
Experience and Satisfaction with a Family-Based Physical Activity Intervention Using Activity Trackers and Apps: A Qualitative Study
 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. The Step It Up Family Intervention
2.4. Data Collection
- “What did you like about the introductory session?”
- “What did you NOT like about the introductory session?”
- “What did you like about the text messages?”
- “What did you NOT like about the text messages?”
- “Did you experience any difficulties in using the Garmin activity trackers or Garmin apps?”
- “Could you please tell us what it is about the Garmin activity trackers and apps that made you use them regularly?”
- “What did you think of the features of the Garmin activity trackers and apps? What did you like about them, and what not?”
2.5. Data Analysis
3. Results
3.1. Sociodemographic Characteristics of Families
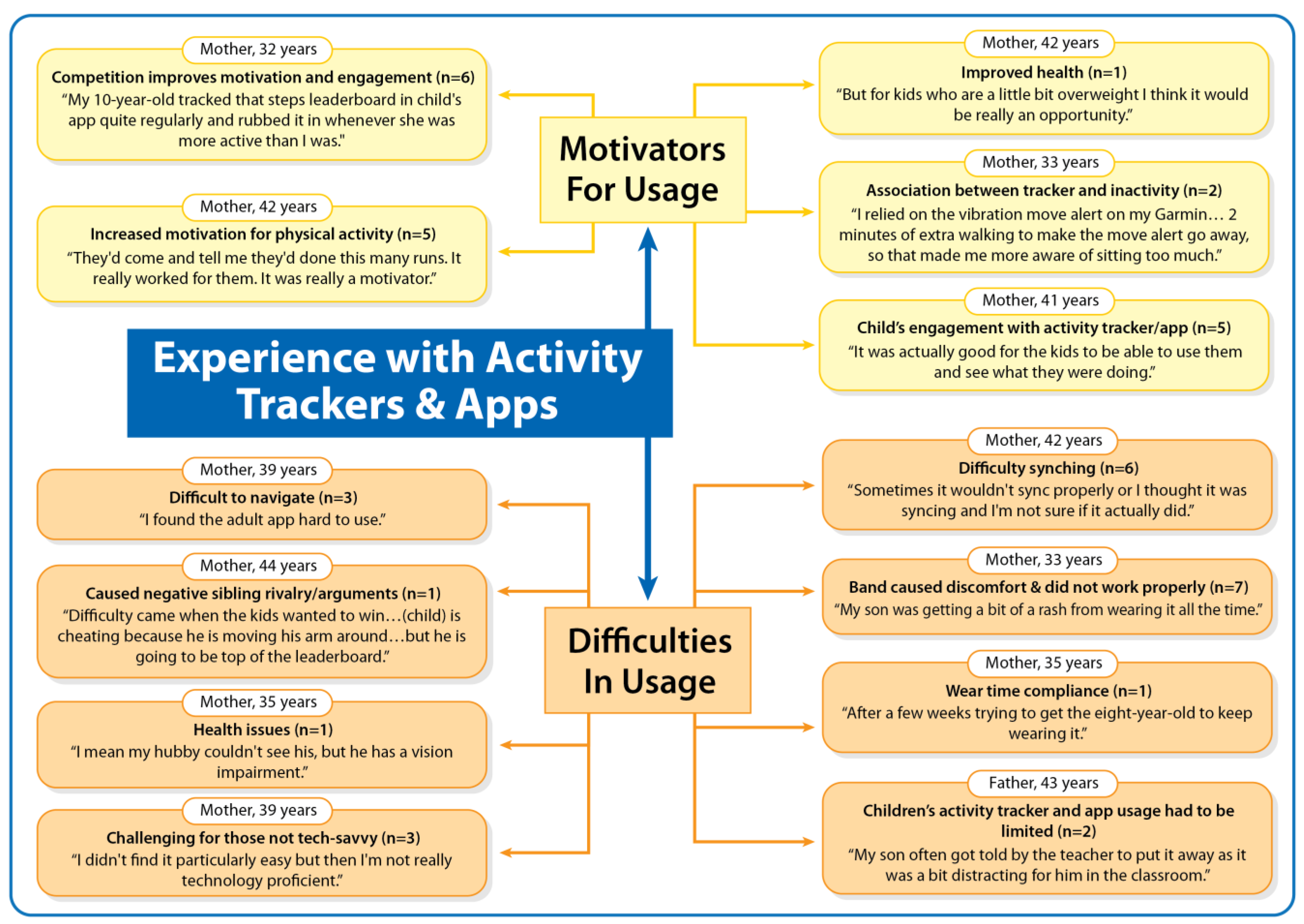
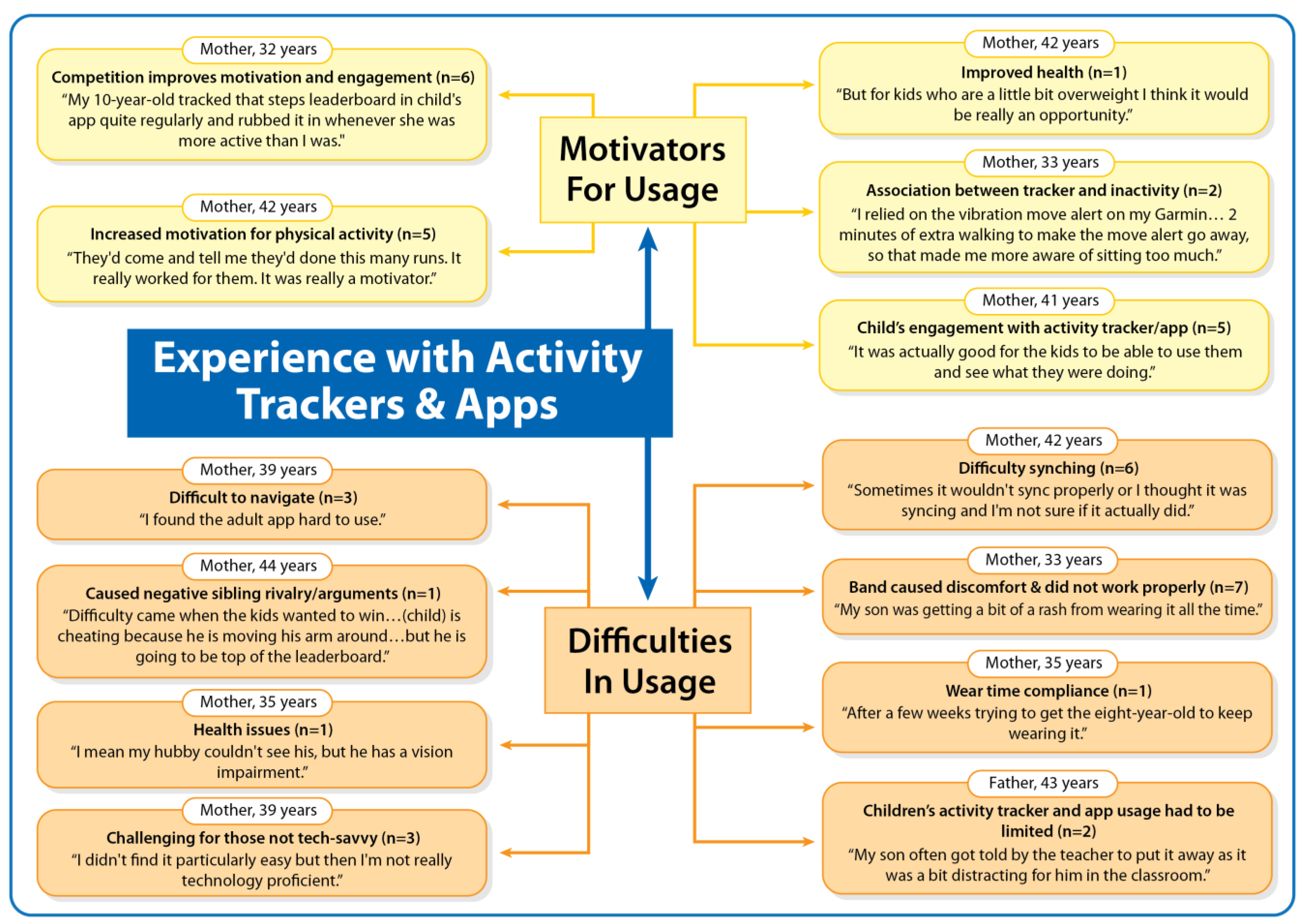
3.2. Experience with the Activity Trackers and Apps
3.2.1. Motivators for Usage
My 10-year-old tracked that steps leaderboard in child’s app quite regularly and rubbed it in whenever she was more active than I was.[Mother, 32 years; physical activity increased within the family]
It was actually good for the kids to be able to use them and see what they were doing.[Mother, 41 years; physical activity increased within the family]
They’d come and tell me they’d done this many runs. It really worked for them. It was really a motivator.[Mother, 42 years; physical activity increased within the family]
I relied on the vibration move alert on my Garmin…2 min of extra walking to make the move alert go away, so that made me more aware of sitting too much.[Mother, 33 years; physical activity increased within the family]
3.2.2. Difficulties in Usage
My son was getting a bit of a rash from wearing it all the time… it would come undone really easily.[Mother, 33 years; physical activity increased within the family]
The child’s band broke part way through.[Mother, 44 years; physical activity increased within the family]
Sometimes it wouldn’t sync properly or I thought it was syncing and I’m not sure if it actually did.[Mother, 42 years; physical activity increased within the family]
I found the adult app hard to use.[Mother, 39 years; physical activity did not increase within the family]
I didn’t find it particularly easy but then I’m not really technology proficient.[Mother, 39 years; physical activity did not increase within the family]
My son often got told by the teacher to put it away as it was a bit distracting for him in the classroom.[Father, 43 years; physical activity increased within the family]
Difficulty came when the kids wanted to win…(child) is cheating because he is moving his arm around…but he is going to be top of the leaderboard.[Mother, 44 years; physical activity increased within the family]
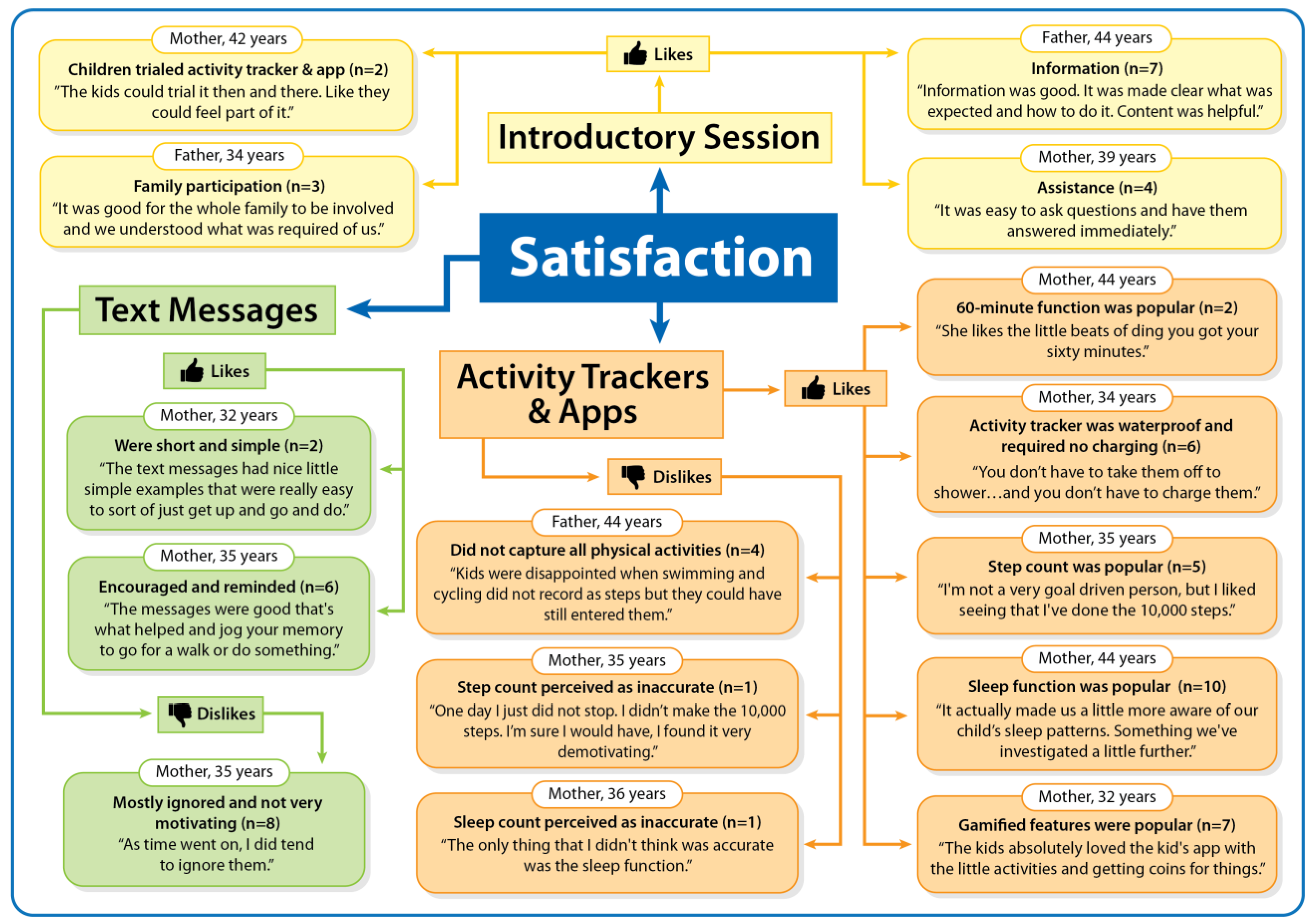
3.3. Satisfaction with the Step it Up Family Intervention Components
3.3.1. Introductory Session
Information was good. It was made clear what was expected and how to do it. Content was helpful.[Father, 44 years; physical activity increased within the family]
It was easy to ask questions and have them answered immediately.[Mother, 39 years; physical activity did not increase within the family]
It was good for the whole family to be involved and we understood what was required of us.[Father, 34 years; physical activity increased within the family]
The kids could trial it then and there. Like they could feel part of it.[Mother, 42 years; physical activity increased within the family]
3.3.2. Activity Trackers and Apps
You don’t have to take them off to shower…and you don’t have to charge them.[Mother, 34 years; physical activity did not increase within the family]
I’m not a very goal driven person, but I liked seeing that I’ve done the 10,000 steps.[Mother, 35 years; physical activity increased within the family]
It actually made us a little more aware of our child’s sleep patterns. Something we’ve investigated a little further.[Mother, 44 years; physical activity increased within the family]
The kids absolutely loved the kid’s app with the little activities and getting coins for things.[Mother, 32 years; physical activity increased within the family]
She likes the little beats of ding you got your sixty minutes.[Mother, 44 years; physical activity increased within the family]
Kids were disappointed when swimming and cycling did not record as steps but they could have still entered them.[Father, 44 years; physical activity increased within the family]
3.3.3. Text Messages
The messages were good that’s what helped and jog your memory to go for a walk or do something.[Mother, 32 years; physical activity increased within the family]
The text messages had nice little simple examples that were really easy to sort of just get up and go and do.[Mother, 32 years; physical activity increased within the family]
In regard to the text messages, they were neutral on the benefits of those. For them it wasn’t motivating.[Mother, 44 years; physical activity increased within the family]
I did read them, but probably didn’t implement them, I guess.[Mother, 41 years; physical activity increased within the family]
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Government, Department of Health and Aged Care. Australian Physical Activity Guidelines for Adults (18–64 years). 2021. Available online: https://www.health.gov.au/health-topics/physical-activity-and-exercise/physical-activity-and-exercise-guidelines-for-all-australians/for-adults-18-to-64-years (accessed on 2 November 2022).
- Australian Government, Department of Health and Aged Care. Australian 24-hour Movement Guidelines for Children (5–12 years) and Young People (13–17 years): An Integration of Physical Activity, Sedentary Behaviour, and Sleep. 2019. Available online: https://www.health.gov.au/sites/default/files/documents/2021/03/australian-24-hour-movement-guidelines-for-children-5-to-12-years-and-young-people-13-to-17-years-an-integration-of-physical-activity-sedentary-behaviour-and-sleep.pdf (accessed on 2 November 2022).
- Australian Institute of Health and Welfare. Insufficient Physical Activity. 2019. Available online: https://www.aihw.gov.au/getmedia/44533aa4-5704-447d-8d2a-4d68d9fa2416/Insufficient (accessed on 2 November 2022).
- Active Healthy Kids Australia. The 2016 Report Card on Physical Activity for Children and Young People. 2016. Available online: https://www.activehealthykids.org/wp-content/uploads/2018/11/australia-report-card-long-form-2016.pdf (accessed on 2 November 2022).
- Australian Institute of Health and Welfare. Physical Activity Across the Life Stages. 2018. Available online: https://www.aihw.gov.au/getmedia/c249ef97-e219-44df-a8bd-f5e50d04064c/aihw-phe-225.pdf.aspx?inline=true (accessed on 10 April 2022).
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2885312/pdf/1479-5868-7-40.pdf (accessed on 1 January 2023). [CrossRef]
- Saunders, J.T.; Gray, C.E.; Poitras, J.P.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Olds, T.; Gorber, C.; Kho, M.E.; Sampson, M.; et al. Combinations of physical activity, sedentary behaviour and sleep: Relationships with health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S240–S265. [Google Scholar] [CrossRef]
- Barnett, L.M.; Lai, S.M.; Veldman, S.L.C.; Hardy, L.H.; Cliff, D.P.; Morgan, P.J.; Zask, A.; Lubans, D.R.; Shultz, S.P.; Ridgers, N.D.; et al. Correlates of gross motor competence in children and adolescents: A systematic review and meta-analysis. Sports Med. 2016, 46, 1663–1688. [Google Scholar] [CrossRef]
- Brown, W.J.; Bauman, A.E.; Bull, F.C.; Burton, N.W. Development of Evidence-Based Physical Activity Recommendations for Adults (18–64 Years); Australian Government Department of Health: Woden Town, Australia, 2012. Available online: https://www.health.gov.au/sites/default/files/documents/2021/03/development-of-evidence-based-physical-activity-for-adults-18-to-64-years.pdf (accessed on 10 April 2022).
- Medibank Private. The Cost of Physical Inactivity. Medibank Health Foundation. 2008. Available online: https://www.medibank.com.au/content/dam/client/documents/pdfs/The_Cost_Of_Physical_Inactivity_08.pdf (accessed on 1 January 2023).
- Mitchell, J. Physical inactivity in childhood from preschool to adolescence. ACSMs Health Fit. J. 2019, 23, 21–25. [Google Scholar] [CrossRef]
- Schoeppe, S.; Liersch, S.; Röbl, M.; Krauth, C.; Walter, U. Mothers and fathers both matter: The positive influence of parental physical activity modelling on children’s leisure-time physical activity. Pediatr. Exerc. Sci. 2016, 28, 466–472. [Google Scholar] [CrossRef]
- Schoeppe, S.; Trost, S. Maternal and paternal support for physical activity and healthy eating behaviours in preschool children. BMC Public Health 2015, 15, 971. [Google Scholar] [CrossRef] [PubMed]
- Schoeppe, S.; Vandelanotte, C.; Bere, E.; Lien, N.; Verloigne, M.; Kovácse, E.; Manios, Y.; Bjelland, M.; Vikb, F.N.; Van Lippevelde, W. The influence of parental modelling on children’s physical activity and screen time: Does it differ by gender? Eur. J. Public Health 2017, 27, 152–157. [Google Scholar] [CrossRef]
- Trost, S.G.; Loprinzi, P.D. Parental influences on physical activity behavior in children and adolescents: A brief review. Am. J. Lifestyle Med. 2011, 5, 171–181. [Google Scholar] [CrossRef]
- Sleddens, E.F.C.; Gubbels, J.S.; Kremers, S.P.J.; van der Plas, E.; Thijs, C. Bidirectional associations between activity-related parenting practices, and child physical activity, sedentary screen-based behavior and body mass index: A longitudinal analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 89. [Google Scholar] [CrossRef]
- Rainham, D.J.; Bennett, M.; Blanchard, C.M.; Kirk, S.F.L.; Rehman, L.; Stone, M.; Stevens, D. Parents and children should be more active together to address physical inactivity and sedentary behaviours. Front. Public Health. 2022, 10, 633111. [Google Scholar] [CrossRef]
- Brown, H.E.; Atkin, A.J.; Panter, J.; Wong, G.; Chinapaw, M.J.; Sluijs, E.M.F. Family-based interventions to increase physical activity in children: A systematic review, meta-analysis and realist synthesis. Obes. Rev. 2016, 17, 345–360. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Young, M.D. Influence of fathers on children’s physical activity and dietary behaviors: Insights, recommendations and future directions. Curr. Obes. Rep. 2017, 6, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Guagliano, J.M.; Armitage, S.M.; Brown, H.E.; Coombes, E.; Fusco, F.; Hughes, C.; Jones, A.P.; Morton, K.L.; van Sluijs, M.F. A whole family-based physical activity promotion intervention: Findings from the families reporting every step to health (FRESH) pilot randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 120. [Google Scholar] [CrossRef]
- Wunsch, K.; Eckert, T.; Fiedler, J.; Cleven, L.; Niermann, C.; Reiterer, H.; Renner, B.; Wolf, A. Effects of a collective family-based mobile health intervention called “SMARTFAMILY” on promoting physical activity and healthy eating: Protocol for a randomized controlled trial. J. Med. Internet Res. Protoc. 2020, 9, e20534. [Google Scholar] [CrossRef] [PubMed]
- Schoeppe, S.; Salmon, J.; Williams, S.L.; Power, D.; Alley, S.; Rebar, A.L.; Hayman, M.; Duncan, M.J.; Vandelanotte, C. Effects of an activity tracker and app intervention to increase physical activity in whole families-The Step it Up Family Feasibility Study. Int. J. Environ. Res. Public Health 2020, 17, 7655. [Google Scholar] [CrossRef] [PubMed]
- Schoeppe, S.; Salmon, J.; Williams, S.; Power, D.; Waters, K.; Alley, S.; Rebar, A.L.; Hayman, M.; Duncan, M.J.; Vandelanotte, C. Feasibility of using activity trackers and apps to increase physical activity in whole families: The Step it Up Family intervention. Digit. Health 2022, 8, 20552076221129083. [Google Scholar] [CrossRef] [PubMed]
- Guagliano, J.M.; Brown, H.E.; Coombe, E.; Hughes, C.; Jones, A.P.; Morton, K.L.; Wilson, E.C.F.; van Sluijs, E.M.F. The development and feasibility of a randomised family-based physical activity promotion intervention: The families reporting every Step to health (FRESH) study. Pilot. Feasibility Stud. 2019, 5, 21. [Google Scholar] [CrossRef]
- Creaser, A.V.; Hall, J.; Costa, S.; Bingham, D.D.; Clemes, S.A. Exploring families’ acceptance of wearable activity trackers: A mixed-methods study. Int. J. Environ. Res. Public Health 2022, 19, 3472. [Google Scholar] [CrossRef]
- Henriksen, A.; Mikalsen, M.H.; Woldaregay, A.Z.; Muzny, M.; Hartvigsen, G.; Hopstock, L.A.; Grimsgaard, S. Using fitness trackers and smartwatches to measure physical activity in research: Analysis of consumer wrist-worn wearables. J. Med. Internet Res. 2018, 20, e110. [Google Scholar] [CrossRef]
- Alley, S.; Schoeppe, S.; Vandelanotte, C. Interest and preferences for using advanced physical activity tracking devices: A national cross-sectional survey. BMJ Open 2016, 6, e011243. [Google Scholar] [CrossRef] [Green Version]
- Ridgers, N.D.; Timperio, A.; Brown, H.; Ball, K.; Macfarlane, S.; Lai, S.K.; Richards, K.; Mackintosh, K.A.; McNarry, M.A.; Foster, M.; et al. Wearable activity tracker use among Australian adolescents: Usability and acceptability study. JMIR mHealth uHealth 2018, 6, e86. [Google Scholar] [CrossRef] [PubMed]
- Klein, D. Electronic activity trackers encourage family fun and fitness. Australas. Med. J. 2015, 8, 216–218. [Google Scholar] [CrossRef]
- Communications and Media in Australia: Trends and Developments in Telecommunications 2020–21. 2021. Available online: https://www.acma.gov.au/sites/default/files/2021-12/Trends%20and%20developments%20in%20telecommunications%202020-21_0.pdf (accessed on 10 April 2022).
- Brickwood, K.J.; Watson, G.; O’Brien, J.; Williams, A.D. Consumer-based wearable activity trackers increase physical activity participation: Systematic Review and meta-analysis. JMIR mHealth uHealth 2019, 7, e11819. [Google Scholar] [CrossRef] [PubMed]
- Laranjo, L.; Ding, D.; Heleno, B.; Kocaballi, B.; Quiroz, J.C.; Tong, H.L.; Chahwan, B.; Neves, A.L.; Gabarron, E.; Dao, K.P.; et al. Do smartphone applications and activity trackers increase physical activity in adults? Systematic review, meta-analysis and metaregression. Br. J. Sports Med. 2021, 55, 422–432. [Google Scholar] [CrossRef] [PubMed]
- Casado-Robles, C.; Viciana, J.; Guijarro-Romero, S.; Mayorga-Vega, D. Effects of consumer-wearable activity tracker-based programs on objectively measured daily physical activity and sedentary behavior among school-aged children: A systematic review and meta-analysis. Sports Med. Open 2022, 8, 18. [Google Scholar] [CrossRef]
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.L.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 127. [Google Scholar] [CrossRef]
- Rodríguez-González, P.; Hassan, M.A.; Gao, Z. Effects of family-based Interventions Using Mobile Apps on Youth’s Physical Activity: A Systematic Review. J. Clin. Med. 2022, 11, 4798. [Google Scholar] [CrossRef]
- Bianchi-Hayes, J.; Schoenfeld, E.; Cataldo, R.; Hou, W.; Messina, C.; Pati, S. Combining activity trackers with motivational interviewing and mutual support to increase physical activity in parent-adolescent dyads: Longitudinal observational feasibility study. JMIR Pediatr. Parent. 2018, 1, e3. [Google Scholar] [CrossRef]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Burnard, P. A method of analysing interview transcripts in qualitative research. Nurse Educ. Today 1991, 11, 461–466. [Google Scholar] [CrossRef]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs. Health Sci. 2013, 3, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Hilland, T.; Ridgers, N.; Stratton, G.; Knowles, Z.; Fairclough, S. Origins of perceived physical education ability and worth among English adolescents. Eur. Phys. Edu. Rev. 2018, 24, 165–180. [Google Scholar] [CrossRef]
- Mackintosh, K.A.; Chappel, S.E.; Salmon, J.; Timperio, A.; Ball, K.; Brown, H.; Macfarlane, S.; Ridgers, N.D. Parental perspectives of a wearable activity tracker for children younger than 13 years: Acceptability and usability study. JMIR mHealth uHealth 2019, 7, e13858. [Google Scholar] [CrossRef] [PubMed]
- Schoeppe, S.; Duncan, M.J.; Plotnikoff, R.C.; Mummery, W.K.; Rebar, A.; Alley, S.; To, Q.; Short, C.E.; Vandelanotte, C. Acceptability, usefulness and satisfaction with a web-based video-tailored physical activity intervention: The TaylorActive randomised controlled trial. J. Sport Health Sci. 2022, 11, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Guest, G.; Namey, E.; Chen, M. A Simple method to assess and report thematic saturation in qualitative research. PLoS ONE 2020, 15, e0232076. [Google Scholar] [CrossRef] [PubMed]
- Caperchione, C.; Vandelanotte, C.; Corry, K.; Power, D.; Gill, N.; Duncan, M.J. Qualitative exploration of the feasibility and acceptability of workplace-based microgrants to improve physical activity: The 10,000 Steps Pedometer Microgrant Scheme. J. Occup. Environ. Med. 2018, 60, e406–e411. [Google Scholar] [CrossRef]
- Hardcastle, S.; Hagger, M. ‘You can’t do it on your own’: Experiences of a motivational interviewing intervention on physical activity and dietary behaviour. Psychol. Sport Exerc. 2011, 12, 314–323. [Google Scholar] [CrossRef]
- Lamers, C.R.; de Roos, N.M.; Koppelman, L.J.M.; Hopman, M.T.E.; Witteman, B.J.M. Patient experiences with the role of physical activity in inflammatory bowel disease: Results from a survey and interviews. BMC Gastroenterol. 2021, 21, 172. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Brookes, D.S.K. Effectiveness of a novel digital application to promote fundamental movement skills in 3- to 6-year-old children: A randomized controlled trial. J. Sports Sci. 2021, 39, 453–459. [Google Scholar] [CrossRef]
- Maher, C.; Olds, T.; Vandelanotte, C.; Plotnikoff, R.; Edney, S.; Ryan, J.; DeSmet, A.; Curtis, R.G. Gamification in a physical activity app–what gamification features are being used, by whom, and does it make a difference? Games Health 2022, 11, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Edeny, S.; Olds, T.; Ryan, J.; Vandelanotte, C.; Plotnikoff, R.; Curtis, R.; Maher, C. A social networking and gamified app to increase physical activity: Cluster-RCT. Am. J. Prev. Med. 2020, 58, e51–e61. [Google Scholar] [CrossRef] [PubMed]
- Mclaughlin, M.; Delaney, T.; Hall, A.; Byaruhanga, J.; Mackie, P.; Grady, A.; Reilly, K.; Campbell, E.; Sutherland, R.; Wiggers, J.; et al. Associations between digital health intervention engagement, physical activity, and sedentary behavior: Systematic review and meta-analysis. J. Med. Internet Res. 2021, 23, e23180. [Google Scholar] [CrossRef] [PubMed]
- Vandelanotte, C.; Van Itallie, A.; Brown, W.; Mummery, W.K.; Duncan, M.J. Every step counts: Understanding the success of implementing the 10,000 Steps project. Stud. Health Technol. Inform. 2020, 268, 15–30. [Google Scholar] [CrossRef]
- Ng, M.; Wenden, E.; Lester, L.; Westgarth, C.; Christian, H. A mobile health intervention to encourage physical activity in children: A randomised controlled trial. BMC Pediatr. 2022, 22, 276. [Google Scholar] [CrossRef]
- Shin, H.; Kim, S.K.; Lee, M. Mobile phone interventions to improve adolescents’ physical health: A systematic review and meta-analysis. Public Health Nurs. 2019, 36, 787–799. [Google Scholar] [CrossRef]
- Tripicchio, G.L.; Kay, M.; Herring, S.; Cos, T.; Bresnahan, C.; Gartner, D.; Sosinsky, L.S.; Bass, S.B. Development and preliminary feasibility of iByte4Health: A mobile health (mHealth) pediatric obesity prevention intervention to engage parents with low-income of children 2–9 years. Nutrients 2021, 13, 4240. [Google Scholar] [CrossRef]
- Callender, C.; Thompson, D. Text messaging based obesity prevention program for parents of pre-adolescent African American girls. Children 2017, 4, 105. [Google Scholar] [CrossRef]
- Maher, C.A.; Davis, C.R.; Curtis, R.G.; Short, C.E.; Murphy, K.J. A physical activity and diet program delivered by artificially intelligent virtual health coach: Proof-of-concept study. JMIR mHealth uHealth 2020, 8, e17558. [Google Scholar] [CrossRef]
- To, Q.; Green, C.; Vandelanotte, C. Feasibility, usability and effectiveness of a machine learning based physical activity chatbot: A quasi-experimental study. JMIR mHealth uHealth 2021, 9, e28577. [Google Scholar] [CrossRef]
- Meltzer, L.J.; Montgomery-Downs, H.E. Sleep in the family. Pediatr. Clin. North Am. 2011, 58, 765–774. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| N (Families) | 19 | |
| Parental age, M (SD) | 38.4 (4.8) | |
| Child age, M (SD) | 7.6 (1.4) | |
| Parental role, n (%) | ||
| Mother | 16 (84.2) | |
| Father | 3 (15.8) | |
| Parental education, n (%) | ||
| 13+ years | 14 (73.7) | |
| 0–12 years | 5 (26.3) | |
| Parental employment status, n(%) | ||
| Employed | 15 (78.9) | |
| Unemployed | 4 (21.1) | |
| Parental ethnicity, n(%) | ||
| Caucasian | 18 (94.7) | |
| Asian | 1 (5.3) | |
| Location, n (%) | ||
| Rural/Regional area | 17 (89.5) | |
| Major city | 2 (10.5) | |
| Number of children enrolled in the intervention, n (%) | ||
| One child | 10 (52.6) | |
| Two children | 9 (47.4) | |
| Physical activity increases postintervention, n (%) | ||
| In at least one parent within the family | 12 (63.16) | |
| In at least one child within the family | 15 (78.9) | |
| In at least one member within the family | 16 (84.2) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schoeppe, S.; Waters, K.; Salmon, J.; Williams, S.L.; Power, D.; Alley, S.; Rebar, A.L.; Hayman, M.; Duncan, M.J.; Vandelanotte, C. Experience and Satisfaction with a Family-Based Physical Activity Intervention Using Activity Trackers and Apps: A Qualitative Study. Int. J. Environ. Res. Public Health 2023, 20, 3327. https://doi.org/10.3390/ijerph20043327
Schoeppe S, Waters K, Salmon J, Williams SL, Power D, Alley S, Rebar AL, Hayman M, Duncan MJ, Vandelanotte C. Experience and Satisfaction with a Family-Based Physical Activity Intervention Using Activity Trackers and Apps: A Qualitative Study. International Journal of Environmental Research and Public Health. 2023; 20(4):3327. https://doi.org/10.3390/ijerph20043327
Chicago/Turabian StyleSchoeppe, Stephanie, Kim Waters, Jo Salmon, Susan L. Williams, Deborah Power, Stephanie Alley, Amanda L. Rebar, Melanie Hayman, Mitch J. Duncan, and Corneel Vandelanotte. 2023. "Experience and Satisfaction with a Family-Based Physical Activity Intervention Using Activity Trackers and Apps: A Qualitative Study" International Journal of Environmental Research and Public Health 20, no. 4: 3327. https://doi.org/10.3390/ijerph20043327