
Factors Associated with Suicidal Ideation and Suicide Attempt in Brazilian Transgender Youth
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
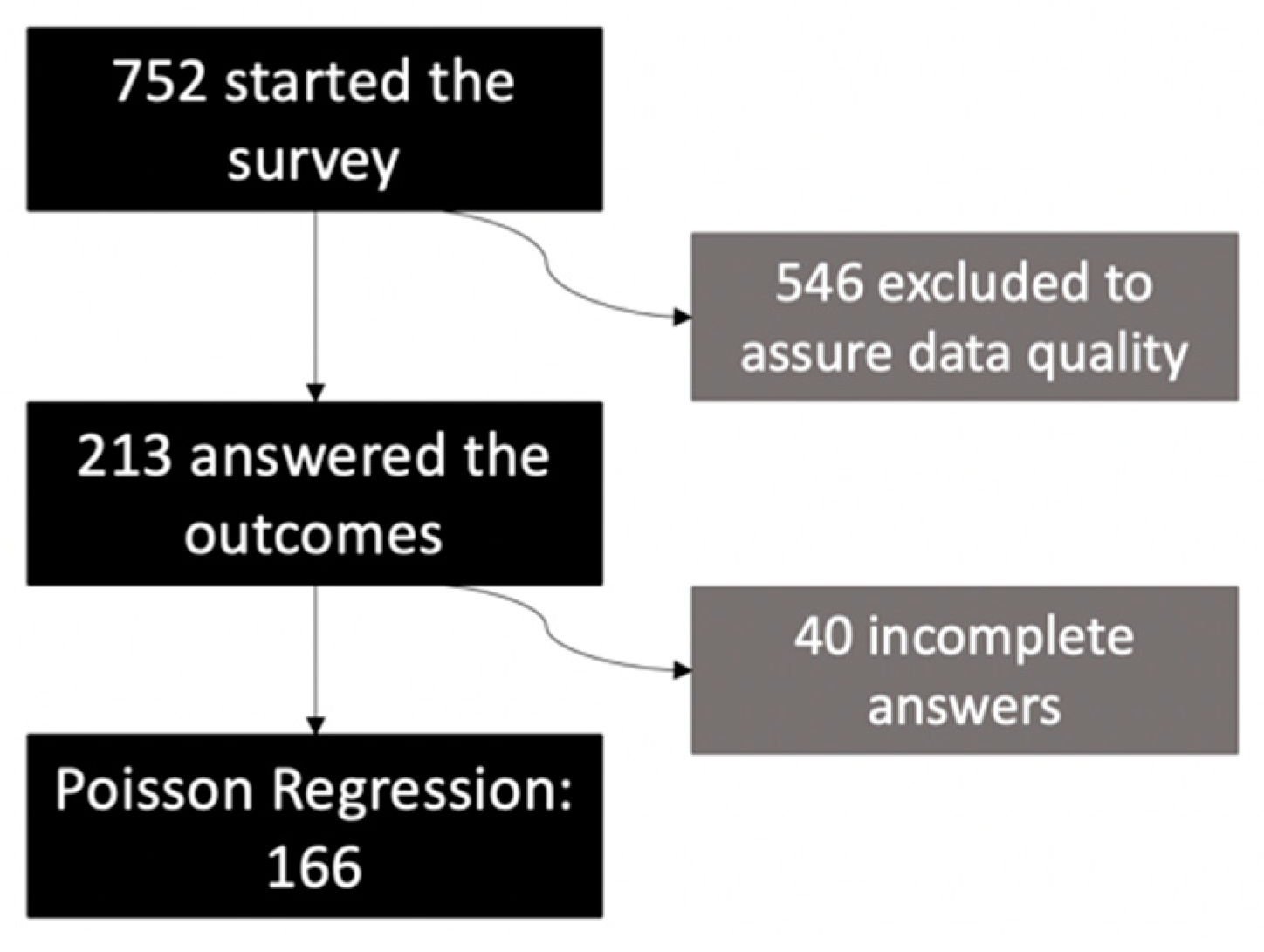
2.1. Study Sample
2.2. Measures
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giblon, R.; Bauer, G.R. Health care availability, quality, and unmet need: A comparison of transgender and cisgender residents of Ontario, Canada. BMC Health Serv. Res. 2017, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bass, M.; Gonzalez, L.J.; Colip, L.; Sharon, N.; Conklin, J. Rethinking gender: The nonbinary approach. Am. J. Health Syst. Pharm. 2018, 75, 709–711. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Fact Sheets. Suicide. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 2 November 2022).
- World Health Organization. Suicide Rates. Available online: https://www.who.int/data/gho/data/themes/mental-health/suicide-rates (accessed on 2 November 2022).
- Clark, T.C.; Lucassen, M.F.; Bullen, P.; Denny, S.J.; Fleming, T.M.; Robinson, E.M.; Rossen, F.V. The health and well-being of transgender high school students: Results from the New Zealand adolescent health survey (Youth’12). J. Adolesc. Health 2014, 55, 93–99. [Google Scholar] [CrossRef]
- Johns, M.M.; Lowry, R.; Andrzejewski, J.; Barrios, L.C.; Demissie, Z.; McManus, T.; Caponnetto, M.; Underwood, J.M. Transgender identity and experiences of violence victimization, substance use, suicide risk, and sexual risk behaviors among high school students—19 states and large urban school districts, 2017. Morb. Mortal. Wkly. Rep. 2019, 68, 67. [Google Scholar] [CrossRef] [PubMed]
- Surace, T.; Fusar-Poli, L.; Vozza, L.; Cavone, V.; Arcidiacono, C.; Mammano, R.; Basile, L.; Rodolico, A.; Bisicchia, P.; Caponnetto, P.; et al. Lifetime prevalence of suicidal ideation and suicidal behaviors in gender non-conforming youths: A meta-analysis. Eur. Child. Adolesc. Psychiatry 2021, 30, 1147–1161. [Google Scholar] [CrossRef]
- Chen, R.; Zhu, X.; Wright, L.; Drescher, J.; Gao, Y.; Wu, L.; Ying, X.; Qi, J.; Chen, C.; Xi, Y.; et al. Suicidal ideation and attempted suicide amongst Chinese transgender persons: National population study. J. Affect. Disord. 2019, 245, 1126–1134. [Google Scholar] [CrossRef]
- Kingsbury, M.; Hammond, N.G.; Johnstone, F.; Colman, I. Suicidality among sexual minority and transgender adolescents: A nationally representative population-based study of youth in Canada. CMAJ 2022, 194, E767–E774. [Google Scholar] [CrossRef]
- Chinazzo, I.R.; Lobato, M.I.R.; Nardi, H.C.; Koller, S.H.; Saadeh, A.; Costa, A.B. Impact of minority stress in depressive symptoms, suicide idea and suicide attempt in trans people. Cien. Saude Colet. 2020, 26 (Suppl. 3), 5045–5056. [Google Scholar] [CrossRef]
- Corrêa, F.H.M.; Rodrigues, B.B.; Mendonça, J.C.; Cruz, L.R.D. Pensamento suicida entre a população transgênero: Um estudo epidemiológico. J. Bras. Psiquiatr. 2020, 69, 13–22. [Google Scholar] [CrossRef]
- Silva, G.W.D.S.; Meira, K.C.; Azevedo, D.M.D.; Sena, R.C.F.D.; Lins, S.L.D.F.; Dantas, E.S.O.; Miranda, F.A.N.D. Fatores associados à ideação suicida entre travestis e transexuais assistidas por organizações não governamentais. Cien. Saude Colet. 2021, 26, 4955–4966. [Google Scholar] [CrossRef]
- Transgender Europe. TMM Update-Trans Day of Remembrance 2022. Available online: https://transrespect.org/en/tmm-update-tdor-2022/ (accessed on 15 January 2023).
- Acontece Arte e Política LGBTI+; ANTRA (Associação Nacional de Travestis e Transexuais); ABGLT (Associação Brasileira de Lésbicas, Gays, Bissexuais, Travestis, Transexuais e Intersexos). Mortes e violências contra LGBTI+ No Brasil: Dossiê 2021. Acontece, ANTRA, ABGLT: Florianópolis, SC, Brazil, 2022. Available online: https://observatoriomorteseviolenciaslgbtibrasil.org/ (accessed on 15 January 2023).
- Observatório Trans. Available online: https://observatoriotrans.org/educa-trans (accessed on 15 January 2023).
- Conselho Nacional de Combate à Discriminação. Brasil Sem Homofobia: Programa de Combate à Violência e à Discriminação Contra GLTB e Promoção da Cidadania Homossexual; Ministério da Saúde: Brasília, Brazil, 2004. [Google Scholar]
- BRASIL. Ministério da Saúde. Portaria n. 1.707, de 18 de Agosto de 2008, Institui, No Âmbito do Sistema Único de Saúde (SUS), o Processo Transexualizador, a ser Implantado nas Unidades Federadas, Respeitadas as Competências das três Esferas de Gestão. Available online: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2008/prt1707_18_08_2008.html (accessed on 15 January 2023).
- BRASIL. Ministério da Saúde. Redefine e Amplia o Processo Transexualizador No Sistema Único de Saúde (SUS). Portaria n. 2.803, de 19 de Novembro de 2013. Available online: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2013/prt2803_19_11_2013.html (accessed on 15 January 2023).
- CONSELHO FEDERAL DE MEDICINA. Resolução n. 2.265, de 20 de Setembro de 2019, Dispõe Sobre o Cuidado Específico à Pessoa com Incongruência de Gênero ou Transgênero. Available online: https://sistemas.cfm.org.br/normas/visualizar/resolucoes/BR/2019/2265 (accessed on 15 January 2023).
- CONSELHO NACIONAL DE JUSTIÇA. Provimento n. 73, de 28 de Junho de 2018, Dispõe Sobre a Averbação da Alteração do Prenome e do Gênero nos Assentos de Nascimento e Casamento de Pessoa Transgênero no Registro Civil das Pessoas Naturais (RCPN). Available online: https://atos.cnj.jus.br/atos/detalhar/2623 (accessed on 15 January 2023).
- Costa, A.B.; Filho, H.T.D.R.; Pase, P.F.; Fontanari, A.M.V.; Catelan, R.F.; Mueller, A.; Cardoso, D.; Soll, B.; Schwarz, K.; Schneider, M.A.; et al. Healthcare needs of and access barriers for Brazilian transgender and gender diverse people. J. Immigr. Minor. Health 2018, 20, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Rocon, P.C.; Sodré, F.; Rodrigues, A.; Barros, M.E.B.D.; Wandekoken, K.D. Desafios enfrentados por pessoas trans para acessar o processo transexualizador do Sistema Único de Saúde. Interface-Comun. Saúde Educ. 2019, 23. [Google Scholar] [CrossRef]
- Hendricks, M.L.; Testa, R.J. A conceptual framework for clinical work with transgender and gender nonconforming clients: An adaptation of the Minority Stress Model. Prof. Psychol. Res. Pract. 2012, 43, 460. [Google Scholar] [CrossRef]
- Meyer, I.H. Minority stress and mental health in gay men. J. Health Soc. Behav. 1995, 36, 38–56. [Google Scholar] [CrossRef]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2003, 129, 674. [Google Scholar] [CrossRef]
- Meyer, I.H. Resilience in the study of minority stress and health of sexual and gender minorities. Psychol. Sex Orientat. Gend. Divers. 2015, 2, 209. [Google Scholar] [CrossRef]
- Joiner, T.E., Jr.; Van Orden, K.A. The interpersonal-psychological theory of suicidal behavior indicates specific and crucial psychotherapeutic targets. Int. J. Cogn. Ther. 2008, 1, 80–89. [Google Scholar] [CrossRef]
- Testa, R.J.; Michaels, M.S.; Bliss, W.; Rogers, M.L.; Balsam, K.F.; Joiner, T. Suicidal ideation in transgender people: Gender minority stress and interpersonal theory factors. J. Abnorm. Psychol. 2017, 126, 125. [Google Scholar] [CrossRef]
- Phillip, A.; Pellechi, A.; DeSilva, R.; Semler, K.; Makani, R. A plausible explanation of increased suicidal behaviors among transgender youth based on the interpersonal theory of suicide (IPTS): Case series and literature review. J. Psychiatr. Pract. 2022, 28, 3–13. [Google Scholar] [CrossRef]
- Austin, A.; Craig, S.L.; D’Souza, S.; McInroy, L.B. Suicidality among transgender youth: Elucidating the role of interpersonal risk factors. J. Interpers. Violence 2022, 37, NP2696–NP2718. [Google Scholar] [CrossRef]
- Bauer, G.R.; Braimoh, J.; Scheim, A.I.; Dharma, C. Transgender-inclusive measures of sex/gender for population surveys: Mixed-methods evaluation and recommendations. PLoS ONE 2017, 12, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Sausa, L.A.; Sevelius, J.; Keatley, J.; Iñiguez, J.R.; Reyes, M. Recommendations for Inclusive Data Collection of Trans People in HIV Prevention, Care & Services; Center of Excellence for Transgender HIV Prevention: San Francisco, CA, USA, 2009; Available online: https://prevention.ucsf.edu/transhealth/education/data-recs-long (accessed on 20 October 2022).
- Borsa, J.C.; Damásio, B.F.; Bandeira, D.R. Cross-cultural adaptation and validation of psychological instruments: Some considerations. Paidéia 2012, 22, 423–432. [Google Scholar] [CrossRef]
- Fontanari, A.M.V.; Pase, P.F.; Churchill, S.; Soll, B.; Schwarz, K.; Schneider, M.A. Dealing with gender-related and general stress: Substance use among Brazilian transgender youth. Addict. Behav. Rep. 2019, 9, 100166. [Google Scholar] [CrossRef]
- Dunn, E.C.; Avenue, H.; Green, J.G. The Modified Depression Scale (MDS): A brief, no-cost assessment tool to estimate the level of depressive symptoms in students and schools. School Ment. Health 2012, 4, 34–45. [Google Scholar] [CrossRef]
- Scheim, A.I.; Bauer, G.R. The Intersectional Discrimination Index: Development and validation of measures of self-reported enacted and anticipated discrimination for intercategorical analysis. Soc. Sci. Med. 2019, 226, 225–235. [Google Scholar] [CrossRef]
- Griep, R.H.; Chor, D.; Faerstein, E.; Werneck, G.L.; Lopes, C.S. Validade de constructo de escala de apoio social do Medical Outcomes Study adaptada para o português no Estudo Pró-Saúde. Cad. Saude Publica 2005, 21, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Gotovac, S.; Bauer, G.R.; for the Trans Youth CAN! Research Team. Development and Validation of Gender Distress and Gender Positivity Measures for Transgender Youth. Oral Presentation Given at CANADIAN Psychological Association Convention. 17 June 2021. Online Conference. Available online: https://transyouthcan.ca/results/ (accessed on 15 January 2023).
- Saewyc, E.M.; Gotovac, S.; Villalobos, M.C.; Scheim, A.; Vandermorris, A.; Bauer, G. Development and Validation of new Gender Distress and Gender Positivity Scales for Young Transgender Adolescents in Canada. J. Adolesc. Health 2022, 70, S10. [Google Scholar] [CrossRef]
- Garthe, R.C.; Blackburn, A.M.; Kaur, A.; Sarol Jr, J.N.; Goffnett, J.; Rieger, A.; Deutsch, A.; Smith, D.C. Suicidal Ideation Among Transgender and Gender Expansive Youth: Mechanisms of Risk. Transgender Health 2022, 7, 416–422. [Google Scholar] [CrossRef]
- Perez-Brumer, A.; Day, J.K.; Russell, S.T.; Hatzenbuehler, M.L. Prevalence and correlates of suicidal ideation among transgender youth in California: Findings from a representative, population-based sample of high school students. J. Am. Acad. Child. Adolesc. Psychiatry 2017, 56, 739–746. [Google Scholar] [CrossRef]
- Johnson, K.C.; LeBlanc, A.J.; Deardorff, J.; Bockting, W.O. Invalidation experiences among non-binary adolescents. J. Sex Res. 2020, 57, 222–233. [Google Scholar] [CrossRef]
- Conlin, S.E.; Douglass, R.P.; Larson-Konar, D.M.; Gluck, M.S.; Fiume, C.; Heesacker, M. Exploring nonbinary gender identities: A qualitative content analysis. J. LGBT Issues Couns. 2019, 13, 114–133. [Google Scholar] [CrossRef]
- Taylor, A.K.; Condry, H.; Cahill, D. Implementation of teaching on LGBT health care. Clin. Teach. 2018, 15, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Scandurra, C.; Carbone, A.; Baiocco, R.; Mezzalira, S.; Maldonato, N.M.; Bochicchio, V. Gender identity milestones, minority stress and mental health in three generational cohorts of Italian binary and nonbinary transgender people. Int. J. Environ. Res. Public Health 2021, 18, 9057. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM 5; Artmed: Porto Alegre, Brazil, 2014. [Google Scholar]
- Lindley, L.; Galupo, M.P. Gender dysphoria and minority stress: Support for inclusion of gender dysphoria as a proximal stressor. Psychol. Sex Orientat. Gend. Divers. 2020, 7, 265. [Google Scholar] [CrossRef]
- de Vries, A.L.; Cohen-Kettenis, P.T. Clinical management of gender dysphoria in children and adolescents: The Dutch approach. J. Homosex 2012, 59, 301–320. [Google Scholar] [CrossRef] [PubMed]
- Coleman, E.; Radix, A.E.; Bouman, W.P.; Brown, G.R.; de Vries, A.L.C.; Deutsch, M.B.; Ettner, R.; Fraser, L.; Goodman, M.; Green, J.; et al. Standards of care for the health of transgender and gender diverse people, version 8. Int. J. Transgender Health 2022, 23 (Suppl. 1), S1–S259. [Google Scholar] [CrossRef] [PubMed]
- Fontanari, A.M.V.; Vilanova, F.; Schneider, M.A.; Chinazzo, I.; Soll, B.M.; Schwarz, K.; Lobato, M.I.R.; Costa, A.B. Gender affirmation is associated with transgender and gender nonbinary youth mental health improvement. LGBT Health 2020, 7, 237–247. [Google Scholar] [CrossRef]
- Hembree, W.C.; Cohen-Kettenis, P.T.; Gooren, L.; Zhong, S.; Zhao, L. Endocrine treatment of gender-dysphoric/genderincongruent persons: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2017, 102, 3869–3903. [Google Scholar] [CrossRef]
- Mezzalira, S.; Scandurra, C.; Mezza, F.; Miscioscia, M.; Innamorati, M.; Bochicchio, V. Gender Felt Pressure, Affective Domains, and Mental Health Outcomes among Transgender and Gender Diverse (TGD) Children and Adolescents: A Systematic Review with Developmental and Clinical Implications. Int. J. Environ. Res. Public Health 2023, 20, 785. [Google Scholar] [CrossRef]
- Klein, A.; Golub, S.A. Family rejection as a predictor of suicide attempts and substance misuse among transgender and gender nonconforming adults. LGBT Health 2016, 3, 193–199. [Google Scholar] [CrossRef]
- Pariseau, E.M.; Chevalier, L.; Long, K.A.; Clapham, R.; Edwards-Leeper, L.; Tishelman, A.C. The relationship between family acceptance-rejection and transgender youth psychosocial functioning. Clin. Pract. Pediatr. Psychol. 2019, 7, 267. [Google Scholar] [CrossRef]
- Peng, K.; Zhu, X.; Gillespie, A.; Wang, Y.; Gao, Y.; Xin, Y.; Qi, J.; Ou, J. Self-reported Rates of Abuse, Neglect, and Bullying Experienced by Transgender and Gender-Nonbinary Adolescents in China. JAMA Netw. Open. 2019, 2, e1911058. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Trans Men | Trans Women | Non-Binary | χ2 | df | p | Total | |
|---|---|---|---|---|---|---|---|
| Live in | |||||||
| Capital | 77 (77.8%) | 39 (88.6%) | 51 (79.7%) | 3.193 | 4 | 0.526 | 167 (80.7%) |
| Metropolitan region | 18 (18.2%) | 4 (9.1%) | 12 (18.8%) | 34 (16.4%) | |||
| Countryside | 4 (4.0%) | 1 (2.3%) | 1 (1.6%) | 6 (2.9%) | |||
| Brazil Region | |||||||
| Southeast | 45 (46.4%) | 19 (44.2%) | 31 (50.8%) | 2.939 | 8 | 0.938 | 95 (47.3%) |
| South | 32 (33.0%) | 11 (25.6%) | 17 (27.9%) | 60 (29.9%) | |||
| Other | 20 (20.7%) | 13 (30.3%) | 13 (21.4%) | 46 (22.9%) | |||
| School | |||||||
| Public school | 50 (48.5%) | 22 (50.0%) | 28 (43.1%) | 2.549 | 6 | 0.863 | 100 (47.2%) |
| Private school | 17 (16.5%) | 8 (18.2%) | 8 (12.3%) | 33 (15.6%) | |||
| Homeschooled | 2 (1.9%) | 1 (2.3%) | 2 (3.1%) | 5 (2.4%) | |||
| Not studying | 34 (33.0%) | 13 (29.5%) | 27 (41.5%) | 74 (34.9%) |
| Trans Men | Trans Women | Non-Binary | χ2 | df | p | Total | |
|---|---|---|---|---|---|---|---|
| Suicidal Ideation | |||||||
| No | 26 (26.0%) | 16 (38.1%) | 14 (23.0%) | 3.104 | 2 | 0.212 | 56 (27.6%) |
| Yes | 74 (74.0%) | 26 (61.9%) | 57 (77.0%) | 147 (72.4%) | |||
| Suicidal Attempt | |||||||
| No | 56 (56.6%) | 26 (60.5%) | 35 (57.4%) | 0.189 | 2 | 0.910 | 117 (57.6%) |
| Yes | 43 (43.4%) | 17 (39.5%) | 26 (42.6%) | 86 (42.4%) | |||
| Depressive Symptoms | |||||||
| No | 37 (36.6%) | 23 (53.5%) | 29 (45.3%) | 3.741 | 2 | 0.154 | 89 (42.8%) |
| Yes | 64 (63.4%) | 20 (46.5%) | 35 (54.7%) | 119 (57.2%) |
| Trans Men | Trans Women | Non-Binary | F | p | Total | |
|---|---|---|---|---|---|---|
| Deprivation | 4.37 (0.69) | 4.10 (0.85) | 4.35 (0.69) | 2.256 | 0.107 | 4.31 (0.73) |
| Age | 18.16 (2.42) | 19.91 (2.81) | 18.17 (2.11) | 9.098 | 0.000 * | 18.52 (2.51) |
| Discrimination | 7.45 (1.87) | 7.79 (1.68) | 7.63 (1.86) | 0.521 | 0.595 | 7.58 (1.82) |
| Gender Distress | 3.98 (0.46) | 4.03 (0.53) | 3.57 (0.67) | 12.179 | 0.000 * | 3.88 (0.57) |
| Gender Positivity | 3.26 (0.54) | 3.40 (0.64) | 3.43 (0.65) | 1.709 | 0.184 | 3.34 (0.60) |
| Parents’ Support to GI | 2.43 (1.13) | 2.75 (1.31) | 2.40 (1.15) | 1.395 | 0.250 | 2.49 (1.18) |
| Friends’ Support to GI | 3.47 (0.53) | 3.41 (0.57) | 3.31 (0.61) | 1.498 | 0.226 | 3.41 (0.57) |
| Social Support | ||||||
| Affective | 11.31 (3.56) | 10.79 (4.58) | 10.52 (3.98) | 0.817 | 0.443 | 10.96 (3.92) |
| Positive Social Interaction | 13.98 (5.00) | 13.38 (5.49) | 12.63 (5.55) | 1.235 | 0.293 | 13.43 (5.28) |
| Emotional/Information | 26.56 (9.83) | 26.78 (10.26) | 26.22 (9.81) | 0.045 | 0.956 | 26.50 (9.87) |
| Material | 13.29 (4.51) | 12.90 (5.00) | 12.86 (4.69) | 0.196 | 0.822 | 13.07 (4.65) |
| Step 1 | Step 2 | Step 3 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p | Exp (B) | CI (95%) | p | Exp (B) | CI (95%) | p | Exp (B) | CI (95%) | ||||
| Deprivation | 0.00 * | 0.85 | 0.77 | 0.95 | 0.04 * | 0.90 | 0.81 | 1.00 | 0.05 * | 0.90 | 0.82 | 1.00 |
| Material Support | 0.15 | 0.99 | 0.97 | 1.01 | 0.77 | 1.00 | 0.98 | 1.02 | 0.25 | 1.01 | 0.99 | 1.03 |
| Discrimination | - | - | - | - | 0.02 * | 1.09 | 1.02 | 1.17 | 0.09 | 1.06 | 0.99 | 1.14 |
| Gender Distress | - | - | - | - | 0.01 * | 1.29 | 1.07 | 1.56 | 0.01 * | 1.27 | 1.06 | 1.52 |
| Gender Positivity | - | - | - | - | 0.03 * | 0.82 | 0.68 | 0.98 | 0.23 | 0.89 | 0.75 | 1.07 |
| Parents’ Support to Gender Identity | - | - | - | - | 0.39 | 0.96 | 0.88 | 1.05 | 0.37 | 0.96 | 0.88 | 1.05 |
| Depressive Symptoms | - | - | - | - | - | - | - | - | 0.00 * | 1.04 | 1.02 | 1.06 |
| Step 1 | Step 2 | Step 3 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p | Exp (B) | CI (95%) | p | Exp (B) | CI (95%) | p | Exp (B) | CI (95%) | ||||
| Deprivation | 0.01 * | 0.77 | 0.63 | 0.95 | 0.09 | 0.84 | 0.68 | 1.03 | 0.05 * | 0.81 | 0.67 | 1.00 |
| Material Support | 0.31 | 0.98 | 0.94 | 1.00 | 0.73 | 1.01 | 0.97 | 1.05 | 0.31 | 1.02 | 0.98 | 1.06 |
| Discrimination | - | - | - | - | 0.05 * | 1.17 | 0.99 | 1.37 | 0.07 | 1.14 | 0.99 | 1.31 |
| Gender Distress | - | - | - | - | 0.06 | 1.39 | 0.98 | 1.99 | 0.16 | 1.24 | 0.91 | 1.81 |
| Gender Positivity | - | - | - | - | 0.09 | 0.75 | 0.53 | 1.05 | 0.23 | 0.82 | 0.60 | 1.13 |
| Parents’ Support to Gender Identity | - | - | - | - | 0.49 | 0.95 | 0.81 | 1.11 | 0.67 | 0.97 | 0.83 | 1.13 |
| Depressive Symptoms | - | - | - | - | - | - | - | - | 0.01 * | 1.89 | 1.19 | 2.98 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chinazzo, Í.R.; Fontanari, A.M.V.; Costa, A.B.; Lobato, M.I.R. Factors Associated with Suicidal Ideation and Suicide Attempt in Brazilian Transgender Youth. Int. J. Environ. Res. Public Health 2023, 20, 3215. https://doi.org/10.3390/ijerph20043215
Chinazzo ÍR, Fontanari AMV, Costa AB, Lobato MIR. Factors Associated with Suicidal Ideation and Suicide Attempt in Brazilian Transgender Youth. International Journal of Environmental Research and Public Health. 2023; 20(4):3215. https://doi.org/10.3390/ijerph20043215
Chicago/Turabian StyleChinazzo, Ítala Raymundo, Anna Martha Vaitses Fontanari, Angelo Brandelli Costa, and Maria Inês Rodrigues Lobato. 2023. "Factors Associated with Suicidal Ideation and Suicide Attempt in Brazilian Transgender Youth" International Journal of Environmental Research and Public Health 20, no. 4: 3215. https://doi.org/10.3390/ijerph20043215