2. Materials and Methods
The analysis covered 7689 incidents of violence from 2015–2020 taking place in the area subordinate to the Provincial Police Headquarters in Poznań. The study was based on anonymized documentation of forensic medical examinations performed at the Department of Forensic Medicine in Poznań at the request of the Police and private (80.3% and 19.7% of all tests performed, respectively). Descriptive statistics were carried out in the following categories: number of incidents per year and per commissioning entity, victim’s exposure to the health damage, the use of medical help, victim’s age and sex, incident location, type of injury, body location of the injury, method of impact, offender-victim ratio, the profession of the victim, gender of the perpetrator, and additional remarks.
Additional remarks include information the authors found interesting and important for future studies that were not matched to the main categories, such as incidents committed by more than one perpetrator, juvenile perpetrators, pregnant victims, or victims’ ethnicity.
The results are presented as a percentage.
Descriptive statistics were used: mean, median, standard deviation (SD), first and third-quartile values (IQR), and range.
The significance level was p = 0.05, but results relevant to the levels p = 0.01 and p = 0.001 were also indicated. Any p-values that showed statistically significant results were highlighted in bold. For p < 0.0001, the notation p < 0.001 has always been used.
All calculations and graphs were made using the statistical package R v. 4.0.2.
3. Results
Based on the obtained data from the victims during the obduction, 8893 perpetrators were recorded, of which men accounted for the vast majority (84.3%). Unknown perpetrators were the most common (40.0%). Following the analysis, 7689 victims were registered, representing men (59.5%) and women (40.4%). The age of the examined persons was between 1 and 94, with an average age of about 37 and a median of 35. The highest incidents were recorded in public places (52.9%). Physical workers and students were the most commonly exposed to violent actions. The most significant number of injuries were caused by fist strikes (26.9%). The types of injuries in the majority were bruises and contusions (45.1%), with the most prevalent injury site being the head and neck area (30.6%).
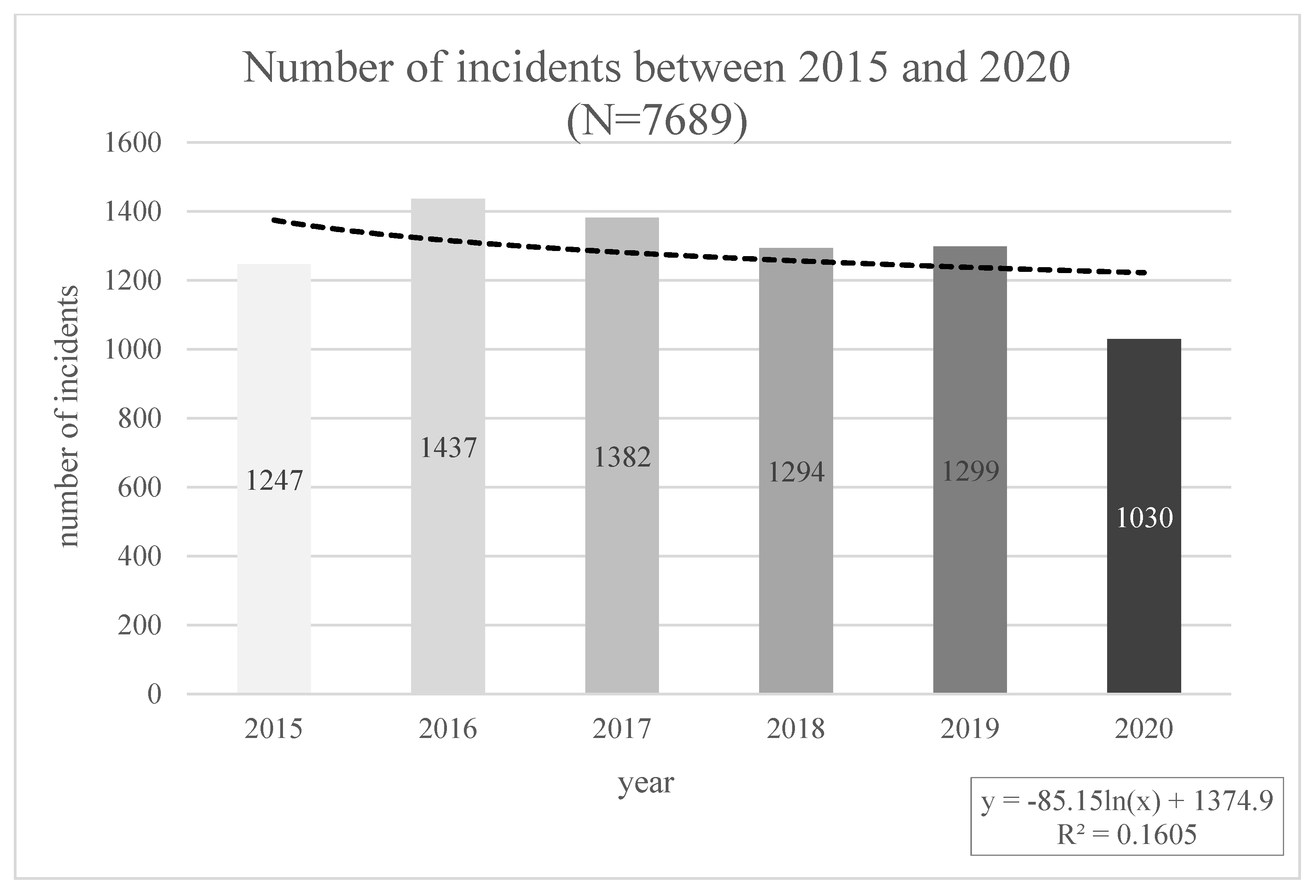
The frequency of recorded incidents between 2015 and 2020 is presented in
Figure 1. The highest number of forensic examinations was conducted in 2016. (
n = 1437) and the fewest in 2020 (
n = 1030). The reason for the low number of examinations conducted in 2020 might result from the start of the COVID-19 pandemic, the restrictions and limitations introduced, and thus the lower frequency of reporting by victims of incidents, as well as reducing the activities of Forensic Medicine Department in Poznan and the related cessation of examinations from March 22 to May 15. Disregarding the exceptional year 2020, due to the events mentioned above, the number of incidents oscillates at a similar level during the period under review.
The most significant number of examinations were performed based on private orders (
n = 1516; 19.7%) and orders from Police Commissariats located in the city of Poznań, i.e., Grunwald (
n = 943; 12.3%), New Town (
n = 831; 10.8%) and Old Town (
n = 792; 10.3%). The smallest number of orders came from the Konin City Police Station and the Czerniejewo Police Station (
Table 1).
Moreover, out of the forensic examination, 6607 (85.9%) failed to comply with the criteria for violating bodily functions or health disorders lasting more than seven days (
Table 2). In 23 cases, it was impossible to determine this parameter, which may have resulted, for example, from the victim’s failure to appear for a reassessment of injuries, despite recommendations.
A total of 4371 cases (56.8%) involved visits to the ED/Emergency Room or the arrival of the Emergency Medical Service (EMS) (
Table 3).
However, the injured required hospitalization in only 4% of the analyzed cases. Hospitalization requires admitting the injured person to a hospital ward and performing surgical procedures due to the injuries suffered.
The injuries were sustained by both men (59.5%) and women (40.4%), and in only two cases was it impossible to determine the sex (
Table 4).
The victims’ mean age was approximately 37 years and the median 35 years, with a range of participants from 1 to 94 years old (
Table 5).
Frequently, incidents occurred in public places (52.9%), further in private areas (39.1%), and the fewest events were recorded at the workplace (8.0%). Public places refer to stairwells, allotments, gates, parking lots, schools, stores, and other areas of public use (
Table 6).
Furthermore, amid all recorded injury types (
n = 12,505), the most common injuries found in reporting victims of violence were mild injuries in the form of bruises and contusions (
n = 5641; 45.1%), surface abrasions, redness, and discoloration (
n = 3675; 29.4%) (
Table 7).
Additional observed injury types occurring at a rate of less than 1% were joint sprains and twists, concussions, muscle and tendon injuries, thermal burns, lacerates, stab and gunshot wounds, hair loss, amputations, ear injuries, internal injuries, chemical injuries, eye injuries, and frostbite. No injuries were reported in 646 cases.
Of the total injury sites (
n = 15,537), the head and neck (
n = 4759; 30.6%) and upper limb were the most affected: forearm and hand injuries accounted for 17.0%, and injuries in the arm and shoulder girdle were 16.0% (
Table 8). Less frequent injuries were observed in the case of lower limbs, as lower leg and foot injuries accounted for 9.9% while the thigh and hip joints for 9.0%.
In 641 cases, no visible injuries were reported. The fewest reported injuries were in the genital region (n = 16; 0.1%) and internal injuries (n = 2; 0.01%).
Table 9 summarizes the perpetrator’s methods of inflicting injuries, with frequencies recorded at a total of 13,171. Most commonly, the perpetrator was punched with a fist (
n = 3543; 26.9%) and jerked and pushed and used a firm grip or twisted and dragged by the hair (
n = 3248; 24.7%).
The objects most often used to cause injury were complex and blunt-edged objects (n = 1050); next sharp-edged things such as a knife or axe (n = 170), and a minor percentage were the use of leather belts, cables, and rope (n = 24) or firearms (n = 12).
Table 10 shows data on the perpetrator’s relationship with the victim. However, in as many as 40.0% of cases, the perpetrator was unknown to the victim, and in 32.0% of the perpetrator was known to the victim, the relationship was not specified. In addition, a high incidence of violence perpetrated against victims by a spouse (10.0% of perpetrators) or current partner (4.2%) was observed.
In a small percentage of no more than 1%, injuries were caused by an animal, a parent’s partner, medical personnel, or workplace equipment.
The professional profile of victims reporting for medical examinations was also analyzed. Data are shown in
Figure 2. Regarding the 5609 occupations reported (unknown occupations were not included), the most significant proportion were physical workers (19.3%) and students (19%). Subsequently, office workers had the highest number of injuries, accounting for 16.7% of victims. The unemployed were victims in 8.8% of the discussed cases.
In analyzing the documents from the examinations, additional criteria were taken into account, such as the involvement of more than one perpetrator, offenses under Article 217 of the penal code, unconsciousness of the victim, the action of a minor perpetrator, the origin of the victim other than Polish (division into post-Soviet, EU, non-EU and post-Soviet countries) as well as self-harm and pregnant victims. In as many as 1204 events, two or more perpetrators committed acts of violence.
The victims included 207 people of non-Polish origin, of whom 128 were from post-Soviet countries (e.g., Ukraine, Belarus) and 43 from countries belonging to the European Union. In 28 cases, the injuries were self-inflicted. All of the additional observations are summarized in
Figure 3.
As reported by the victims, the perpetrators were most often men (84.3%), and only 9.6% of the noted cases were women (
Figure 4).
_Chan.jpg)

 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}