
Correlation between Generic and Disease-Specific Quality of Life Questionnaires in Patients with Venous Ulcerations: A Cross-Sectional Study Carried out in a Primary Health Care Setting in Brazil
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Aspects
2.2. Study Design and Location
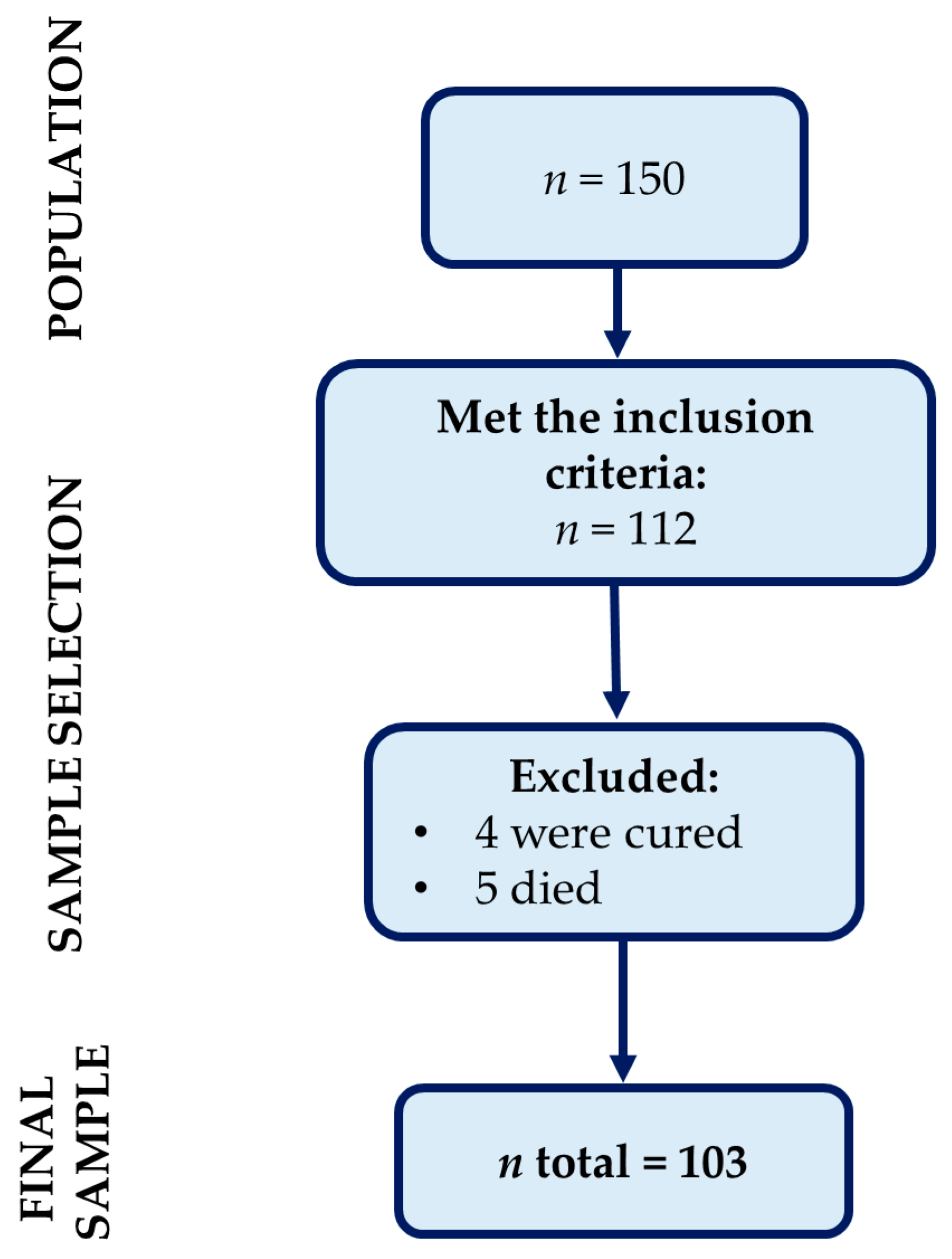
2.3. Population and Sample
2.4. Instruments and Variables
2.5. Data collection and Availability
2.6. Analysis and Data Processing
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singh, A.; Zahra, F. Chronic Venous Insufficiency; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Mansilha, A.; Sousa, J. Pathophysiological Mechanisms of Chronic Venous Disease and Implications for Venoactive Drug Therapy. Int. J. Mol. Sci. 2018, 19, 1669. [Google Scholar] [CrossRef] [Green Version]
- Chi, Y.W.; Raffetto, J.D. Venous leg ulceration pathophysiology and evidence based treatment. Vasc. Med. 2015, 20, 168–181. [Google Scholar] [CrossRef]
- Eberhardt, R.T.; Raffetto, J.D. Chronic venous insufficiency. Circulation 2014, 130, 333–346. [Google Scholar] [CrossRef]
- Folguera-Alvarez, C.; Garrido-Elustondo, S.; Rico-Blazquez, M.M.; Esparza-Garrido, M.I.; Verdu-Soriano, J.; Grupo, E.; Grupo, E. Effectiveness of double-layered compression therapy against crepe bandage for healing venous ulcers in primary care. Randomized clinical trial. Aten. Primaria 2020, 52, 712–721. [Google Scholar] [CrossRef]
- Rabe, E.; Pannier, F. Societal costs of chronic venous disease in CEAP C4, C5, C6 disease. Phlebology 2010, 25 (Suppl. S1), 64–67. [Google Scholar] [CrossRef]
- Barnsbee, L.; Cheng, Q.; Tulleners, R.; Lee, X.; Brain, D.; Pacella, R. Measuring costs and quality of life for venous leg ulcers. Int. Wound J. 2019, 16, 112–121. [Google Scholar] [CrossRef] [Green Version]
- Davies, A.H. The Seriousness of Chronic Venous Disease: A Review of Real-World Evidence. Adv. Ther. 2019, 36, 5–12. [Google Scholar] [CrossRef]
- The World Health Organization Quality of Life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [CrossRef]
- Cheng, Q.; Kularatna, S.; Lee, X.J.; Graves, N.; Pacella, R.E. Comparison of EQ-5D-5L and SPVU-5D for measuring quality of life in patients with venous leg ulcers in an Australian setting. Qual. Life Res. 2019, 28, 1903–1911. [Google Scholar] [CrossRef]
- Ciconelli, R.M.; Ferraz, M.B.; dos Santos, W.S.; Meinão, I.M.; Quaresma, M.R. Traducao para a lingua portuguesa e validacao do questionario generico de avaliacao de qualidade de vida SF-36 (Brasil SF-36). Rev. Bras. Reumatol. 1999, 39, 143–150. [Google Scholar]
- Couto, R.C.; Leal, F.J.; Pitta, G.B.B.; Andreoni, S. Responsiveness of the CCVUQ-Br quality of life questionnaire in chronic venous ulcer patients. J. Vasc. Bras. 2020, 19, e20190047. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, S.R.S.; Perico, L.A.D.; Dias, V. The complexity of the work of nurses in Primary Health Care. Rev. Bras. Enferm. 2018, 71, 704–709. [Google Scholar] [CrossRef] [Green Version]
- Homs-Romero, E.; Romero-Collado, A.; Verdu, J.; Blanch, J.; Rascon-Hernan, C.; Marti-Lluch, R. Validity of Chronic Venous Disease Diagnoses and Epidemiology Using Validated Electronic Health Records From Primary Care: A Real-World Data Analysis. J. Nurs. Scholarsh. 2021, 53, 296–305. [Google Scholar] [CrossRef]
- Torres, S.; Araujo, R.O.E.; Costa, I.K.F.; Tiburcio, M.P.; Sousa, A.J.G.; Pergola-Marconato, A.M.; Mansano-Schlosser, T.C.; Salvetti, M.G.; Mendes, F.R.P.; Torres, G.V.; et al. Health-related quality of life in patients with venous leg ulcer treated in primary care in Brazil and Portugal. PLoS ONE 2018, 13, e0195990. [Google Scholar] [CrossRef]
- Dias, T.Y.; Costa, I.K.; Melo, M.D.; Torres, S.M.; Maia, E.M.; Torres Gde, V. Quality of life assessment of patients with and without venous ulcer. Rev. Lat. Am. Enfermagem. 2014, 22, 576–581. [Google Scholar] [CrossRef] [Green Version]
- Couto, R.C.; Leal, F.J.; Pitta, G.B.B. Validation of the Portuguese language version of a chronic venous ulcer quality of life questionnaire (Charing Cross Venous Ulcer Questionnaire—CCVUQ-Brazil). J. Vasc. Bras. 2016, 15, 4–10. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: London, UK, 1988. [Google Scholar]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef] [Green Version]
- Zulec, M.; Rotar Pavlic, D.; Zulec, A. The Effect of an Educational Intervention on Self-Care in Patients with Venous Leg Ulcers-A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 4657. [Google Scholar] [CrossRef]
- Phillips, C.J.; Humphreys, I.; Thayer, D.; Elmessary, M.; Collins, H.; Roberts, C.; Naik, G.; Harding, K. Cost of managing patients with venous leg ulcers. Int. Wound J. 2020, 17, 1074–1082. [Google Scholar] [CrossRef]
- Joaquim, F.L.; Silva, R.; Garcia-Caro, M.P.; Cruz-Quintana, F.; Pereira, E.R. Impact of venous ulcers on patients’ quality of life: An integrative review. Rev. Bras. Enferm. 2018, 71, 2021–2029. [Google Scholar] [CrossRef]
- Park, S.H. Tools for assessing fall risk in the elderly: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2018, 30, 1–16. [Google Scholar] [CrossRef]
- Jebril, W.; Nowak, M.; Palin, L.; Nordgren, M.; Bachar-Wikstrom, E.; Wikstrom, J.D. Topical oxygen treatment relieves pain from hard-to-heal leg ulcers and improves healing: A case series. J. Wound Care 2022, 31, 4–11. [Google Scholar] [CrossRef]
- Moscicka, P.; Cwajda-Bialasik, J.; Szewczyk, M.T.; Jawien, A. Healing Process, Pain, and Health-Related Quality of Life in Patients with Venous Leg Ulcers Treated with Fish Collagen Gel: A 12-Week Randomized Single-Center Study. Int. J. Environ. Res. Public Health 2022, 19, 7108. [Google Scholar] [CrossRef]
- Kreiss, C.; Schnell, T. Have a good day! An experience-sampling study of daily meaningful and pleasant activities. Front. Psychol. 2022, 13, 977687. [Google Scholar] [CrossRef]
- Folguera-Alvarez, C.; Garrido-Elustondo, S.; Rico-Blazquez, M.; Verdu-Soriano, J. Factors Associated With the Quality of Life of Patients With Venous Leg Ulcers in Primary Care: Cross-Sectional Study. Int. J. Low Extrem. Wounds 2022, 21, 521–528. [Google Scholar] [CrossRef]
- Abelyan, G.; Abrahamyan, L.; Yenokyan, G. A case-control study of risk factors of chronic venous ulceration in patients with varicose veins. Phlebology 2018, 33, 60–67. [Google Scholar] [CrossRef]
- Melikian, R.; O’Donnell, T.F., Jr.; Suarez, L.; Iafrati, M.D. Risk factors associated with the venous leg ulcer that fails to heal after 1 year of treatment. J. Vasc. Surg. Venous Lymphat. Disord. 2019, 7, 98–105. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Variables | n | % | p |
|---|---|---|---|
| Gender | |||
| Female | 75 | 72.8 | <0.001 |
| Male | 28 | 27.2 | |
| Age group | |||
| ≥60 years | 64 | 62.1 | 0.014 |
| <60 years | 39 | 37.9 | |
| Marital status | |||
| Single/widowed/divorced | 53 | 51.5 | 0.078 |
| Married/stable union | 50 | 48.5 | |
| Income | |||
| ≤1 minimum wage * | 85 | 82.5 | <0.001 |
| >1 and <3 minimum wage | 15 | 14.6 | |
| ≥3 minimum wage | 3 | 2.9 | |
| Occupation | |||
| Not active | 82 | 79.6 | <0.001 |
| Active | 21 | 20.4 | |
| Education | |||
| Elementary school or less | 82 | 79.6 | <0.001 |
| High school or more | 21 | 20.4 |
| Scales of QV | Mean (SD) | Percentiles | p * | α ** | ||
|---|---|---|---|---|---|---|
| 25 | 50 | 75 | ||||
| SF-36 (n = 103) | ||||||
| Domains | 0.68 | |||||
| Physical role functioning | 8.1 (17.8) | 0.0 | 0.0 | 5.0 | <0.001 | |
| Physical functioning | 8.2 (27.0) | 0.0 | 0.0 | 0.0 | <0.001 | |
| Pain | 25.0 (19.4) | 10.0 | 20.0 | 40.0 | <0.001 | |
| Social role functioning | 30.0 (21.9) | 12.5 | 37.5 | 37.5 | <0.001 | |
| Emotional role functioning | 48.5 (29.8) | 33.3 | 66.6 | 66.6 | <0.001 | |
| General health perceptions | 51.6 (14.2) | 45.0 | 55.0 | 60.0 | <0.001 | |
| Vitality | 52.1 (11.9) | 45.0 | 50.0 | 60.0 | 0.002 | |
| Mental health | 57.4 (8.2) | 52.0 | 56.0 | 64.0 | <0.001 | |
| Total score | 35.2 (9.2) | 27.9 | 33.6 | 40.7 | 1.000 | |
| Dimensions | ||||||
| Physical health | 29.0 (9.2) | 23.0 | 27.0 | 33.0 | <0.001 | |
| Mental health | 48.1 (9.6) | 40.7 | 48.0 | 40.7 | 1.000 | |
| CCVUQ (n = 103) | 0.89 | |||||
| Cosmesis division | 48.6 (18.6) | 33.4 | 48.5 | 63.5 | 0.196 | |
| Emotional status division | 54.3 (20.1) | 37.8 | 57.5 | 60.4 | 0.280 | |
| Social interaction division | 58.4 (20.1) | 43.6 | 65.3 | 71.8 | <0.001 | |
| Domestic activities division | 63.4 (20.4) | 49.9 | 71.3 | 83.1 | <0.001 | |
| Overall | 54.5 (15.6) | 44.6 | 56.0 | 66.7 | 1.000 | |
| Scales of QV | CCVUQ | ||||
|---|---|---|---|---|---|
| Domestic Activities Division | Social Interaction Division | Cosmesis Division | Emotional Status Division | Overall | |
| SF-36 | r * (p **) | r (p) | r (p) | r (p) | r (p) |
| Domains | |||||
| Physical role functioning | −0.50 (<0.001) | −0.43 (<0.001) | −0.15 (0.143) | −0.16 (0.103) | −0.34 (<0.001) |
| Physical functioning | −0.31 (0.001) | −0.42 (<0.001) | −0.19 (0.056) | −0.20 (0.039) | −0.30 (0.002) |
| Vitality | −0.29 (0.003) | −0.29 (0.003) | −0.32 (<0.001) | −0.36 (<0.001) | 0.39 (<0.001) |
| Mental health | 0.06 (0.530) | −0.21 (0.030) | −0.27 (0.006) | −0.27 (0.005) | −0.27 (0.006) |
| Pain | 0.37 (<0.001) | 0.29 (0.003) | 0.16 (0.098) | 0.21 (0.029) | 0.30 (0.002) |
| Emotional role functioning | 0.29 (0.003) | 0.19 (0.058) | 0.45 (<0.001) | 0.49 (<0.001) | 0.47 (<0.001) |
| Social role functioning | 0.20 (0.043) | 0.21 (0.036) | 0.13 (0.193) | 0.16 (0.108) | 0.23 (0.020) |
| General health perceptions | 0.25 (0.010) | 0.30 (0.002) | 0.15 (0.137) | 0.16 (0.111) | 0.26 (0.007) |
| Total score | 0.17 (0.088) | 0.03 (0.740) | 0.12 (0.229) | 0.17 (0.090) | 0.17 (0.079) |
| Dimensions | |||||
| Physical health | −0.10 (0.300) | −0.17 (0.088) | −0.22 (0.025) | −0.21 (0.036) | −0.19 (0.055) |
| Mental health | 0.28 (0.004) | 0.18 (0.062) | 0.26 (0.008) | 0.30 (0.002) | 0.33 (0.001) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Oliveira Viana Pereira, D.M.; de Souza Oliveira, A.C.; de Oliveira Júnior, S.A.; Jacinto, M.A.G.; Dionísio, A.J.; Lima, A.E.O.; da Silva Dantas, B.A.; de Oliveira Sousa, S.L.; Martínez, C.S.G.; de Vasconcelos Torres, G. Correlation between Generic and Disease-Specific Quality of Life Questionnaires in Patients with Venous Ulcerations: A Cross-Sectional Study Carried out in a Primary Health Care Setting in Brazil. Int. J. Environ. Res. Public Health 2023, 20, 3583. https://doi.org/10.3390/ijerph20043583
de Oliveira Viana Pereira DM, de Souza Oliveira AC, de Oliveira Júnior SA, Jacinto MAG, Dionísio AJ, Lima AEO, da Silva Dantas BA, de Oliveira Sousa SL, Martínez CSG, de Vasconcelos Torres G. Correlation between Generic and Disease-Specific Quality of Life Questionnaires in Patients with Venous Ulcerations: A Cross-Sectional Study Carried out in a Primary Health Care Setting in Brazil. International Journal of Environmental Research and Public Health. 2023; 20(4):3583. https://doi.org/10.3390/ijerph20043583
Chicago/Turabian Stylede Oliveira Viana Pereira, Dalyanna Mildred, Adriana Catarina de Souza Oliveira, Severino Azevedo de Oliveira Júnior, Maria Angélica Gomes Jacinto, Alessandra Justino Dionísio, Alana Ellen Oliveira Lima, Bruno Araújo da Silva Dantas, Silvana Loana de Oliveira Sousa, Carmelo Sergio Gómez Martínez, and Gilson de Vasconcelos Torres. 2023. "Correlation between Generic and Disease-Specific Quality of Life Questionnaires in Patients with Venous Ulcerations: A Cross-Sectional Study Carried out in a Primary Health Care Setting in Brazil" International Journal of Environmental Research and Public Health 20, no. 4: 3583. https://doi.org/10.3390/ijerph20043583