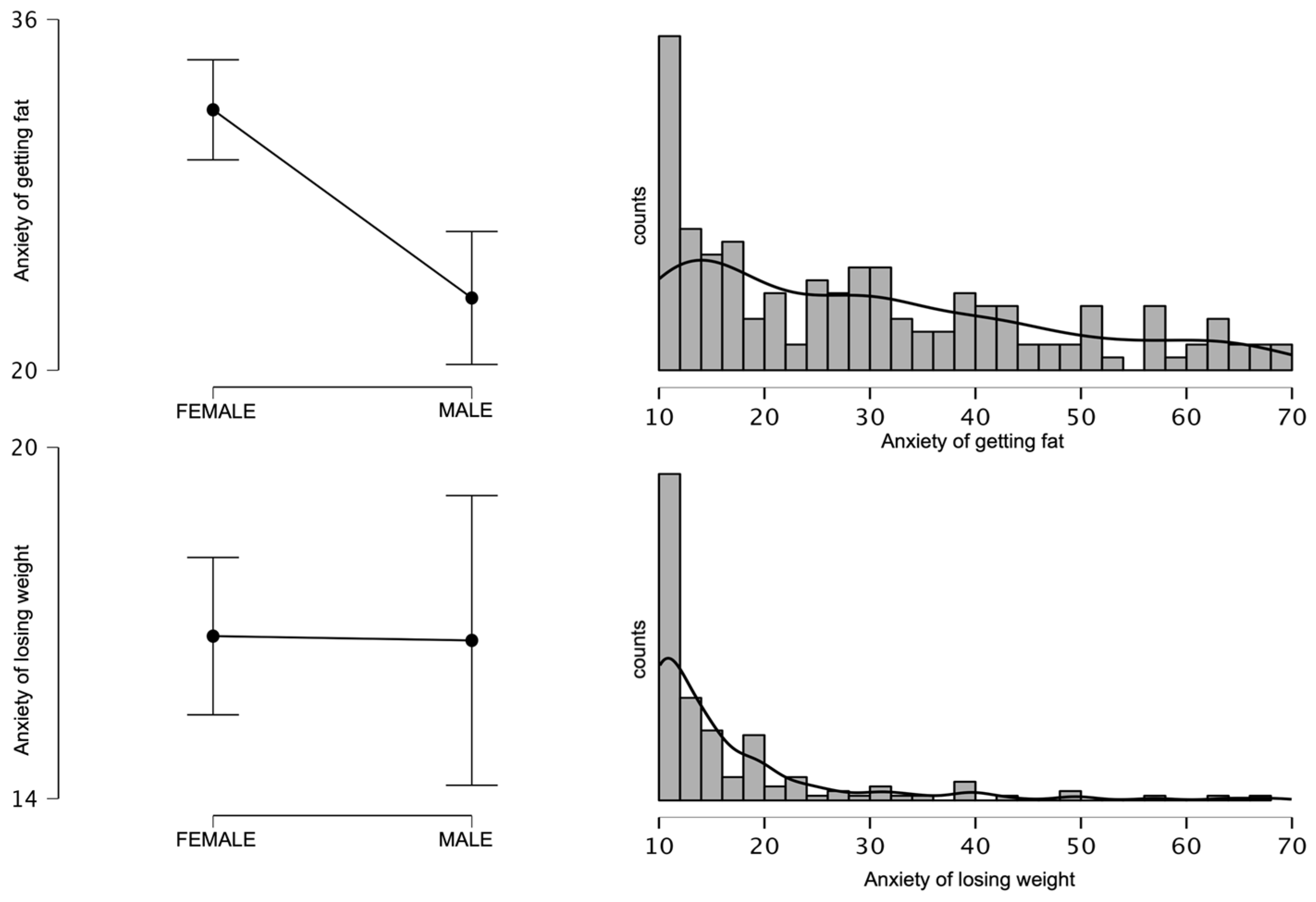
4.3.1. Variables Distribution and Their Relationship with Gender
4.3.2. Association of BMI and Self Perception of Weight Status with Body Mass Anxiety
4.3.3. Association of Weighing Frequency and Dietary Adherence with Body Mass Anxiety
4.3.4. Correlation Analysis of Body Mass Anxiety Scales with Other Variables
5. Main Discussion
6. Conclusions
7. Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CFA | Confirmatory factor analysis |
| AGF | Anxiety about getting fat |
| ALW | Anxiety about losing weight |
| BMAS-20 | Body mass anxiety scale—20 items |
| PL-BMAS-20 Polish version of body mass anxiety scale | 20 items |
| EN-BMAS-20 English version of body mass anxiety scale | 20 items |
| BMI | Body mass index |
| HADS | The Hospital Anxiety and Depression Scale |
| SWSP | Self-perception of weight status |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Czasami Odczuwamy Lęk Związany z Naszym Ciałem, Jego Wyglądem Czy po Prostu Masą Ciała. Poniżej Znajdują Się Zdania Opisujące Takie Przeżycia. Określ na Podanej Skali Jak Bardzo Dotyczą One Ciebie. Jeżeli Opisane Sytuacje Nie Miały Miejsca Wyobraź je Sobie i Spróbuj Odpowiedzieć Jak Bardzo Mogłyby Cię Dotyczyć | Zupełnie Mnie Nie Dotyczy | w Pełni Mnie Dotyczy | |||||
|---|---|---|---|---|---|---|---|
| Czasami jak wydaje mi się, że przytyłam/łem to czuję negatywne napięcie i ogarniający mnie smutek | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Boję się, że w przyszłości schudnę i nic na to nie poradzę | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Czasami jak wydaje mi się, że schudam/łem czuję, że trace radośc życia | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Po każdym nawet małym posiłku mam wrażenie, że przybyło mi ciała | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Gdy widzę, że moja masa ciała trochę spadła czuję lęk | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Czuje, że moje ciało jest jak szkielet i nie jest atrakcyjne | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Boje się czasami na siebie patrzeć z obawy, że przytyłam/łem | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Czasami mam wrażenie, że tyję od samego oddychania | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Jedząc czuję napięcie związane wpływem posiłku na wygląd mojego ciała | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Przejadam się i nie umiem tego kontrolować, inaczej pojawia się lęk że stracę kilogramy | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Są dni, kiedy patrząc na siebie np. w lustrze mam wrażenie, że znowu przytyłam/łem | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Po zjedzeniu zdarza mi się mieć wrażenie, że jestem od razu grubsza/y | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Bywają dni kiedy patrząc na swoje ciało w lustrze mam wrażenie że znowu schudłam/łem | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Obawiam się sytuacji jedzenia z innymi i ich komentarzy, że nic nie jem i jestem chuda/y | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Zdarza się, że jem na siłę, żeby tylko nie schudnąć | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Unikam ważenia się, bo wywołuje u mnie lęk, że schudłam/em | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Ogólnie unikam oglądani się w lustrze, żeby nie okazało się że schudłam/em | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Nawet niewielki wzrost wagi powoduje u mnie lęk | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Boję się wejść na wagę, żeby się nie okazało, że się zmieniła | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Nie lubię się ważyć, bo obawiam się, że przytyłam/em | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
Appendix B
| Sometimes You Can Feel Anxious about Your Body Image, Appearance or Body Weight. Below Are the Statements—On the Scales Provided, Please Indicate How It Applies to You. If the Statement Doesn’t Apply to You, Try to Put Yourself in Such a Situation and Answer the Question | Does Not Concern Me at All | Fully Concerns Me | |||||
|---|---|---|---|---|---|---|---|
| Sometimes when it seems to me that I have gained weight, I feel negative tension and overwhelming sadness. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| I am afraid that in the future I will lose weight and I cannot do anything about it. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Sometimes, when it seems to me that I have lost weight, I feel that I am losing the joy of life. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| After each meal, even a small one, I have the feeling that I have gained weight. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| When I see that my body weight has dropped a little, I feel anxious. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| I have the feeling that my body is like a skeleton and is not attractive. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Sometimes I am afraid to look at myself because I’m afraid that I have gained weight. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Sometimes it feels like I’m getting fat just from breathing. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| During meals I feel stress about how it will influence my body. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| I overeat and I can’t control it, otherwise I’m afraid that I will lose weight. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| There are days when looking at myself, e.g., in the mirror, I have a feeling that I have gained weight again. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| After meals, sometimes I have the impression that I am immediately fatter. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| There are days when looking at my body in the mirror I have the impression that I lost weight again. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| I’m afraid of having meals with others and their comments that I don’t eat anything and I’m skinny. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| It happens that I force myself to eat to not lose weight. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| I avoid weighing myself because it makes me afraid that I have lost weight. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Generally, I avoid looking in the mirror so that it does not turn out that I have lost weight. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Even a slight increase in weight makes me anxious. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| I’m afraid to step on the scale because it could turn out that my weight has changed. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| I do not like to weigh myself because I am afraid that I have gained weight. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
Appendix C
| Score | AGF | ALW | |
|---|---|---|---|
| (Sum of Points): | |||
| Question | 1 | - | |
| 2 | - | ||
| 3 | - | ||
| 4 | - | ||
| 5 | - | ||
| 6 | - | ||
| 7 | - | ||
| 8 | - | ||
| 9 | - | ||
| 10 | - | ||
| 11 | - | ||
| 12 | - | ||
| 13 | - | ||
| 14 | - | ||
| 15 | - | ||
| 16 | - | ||
| 17 | - | ||
| 18 | - | ||
| 19 | - | ||
| 20 | - | ||
References
- Lacaille, L.J.; Dauner, K.N.; Bas, R.J.K.; Pedersen, J. Psychosocial and Environmental Determinants of Eating Behaviors, Physical Activity, and Weight Change among College Students: A Qualitative Analysis. J. Am. Coll. Health 2011, 59, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Gahagan, S. Development of eating behavior: Biology and context. J. Dev. Behav. Pediatr. 2012, 33, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Guzek, D.; Skolmowska, D.; Głąbska, D. Appetitive Traits in a Population-Based Study of Polish Adolescents within the PLACE-19 Study: Validation of the Adult Eating Behavior Questionnaire. Nutrients 2020, 12, 3889. [Google Scholar] [CrossRef] [PubMed]
- Dondzilo, L.; Rieger, E.; Jayawardena, N.; Bell, J. Drive for Thinness Versus Fear of Fat: Approach and Avoidance Motivation Regarding Thin and Non-thin Images in Women. Cogn. Ther. Res. 2019, 43, 585–593. [Google Scholar] [CrossRef]
- Major, B.; Hunger, J.M.; Bunyan, D.P.; Miller, C.T. The ironic effects of weight stigma. J. Exp. Soc. Psychol. 2014, 51, 74–80. [Google Scholar] [CrossRef]
- Carpino, T.; Louanna, T. Young Women’s Perceptions and Experiences of Skinny and Fat Shaming. Ph.D. Thesis, Carleton University, Ottawa, ON, Canada, 2017. [Google Scholar] [CrossRef]
- Hund, A.R.; Espelage, D.L. Childhood emotional abuse and disordered eating among undergraduate females: Mediating influence of alexithymia and distress. Child Abus. Negl. 2006, 30, 393–407. [Google Scholar] [CrossRef] [PubMed]
- Striegel-Moore, R.H.; Cachelin, F.M. Etiology of Eating Disorders in Women. Couns. Psychol. 2001, 29, 635–661. [Google Scholar] [CrossRef]
- Toyokawa, S.; Uddin, M.; Koenen, K.C.; Galea, S. How does the social environment ‘get into the mind’? Epigenetics at the intersection of social and psychiatric epidemiology. Soc. Sci. Med. 2012, 74, 67–74. [Google Scholar] [CrossRef]
- Reber, A.S.; Reber, E.S.; Kurcz, I.; Skarzyńska, K.; Janasiewicz-Kruszyńska, B. The Penguin Dictionary of Psychology; Penguin Press: London, UK, 2005. [Google Scholar] [CrossRef]
- Saha, S.; Lim, C.C.W.; Cannon, D.L.; Burton, L.; Bremner, M.; Cosgrove, P.; Huo, Y.; McGrath, J. Co-morbidity between mood and anxiety disorders: A systematic review and meta-analysis. Depress. Anxiety 2021, 38, 286–306. [Google Scholar] [CrossRef]
- Musher-Eizenman, D.R.; Holub, S.C.; Miller, A.B.; Goldstein, S.E.; Edwards-Leeper, L. Body Size Stigmatization in Preschool Children: The Role of Control Attributions. J. Pediatr. Psychol. 2004, 29, 613–620. [Google Scholar] [CrossRef]
- Vartanian, L.R.; Herman, C.P.; Polivy, J. Implicit and explicit attitudes toward fatness and thinness: The role of the internalization of societal standards. Body Image 2005, 2, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Laessle, R.G.; Tuschl, R.J.; Kotthaus, B.C.; Pirke, K.M. A Comparison of the Validity of Three Scales for the Assessment of Dietary Restraint. J. Abnorm. Psychol. 1989, 98, 504. [Google Scholar] [CrossRef] [PubMed]
- Cash, T.F.; Counts, B.; Huffine, C.E. Current and vestigial effects of overweight among women: Fear of fat, attitudinal body image, and eating behaviors. J. Psychopathol. Behav. Assess. 1990, 12, 157–167. [Google Scholar] [CrossRef]
- Amiri, S.; Behnezhad, S. Obesity and anxiety symptoms: A systematic review and meta-analysis. Neuropsychiatrie 2019, 33, 72–89. [Google Scholar] [CrossRef]
- Willem, C.; Gandolphe, M.C.; Doba, K.; Roussel, M.; Verkindt, H.; Pattou, F.; Nandrino, J.L. Eating in case of emotion dys-regulation, depression and anxiety: Different pathways to emotional eating in moderate and severe obesity. Clin. Obes. 2020, 10, e12388. [Google Scholar] [CrossRef]
- Guerdjikova, A.I.; Mori, N.; Casuto, L.S.; McElroy, S.L. Update on Binge Eating Disorder. Med. Clin. N. Am. 2019, 103, 669–680. [Google Scholar] [CrossRef]
- Suzuki, Y.; Ikeda, A.; Maruyama, K.; Sakamoto, N.; Wada, H.; Tanigawa, T. The association between obesity and hyperactivity/anxiety among elementary school students in Japan. Int. J. Behav. Med. 2020, 27, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, E.C.; Haase, A.M.; Verplanken, B. Anxiety and the development and maintenance of anorexia nervosa: Protocol for a systematic review. Syst. Rev. 2018, 7, 14. [Google Scholar] [CrossRef] [Green Version]
- Keski-Rahkonen, A.; Mustelin, L. Epidemiology of eating disorders in Europe: Prevalence, incidence, comorbidity, course, consequences, and risk factors. Curr. Opin. Psychiatry 2016, 29, 340–345. [Google Scholar] [CrossRef]
- Goldfarb, L.A.; Dykens, E.M.; Gerrard, M. Goldfarb Fear of Fat Scale. J. Personal. Assess. 1985, 49, 329–332. [Google Scholar] [CrossRef]
- Przybyła-Basista, H.; Buszman, K.; Flakus, M. An examination of the factor structure of the Goldfarb Fear of Fat Scale in clinical and non-clinical samples of Polish women. Body Image 2022, 40, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Borgers, T.; Krüger, N.; Vocks, S.; Thomas, J.J.; Plessow, F.; Hartmann, A.S. Overcoming limitations of self-report: An assessment of fear of weight gain in anorexia nervosa and healthy controls using implicit association tests. J. Eat. Disord. 2021, 9, 26. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.C.; Bewell-Weiss, C.V. Nonfat phobic anorexia nervosa: Clinical characteristics and response to inpatient treatment. Int. J. Eat. Disord. 2011, 44, 220–224. [Google Scholar] [CrossRef]
- Costa, P.T.; McCrae, R.R. The Revised NEO Personality Inventory (NEO-PI-R). In The SAGE Handbook of Personality Theory and Assessment: Volume 2—Personality Measurement and Testing; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2008; pp. 179–198. [Google Scholar] [CrossRef]
- Juczyński, Z.; Ogińska-Bulik, N. Narzędzia Pomiaru Stresu i Radzenia Sobie ze Stresem; Pracownia Testów Psychologicznych: Warsaw, Poland, 2009. [Google Scholar]
- Stern, A. The Hospital Anxiety and Depression Scale. Occup. Med. (Chic. Ill.) 2014, 64, 393–394. [Google Scholar] [CrossRef]
- Poprawa, R. Research on the Polish short version of the Impulsive Behavior Scale UPPS-P. Alcohol. Drug Addict. 2019, 32, 35–62. [Google Scholar] [CrossRef]
- Wytykowska, A.; Białaszek, W.; Ostaszewski, P. Psychometryczne właściwości polskiej wersji krótkiej skali wrażliwości nakary i nagrody (SPSRQ-SF Cooper i Gomez, 2008). Stud. Psychol. 2014, 52, 28–39. [Google Scholar]
- Nęcka, E.; Wujcik, R.; Orzechowski, J.; Gruszka, A.; Janik, B.; Nowak, M.; Wójcik, N. NAS-50 and NAS-40: New scales for the assessment of self-control. Pol. Psychol. Bull. 2016, 47, 346–355. [Google Scholar] [CrossRef]
- Lipowska, M.; Lipowski, M. Polish normalization of the Body Esteem Scale. Health Psychol. Rep. 2013, 1, 72–81. [Google Scholar] [CrossRef]
- George, D.; Mallery, P. IBM SPSS Statistics 23 Step by Step A Simple Guide and Reference 14th Edition Answers to Selected Exercises; Routledge: New York, NY, USA, 2019. [Google Scholar] [CrossRef]
- Sawilowsky, S.S. New Effect Size Rules of Thumb. J. Mod. Appl. Stat. Methods 2009, 8, 597–599. [Google Scholar] [CrossRef]
- Chambliss, H.O.; Finley, C.E.; Blair, S.N. Attitudes toward Obese Individuals among Exercise Science Students. Med. Sci. Sports Exerc. 2004, 36, 468–474. [Google Scholar] [CrossRef]
- Allison, D.B.; Basile, V.C.; Yuker, H.E. The measurement of attitudes toward and beliefs about obese persons. Int. J. Eat. Disord. 1991, 10, 599–607. [Google Scholar] [CrossRef]
- Gerlach, G.; Herpertz, S.; Loeber, S. Personality traits and obesity: A systematic review. Obes. Rev. 2015, 16, 32–63. [Google Scholar] [CrossRef] [PubMed]
- Michaud, A.; Vainik, U.; Garcia-Garcia, I.; Dagher, A. Overlapping Neural Endophenotypes in Addiction and Obesity. Front. Endocrinol. 2017, 8, 127. [Google Scholar] [CrossRef] [PubMed]
- Tapper, K.; Baker, L.; Jiga-Boy, G.; Haddock, G.; Maio, G.R. Sensitivity to reward and punishment: Associations with diet, alcohol consumption, and smoking. Pers. Individ. Differ. 2015, 72, 79–84. [Google Scholar] [CrossRef]
- Conrad, S.W. Resistance of the obese to reducing. J. Am. Diet. Assoc. 1954, 30, 581–588. [Google Scholar] [CrossRef]
- Matoti-Mvalo, T.; Puoane, T. Perceptions of body size and its association with HIV/AIDS. S. Afr. J. Clin. Nutr. 2011, 24, 40–45. [Google Scholar] [CrossRef]
- Puoane, T.; Hughes, G.D. Impact of the HIV/AIDS pandemic on non-communicable disease prevention. S. Afr. Med. J. 2005, 95, 228–230. [Google Scholar]
- Tiggemann, M.; Raven, M. Dimensions of control in bulimia and anorexia nervosa: Internal control, desire for control, or fear of losing self-control? Eat. Disord. 1998, 6, 65–71. [Google Scholar] [CrossRef]
- A Rikani, A.; Choudhry, Z.; Choudhry, A.M.; Ikram, H.; Asghar, M.W.; Kajal, D.; Waheed, A.; Mobassarah, N.J. A critique of the literature on etiology of eating disorders. Ann. Neurosci. 2013, 20, 157–161. [Google Scholar] [CrossRef]
- Ramacciotti, C.E.; Dell’Osso, L.; Paoli, R.A.; Ciapparelli, A.; Coli, E.; Kaplan, A.S.; Garfinkel, P.E. Characteristics of eating disorder patients without a drive for thinness. Int. J. Eat. Disord. 2002, 32, 206–212. [Google Scholar] [CrossRef]
- Korn, J.; Vocks, S.; Rollins, L.H.; Thomas, J.J.; Hartmann, A.S. Fat-Phobic and Non-Fat-Phobic Anorexia Nervosa: A Conjoint Analysis on the Importance of Shape and Weight. Front. Psychol. 2020, 11, 90. [Google Scholar] [CrossRef] [PubMed]
- Levinson, C.A.; Zerwas, S.; Calebs, B.; Forbush, K.; Kordy, H.; Watson, H.; Hofmeier, S.; Levine, M.; Crosby, R.D.; Peat, C.; et al. The core symptoms of bulimia nervosa, anxiety, and depression: A network analysis. J. Abnorm. Psychol. 2017, 126, 340–354. [Google Scholar] [CrossRef] [PubMed]
- Mashalpourfard, M. Relationship of social anxiety, body image perception and depression with bulimia nervosa and anorexia nervosa in youth. J. Fundam. Ment. Health 2018, 20, 138–147. [Google Scholar]
- Bulik, C.M.; Allison, D.B. The genetic epidemiology of thinness. Obes. Rev. 2001, 2, 107–115. [Google Scholar] [CrossRef]
- Tantleff-Dunn, S.; Hayes, S.; Braun, C.P. How did you get so thin? The effect of attribution on perceptions of underweight females. Eat. Weight. Disord.-Stud. Anorexia, Bulim. Obes. 2009, 14, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Lox, C.L.; Osborn, M.C.; Pellett, T.L. Body Image and Affective Experiences of Subjectively Underweight Females: Implications for Exercise Behavior. J. Appl. Biobehav. Res. 1998, 3, 110–118. [Google Scholar] [CrossRef]
- Harmatz, M.; Gronendyke, J.; Thomas, T. The underweight male: The unrecognized problem group of body image research. J. Obes. Weight. Regul. 1985, 4, 258–267. [Google Scholar]
- Liyanage, G.; Karunainathan, T.; Jeyarajah, L.; Thevatheepan, P.; Thavendra, M.; Seneviwickrama, M. Body image dissatisfaction and its determinants in urban Sri Lankan adolescents. Ceylon. Med. J. 2021, 66, 185. [Google Scholar] [CrossRef]
- Jimenez-Flores, P.; Jimenez-Cruz, A.; Bacardi-Gascon, M. Body-image dissatisfaction in children and adolescents: A systematic review. Nutr. Hosp. 2017, 34, 479–489. [Google Scholar]
- Henningsen, L. Attaining Idealized Status: Motivation to Diet and Exercise after Exposure to Women with Ideal Body Types in Relationships. Ph.D. Thesis, Carroll College, Helena, Montana, 1899. [Google Scholar]
- Ogden, J. The Psychology of Eating: From Healthy to Disordered Behavior, 2nd ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2010. [Google Scholar]
- Lindberg, L.; Hagman, E.; Danielsson, P.; Marcus, C.; Persson, M. Anxiety and depression in children and adolescents with obesity: A nationwide study in Sweden. BMC Med. 2020, 18, 30. [Google Scholar] [CrossRef]
- Rostampour, N.; Naderi, M.; Kheiri, S.; Safavi, P. The Relationship Between Body Mass Index and Depression, Anxiety, Body Image, and Eating Attitudes in Adolescents in Iran. Adv. Biomed. Res. 2022, 11, 51. [Google Scholar] [PubMed]
- Rajan, T.M.; Menon, V. Psychiatric disorders and obesity: A review of association studies. J. Postgrad. Med. 2017, 63, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Scott, K.M.; Bruffaerts, R.; E Simon, G.; Alonso, J.; Angermeyer, M.; de Girolamo, G.; Demyttenaere, K.; Gasquet, I.; Haro, J.M.; Karam, E.; et al. Obesity and mental disorders in the general population: Results from the world mental health surveys. Int. J. Obes. 2008, 32, 192–200. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, S.A.; Ball, K.; Crawford, D.; Mishra, G.D. An Index of Diet and Eating Patterns Is a Valid Measure of Diet Quality in an Australian Population. J. Nutr. 2008, 138, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Ernst, M.; Werner, A.M.; Tibubos, A.N.; Beutel, M.E.; de Zwaan, M.; Brähler, E. Gender-Dependent Associations of Anxiety and Depression Symptoms With Eating Disorder Psychopathology in a Representative Population Sample. Front. Psychiatry 2021, 12, 645654. [Google Scholar] [CrossRef] [PubMed]
- Brumpton, B.; Langhammer, A.; Romundstad, P.; Chen, Y.; Mai, X.-M. The associations of anxiety and depression symptoms with weight change and incident obesity: The HUNT Study. Int. J. Obes. 2013, 37, 1268–1274. [Google Scholar] [CrossRef]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.; Zitman, F.G. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef]
- Sahle, B.W.; Breslin, M.; Sanderson, K.; Patton, G.; Dwyer, T.; Venn, A.; Gall, S. Association between depression, anxiety and weight change in young adults. BMC Psychiatry 2019, 19, 1–12. [Google Scholar] [CrossRef]
- Milaneschi, Y.; Simmons, W.K.; Van Rossum, E.F.C.; Penninx, B.W. Depression and obesity: Evidence of shared biological mechanisms. Mol. Psychiatry 2019, 24, 18–33. [Google Scholar] [CrossRef]
- Schooler, D.; Daniels, E.A. “I am not a skinny toothpick and proud of it”: Latina adolescents’ ethnic identity and responses to mainstream media images. Body Image 2014, 11, 11–18. [Google Scholar] [CrossRef]
- Tuoyire, D.A.; Kumi-Kyereme, A.; Doku, D.T.; Amo-Adjei, J. Perceived ideal body size of Ghanaian women: “Not too skinny, but not too fat”. Women Health 2018, 58, 583–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| Items | Anxiety about | Alfa Cr/% of the Variance | ||
|---|---|---|---|---|
| Getting Fat | Losing Weight | |||
| 7. Boje się czasami na siebie patrzeć z obawy, że przytyłam/łem. (Sometimes I am afraid to look at myself because I’m afraid that I have gained weight) | 0.925 | 0.964/39.3% | 0.916/70.7% | |
| 17. Nawet niewielki wzrost wagi powoduje u mnie lęk. (Generally, I avoid looking in the mirror so that it does not turn out that I have lost weight) | 0.893 | |||
| 8. Czasami mam wrażenie, że tyję od samego oddychania. (Sometimes it feels like I’m getting fat just from breathing) | 0.885 | |||
| 20. Nie lubię się ważyć, bo obawiam się, że przytyłam/em. (I do not like to weigh myself because I am afraid that I have gained weight) | 0.878 | |||
| 4. Po każdym nawet małym posiłku mam wrażenie, że przybyło mi ciała (After each, even a small meal, I have the feeling that I have gained weight) | 0.865 | |||
| 11. Są dni, kiedy patrząc na siebie np. w lustrze mam wrażenie, że znowu przytyłam/łem (There are days when looking at myself, e.g., in the mirror, I have a feeling that I have gained weight again) | 0.858 | |||
| 19. Boję się wejść na wagę, żeby się nie okazało, że się zmieniła (I’m afraid to step on the scale because it could turn out that my weight has changed) | 0.855 | |||
| 12. Po zjedzeniu zdarza mi się mieć wrażenie, że jestem od razu grubsza/y (After meals, sometimes I have the impression that I am immediately fatter) | 0.851 | |||
| 9. Jedząc czuję napięcie związane wpływem posiłku na wygląd mojego ciała (During meals I feel stress about how it will influence my body) | 0.838 | |||
| 1. Czasami jak wydaje mi się, że przytyłam/łem to czuję negatywne napięcie i ogarniający mnie smutek (Sometimes when it seems to me that I have gained weight, I feel negative tension and overwhelming sadness) | 0.834 | |||
| 15. Zdarza się, że jem na siłę, żeby tylko nie schudnąć (It happens that I force myself to eat to not lose the weight) | 0.925 | 0.935/31.4% | ||
| 16. Unikam ważenia się, bo wywołuje u mnie lęk, że schudłam/em (I avoid weighing myself because it makes me afraid that I have lost weight) | 0.882 | |||
| 5. Gdy widzę, że moja masa ciała trochę spadła czuję lęk (When I see that my body weight has dropped a little, I feel anxious) | 0.878 | |||
| 6. Czuje, że moje ciało jest jak szkielet i nie jest atrakcyjne (I have the feeling that my body is like a skeleton and is not attractive) | 0.850 | |||
| 17. Ogólnie unikam oglądani się w lustrze, żeby nie okazało się że schudłam/em (Generally, I avoid looking in the mirror so that it does not turn out that I have lost weight) | 0.832 | |||
| 14. Obawiam się sytuacji jedzenia z innymi i ich komentarzy, że nic nie jem i jestem chuda/y (I’m afraid of having meals with others and their comments that I don’t eat anything and I’m skinny) | 0.772 | |||
| 2. Boję się, że w przyszłości schudnę i nic na to nie poradzę (I am afraid that in the future I will lose weight and I cannot do anything about it) | 0.753 | |||
| 13. Bywają dni, kiedy patrząc na swoje ciało w lustrze mam wrażenie, że znowu schudłam/łem (There are days when looking at my body in the mirror I have the impression that I lost weight again) | 0.739 | |||
| 3. Czasami jak wydaje mi się, że schudłam/łem czuję, że tracę radość życia (Sometimes when it seems to me that I have lost weight, I feel that I am losing the joy of life) | 0.727 | |||
| 10. Przejadam się i nie umiem tego kontrolować, inaczej pojawia się lęk że stracę kilogramy (I overeat and I can’t control it, otherwise I’m afraid that I will lose weight) | 0.666 | |||
| Items | Anxiety about | Alfa Cr/% of the Variance | ||
|---|---|---|---|---|
| Getting Fat | Losing Weight | |||
| 20. I do not like to weigh myself because I am afraid that I have gained weight. | 0.921 | 38.75%/0.949 | 64.88%/0.908 | |
| 18. Even a slight increase in weight makes me anxious. | 0.920 | |||
| 12. After meals, sometimes I have the impression that I am immediately fatter. | 0.918 | |||
| 7. Sometimes I am afraid to look at myself because I’m afraid that I have gained weight. | 0.872 | |||
| 11. There are days when looking at myself, e.g., in the mirror, I have a feeling that I have gained weight again. | 0.846 | |||
| 9. During meals I feel stress about how it will influence my body. | 0.810 | |||
| 4. After each meal, even a small one, I have the feeling that I have gained weight. | 0.797 | |||
| 19. I’m afraid to step on the scale because it could turn out that my weight has changed. | 0.748 | |||
| 1. Sometimes when it seems to me that I have gained weight, I feel negative tension and overwhelming sadness. | 0.737 | |||
| 8. Sometimes it feels like I’m getting fat just from breathing. | 0.700 | |||
| 3. Sometimes when it seems to me that I have lost weight, I feel that I am losing the joy of life. | 0.900 | 26.13%/0.900 | ||
| 16. I avoid weighing myself because it makes me afraid that I have lost weight. | 0.837 | |||
| 5. When I see that my body weight has dropped a little, I feel anxious. | 0.833 | |||
| 6. I have the feeling that my body is like a skeleton and is not attractive. | 0.767 | |||
| 17. Generally, I avoid looking in the mirror so that it does not turn out that I have lost weight. | 0.738 | |||
| 15. It happens that I force myself to eat to not lose the weight. | 0.727 | |||
| 14. I’m afraid of having meals with others and their comments that I don’t eat anything and I’m skinny. | 0.720 | |||
| 13. There are days when looking at my body in the mirror I have the impression that I lost weight again. | 0.631 | |||
| 2. I am afraid that in the future I will lose weight and I cannot do anything about it. | 0.630 | |||
| 10. I overeat and I can’t control it, otherwise I’m afraid that I will lose weight. | 0.546 | |||
| AGF | ALW | |||
|---|---|---|---|---|
| When Was the Last Time You Weighed Yourself? | M | SD | M | SD |
| More than year ago | 34.00 | 12.63 | 12.00 | 1.69 |
| During the last six months | 24.46 | 14.20 | 16.46 | 8.99 |
| In the last two weeks | 28.53 | 16.24 | 15.87 | 7.02 |
| In the last month | 32.00 | 16.56 | 20.64 | 15.8 |
| In the last week | 29.22 | 16.27 | 17.43 | 10.2 |
| AGF | ALW | |||
|---|---|---|---|---|
| Have You Ever Been on a Diet for Weight Loss? | M | SD | M | SD |
| No | 24.64 | 15.11 | 18.61 | 14.17 |
| Yes, in the last month | 39.00 | 16.60 | 15.57 | 6.47 |
| Yes, in the last six months | 35.00 | 17.40 | 14.00 | 7.56 |
| Yes, over the past year | 17.00 | 3.58 | 13.67 | 4.93 |
| Yes, but I don’t remember when | 31.33 | 13.04 | 19.00 | 9.54 |
| AGF | ALW | |
|---|---|---|
| AGE | 0.00 | 0.09 |
| BMI | 0.25 *** | −0.03 |
| PSS-10 | 0.41 *** | 0.11 |
| HADS_Depression | 0.26 ** | 0.24 ** |
| HADS_Anxiety | 0.50 *** | 0.12 |
| SUPPS_ERA | 0.44 *** | 0.07 |
| SUPPS_LC | 0.27 ** | 0.03 |
| SUPPS_SS | −0.06 | −0.08 |
| SPSRQ_P | 0.37 *** | 0.06 |
| SPSRQ_R | 0.11 | 0.06 |
| NEO FFI_N | 0.42 *** | 0.05 |
| NEO FFI_E | −0.05 | −0.25 *** |
| NEO FFI_O | 0.11 | −0.07 ** |
| NEO FFI_A | 0.05 | −0.20 * |
| NEO FFI_C | −0.22 ** | −0.12 * |
| NAS-50_IP | −0.16 | 0.03 |
| NAS-50_PC | 0.00 | −0.11 |
| NAS-50_SF | −0.16 | −0.26 *** |
| NAS-50_IA | −0.40 *** | 0.04 ** |
| NAS-50_GM | −0.20 * | 0.02 |
| BES_PA | −0.35 *** | −0.11 |
| BES_UBS | −0.46 *** | −0.24 |
| BES_PC | −0.54 *** | 0.04 *** |
| BES_SA | −0.34 *** | −0.14 |
| BES_WC | −0.60 *** | 0.06 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Styk, W.; Wojtowicz, E.; Zmorzynski, S. I Don’t Want to Be Thin! Fear of Weight Change Is Not Just a Fear of Obesity: Research on the Body Mass Anxiety Scale. Int. J. Environ. Res. Public Health 2023, 20, 2888. https://doi.org/10.3390/ijerph20042888
Styk W, Wojtowicz E, Zmorzynski S. I Don’t Want to Be Thin! Fear of Weight Change Is Not Just a Fear of Obesity: Research on the Body Mass Anxiety Scale. International Journal of Environmental Research and Public Health. 2023; 20(4):2888. https://doi.org/10.3390/ijerph20042888
Chicago/Turabian StyleStyk, Wojciech, Ewa Wojtowicz, and Szymon Zmorzynski. 2023. "I Don’t Want to Be Thin! Fear of Weight Change Is Not Just a Fear of Obesity: Research on the Body Mass Anxiety Scale" International Journal of Environmental Research and Public Health 20, no. 4: 2888. https://doi.org/10.3390/ijerph20042888
APA StyleStyk, W., Wojtowicz, E., & Zmorzynski, S. (2023). I Don’t Want to Be Thin! Fear of Weight Change Is Not Just a Fear of Obesity: Research on the Body Mass Anxiety Scale. International Journal of Environmental Research and Public Health, 20(4), 2888. https://doi.org/10.3390/ijerph20042888