
Effectiveness of the Ponseti Method in the Treatment of Clubfoot: A Systematic Review

 , and
, and
Abstract
:1. Introduction
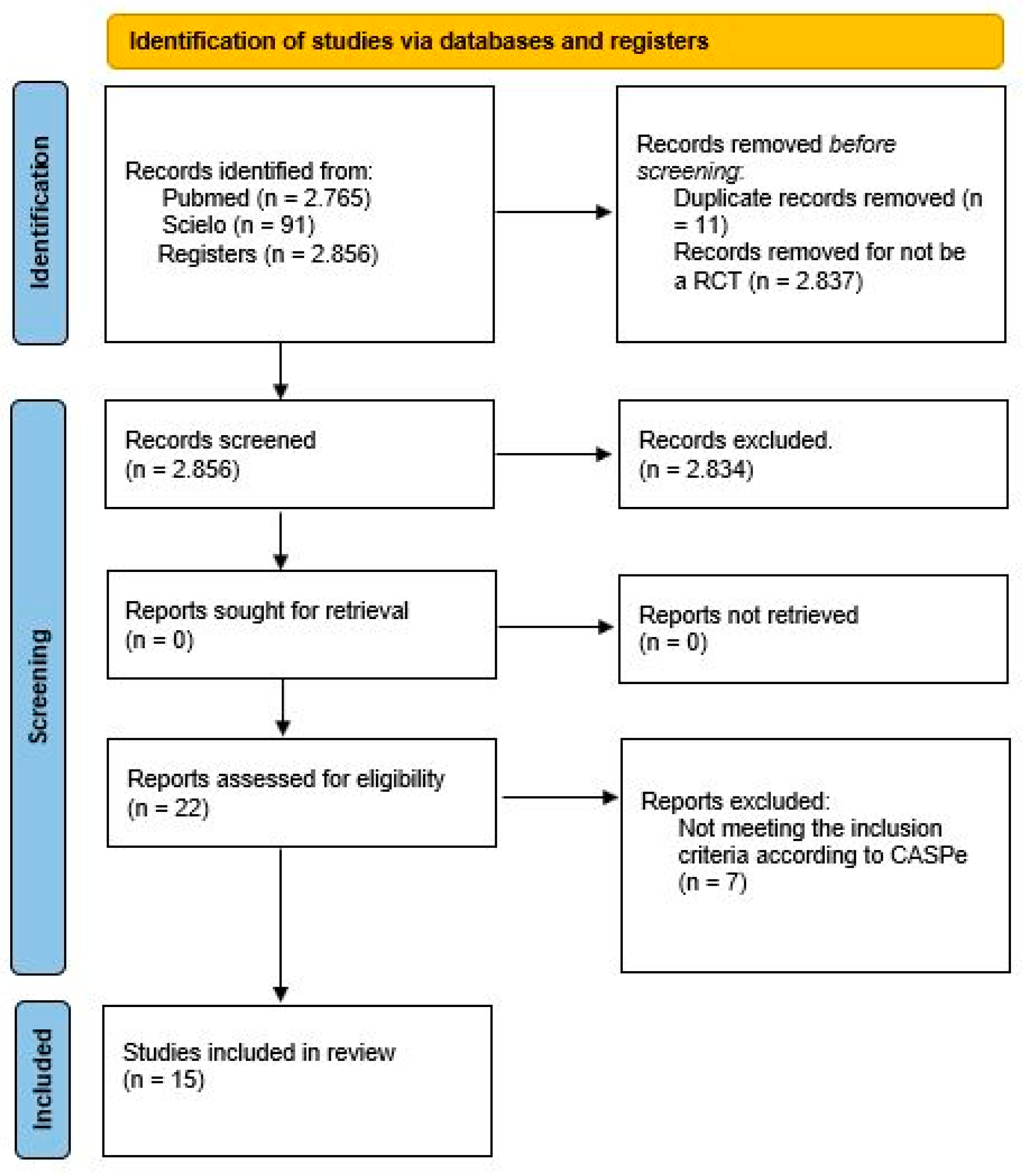
2. Materials and Methods
- Stress radiography in the assessment of residual deformity in clubfoot following postero-medial soft tissue release.
- Correcting congenital talipes equinovarus in children using three different corrective methods.
- Evaluación ultrasonográfica del tendón de Aquiles en niños con pie equino varo aducto congénito posterior a tenotomía de Aquiles con el método de Ponseti. Seguimiento a 12 semanas.
- Are scoring systems useful for predicting results of treatment for clubfoot using the Ponseti method?
- Ultrasonographic aspects of the Achilles tendon after tenotomy for the treatment of congenital clubfoot by the Ponseti technique.
- Does the presence of clubfoot delay the onset of walking?
- Ponseti method in Brazil: first ten years of a clubfoot website—users profile.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sanghvi, A.; Mittal, V. Conservative Management of Idiopathic Clubfoot: Kite versus Ponseti Method. J. Orthop. Surg. 2009, 17, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Chueire, A.J.F.G.; Carvalho Filho, G.; Kobayashi, O.Y.; Carrenho, L. Treatment of congenital clubfoot using Ponseti method. Rev. Bras. Ortop. 2016, 51, 313–318. [Google Scholar] [CrossRef] [Green Version]
- Hui, C.; Joughin, E.; Nettel-Aguirre, A.; Goldstein, S.; Harder, J.; Kiefer, G.; Parsons, D.; Brauer, C.; Howard, J. Comparison of cast materials for the treatment of congenital idiopathic clubfoot using the Ponseti method: A prospective randomized controlled trial. Can. J. Surg. 2014, 57, 247–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Changulani, M.; Rajagopal, T.; Bass, A. Treatment of idopathic club foot using the ponseti method: Initial experience. J. Bone Jt. Surg. 2006, 88, 1385–1387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaqueto, P.A.; Martins, G.S.; Mennucci, F.S.; Bittar, C.K.; Zabeu, J.L.A. Functional and clinical results achieved in congenital clubfoot patients treated by Ponseti’s technique. Rev. Bras. Ortop. 2016, 51, 657–661. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.S.; Masood, Q.M.; Bashir, A.; Shah, F.Y.; Halwai, M.A. Results of a Standard versus an Accelerated Ponseti Protocol for Clubfoot: A Prospective Randomized Study. Clin. Orthop. Surg. 2020, 12, 100. [Google Scholar] [CrossRef] [PubMed]
- Garcia, L.C.; Jesus, L.R.D.; Trindade, M.D.O.; Garcia Filho, F.C.; Pinheiro, M.L.; Sá, R.J.P.D. Evaluation of kite and Ponseti methods in the treatment of idiopathic congenital clubfoot. Acta Ortop. Bras. 2018, 26, 366–369. [Google Scholar] [CrossRef] [PubMed]
- Lara, L.C.R.; Neto, D.J.C.M.; Prado, F.R.; Barreto, A.P. Treatment of idiopathic congenital clubfoot using the Ponseti method: Ten years of experience. Rev. Bras. Ortop. 2013, 48, 362–367. [Google Scholar] [CrossRef] [Green Version]
- Matuszewski, Ł.; Gil, L.; Karski, J. Early results of treatment for congenital clubfoot using the Ponseti method. Eur. J. Orthop. Surg. Traumatol. 2012, 22, 403–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sud, A.; Tiwari, A.; Sharma, D.; Kapoor, S. Ponseti’s vs. Kite’s method in the treatment of clubfoot-a prospective randomised study. Int. Orthop. 2008, 32, 409–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alves, C.; Escalda, C.; Fernandes, P.; Tavares, D.; Neves, C.M. Ponseti Method: Does Age at the Beginning of Treatment Make a Difference? Clin. Orthop. 2009, 467, 1271–1277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zwick, E.B.; Kraus, T.; Maizen, C.; Steinwender, G.; Linhart, W.E. Comparison of Ponseti versus Surgical Treatment for Idiopathic Clubfoot: A Short-term Preliminary Report. Clin. Orthop. 2009, 467, 2668–2676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aydin, B.K.; Sofu, H.; Senaran, H.; Erkocak, O.F.; Acar, M.A.; Kirac, Y. Treatment of Clubfoot with Ponseti Method Using Semirigid Synthetic Softcast. Medicine 2015, 94, e2072. [Google Scholar] [CrossRef] [PubMed]
- Firth, G.; Eltringham, M.; Shnier, G. Early results of the Ponseti technique for a clubfoot clinic in South Africa. SA Orthop. J. 2009, 8, 67–71. [Google Scholar]
- Gintautienė, J.; Čekanauskas, E.; Barauskas, V.; Žalinkevičius, R. Comparison of the Ponseti method versus early tibialis anterior tendon transfer for idiopathic clubfoot: A prospective randomized study. Medicina 2016, 52, 163–170. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Pirani Classification System | |
|---|---|
| 6 Clinical Signs are Measured as 0 (Normal), 0.5 (Moderately Normal) and 1 (Severe) | |
| MIDFOOT GRADUATION | HINDFOOT GRADUATION |
| There are 3 clinical signs | There are 3 clinical signs |
| (maximum 3 points) | (maximum 3 points) |
|
|
|
|
|
|
| Methodology | |||||
|---|---|---|---|---|---|
| PubMed | Ponseti method | Free full text 269 results | Randomized controlled trial | 9 results | 5 articles chosen |
| PubMed | Clubfoot | Free full text 832 results | Randomized controlled trial | 11 results | 6 articles chosen |
| SciELO | Clubfoot | Without filter | 57 results | 9 articles chosen | |
| PubMed | Pes equinovarus | Free full text 815 results | Randomized controlled trial | 11 results | 0 articles chosen |
| SciELO | Ponseti Method | Without filter | 17 results | 2 articles chosen | |
| SciELO | Pes equinovarus | Without filter | 12 results | 0 articles chosen | |
| SciELO | Pie zambo | Without filter | 5 results | 0 articles chosen | |
| PubMed | Congenital talipes equinovarus | Free full text 849 results | Randomized controlled trial | 11 results | 0 articles chosen |
| Title | CASPe Score | Results |
|---|---|---|
| Stress radiography in the assessment of residual deformity in clubfoot following postero-medial soft tissue release. | 5/11 | Eliminate |
| Treatment of idiopathic clubfoot using the Ponseti method. | 10/11 | Acceptable |
| Ponseti vs. Kite’s method in the treatment of clubfoot—a prospective randomised study. | 10/11 | Acceptable |
| Ponseti Method Does Age at the Beginning of Treatment Make a Difference? | 9/11 | Acceptable |
| Comparison of Ponseti versus surgical treatment for idiopathic clubfoot. | 9/11 | Acceptable |
| Early results of the Ponseti technique for a clubfoot clinic in South Africa. | 9/11 | Acceptable |
| Conservative management of idiopathic clubfoot: Kite versus Ponseti method. | 10/11 | Acceptable |
| Early results of treatment for congenital clubfoot using the Ponseti method. | 9/11 | Acceptable |
| Treatment of idiopathic congenital clubfoot using the Ponseti method: ten years of experience. | 10/11 | Acceptable |
| Comparison of cast materials for the treatment of congenital idiopathic clubfoot using the Ponseti method: a prospective randomized controlled trial. | 10/11 | Acceptable |
| Treatment of clubfoot with ponseti method using semirigid synthetic softcast. | 11/11 | Acceptable |
| Correcting congenital talipes equinovarus in children using three different corrective methods. | 5/11 | Eliminate |
| Functional and clinical results achieved in congenital clubfoot patients treated by Ponseti’s technique. | 8/11 | Acceptable |
| Comparison of the Ponseti method versus early tibialis anterior tendon transfer for idiopathic clubfoot: A prospective randomized study. | 10/11 | Acceptable |
| Treatment of congenital clubfoot using Ponseti method. | 9/11 | Acceptable |
| Evaluación ultrasonográfica del tendón de Aquiles en niños con pie equino varo aducto congénito posterior a tenotomía de Aquiles con el método de Ponseti. Seguimiento a 12 semanas. | 4/11 | Eliminate |
| Are scoring systems useful for predicting results of treatment for clubfoot using the Ponseti method? | 5/11 | Eliminate |
| Ultrasonographic aspects of the Achilles tendon after tenotomy for the treatment of congenital clubfoot by the Ponseti technique. | 0/11 | Eliminate |
| Evaluation of kite and Ponseti methods in the treatment of idiopathic congenital clubfoot. | 10/11 | Acceptable |
| Results of a standard versus an accelerated Ponseti protocol for clubfoot: a prospective randomized study. | 11/11 | Acceptable |
| Does the presence of clubfoot delay the onset of walking? | 5/11 | Eliminate |
| Ponseti method in Brazil: first ten years of a clubfoot website—users profile. | 0/11 | Eliminate |
| Title | Author | Year | Type of Study | Sample (N) | Duration of Study | Results |
|---|---|---|---|---|---|---|
| Treatment of idiopathic clubfoot using the Ponseti method | Changulani et al. [4] | 2006 | Randomized controlled trial | 66 patients (100 clubfoot) | 2 years | The use of the Ponseti method, which is a simple and effective method to treat congenital idiopathic clubfoot, led to the prevention of surgery in up to 89% of cases. |
| Ponseti vs. Kite’s method in the treatment of clubfoot—a prospective randomised study | Sud et al. [10] | 2008 | Randomized controlled trial | 45 patients (67 clubfoot) | 1 year | It was found that the correction of clubfoot was significantly improved with the Ponseti method (with fewer days and fewer casts) as compared to the Kite method. |
| Ponseti Method Does Age at the Beginning of Treatment Make a Difference? | Alves et al. [11] | 2009 | Randomized controlled trial | 68 patients (102 clubfoot) | 2 years | All feet (100%) were initially corrected and no feet required extensive surgery, regardless of age, at start of treatment. There were no differences between Groups I and II in the number of casts, tenotomies, success in terms of rate of initial correction, recurrence rate and tibial transfer rate previous. The rate of extensive surgery avoidance when using the Ponseti method was 100% in Groups I and II; relapses occurred in 8% of feet in young and older children. |
| Comparison of Ponseti versus Surgical treatment for idiopathic clubfoot | Zwick et al. [12] | 2009 | Randomized controlled trial | 19 patients (28 clubfoot) | 3 years and a half | In the group for which the Ponseti method was performed, better results were obtained; no patient had foot pain or plantigrade feet. |
| Early results of the Ponseti technique for a clubfoot clinic in South Africa | Firth et al. [14] | 2009 | Randomized controlled trial | 70 patients (106 clubfoot) | 6 years | The Ponseti technique led to good results for clubfoot, but no significant differences were found between the group that received previous treatment and the group that did not. |
| Conservative management of idiopathic clubfoot: Kite versus Ponseti method | Sanghvi y Mittal [1] | 2009 | Randomized controlled trial | 42 patients (64 clubfoot) | 3 years | The results obtained with the Kite and Ponseti methods were similar (79% vs. 87%). With the Ponseti method, the number of casts was significantly lower, as well as the time needed to achieve correction, and a greater maximum ankle dorsiflexion was obtained. |
| Early results of treatment for congenital clubfoot using the Ponseti method | Matuszewski et al. [9] | 2011 | Randomized controlled trial | 35 patients (47 clubfoot) | 4 years | All patients achieved satisfactory results, and there have not been any known recurrences. |
| Treatment of idiopathic congenital clubfoot using the Ponseti method: ten years of experience | Lara et al. [8] | 2013 | Randomized controlled trial | 155 patients (229 clubfoot) | 10 years | The Ponseti method was used in both groups and correction was achieved, but in the group with younger patients, the results were more satisfactory and fewer casts were used. |
| Comparison of cast materials for the treatment of congenital idiopathic clubfoot using the Ponseti method: a prospective randomized controlled trial | Hui et al. [3] | 2014 | Randomized controlled trial | 30 patients (44 clubfoot) | 2 years and a half | When performing the Ponseti method, there were no significant differences when using different materials in the mean number of casts needed to correct clubfoot. |
| Treatment of clubfoot with Ponseti method using semirigid synthetic softcast | Aydin et al. [13] | 2015 | Randomized controlled trial | 196 patients (249 clubfoot) | 1 year | There were no significant differences in the results of the Ponseti method when using the classical material (POP) or using a semirigid synthetic soft cast. |
| Functional and clinical results achieved in congenital clubfoot patients treated by Ponseti’s technique | Jaqueto et al. [5] | 2016 | Randomized controlled trial | 31 patients (51 clubfoot) | 5 years and a half | The Ponseti method offered functional and clinical efficacy in patients with a success rate of 90.2% and an improvement in the Pirani classification values. |
| Comparison of the Ponseti method versus early tibialis anterior tendon transfer for idiopathic clubfoot: A prospective randomized study | Gintautiene et al. [15] | 2016 | Randomized controlled trial | 39 patients (55 clubfoot) | 2 years | An early transfer of the tibialis anterior tendon allowed a reduction in the duration of the use of the orthosis and led to the same results as with the Ponseti method. However, a less significant difference in dorsiflexion of the foot was observed in those patients who underwent a tibialis anterior tendon transfer. |
| Treatment of congenital clubfoot using Ponseti method | Chueire et al. [2] | 2016 | Randomized controlled trial | 26 patients (39 clubfoot) | 4 years | The Ponseti method offered good clubfoot results with fewer soft tissue injuries. |
| Evaluation of Kite and Ponseti methods in the treatment of idiopathic congenital clubfoot | García et al. [7] | 2018 | Randomized controlled trial | 100 patients (127 clubfoot) | 1 year and 4 months | It was shown that the efficacy of the treatment with the Ponseti method was higher than with the Kite method. |
| Results of a standard versus an accelerated Ponseti protocol for clubfoot: A prospective randomized study | Islam et al. [6] | 2020 | Randomized controlled trial | 100 patients (158 clubfoot) | 1 year | The data suggest that performing the accelerated Ponseti technique, that is, changing casts twice a week, reduces immobilization time without affecting the final results and is as safe and effective as the traditional Ponseti method. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Carrero, E.; Castillo-López, J.M.; Medina-Alcantara, M.; Domínguez-Maldonado, G.; Garcia-Paya, I.; Jiménez-Cebrián, A.M. Effectiveness of the Ponseti Method in the Treatment of Clubfoot: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 3714. https://doi.org/10.3390/ijerph20043714
López-Carrero E, Castillo-López JM, Medina-Alcantara M, Domínguez-Maldonado G, Garcia-Paya I, Jiménez-Cebrián AM. Effectiveness of the Ponseti Method in the Treatment of Clubfoot: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(4):3714. https://doi.org/10.3390/ijerph20043714
Chicago/Turabian StyleLópez-Carrero, Elena, José Manuel Castillo-López, Miguel Medina-Alcantara, Gabriel Domínguez-Maldonado, Irene Garcia-Paya, and Ana María Jiménez-Cebrián. 2023. "Effectiveness of the Ponseti Method in the Treatment of Clubfoot: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 4: 3714. https://doi.org/10.3390/ijerph20043714