
Effect of Whole-Body Vibration Training on Hemorheological Blood Indices in Young, Healthy Women
 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
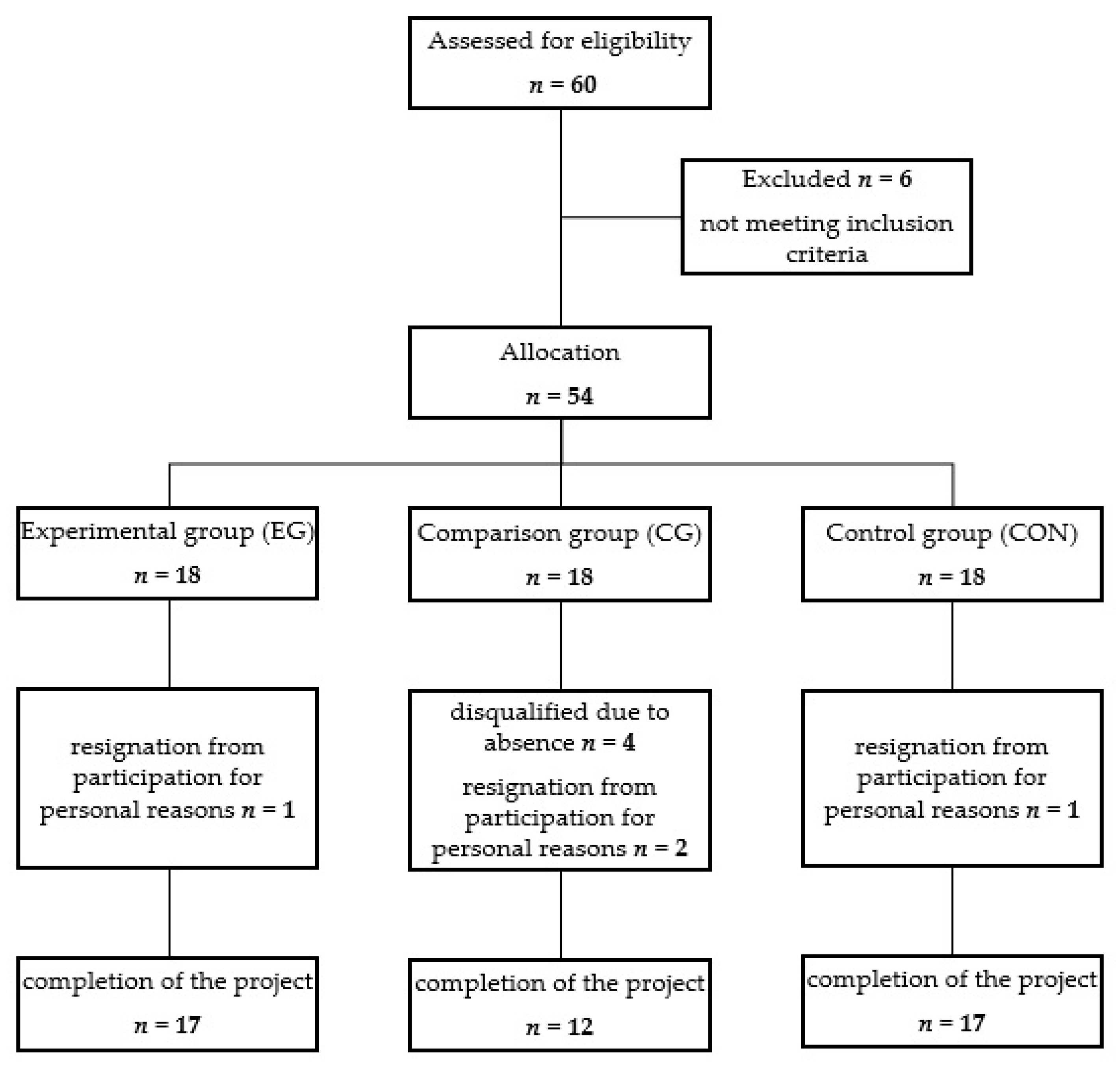
2.1. Participants
2.2. Study Protocol
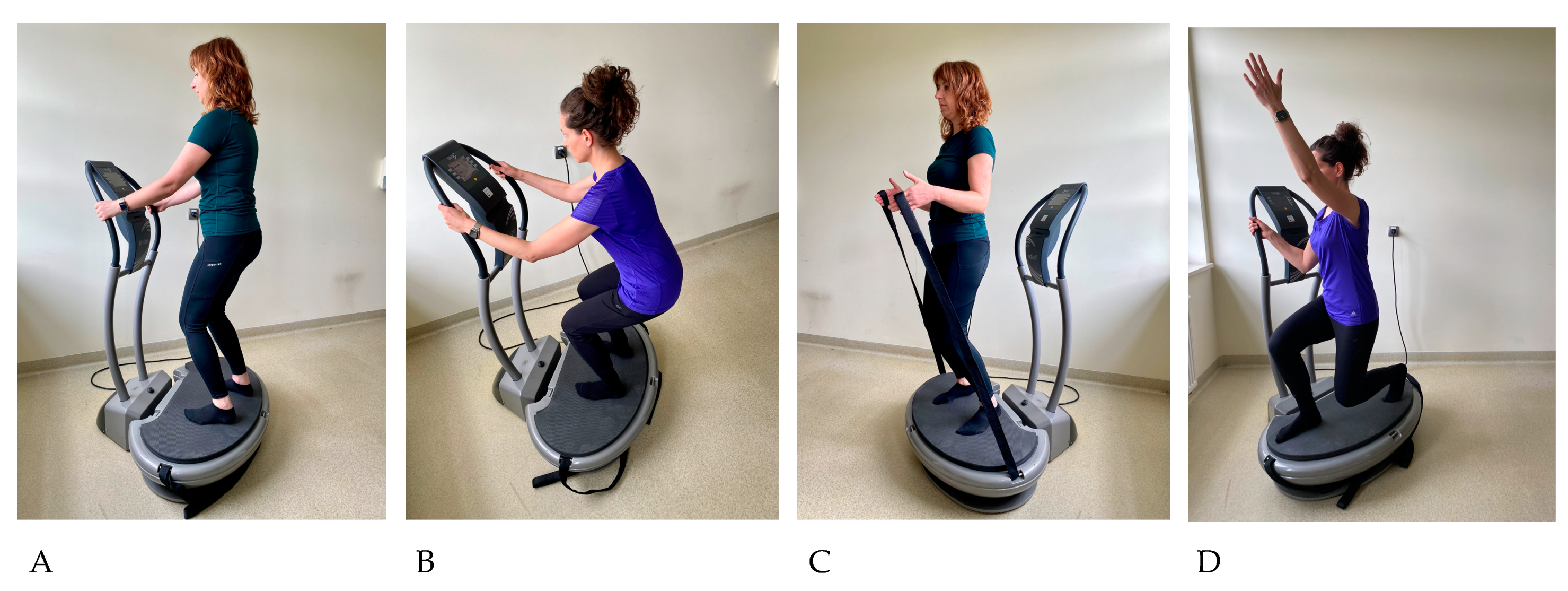
2.3. Exercises Program
2.4. Body Composition Analysis
2.5. Analysis of Nutrition and Assessment of the Level of Physical Activity
2.6. Blood Collection and Laboratory Indices
2.7. Statistical Analysis
3. Results
3.1. Subjects’ Characteristics
3.2. Short-Term Effects of Exercise
3.2.1. Hematological Indices
3.2.2. Elongation Index (EI)
3.2.3. Aggregation Indices and Fibrinogen Concentration
3.3. The Effects of a 12-Week Training Program
3.3.1. Hematological Indices
3.3.2. Elongation Index (EI)
3.3.3. Aggregation Indices and Fibrinogen Concentration
3.3.4. Changes in the Blood Plasma Volume (ΔPV)
4. Discussion
Study Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cochrane, D.J. Vibration Exercise: The Potential Benefits. Int. J. Sports Med. 2011, 32, 75–99. [Google Scholar] [CrossRef] [PubMed]
- Eklund, G.; Hagbarth, K.E. Normal Variability of Tonic Vibration Reflex in Man. Exp. Neurol. 1966, 16, 80–92. [Google Scholar] [CrossRef] [PubMed]
- Zaidell, L.N.; Mileva, K.N.; Sumners, D.P.; Bowtell, J.L. Experimental Evidence of the Tonic Vibration Reflex During Whole-Body Vibration of the Loaded and Unloaded Leg. PLoS ONE 2013, 8, e85247. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, M.; Bosco, C. The Use of Vibration as an Exercise Intervention. Exerc. Sport Sci. Rev. 2003, 31, 3–7. [Google Scholar] [CrossRef]
- Pérez-Turpin, J.A.; Zmijewski, P.; Jimenez-Olmedo, J.M.; Jové-Tossi, M.A.; Martínez-Carbonell, A.; Suárez-Llorca, C.; Andreu-Cabrera, E. Effects of Whole Body Vibration on Strength and Jumping Performance in Volleyball and Beach Volleyball Players. Biol. Sport 2014, 31, 239–245. [Google Scholar] [CrossRef]
- ElDeeb, A.M.; Abdel-Aziem, A.A. Effect of Whole-Body Vibration Exercise on Power Profile and Bone Mineral Density in Postmenopausal Women with Osteoporosis: A Randomized Controlled Trial. J. Manipulative Physiol. Ther. 2020, 43, 384–393. [Google Scholar] [CrossRef]
- Milanese, C.; Piscitelli, F.; Zenti, M.G.; Moghetti, P.; Sandri, M.; Zancanaro, C. Ten-Week Whole-Body Vibration Training Improves Body Composition and Muscle Strength in Obese Women. Int. J. Med. Sci. 2013, 10, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.K.; Feland, J.B.; Johnson, A.W.; Mack, G.W.; Mitchell, U.H. Effect of Whole Body Vibration on Skin Blood Flow and Nitric Oxide Production. J. Diabetes Sci. Technol. 2014, 8, 889–894. [Google Scholar] [CrossRef]
- Lythgo, N.; Eser, P.; de Groot, P.; Galea, M. Whole-Body Vibration Dosage Alters Leg Blood Flow. Clin. Physiol. Funct. Imaging 2009, 29, 53–59. [Google Scholar] [CrossRef]
- Huh, J.Y.; Mougios, V.; Skraparlis, A.; Kabasakalis, A.; Mantzoros, C.S. Irisin in Response to Acute and Chronic Whole-Body Vibration Exercise in Humans. Metabolism 2014, 63, 918–921. [Google Scholar] [CrossRef]
- Elmantaser, M.; McMillan, M.; Smith, K.; Khanna, S.; Chantler, D.; Panarelli, M.; Ahmed, S.F. A Comparison of the Effect of Two Types of Vibration Exercise on the Endocrine and Musculoskeletal System. J. Musculoskelet. Neuronal Interact. 2012, 12, 144–154. [Google Scholar]
- Szanto, S.; Mody, T.; Gyurcsik, Z.; Babjak, L.B.; Somogyi, V.; Barath, B.; Varga, A.; Matrai, A.A.; Nemeth, N. Alterations of Selected Hemorheological and Metabolic Parameters Induced by Physical Activity in Untrained Men and Sportsmen. Metabolites 2021, 11, 870. [Google Scholar] [CrossRef] [PubMed]
- Kenney, W.L.; Wilmore, J.H.; Costill, D.L. Cardiorespiratory Responses to Acute Exercises. In Physiology of Sport and Exercise, 8th ed.; Human Kinetics Inc.: Champaign, IL, USA, 2022; pp. 214–238. ISBN 9781718201736. [Google Scholar]
- Nemkov, T.; Skinner, S.C.; Nader, E.; Stefanoni, D.; Robert, M.; Cendali, F.; Stauffer, E.; Cibiel, A.; Boisson, C.; Connes, P.; et al. Acute Cycling Exercise Induces Changes in Red Blood Cell Deformability and Membrane Lipid Remodeling. Int. J. Mol. Sci. 2021, 22, 896. [Google Scholar] [CrossRef] [PubMed]
- Romagnoli, M.; Alis, R.; Martinez-Bello, V.; Sanchis-Gomar, F.; Aranda, R.; Gomez-Cabrera, M.C. Blood Rheology Effect of Submaximal Exercise on Young Subjects. Clin. Hemorheol. Microcirc. 2014, 56, 111–117. [Google Scholar] [CrossRef]
- Yalcin, O.; Erman, A.; Muratli, S.; Bor-Kucukatay, M.; Baskurt, O.K. Time Course of Hemorheological Alterations After Heavy Anaerobic Exercise in Untrained Human Subjects. J. Appl. Physiol. 2003, 94, 997–1002. [Google Scholar] [CrossRef]
- Kilic-Toprak, E.; Unver, F.; Kilic-Erkek, O.; Korkmaz, H.; Ozdemir, Y.; Oymak, B.; Oskay, A.; Bor-Kucukatay, M. Increased Erythrocyte Aggregation Following an Acute Bout of Eccentric Isokinetic Exercise Does Not Exceed Two Days. Biorheology 2018, 55, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Cakir-Atabek, H.; Atsak, P.; Gunduz, N.; Bor-Kucukatay, M. Effects of Resistance Training Intensity on Deformability and Aggregation of Red Blood Cells. Clin Hemorheol. Microcirc. 2009, 41, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Simmonds, M.J.; Connes, P.; Sabapathy, S. Exercise-Induced Blood Lactate Increase Does Not Change Red Blood Cell Deformability in Cyclists. PLoS ONE 2013, 8, e71219. [Google Scholar] [CrossRef]
- Nader, E.; Skinner, S.; Romana, M.; Fort, R.; Lemonne, N.; Guillot, N.; Gauthier, A.; Antoine-Jonville, S.; Renoux, C.; Hardy-Dessources, M.D.; et al. Blood Rheology: Key Parameters, Impact on Blood Flow, Role in Sickle Cell Disease and Effects of Exercise. Front. Physiol. 2019, 10, 1329. [Google Scholar] [CrossRef]
- Connes, P.; Simmonds, M.J.; Brun, J.F.; Baskurt, O.K. Exercise Hemorheology: Classical Data, Recent Findings and Unresolved Issues. Clin. Hemorheol. Microcirc. 2013, 53, 187–199. [Google Scholar] [CrossRef] [PubMed]
- Brun, J.F.; Varlet-Marie, E.; Connes, P.; Aloulou, I. Hemorheological Alterations Related to Training and Overtraining. Biorheology 2010, 47, 95–115. [Google Scholar] [CrossRef] [PubMed]
- Biernat, E.; Stupnicki, R.; Gajewski, A.K. Międzynarodowy Kwestionariusz Aktywności Fizycznej (IPAQ)—Wersja Polska. Wych. Fiz. i Sport 2007, 51, 47–54. [Google Scholar]
- Nuttall, F.Q. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr. Today 2015, 50, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Jarosz, M. Normy Żywienia dla Populacji Polski; Instytut Żywności i Żywienia: Warszawa, Poland, 2017; ISBN 9788386060894. [Google Scholar]
- Tomás, R.; Lee, V.; Going, S. The Use of Vibration Exercise in Clinical Populations. ACSMS Health Fit. J. 2011, 15, 25–31. [Google Scholar] [CrossRef]
- Albasini, A.; Krause, M.; Rembitzki, I. Indications and Contraindications in the Clinical Application of WBV: Immediate and Long-term Affects and Their Influence on the Selection of Dosage. In Using Whole Body Vibration in Physical Therapy and Sport: Clinical Practice and Treatment Exercises, 1st ed.; Churchill Livingstone Elsevier: Edinburgh, NY, USA, 2010; pp. 65–87. ISBN 9780702031731. [Google Scholar]
- Hardeman, M.R.; Dobbe, J.G.; Ince, C. The Laser-Assisted Optical Rotational Cell Analyzer (LORCA) as Red Blood Cell Aggregometer. Clin. Hemorheol. Microcirc. 2001, 25, 1–11. [Google Scholar]
- Dill, D.B.; Costill, D.L. Calculation of Percentage Changes in Volumes of Blood, Plasma and Red Cell in Dehydration. J. Appl. Physiol. 1974, 37, 247–248. [Google Scholar] [CrossRef]
- Harrison, M.H.; Graveney, M.J.; Cochrane, L.A. Some Sources of Error in the Calculation of Relative Change in Plasma Volume. Eur. J. Appl. Physiol. Occup. Physiol. 1982, 50, 13–21. [Google Scholar] [CrossRef]
- Games, K.E.; Sefton, J.M.; Wilson, A.E. Whole-Body Vibration and Blood Flow and Muscle Oxygenation: A Meta-Analysis. J. Athl. Train. 2015, 50, 542–549. [Google Scholar] [CrossRef]
- Sá-Caputo, D.; Paineiras-Domingos, L.; Carvalho-Lima, R.; Dias-Costa, G.; de Paiva, P.C.; de Azeredo, C.F.; Carmo, R.C.; Dionello, C.F.; Moreira-Marconi, E.; Frederico, É.H.; et al. Potential Effects of Whole-Body Vibration Exercises on Blood Flow Kinetics of Different Populations: A Systematic Review with a Suitable Approach. Afr. J. Tradit. Complement. Altern. Med. 2017, 14, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Kerschan-Schindl, K.; Grampp, S.; Henk, C.; Resch, H.; Preisinger, E.; Fialka-Moser, V.; Imhof, H. Whole-body Vibration Exercise Leads to Alterations in Muscle Blood Volume. Clin. Physiol. 2001, 21, 377–382. [Google Scholar] [CrossRef]
- Lai, C.L.; Chen, H.Y.; Tseng, S.Y.; Liao, W.C.; Liu, B.T.; Lee, M.C.; Chen, H.S. Effect of Whole-Body Vibration for 3 Months on Arterial Stiffness in the Middle-Aged and Elderly. Clin. Interv. Aging 2014, 9, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Sackner, M.A.; Gummels, E.; Adams, J.A. Nitric Oxide is Released into Circulation with Whole-Body, Periodic Acceleration. Chest 2005, 127, 30–39. [Google Scholar] [CrossRef]
- Brun, J.F.; Khaled, S.; Raynaud, E.; Bouix, D.; Micallef, J.P.; Orsetti, A. The Triphasic Effects of Exercise on Blood Rheology: Which Relevance to Physiology and Pathophysiology? Clin. Hemorheol. Microcirc. 1998, 19, 89–104. [Google Scholar] [PubMed]
- Ahmadizad, S.; El-Sayed, M.S. The Acute Effects of Resistance Exercise on the Main Determinants of Blood Rheology. J. Sports Sci. 2005, 23, 243–249. [Google Scholar] [CrossRef]
- Theodorou, A.A.; Gerodimos, V.; Karatrantou, K.; Paschalis, V.; Chanou, K.; Jamurtas, A.Z.; Nikolaidis, M.G. Acute and Chronic Whole-Body Vibration Exercise does not Induce Health-Promoting Effects on the Blood Profile. J. Hum. Kinet. 2015, 46, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Connes, P.; Bouix, D.; Py, G.; Prefaut, C.; Mercier, J.; Brun, J.F.; Caillaud, C. Opposite Effects of in Vitro Lactate on Erythrocyte Deformability in Athletes and Untrained Subjects. Clin. Hemorheol. Microcirc. 2004, 31, 11–18. [Google Scholar]
- Monnier, J.F.; Benhaddad, A.A.; Micallef, J.P.; Mercier, J.; Brun, J.F. Relationships Between Blood Viscosity and Insulin-Like Growth Factor I Status in Athletes. Clin. Hemorheol. Microcirc. 2000, 22, 277–286. [Google Scholar]
- Teległów, A.; Mardyła, M.; Myszka, M.; Pałka, T.; Maciejczyk, M.; Bujas, P.; Mucha, D.; Ptaszek, B.; Marchewka, J. Effect of Intermittent Hypoxic Training on Selected Biochemical Indicators, Blood Rheological Properties, and Metabolic Activity of Erythrocytes in Rowers. Biology 2022, 11, 1513. [Google Scholar] [CrossRef]
- Kilic-Toprak, E.; Ardic, F.; Erken, G.; Unver-Kocak, F.; Kucukatay, V.; Bor-Kucukatay, M. Hemorheological Responses to Progressive Resistance Exercise Training in Healthy Young Males. Med. Sci. Monit. 2012, 18, CR351-60. [Google Scholar] [CrossRef]
- Boyle, L.J.; Nagelkirk, P.R. The Effects of Whole Body Vibration and Exercise on Fibrinolysis in Men. Eur. J. Appl. Physiol. 2010, 110, 1057–1061. [Google Scholar] [CrossRef]
- Myint, P.K.; Luben, R.N.; Wareham, N.J.; Welch, A.A.; Bingham, S.A.; Khaw, K.-T. Physical Activity and Fibrinogen Concentrations in 23,201 Men and Women in the EPIC-Norfolk Population-Based Study. Atherosclerosis 2008, 198, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Kabata-Piżuch, A.; Suder, A.; Jagielski, P.; Kubasiak, K.; Handzlik, P.; Teległów, A.; Marchewka, A. Effect of Vibrotherapy on Body Fatness, Blood Parameters and Fibrinogen Concentration in Elderly Men. J. Clin. Med. 2021, 10, 3259. [Google Scholar] [CrossRef] [PubMed]
- Ghazalian, F. Effects of Whole Body Vibration Training on Inflammatory Markers in Young Healthy Males. Ann. Mil. Health Sci. Res. 2019, 17, e89326. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Parameter | EG (n = 17) | CG (n = 12) | CON (n = 17) | p |
|---|---|---|---|---|
| Age [years] | 21.65 ± 1.8 | 20.17 ± 1.75 | 19.53 ± 0.72 | 0.064 |
| BH [cm] | 162.76 ± 7.51 | 164.67 ± 5.94 | 167.24 ± 4.56 | 0.187 |
| BM [kg] | 56.57 ± 7.18 | 59.43 ± 6.04 | 63.29 ± 8.71 ^ | 0.029 |
| BMI [kg/cm2] | 21.31 ± 1.87 | 22.02 ± 2.91 | 22.57 ± 2.44 | 0.351 |
| PBF [%] | 23.04 ± 6.11 | 25.62 ± 4.14 | 26.25 ± 5.76 | 0.351 |
| FM [kg] | 13.34 ± 4.54 | 15.4 ± 3.85 | 17.03 ± 5.89 | 0.119 |
| FFM [kg] | 43.24 ± 3.81 | 44.03 ± 2.84 | 46.25 ± 3.24 ^ | 0.013 |
| Parameter | I | II | Δ II-I | III | IV | Δ IV-III | Δ IV-II | ANOVA p Values (η2) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Time | Group | T × G | |||||||||
| RBC [106/µL] | EG | 4.34 ± 0.3 | 4.41 ± 0.29 | 0.07 ± 0.17 | 4.31 ± 0.27 | 4.38 ± 0.27 | 0.07 ± 0.08 | −0.03 ± 0.25 | 0.400 (0.035) | 0.130 (0.083) | 0.467 (0.031) |
| CG | 4.49 ± 0.31 | 4.52 ± 0.34 | 0.03 ± 0.11 | 4.53 ± 0.29 | 4.53 ± 0.29 | 0 ± 0.09 | 0.01 ± 0.18 | ||||
| Hb [g/dL] | EG | 12.71 ± 0.68 | 12.99 ± 0.76 | 0.28 ± 0.46 | 12.44 ± 0.66 # | 12.7 ± 0.7 # | 0.26 ± 0.25 | −0.29 ± 0.49 | 0.132 (0.065) | 0.009 (0.227) | 0.176 (0.059) |
| CG | 13.34 ± 0.74 | 13.41 ± 0.78 | 0.07 ± 0.31 | 13.39 ± 0.79 | 13.34 ± 0.79 | −0.05 ± 0.25 | −0.07 ± 0.72 | ||||
| Ht [%] | EG | 38 ± 1.93 | 38.68 ± 2.06 | 0.68 ± 1.52 | 37.19 ± 1.97 | 37.81 ± 1.76 | 0.62 ± 0.79 | −0.87 ± 2.16 | 0.416 (0.030) | 0.098 (0.098) | 0.066 (0.102) |
| CG | 38.73 ± 2.18 | 38.86 ± 2.51 | 0.13 ± 1.05 | 39.33 ± 1.94 | 39.16 ± 1.91 | −0.17 ± 0.85 | 0.30 ± 2.02 | ||||
| MCV [fl] | EG | 87.75 ± 3.87 | 87.86 ± 3.53 | 0.12 ± 0.93 | 86.46 ± 3.38 | 86.46 ± 3.4 † | 0 ± 0.49 | −1.41 ± 1.39 | 0.111 (0.083) | 0.596 (0.011) | <0.001 (0.240) |
| CG | 86.46 ± 2.82 | 86.09 ± 2.77 | −0.37 ± 0.99 | 86.89 ± 2.89 | 86.51 ± 3.04 | −0.38 ± 0.68 | 0.42 ± 1.7 | ||||
| MCH [pg] | EG | 29.35 ± 1.19 | 29.49 ± 1.14 | 0.15 ± 0.35 | 28.92 ± 1.28 | 29.02 ± 1.29 | 0.10 ± 0.31 | −0.47 ± 0.62 | <0.001 (0.202) | 0.330 (0.035) | 0.233 (0.052) |
| CG | 29.78 ± 1.07 | 29.73 ± 1.01 | −0.05 ± 0.29 | 29.59 ± 1.44 | 29.48 ± 1.44 | −0.11 ± 0.62 | −0.24 ± 0.82 | ||||
| MCHC [g/dL] | EG | 33.44 ± 0.64 | 33.58 ± 0.44 # | 0.14 ± 0.50 | 33.46 ± 0.79 | 33.58 ± 0.75 | 0.12 ± 0.47 | 0 ± 0.82 | 0.107 (0.078) | 0.002 (0.298) | 0.110 (0.077) |
| CG | 34.47 ± 0.88 | 34.53 ± 0.62 | 0.06 ± 0.72 | 34.05 ± 0.85 | 34.06 ± 0.78 | 0.01 ± 0.31 | −0.47 ± 0.55 | ||||
| RDW-SD [fl] | EG | 41.1 ± 3.16 | 40.96 ± 2.94 | −0.14 ± 0.94 | 40.6 ± 2.28 | 40.6 ± 2.28 | −0.01 ± 0.40 | −0.37 ± 2.5 | 0.743 (0.015) | 0.165 (0.070) | 0.127 (0.068) |
| CG | 39.12 ± 2.49 | 38.88 ± 2.23 | −0.23 ± 0.23 | 40.17 ± 3.73 | 40.17 ± 3.73 | −0.33 ± 0.63 | 0.95 ± 2.43 | ||||
| PLT [103/µL] | EG | 263.82 ± 55.6 | 286.47 ± 62.54 | 22.65 ± 17.51 | 275.71 ± 61.04 | 285.94 ± 54.49 | 10.24 ± 12.57 | −0.53 ± 48.63 | 0.126 (0.068) | 0.152 (0.075) | 0.723 (0.016) |
| CG | 301.42 ± 61.7 | 307.58 ± 65.8 | 6.17 ± 19.45 | 310.58 ± 63.56 | 315.25 ± 65.05 | 4.67 ± 14.07 | 7.67 ± 57.07 | ||||
| RETC [106/mm3] | EG | 0.05 ± 0.01 | 0.05 ± 0.01 | 0 ± 0.01 | 0.05 ± 0.01 | 0.05 ± 0.01 # | 0 ± 0 | 0 ± 0.01 | 0.110 (0.084) | 0.027 (0.169) | 0.678 (0.011) |
| CG | 0.06 ± 0.02 | 0.06 ± 0.02 | 0 ± 0.01 | 0.06 ± 0.01 | 0.06 ± 0.01 | 0 ± 0.01 | 0 ± 0.01 | ||||
| Shear Stress [Pa] | I | II | Δ II-I | III | IV | Δ IV-III | Δ IV-II | ANOVA p Values (η2) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Time | Group | T × G | |||||||||
| (0.3) | EG | 0.002 ± 0.011 | 0.001 ± 0.011 | −0.001 ± 0.006 | 0.022 ± 0.019 | 0.025 ± 0.017 † | 0.003 ± 0.023 | 0.024 ± 0.014 | <0.001 (0.341) | 0.062 (0.093) | <0.001 (0.283) |
| CG | 0.036 ± 0.01 | 0.036 ± 0.01 | 0 ± 0.006 | 0.039 ± 0.008 | 0.036 ± 0.008 | −0.003 ± 0.005 | 0 ± 0.008 | ||||
| (0.58) | EG | 0.049 ± 0.011 | 0.048 ± 0.009 | −0.001 ± 0.005 | 0.06 ± 0.008 | 0.06 ± 0.01 † | 0 ± 0.009 | 0.012 ± 0.009 | 0.004 (0.168) | 0.096 (0.098) | <0.001 (0.328) |
| CG | 0.068 ± 0.006 | 0.069 ± 0.007 | 0.001 ± 0.005 | 0.067 ± 0.006 | 0.066 ± 0.01 | −0.001 ± 0.006 | −0.004 ± 0.009 | ||||
| (1.13) | EG | 0.118 ± 0.011 | 0.119 ± 0.011 | 0.001 ± 0.004 | 0.126 ± 0.009 | 0.125 ± 0.009 | −0.001 ± 0.008 | 0.006 ± 0.012 | 0.03 (0.091) | 0.624 (0.002) | 0.158 (0.069) |
| CG | 0.137 ± 0.008 | 0.139 ± 0.008 | 0.001 ± 0.005 | 0.138 ± 0.008 | 0.139 ± 0.012 | 0 ± 0.006 | 0 ± 0.117 | ||||
| (2.19) | EG | 0.221 ± 0.014 | 0.223 ± 0.015 | 0.001 ± 0.005 | 0.224 ± 0.019 | 0.221 ± 0.019 | −0.003 ± 0.019 | −0.001 ± 0.023 | 0.942 (0.005) | 0.532 (0.009) | 0.963 (0.002) |
| CG | 0.24 ± 0.009 | 0.241 ± 0.01 | 0.001 ± 0.006 | 0.24 ± 0.008 | 0.24 ± 0.01 | −0.001 ± 0.008 | −0.001 ± 0.012 | ||||
| (4.24) | EG | 0.33 ± 0.016 | 0.331 ± 0.016 | 0.001 ± 0.005 | 0.326 ± 0.025 | 0.322 ± 0.028 | −0.004 ± 0.030 | −0.009 ± 0.031 | 0.645 (0.016) | 0.754 (0.005) | 0.598 (0.019) |
| CG | 0.345 ± 0.01 | 0.345 ± 0.011 | 0.001 ± 0.007 | 0.345 ± 0.008 | 0.346 ± 0.007 | 0.001 ± 0.008 | 0 ± 0.012 | ||||
| (8.24) | EG | 0.412 ± 0.018 | 0.413 ± 0.017 | 0.001 ± 0.008 | 0.409 ± 0.025 | 0.404 ± 0.031 | −0.004 ± 0.029 | −0.009 ± 0.032 | 0.876 (0.008) | 0.486 (0.025) | 0.478 (0.027) |
| CG | 0.428 ± 0.01 | 0.429 ± 0.011 | 0.001 ± 0.008 | 0.429 ± 0.008 | 0.431 ± 0.007 | 0.001 ± 0.008 | 0.002 ± 0.012 | ||||
| (15.98) | EG | 0.482 ± 0.017 | 0.483 ± 0.016 | 0.001 ± 0.007 | 0.478 ± 0.023 | 0.473 ± 0.029 | −0.004 ± 0.026 | −0.009 ± 0.028 | 0.923 (0.006) | 0.398 (0.046) | 0.267 (0.048) |
| CG | 0.491 ± 0.011 | 0.491 ± 0.012 | −0.001 ± 0.009 | 0.495 ± 0.01 | 0.495 ± 0.008 | 0.001 ± 0.009 | 0.004 ± 0.014 | ||||
| (31.03) | EG | 0.535 ± 0.014 | 0.536 ± 0.013 | 0 ± 0.006 | 0.531 ± 0.02 | 0.527 ± 0.025 | −0.004 ± 0.024 | −0.008 ± 0.023 | 0.792 (0.009) | 0.303 (0.039) | 0.256 (0.048) |
| CG | 0.536 ± 0.012 | 0.536 ± 0.014 | 0 ± 0.009 | 0.538 ± 0.011 | 0.539 ± 0.009 | 0.002 ± 0.011 | 0.003 ± 0.016 | ||||
| (60.3) | EG | 0.569 ± 0.015 | 0.569 ± 0.013 | 0 ± 0.005 | 0.567 ± 0.017 | 0.563 ± 0.021 | −0.004 ± 0.020 | −0.006 ± 0.021 | 0.235 (0.053) | 0.368 (0.030) | 0.084 (0.101) |
| CG | 0.563 ± 0.017 | 0.564 ± 0.021 | 0.001 ± 0.014 | 0.572 ± 0.011 | 0.596 ± 0.081 | 0.023 ± 0.074 | 0.032 ± 0.079 | ||||
| Parameter | I | II | Δ II-I | III | IV | Δ IV-III | Δ IV-II | ANOVA p Values (η2) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Time | Group | T × G | |||||||||
| AMP [au] | EG | 13.08 ± 1.59 ## | 12.89 ± 1.96 ## | −0.19 ± 2.29 | 15.17 ± 2.14 # | 15.06 ± 2.33 # † | −0.12 ± 2.24 | 2.17 ± 3.34 | 0.104 (0.076) | <0.001 (0.698) | 0.003 (0.162) |
| CG | 17.44 ± 1.91 | 18.24 ± 1.91 | 0.80 ± 2.63 | 17.63 ± 2.27 | 17.08 ± 1.65 | −0.55 ± 1.28 | −1.16 ± 1.45 | ||||
| T½ [s] | EG | 2.36 ± 0.77 | 2.17 ± 0.69 | −0.19 ± 0.47 | 2.51 ± 0.74 | 2.57 ± 1.45 | 0.06 ± 0.88 | 0.40 ± 1.34 | 0.387 (0.038) | 0.392 (0.028) | 0.736 (0.009) |
| CG | 2.54 ± 0.52 | 2.57 ± 0.56 | 0.03 ± 0.33 | 2.64 ± 0.97 | 2.75 ± 0.95 | 0.12 ± 0.37 | 0.19 ± 0.98 | ||||
| AI [%] | EG | 62.02 ± 7.45 | 63.59 ± 7.07 | 1.57 ± 5.00 | 60.45 ± 6.28 | 61.1 ± 9.38 | 0.65 ± 5.05 | −2.49 ± 8.43 | 0.530 (0.028) | 0.392 (0.028) | 0.567 (0.019) |
| CG | 59.74 ± 4.17 | 59.52 ± 4.32 | −0.22 ± 2.53 | 59.67 ± 7.66 | 58.4 ± 7.46 | −1.27 ± 2.78 | −1.13 ± 7.47 | ||||
| fibrinogen [g/L] | EG | 2.57 ± 0.42 | 2.77 ± 0.54 | 0.20 ± 0.24 | 2.6 ± 0.43 | 2.7 ± 0.45 | 0.10 ± 0.15 | −0.07 ± 0.46 | 0.113 (0.071) | 0.865 (0.001) | 0.351 (0.032) |
| CG | 2.68 ± 0.58 | 2.74 ± 0.62 | 0.05 ± 0.20 | 2.53 ± 0.4 | 2.58 ± 0.41 | 0.05 ± 0.13 | −0.16 ± 0.541 | ||||
| Parameter | I | III | Δ III-I | ANOVA p Values (η2) | |||
|---|---|---|---|---|---|---|---|
| Time | Group | T × G | |||||
| RBC [106/µL] | EG | 4.34 ± 0.3 | 4.31 ± 0.27 | −0.03 ± 0.27 | 0.681 (0.004) | 0.126 (0.092) | 0.593 (0.024) |
| CG | 4.49 ± 0.31 | 4.53 ± 0.29 | 0.05 ± 0.1 | ||||
| CON | 4.46 ± 0.24 | 4.48 ± 0.29 | 0.03 ± 0.21 | ||||
| Hb [g/dL] | EG | 12.71 ± 0.68 | 12.44 ± 0.66 # | −0.27 ± 0.78 | 0.356 (0.020) | <0.001 (0.550) | 0.400 (0.042) |
| CG | 13.34 ± 0.74 | 13.39 ± 0.79 | 0.05 ± 0.5 | ||||
| CON | 12.85 ± 0.67 | 12.8 ± 0.71 | −0.05 ± 0.6 | ||||
| Ht [%] | EG | 38 ± 1.93 | 37.19 ± 1.97 | −0.81 ± 2.35 | 0.385 (0.018) | 0.064 (0.120) | 0.144 (0.086) |
| CG | 38.73 ± 2.18 | 39.33 ± 1.94 | 0.6 ± 1.22 | ||||
| CON | 38.75 ± 1.39 | 38.2 ± 1.89 | −0.55 ± 1.85 | ||||
| MCV [fl] | EG | 87.75 ± 3.87 | 86.46 ± 3.38 * | −1.29 ± 1.57 | 0.015 (0.131) | 0.759 (0.013) | 0.534 (0.014) |
| CG | 86.46 ± 2.82 | 86.89 ± 2.89 | 0.43 ± 1.57 | ||||
| CON | 87.06 ± 3.94 | 85.36 ± 4.32 | −1.7 ± 3.05 | ||||
| MCH [pg] | EG | 29.35 ± 1.19 | 28.92 ± 1.28 * | −0.42 ± 0.38 | 0.006 (0.160) | 0.245 (0.063) | 0.613 (0.023) |
| CG | 29.78 ± 1.07 | 29.59 ± 1.44 | −0.18 ± 0.76 | ||||
| CON | 28.88 ± 1.64 | 28.62 ± 1.98 | −0.26 ± 0.83 | ||||
| MCHC [g/dL] | EG | 33.44 ± 0.64 | 33.46 ± 0.79 * | 0.02 ± 0.38 | 0.015 (0.178) | 0.134 (0.073) | 0.895 (0.000) |
| CG | 34.47 ± 0.88 | 34.05 ± 0.85 | −0.42 ± 0.76 | ||||
| CON | 33.15 ± 0.92 | 33.51 ± 0.91 | 0.36 ± 0.83 | ||||
| RDW-SD [fl] | EG | 41.1 ± 3.16 | 40.6 ± 2.28 | −0.5 ± 2.85 | 0.794 (0.002) | 0.366 (0.046) | 0.146 (0.086) |
| CG | 39.12 ± 2.49 | 40.17 ± 3.73 | 1.05 ± 3.05 | ||||
| CON | 41.15 ± 2.34 | 40.29 ± 2.32 | −0.86 ± 1.99 | ||||
| PLT [103/µL] | EG | 263.82 ± 55.6 | 275.71 ± 61.04 | 11.88 ± 42.51 | 0.110 (0.058) | 0.255 (0.062) | 0.966 (0.002) |
| CG | 301.42 ± 61.7 | 310.58 ± 63.56 | 9.17 ± 52.35 | ||||
| CON | 268.06 ± 67.45 | 281.94 ± 76.63 | 13.88 ± 49.45 | ||||
| RETC [106/mm3] | EG | 0.05 ± 0.01 | 0.05 ± 0.01 | 0 ± 0.01 | 0.309 (0.024) | 0.184 (0.076) | 0.122 (0.093) |
| CG | 0.06 ± 0.02 | 0.06 ± 0.01 | −0.01 ± 0.01 | ||||
| CON | 0.05 ± 0.02 | 0.06 ± 0.02 | 0 ± 0.01 | ||||
| Shear Stress [Pa] | I | III | Δ III-I | ANOVA p Values (η2) | |||
|---|---|---|---|---|---|---|---|
| Time | Group | T × G | |||||
| (0.3) | EG | 0 ± 0.01 | 0.02 ± 0.02 * | 0.020 ± 0.020 | <0.001 (0.505) | 0.267 (0.003) | 0.456 (0.057) |
| CG | 0.04 ± 0.01 | 0.04 ± 0.01 | 0.003 ± 0.010 | ||||
| CON | 0.02 ± 0.01 | 0.04 ± 0.02 | 0.024 ± 0.001 | ||||
| (0.58) | EG | 0.049 ± 0.011 | 0.06 ± 0.008 * | 0.011 ± 0.010 | 0.048 (0.088) | 0.498 (0.002) | 0.132 (0.045) |
| CG | 0.068 ± 0.006 | 0.067 ± 0.006 | −0.001 ± 0.008 | ||||
| CON | 0.062 ± 0.008 | 0.06 ± 0.008 | −0.002 ± 0.008 | ||||
| (1.13) | EG | 0.118 ± 0.01 | 0.126 ± 0.009 * | 0.008 ± 0.011 | 0.004 (0.300) | 0.092 (0.094) | 0.187 (0.031) |
| CG | 0.137 ± 0.008 | 0.138 ± 0.008 | 0.001 ± 0.010 | ||||
| CON | 0.129 ± 0.009 | 0.118 ± 0.009 | −0.011 ± 0.012 | ||||
| (2.19) | EG | 0.221 ± 0.014 | 0.224 ± 0.019 | 0.002 ± 0.021 | 0.734 (0.002) | 0.692 (0.057) | 0.298 (0.049) |
| CG | 0.24 ± 0.009 | 0.24 ± 0.008 | 0.001 ± 0.010 | ||||
| CON | 0.233 ± 0.012 | 0.201 ± 0.011 | −0.033 ± 0.015 | ||||
| (4.24) | EG | 0.33 ± 0.016 | 0.326 ± 0.025 | −0.004 ± 0.078 | 0.085 (0.056) | 0.154 (0.042) | 0.365 (0.008) |
| CG | 0.345 ± 0.01 | 0.345 ± 0.00 | 0 ± 0.010 | ||||
| CON | 0.341 ± 0.014 | 0.291 ± 0.014 | −0.050 ± 0.016 | ||||
| (8.24) | EG | 0.412 ± 0.018 | 0.409 ± 0.025 | −0.003 ± 0.029 | 0.876 (0.008) | 0.429 (0.035) | 0.478 (0.027) |
| CG | 0.428 ± 0.01 | 0.429 ± 0.008 | 0.002 ± 0.008 | ||||
| CON | 0.424 ± 0.016 | 0.372 ± 0.015 | −0.052 ± 0.016 | ||||
| (15.98) | EG | 0.482 ± 0.017 | 0.478 ± 0.023 | −0.004 ± 0.026 | 0.258 (0.007) | 0.387 (0.043) | 0.621 (0.001) |
| CG | 0.491 ± 0.011 | 0.495 ± 0.01 | 0.003 ± 0.008 | ||||
| CON | 0.491 ± 0.016 | 0.445 ± 0.015 | −0.046 ± 0.016 | ||||
| (31.03) | EG | 0.535 ± 0.014 | 0.531 ± 0.02 | −0.004 ± 0.022 | 0.148 (0.062) | 0.095 (0.123) | 0.082 (0.156) |
| CG | 0.536 ± 0.012 | 0.538 ± 0.011 | 0.002 ± 0.008 | ||||
| CON | 0.542 ± 0.012 | 0.503 ± 0.012 | −0.039 ± 0.012 | ||||
| (60.3) | EG | 0.569 ± 0.015 | 0.567 ± 0.017 | −0.002 ± 0.021 | 0.087 (0.078) | 0.081 (0.110) | 0.166 (0.094) |
| CG | 0.563 ± 0.017 | 0.572 ± 0.011 | 0.009 ± 0.011 | ||||
| CON | 0.576 ± 0.012 | 0.543 ± 0.014 | −0.033 ± 0.012 | ||||
| Parameter | I | III | Δ III-I | ANOVA p Values (η2) | |||
|---|---|---|---|---|---|---|---|
| Time | Group | T × G | |||||
| AMP [au] | EG | 13.08 ± 1.59 ## | 15.17 ± 2.14 * # | 2.09 ± 2.94 | 0.003 (0.205) | <0.001 (0.550) | 0.170 (0.087) |
| CG | 17.44 ± 1.91 && | 17.63 ± 2.27 & | 0.2 ± 2.65 | ||||
| CON | 13 ± 2.13 | 14.59 ± 1.99 | 1.59 ± 2.18 | ||||
| T½ [s] | EG | 2.36 ± 0.77 | 2.51 ± 0.74 | 0.15 ± 0.92 | 0.597 (0.007) | 0.802 (0.011) | 0.827 (0.009) |
| CG | 2.54 ± 0.52 | 2.64 ± 0.97 | 0.1 ± 1.04 | ||||
| CON | 2.44 ± 0.97 | 2.4 ± 0.97 | −0.04 ± 0.65 | ||||
| AI [%] | EG | 62.02 ± 7.45 | 60.45 ± 6.28 | −1.56 ± 7.71 | 0.769 (0.002) | 0.723 (0.016) | 0.693 (0.018) |
| CG | 59.74 ± 4.17 | 59.67 ± 7.66 | −0.07 ± 8.42 | ||||
| CON | 61.23 ± 7.96 | 61.87 ± 8.52 | 0.64 ± 5.69 | ||||
| fibrynogen [g/L] | EG | 2.57 ± 0.42 | 2.6 ± 0.43 | 0.04 ± 0.4 | 0.792 (0.002) | 0.988 (0.001) | 0.422 (0.039) |
| CG | 2.68 ± 0.58 | 2.53 ± 0.4 | −0.16 ± 0.56 | ||||
| CON | 2.55 ± 0.46 | 2.62 ± 0.61 | 0.07 ± 0.49 | ||||
| p | |||
|---|---|---|---|
| %ΔPV1 | EG | −2.85 ± 5.36 | 0.215 |
| CG | −0.62 ± 3.40 | ||
| %ΔPV2 | EG | −2.77 ± 2.66 | 0.003 |
| CG | 0.64 ± 2.92 | ||
| %ΔPV3 | EG | 3.65 ± 9.42 | 0.137 |
| CG | −1.01 ± 5.54 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gattner, H.; Adamiak, J.; Piotrowska, A.; Czerwińska-Ledwig, O.; Mętel, S.; Kępińska-Szyszkowska, M.; Pilch, W. Effect of Whole-Body Vibration Training on Hemorheological Blood Indices in Young, Healthy Women. Int. J. Environ. Res. Public Health 2023, 20, 3232. https://doi.org/10.3390/ijerph20043232
Gattner H, Adamiak J, Piotrowska A, Czerwińska-Ledwig O, Mętel S, Kępińska-Szyszkowska M, Pilch W. Effect of Whole-Body Vibration Training on Hemorheological Blood Indices in Young, Healthy Women. International Journal of Environmental Research and Public Health. 2023; 20(4):3232. https://doi.org/10.3390/ijerph20043232
Chicago/Turabian StyleGattner, Halina, Justyna Adamiak, Anna Piotrowska, Olga Czerwińska-Ledwig, Sylwia Mętel, Magdalena Kępińska-Szyszkowska, and Wanda Pilch. 2023. "Effect of Whole-Body Vibration Training on Hemorheological Blood Indices in Young, Healthy Women" International Journal of Environmental Research and Public Health 20, no. 4: 3232. https://doi.org/10.3390/ijerph20043232