




The Influence of Ventilation Measures on the Airborne Risk of Infection in Schools: A Scoping Review

 , , , and
, , , and
Abstract
1. Introduction
2. Methods
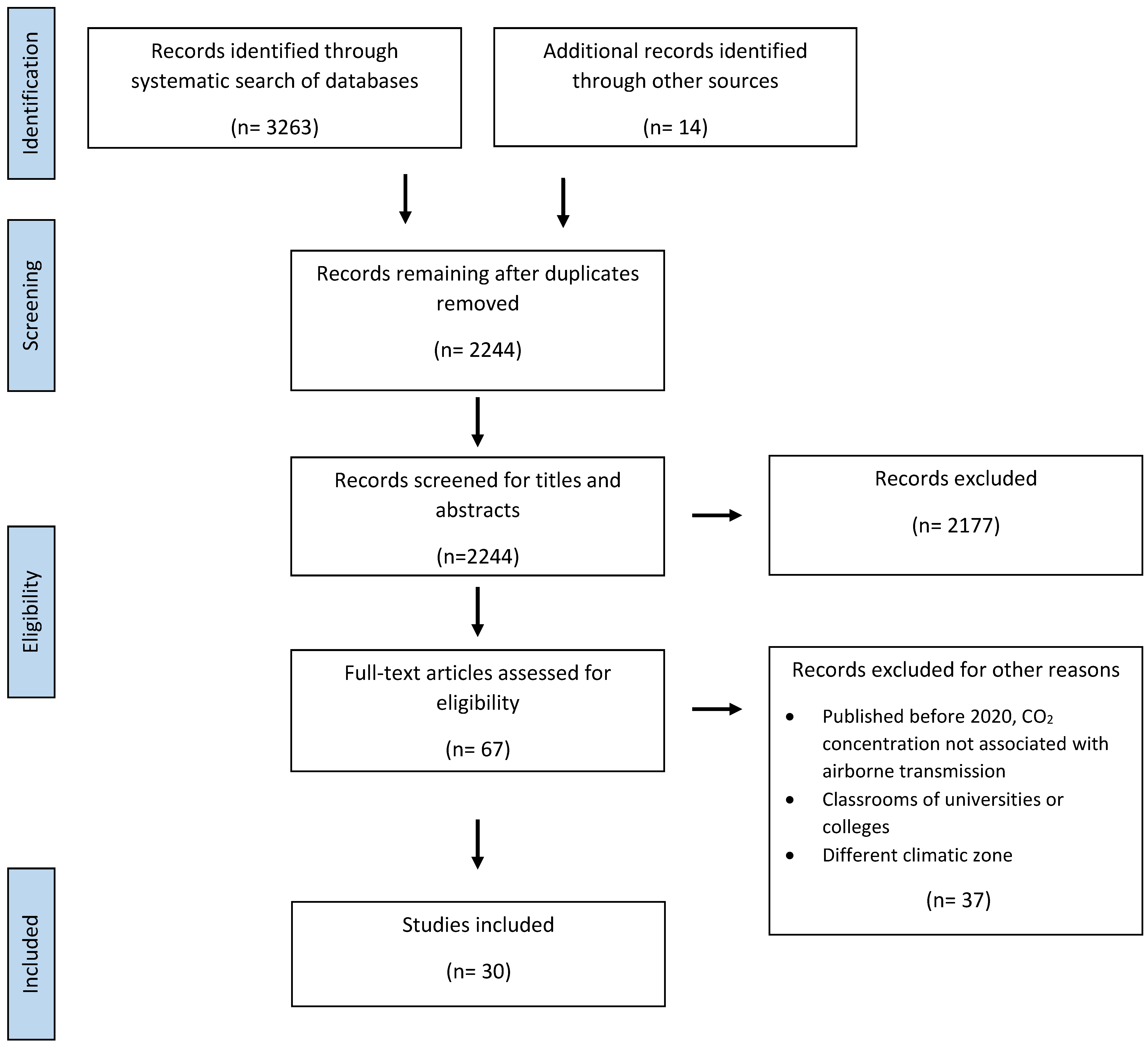
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection and Structuring
3. Results

{kind=link}
| Reference | Study Type | Setting | Methods | Primary Endpoint | Main Results | Side Effects |
|---|---|---|---|---|---|---|
| [24] | Intervention study | 11 classrooms, (9 pre-school, primary and secondary schools), Italy, Jan–Feb 2021 | NV regime. Questionnaire to evaluate occupancy and general ventilation behavior. (1) Control: ventilation as usual. (2) Intervention: door always open, windows open for 10 min during break and when CO2 conc. reaches 700 ppm. Additional measures: use of hand sanitizer, cleaning of surfaces, wearing masks, keeping distance. | CO2 concen-tration | (1) Mean CO2 conc.: 721–1325 ppm. 54% of the classrooms had mean CO2 conc. > 1000 ppm. Maximum CO2 conc.: 867–3947 ppm. (2) 91% of classrooms had mean CO2 conc. < 1000 ppm, 36% had CO2 conc. < 700 ppm. Real time visualization of CO2 conc. better than merely following systematic ventilation protocols. In some classrooms, improved NV was not adequate to achieve good air quality because of structural building elements. | Low temperatures despite the use of radiators |
| [35] | Intervention study | 4 classrooms, 1 elementary school, Denmark, 2 weeks in Mar-Apr 2011 and Jun 2011 each | Visual CO2 feedback, colors representing specific CO2 conc. indicating the need to ventilate (NV). Building with mixing-type MV system. In half of the classrooms the MV system was turned off during season when rooms are heated, measurements were performed one week with visual feedback alternating with one week without visual feedback in all classrooms (cross-over method). During season when rooms are cooled, measurements were performed for 2 weeks either with or without visual feedback in each half of the classrooms. | CO2 concen-tration | Before the intervention: CO2 maximum values up to 1500 ppm. During heating season: windows opened more often and CO2 conc. were lower in intervention group with visual feedback (below or around 1000 ppm vs. conc. up to around 1900 ppm in control group). In the cooling season: no difference in the frequency of opening windows with the visual feedback in classrooms and without mechanical cooling. In classrooms with mechanical cooling, windows were opened more often when visual feedback was used. | Estimated annual heating 15–23% higher, estimated annual cooling 18% lower in classrooms with visual CO2 feedback system. |
| [37] | Intervention study | 81 classrooms 20 primary schools, Netherlands, Oct–Dec 2004 and Jan–Mar 2005 | CO2 measurements taken before, immediately after, and 6 weeks after interventions: (1) Class-specific NV ventilation advice. (2) Class-specific advice and device warning (visual sign) when CO2 conc. > 1200 ppm. (3) Class-specific advice and teaching package. (4) Control group. | CO2 concen-tration | Before interventions: CO2 conc. > 1000 ppm in 64% of the school day. (1) No improvement of ventilation behavior significantly in the longer term. (2) In the short term fewest periods with CO2 conc. > 1000 ppm compared to other groups. (3) > (2) Long term improvement of ventilation situation, CO2 conc. > 1000 ppm in 40% of the school day. | |
| [38] | (1) Cross-sectional study (2) Intervention study | (1) 100 classrooms, 96 Swiss primary and low secondary schools(2) 19 (+4) classrooms, during season when rooms are heated | (1) Standard ventilation as usual, NV in 94% of classrooms. (2.1) Strategic NV during breaks and before/after lessons (rooms unoccupied). Written and oral instructions to teach ventilation behavior. Interactive simulation tool to develop ventilation plan used in 4 classes to develop specific ventilation strategy. (2.2) Control group: Same 19 classrooms as (1) with previous measurements. | CO2 concen-tration | Average percentage of lessons with CO2 conc. < 1000 ppm increased from 18% to 42% as a result of intervention. (1) More than 2/3 of classrooms had CO2 conc. > 2000 ppm. MV: Median CO2 conc.: 686–1320 ppm; maximum median: 1364 ppm. NV: Median CO2 conc.: 862–2898 ppm; maximum median: 2754 ppm. (2.1) Median CO2 conc.: 1097 ppm; median maximum conc. decreased to 1892 ppm. (2.2) Median CO2 conc.: 1600 ppm. Higher CO2 conc. with the number of consecutive lessons in (1) and (2). | |
| [46] | Intervention study | 18 classrooms, 17 primary schools, Netherlands periods when rooms were heated, 2010–2012 | (1) Intervention group (12 classrooms): week 1: standard ventilation; week 2/3: ventilation with mobile MV device; target CO2 conc.: 800 or 1200 ppm for 1 week at a time, cross-over design. Preheated outside air was introduced and air was recirculated. (2) Control group (6 class-rooms): NV, no specific ventilation strategy. | CO2 concen-tration | (1) Mean CO2 conc.: 1399 ppm (SD: 350) in week 1, decreased in week 2 and 3 to mean CO2 conc. of 841 ppm (SD: 65, target set 800 ppm) and mean CO2 conc. of 975 ppm (SD: 73, target set 1200 ppm). More stable CO2 conc. (2) Week 1: mean CO2 conc. 1208 ppm (SD: 244); week 2/3: mean CO2 conc. 1350 (SD: 486). | |
| [34] | Intervention study | 10,441 classrooms, 1419 schools, Italy, September 2021–January 2022 | 316 classrooms in 56 schools with MV (single room ventilation units, most with filters and heat recovery), 205,247 students. Additional measures (masks, distancing, increased NV). MV turned on before start of school, operating throughout school day. Maximum air flow rates 100–1000 m3 h−1 corresponding to VRs per person of 1.4–14 L s−1 student −1. (1) Intervention: Installation of MVS in classrooms (2) Classrooms with NV. Extrapolation of temporal exposure from regional weekly SARS-CoV-2 incidence; relative risk reduction correlated with presence of MVSs in classrooms. | SARS-CoV-2 infection of clusters of cases (≥2 cases until December 2021; ≥3 from January 2022) | (1) 31 infected students (2) 3090 infected students in clusters. Monthly incidence proportion (IP = number of cases/1000 students): increased from 13 September to 23 December 2021 and especially from 7–31 January 2022 (Omicron), lower values in MV classrooms (4.9. vs. 15.3 in NV). Incidence proportion ratio (IPR = ratio between IP in classrooms with and without MV): 0.32. Protective effect of MV greater with higher regional incidence. Greater relative risk reduction (RRR) with higher ventilation rate. In the most conservatively calculated scenario: in total 74% RRR with MV vs. NV; 80% RRR with VR > 10–14 L s−1 student −1. For each additional unit of VR per person, the RRR ranged from 12–15%. This association was significant irrespective of occupancy, educational level, and location. |
| Reference | Study Type | Setting | Methods | Primary Endpoint | Main Results | Side Effects |
|---|---|---|---|---|---|---|
| [36] | Observational study | (1) 9 secondary schools, Spain, December 2020–January 2021. (2) 3 classrooms, 1 secondary school, heating period before and during pandemic. | (1) Survey/interviews on (building) characteristics, heating consumption and thermal comfort. (2) CO2 measurements. (1) and (2) During pandemic: Cross ventilation after each class or at the beginning of the day, during 30 min break, at end of day, and sometimes during classes. Before pandemic: brief individual ventilation periods. | CO2 concen-tration | (2) Reduction of mean CO2 conc. from 2478 ppm (SD: 852) to 1105 ppm (SD 295). The increase of CO2 conc. during school hours decreased from 857 ppm per hour to 135 ppm per hour. CO2 conc. fluctuated less. | (1) and (2) Mean indoor temperature: 18 °C, decrease of 2 °C. Increased heating use 9–40%. |
| [44] | Observational study | 3 classrooms, 1 primary school, Germany Apr–May 2022 | NV for 5 min every 20 min during lessons vs. no ventilation. Reduced occupancy. | CO2 concen-tration | CO2 conc. < 1000 ppm can be achieved through natural cross ventilation. No ventilation: almost linear increase in CO2 conc. | |
| [47] | Observational study | 50 classrooms, 2 K-12 schools, USA, Jan–Mar 2021 | Measurement of CO2 conc. after controlled release in different scenarios. | CO2 concen-tration | Increase of ACH, especially with natural cross ventilation. ACH > 5/h in 90% of classrooms with ventilation vs. ACH < 3/h without ventilation. | |
| [48] | Observational study | 19 classrooms, 7 pre-school, primary or secondary schools, Spain, Sept–Oct 2020 | Measurement with natural cross ventilation continuously during classes and breaks. In some classes, masks were worn. 1 room equipped with additional MV. | CO2 concen-tration | 26% of the classrooms had CO2 conc. > 700 ppm. Better ventilation in preschools: average CO2 conc. 553 ppm, SD 56, max. 1075 ppm. Primary schools: average CO2 conc. 602 ppm, SD 109, max. 1341 ppm. Secondary schools: average CO2 conc. 699 ppm, SD 172, max. 2117 ppm. | |
| [39] | Observational study | 9 classes, 1 classroom, 1 secondary school in Latvia, September 2020 | NV. CO2 measurements during teaching hours and breaks, additional questionnaire. No details about frequency or duration of ventilation. Students usually remained in classrooms during breaks. | CO2 concen-tration | Average CO2 conc. about 2380 ppm, maximum 4424 ppm. Higher CO2 conc. in 3rd and 4th periods, probably due to shorter breaks in the morning. During breaks, CO2 conc. decreased slightly and increased rapidly after breaks. | Average temperature 22 °C, min: 18.5 °C. |
| [49] | Observational study | 2 classrooms, 1 elementary school, Spain, (1) Jan–Mar 2020 before pandemic (2) Nov 2020–Jan 2021 | MV system, measurement of CO2 concentration. (1) Sometimes additional NV. (2) MV sometimes turned off, continuous NV following COVID-19 protocols. | CO2 concen-tration | (1) Mean CO2 conc. 1033 ppm (range 618–1571) or 1079 ppm (range 530–1726) in both classrooms. (2) CO2 conc. 604 ppm (range 466–781) or 740 ppm (range 514–1177). | (2) Lower indoor temperature, more frequent thermal discomfort |
| [50] | Observational study | 2 classrooms, 1 school, Germany, heating period before and during pandemic | Measurements without ventilation and after opening of up to 5 windows and door (NV). | CO2 concen-tration | CO2 conc. ranging between 2500–2800 ppm after a school lesson with no specific ventilation. After several minutes of NV, CO2 conc. around 1000 ppm. | |
| [51] | Observational Study | 2 K-12 schools, USA, fall 2020 | Detection of SARS-CoV-2 cases in 2 schools after implementation of various mitigation strategies (e.g., MERV filters, increased ventilation, social distancing, routine testing, masks). No direct comparison of the effect of the different strategies. | SARS-CoV-2 infection | School A: 109 positive cases (4.9%), R0 0.49; school B: 25 positive cases (2.0%), R0 0.02. 9% of cases responsible for identified clusters. 72% of the cases transmitted in school were associated with noncompliance, many cases of transmission outside school setting. | |
| [52] | Observational study, outbreak analysis | 1 secondary school, Germany, 2020 | Analysis of an outbreak after schools reopened after the first lockdown. Examination of causes and course (clinical, contact, laboratory data, WGS analysis). Students did not wear masks, teachers sometimes wore masks. | SARS-CoV-2 infection | A teacher was identified as the index case, subsequently 31 students, 2 teachers and 3 household contacts were infected. Most infections were in connection with 2 lessons of the index case (1 building, rooms of possible transmission were all located on two floors). Limited ventilation, narrow sanitary facilities, 1 crowded classroom. | |
| [17] | Observational study, outbreak analysis | 1 elementary school, upstate New York, USA, 1974 | Analysis of a large measles outbreak, investigation of the impact of vaccination and ventilation. School equipped with 2 ventilation systems. Air is recirculated after filtration. | Measles Infection | 97% of the children were vaccinated. Index case infected 28 other students, 60 children were subsequently infected. Recirculation of the virus by the ventilation system augmented transmission. The most important exposure sites were the same classroom as the infector(s), another classroom that used the same ventilation system, and school buses. | |
| [45] | Observational study/Case study | 1 school, Israel, May 2020 | Analysis of a SARS-CoV-2 outbreak in a school 10 days after reopening. Air conditioning systems in operation (separate for each classroom). | SARS-CoV-2 infection | 153 students (13.2%) and 25 staff members (16.6%) tested positive after detection of 2 positive index cases. Due to heatwave no masks worn, crowded classes (1.1–1.3 m2 per person), extra-curricular activities. Also contacts on way to school. | |
| [53] | Observational study, mathematical modeling study | 45 classrooms, 11 primary and secondary schools, England, Nov 2015–Mar 2020 | Hybrid ventilation systems. No specific ventilation strategy. CO2 measurement and calculation of infection risk and secondary infections, for two periods (5 days) in (1) Jan and (2) July 2018. | CO2 concen-tration, SARS-CoV-2 infection risk | (1) Average CO2 conc. around 1500 ppm, short periods with max. conc. > 2000 ppm. (2) CO2 conc. half of those in (1) due to warmer temperatures and increased ventilation. Infection risk in (1) about twice that in (2). Variations of secondary infections between the classrooms, even those using the same ventilation system. | |
| [54] | (1) Observational study (2) mathematical modeling study | 4 classrooms, 2 high schools, Italy, winter 2015/2016 | (1) NV with different ventilation scenarios (2) Simulation: MV with different ACH, normal occupancy. Recommended CO2 conc.: max. 700 ppm higher than outdoor concentration. | CO2 concentration, SARS-CoV-2 infection risk | (1) Frequent, short ventilation periods efficiently reduce CO2 conc., but recommended maximum conc. were not guaranteed permanently. Rapid decrease/increase of CO2 conc. during/after ventilation. Maximum CO2 conc.: 5136 ppm (school 1). Continuous increase up to 4680 ppm without ventilation (school 2). Infection risk > 1% even when using additional filtering methods.(2) higher ACH reduced infection risk from 23% (8 L s−1 person−1) to 7.2% (32 L s−1 person−1) with additional filtration (efficiency 95%): 0.38%. | Decrease of indoor temperature, thermal discomfort. Energy consumption can be reduced up to 72% using a “High Energy Air Handling Unit“ with thermal recovery. |
| [30] | Observational study, mathematical modeling study | 101 classrooms, 19 elementary schools, USA, Dec 2017–Sept 2018 | CO2 conc. were measured during the heating and the cooling seasons. MV in 37% of the schools. 18% had either no windows or windows that could not be opened. Certain ventilation strategies were not applied. | CO2 concentration, SARS-CoV-2 transmission risk | No significant differences in CO2 conc. between cooling (mean 990, range 430–2200 ppm) and heating seasons (mean 980 ppm, range 510–1900 ppm). Transmission risk was higher during heating season (increase of 28%). It was lower in classrooms with MV (risk 0.059 vs. 0.081 in NV). Higher transmission risk from teacher to student (mean conc. 0.20/0.35) than from student to teacher (0.14/0.26) or from student to student (0.046/0.091) with mask/without mask. | |
| [55] | Observational study, mathematical modeling study | 3 classrooms, 1 elementary school, South Korea, May 2020 | Measurement of CO2 decay by cross vs. single-sided ventilation with 0%, 15%, 30% and 100% window opening ratio. Air conditioner in operation during ventilation (set at 25 °C). Measurements when unoccupied. Infection risk calculated for different scenarios with 0.5 h to 3 h exposure time. | CO2 concentration, SARS-CoV-2 infection risk | Cross ventilation resulted in higher average ventilation rates (6.38/h (15% opening ratio), 10.53/h (30% opening ratio), 22.39/h (100% opening ratio) than single-sided ventilation 2.13/h (15% opening ratio), 2.90/h (30% opening ratio). VR reduced when air conditioner in operation. Without ventilation, infection risk >1% even with mask and exposure time of 0.5 h. Infection risk <1% with cross ventilation without mask with 30% window opening and 1 h exposure. With single sided ventilation, infection risk of <1% can only be achieved with masks and exposure time of max. 1 h. | Possible risk of cross transmission with strong indoor airflow. 10.2% and 22.5% higher energy consumption (windows opening ratio 15% and 30% vs. 0%). |
| [22] | Mathematical modeling study Additional exemplary observation | 1 classroom, 1 high school, Italy, June 2021 | CO2 measurement and modeling of infection risk for different ventilation and room scenarios. NV primarily during breaks. Models with/without both masks and teacher’s use of a microphone. | CO2 concen-tration, SARS-CoV-2 infection risk | 70–80% reduction of infection risk in log scale by NV. Reduction in intensity with which teachers speak using a microphone: additional 20% risk reduction (without masks) almost 40% (with masks). Increasing total area of the classroom cuts infection risk almost in half. | |
| [56] | Survey, mathematical modeling study | 169 Elementary and K-5 schools, Georgia, USA Nov–Dec 2020 | Survey of different prevention strategies: increased NV, air filtration, masks, physical distancing, barriers on school desks, cohort size. Association of SARS-CoV-2 cases with prevention strategies was calculated. | SARS-CoV-2 infection | 35% lower incidence when schools improved their ventilation strategies, 48% reduction with combination of increased NV and air filtration/purification and 37% reduction when students and staff wore face masks. | |
| [57] | Mathematical modeling study | 111,485 public and private schools, USA | Estimation of occupant density in 1433 representative schools. Simulation of infection risk for two scenarios: one year pandemic scenario and epidemiological scenario, each with different infection prevention strategies. Assumed baseline ventilation rate: 2 ACH. | SARS-CoV-2 infection risk | 90% of schools with infection risk >1%; Dec: 6.83%, July: 3.85%. Infection risk can be lowered by 16.5% by increasing the VR from 2/h to 2.5/h and by 8% by increasing the VR from 5.5/h to 6/h. Reduction using (MERV13) filters and by reduction of occupancy. To achieve an infection risk <1%, a combination of intervention strategies is required. Effectiveness of prevention strategies depended on school characteristics and pandemic periods. | Increased energy costs when using better MERV filters or higher VRs. |
| [58] | Mathematical modeling study | Different indoor spaces, among others, K-12 schools | Modeling of SARS-CoV-2 infection risk in different locations with different indoor air quality (IAQ) strategies. | SARS-CoV-2 infection-/transmission risk | Higher probability (mean, SD) that teacher spreads virus (13.2%, 12.0) than student to student (3.8%, 3.6). Higher infection risk in dining areas (10.1%, 8.9) and gym (8.3%, 7.7) than in library (0.3%, 0.2) due to lower occupancy, relatively better ventilation. Reduction of infection risk: when doubling total supply airflow rate: 37% reduction, 100% outdoor air, or HEPA filter: 27% reduction, displacement ventilation: 26% reduction, partitions: 46% reduction, personal ventilation: 46% reduction. | High costs of implementation and maintaining certain IAQ strategies. |
| [59] | Mathematical modeling study | Various scenarios, including classrooms | Calculation of required VRs in order to obtain an infection risk of <1% for various scenarios. Typical classroom (348 m3) with exposure time of 2 h. | SARS-CoV-2 infection risk | Required VR per infector is 100–350 m3/h (0.25 h exposure time) and 1200–4000 m3/h (3 h exposure time) without masks and VR of 30–90 m3/h (0.25 h exposure time) and 300–1000 m3/h (3 h exposure time) with masks. For a typical classroom, ACH of 4.8–15/h or 1.2–3.5/h are necessary to obtain an infection risk <1% (without or with masks respectively). These VR can be achieved using a normal MV system or NV for all scenarios. | |
| [60] | Mathematical modeling study | Various spaces in public buildings, incl. school classrooms | Calculation of the infection probability for specific rooms and calculation of VR required to achieve a specific probability of infection (with and without masks). | SARS-CoV-2 infection risk | Lower infection probability is easier to achieve in larger rooms, but usually there are more susceptible persons present. Example classrooms: 32 m2, AER 3.68/h, infection probability 0.034. 48 m2, AER: 4.48/h, infection probability 0.019. The total flow rate per infected person is essential in order to reduce the probability of infection. | Increased energy consumption (for MV). |
| [61] | Mathematical modeling study | Typical classroom, 1 high-school | Simulation of different scenarios (e.g., different infectors, intensity of speaking) with 1 infector and only airborne virus transmission using MV or NV. Calculation of required AER and ventilation procedures to obtain a transmission <1 during lessons, corresponding to an individual 4.2% risk of infection. 5 h school time. | CO2 concen-tration, SARS-CoV-2 and seasonal influenza infection risk | CO2 conc. reaches an equilibrium of 750 ppm after 30 min (MV, AER 9.5/h). A maximum CO2 concentration as indicator of transmission can be misrepresentative (due to dynamics). Required AER needed to prevent a seasonal influenza infection: <0.1/h, achieved for all scenarios; to prevent a SARS-CoV-2 infection: 9.5/h and 0.8/h (teacher infector, 60 min loud speaking vs. muted speaking through microphone). Required AER (student as infector) dependent on speaking/breathing time and attendance in classes: 0.8–3.5/h. Long ventilation periods or high AER sometimes not realizable with NV. With NV useful to apply a feedback control strategy with continuous CO2 measurements and adjusted ventilation times. | |
| [16] | Mathematical modeling study based on measurements in real classes | 21 classrooms, 1 elementary school (including 2 kindergarten classrooms), Taiwan | Mechanical fans in elementary school classrooms, air conditioning system in kindergarten classrooms. No mention of additional NV. Class duration 40 min with 5–10 min breaks. | Pandemic influenza transmission risk, infection risk | Elementary school children have an infection probability of 0.56–0.64 and R0 values between 16.11–16.09 (age-dependent). Staff (25–45 years of age) have an infection risk of 0.07 and R0 of 2.80. The transmission potential can be reduced by implementing a higher ACH: R0 = 11.38/7.10/5.10/9.97 for 0.5/1/1.5/2/h ACH for kindergarten children. Vaccination as the most effective measure, combination of measures further reduce transmission risk. | |
| [62] | Mathematical modeling study | Primary and secondary schools, USA | Combination of a multi-zone Wells-Riley model, nationwide representative school building archetype model (with basic infection control scenario, regular and advanced ventilation-related control scenario) and a Monte-Carlo Simulation for estimating transmission risk. Estimates were validated with real outbreak data. | Measles transmission risk | Transmission risk 74 times higher for unvaccinated students, higher in high schools than in elementary schools (median 5.8% and 3.8% respectively). Schools with ductless systems without air filters have the highest transmission risk (median 6.0%), schools with ductless systems with air filters have the lowest (median: 3.7%). Using a better filter reduced transmission risk for unvaccinated students (45% for MERV8, 32% for MERV13, and 29% for HEPA filter, median values). Increasing ventilation rates decreased transmission risk for unvaccinated students (46% basic control scenario, 38% regular, 33% advanced infection control scenario). |
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Statistisches_Bundesamt. 2022. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bildung-Forschung-Kultur/Schulen/_inhalt.html (accessed on 17 June 2022).
- WHO. WHO Director-General’s Opening Remarks at the Mission Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19--11-march-2020 (accessed on 17 August 2022).
- Otte Im Kampe, E.; Lehfeld, A.S.; Buda, S.; Buchholz, U.; Haas, W. Surveillance of COVID-19 school outbreaks, Germany, March to August 2020. Euro. Surveill. 2020, 25, 2001645. [Google Scholar] [CrossRef] [PubMed]
- Kuhfeld, M.; Soland, J.; Tarasawa, B.; Johnson, A.; Ruzek, E.; Liu, J. Projecting the Potential Impact of COVID-19 School Closures on Academic Achievement. Educ. Res. 2020, 49, 549–565. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- UNESCO. Adverse Consequences of School Closures. Available online: https://en.unesco.org/covid19/educationresponse/consequences (accessed on 11 August 2022).
- ECDC. COVID-19 in Children and the Role of School Settings in Transmission—Second Update. 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/children-and-school-settings-covid-19-transmission (accessed on 11 August 2022).
- van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Wang, C.C.; Prather, K.A.; Sznitman, J.; Jimenez, J.L.; Lakdawala, S.S.; Tufekci, Z.; Marr, L.C. Airborne transmission of respiratory viruses. Science 2021, 373, 6558. [Google Scholar] [CrossRef]
- Guo, Z.-D.; Wang, Z.-Y.; Zhang, S.-F.; Li, X.; Li, L.; Li, C.; Cui, Y.; Fu, R.-B.; Dong, Y.-Z.; Chi, X.-Y.; et al. Aerosol and Surface Distribution of Severe Acute Respiratory Syndrome Coronavirus 2 in Hospital Wards, Wuhan, China, 2020. Emerg. Infect. Dis. 2020, 26, 1583–1591. [Google Scholar] [CrossRef]
- Morawska, L.; Cao, J. Airborne transmission of SARS-CoV-2: The world should face the reality. Environ. Int. 2020, 139, 105730. [Google Scholar] [CrossRef]
- Hartmann, A.; Lange, J.; Rotheudt, H.; Kriegel, M. Emissionsrate und Partikelgröße von Bioaerosolen beim Atmen, Sprechen und Husten; Technische Universität Berlin: Berlin, Germany, 2020. [Google Scholar] [CrossRef]
- ECDC. Factsheet for health Professionals on Coronaviruses European Centre for Disease Prevention and Control. 2022. Available online: https://www.ecdc.europa.eu/en/factsheet-health-professionals-coronaviruses (accessed on 17 June 2022).
- Birmili, W.; Selinka, H.C.; Moriske, H.J.; Daniels, A.; Straff, W. Ventilation Concepts in Schools for the Prevention of Transmission of Highly Infectious Viruses (SARS-CoV-2) by Aerosols in Indoor air. Bundesgesundheitsblatt Gesundh. Gesundh. 2021, 64, 1570–1580. [Google Scholar] [CrossRef]
- Coleman, K.K.; Sigler, W.V. Airborne Influenza A Virus Exposure in an Elementary School. Sci. Rep. 2020, 10, 1859. [Google Scholar] [CrossRef]
- Chen, S.C.; Liao, C.M. Modelling control measures to reduce the impact of pandemic influenza among schoolchildren. Epidemiol. Infect. 2008, 136, 1035–1045. [Google Scholar] [CrossRef]
- Riley, R.L.; Riley, E.C.; Murphy, G. Airborne Spread of Measles in a Suburban Elementary-School. Am. Rev. Respir. Dis. 1978, 117, 255. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Ma, Y.; Lu, Q.; Sun, J.; Pei, Y. An outbreak of pulmonary tuberculosis and a follow-up investigation of latent tuberculosis in a high school in an eastern city in China, 2016–2019. PLoS ONE 2021, 16, e0247564. [Google Scholar] [CrossRef] [PubMed]
- Somsen, G.A.; van Rijn, C.; Kooij, S.; Bem, R.A.; Bonn, D. Small droplet aerosols in poorly ventilated spaces and SARS-CoV-2 transmission. Lancet Respir. Med. 2020, 8, 658–659. [Google Scholar] [CrossRef]
- Megahed, N.A.; Ghoneim, E.M. Indoor Air Quality: Rethinking rules of building design strategies in post-pandemic architecture. Environ. Res. 2021, 193, 110471. [Google Scholar] [CrossRef] [PubMed]
- Baloch, R.M.; Maesano, C.N.; Christoffersen, J.; Banerjee, S.; Gabriel, M.; Csobod, É.; de Oliveira Fernandes, E.; Annesi-Maesano, I. Indoor Air Pollution, Physical and Comfort Parameters Related to Schoolchildren’s Health: Data from the European SINPHONIE Study. Sci. Total Environ. 2020, 739, 139870. [Google Scholar] [CrossRef]
- Zivelonghi, A.; Lai, M. Mitigating aerosol infection risk in school buildings: The role of natural ventilation, volume, occupancy and CO2 monitoring. Build. Environ. 2021, 204, 108139. [Google Scholar] [CrossRef]
- Shendell, D.G.; Prill, R.; Fisk, W.J.; Apte, M.G.; Blake, D.; Faulkner, D. Associations between classroom CO2 concentrations and student attendance in Washington and Idaho. Indoor Air 2004, 14, 333–341. [Google Scholar] [CrossRef]
- Di Gilio, A.; Palmisani, J.; Pulimeno, M.; Cerino, F.; Cacace, M.; Miani, A.; de Gennaro, G. CO2 concentration monitoring inside educational buildings as a strategic tool to reduce the risk of Sars-CoV-2 airborne transmission. Environ. Res. 2021, 202, 111560. [Google Scholar] [CrossRef]
- Rudnick, S.N.; Milton, D.K. Risk of indoor airborne infection transmission estimated from carbon dioxide concentration. Indoor Air 2003, 13, 237–245. [Google Scholar] [CrossRef]
- Peng, Z.; Jimenez, J.L. Exhaled CO2 as COVID-19 infection risk proxy for different indoor environments and activities. medRxiv 2021, 8, 392–397. [Google Scholar] [CrossRef]
- Ad-hoc-Arbeitsgruppe_Innenraumrichtwerte, Gesundheitliche Bewertung von Kohlendioxid in der Innenraumluft- Mitteilungen der Ad-hoc-Arbeitsgruppe Innenraumrichtwerte der Innenraumlufthygiene-Kommission des Umweltbundesamtes und der Obersten Landesgesundheitsbehörden. Bundesgesundheitsblatt Gesundh. Gesundh. 2018, 51, 1358–1369. [CrossRef]
- Pettenkofer, M.V. Über den Luftwechsel in Wohngebäuden; Cotta’sche Buchhandlung: Munich, Germany, 1858. [Google Scholar]
- Kriegel, M.; Hartmann, A.; Buchholz, U.; Seifried, J.; Baumgarte, S.; Gastmeier, P. SARS-CoV-2 Aerosol Transmission Indoors: A Closer Look at Viral Load, Infectivity, the Effectiveness of Preventive Measures and a Simple Approach for Practical Recommendations. Int. J. Environ. Res. Public Health 2021, 19, 220. [Google Scholar] [CrossRef] [PubMed]
- Pavilonis, B.; Ierardi, A.M.; Levine, L.; Mirer, F.; Kelvin, E.A. Estimating aerosol transmission risk of SARS-CoV-2 in New York City public schools during reopening. Environ. Res. 2021, 195, 110805. [Google Scholar] [CrossRef] [PubMed]
- Donovan, C.V.; Rose, C.; Lewis, K.N.; Vang, K.; Stanley, N.; Motley, M.; Brown, C.C.; Gray, F.J., Jr.; Thompson, J.W.; Amick, B.C.; et al. SARS-CoV-2 Incidence in K-12 School Districts with Mask-Required Versus Mask-Optional Policies—Arkansas, August-October 2021. MMWR Morb. Mortal Wkly. Rep. 2022, 71, 384–389. [Google Scholar] [CrossRef]
- Falk, A.; Benda, A.; Falk, P.; Steffen, S.; Wallace, Z.; Hoeg, T.B. COVID-19 Cases and Transmission in 17 K-12 Schools—Wood County, Wisconsin, August 31-November 29, 2020. MMWR Morb. Mortal Wkly Rep. 2021, 70, 136–140. [Google Scholar] [CrossRef]
- Robert-Koch-Institut. Die Impfung gegen COVID-19 in Deutschland zeigt eine hohe Wirksamkeit gegen SARS-CoV-2-Infektionen, Krankheitslast und Sterbefälle (Analyse der Impfeffekte im Zeitraum Januar bis Juli 2021). 2021. Available online: https://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2021/35/Art_01.html (accessed on 19 August 2022).
- Buonanno, G.; Ricolfi, L.; Morawska, L.; Stabile, L. Increasing ventilation reduces SARS-CoV-2 airborne transmission in schools: A retrospective cohort study in Italy’s Marche region. Front Public Health 2022, 10, 1087087. [Google Scholar] [CrossRef]
- Wargocki, P.; Da Silva, N.A. Use of visual CO2 feedback as a retrofit solution for improving classroom air quality. Indoor Air 2015, 25, 105–114. [Google Scholar] [CrossRef]
- Monge-Barrio, A.; Bes-Rastrollo, M.; Dorregaray-Oyaregui, S.; González-Martínez, P.; Martin-Calvo, N.; López-Hernández, D.; Arriazu-Ramos, A.; Sánchez-Ostiz, A. Encouraging natural ventilation to improve indoor environmental conditions at schools. Case studies in the north of Spain before and during COVID. Energy Build. 2022, 254, 111567. [Google Scholar] [CrossRef]
- Geelen, L.M.J.; Huijbregts, M.A.J.; Ragas, A.M.J.; Bretveld, R.W.; Jans, H.W.A.; van Doorn, W.J.; Evertz, S.J.C.J.; van der Zijden, A. Comparing the effectiveness of interventions to improve ventilation behavior in primary schools. Indoor Air 2008, 18, 416–424. [Google Scholar] [CrossRef]
- Vassella, C.C.; Koch, J.; Henzi, A.; Jordan, A.; Waeber, R.; Iannaccone, R.; Charriere, R. From spontaneous to strategic natural window ventilation: Improving indoor air quality in Swiss schools. Int. J. Hyg. Environ. Health 2021, 234, 113746. [Google Scholar] [CrossRef]
- Zemitis, J.; Bogdanovics, R.; Bogdanovica, S. The Study of CO2 Concentration in A Classroom During the COVID-19 Safety Measures. E3S Web. Conf. 2021, 246, 01004. [Google Scholar] [CrossRef]
- Rodríguez, D.; Urbieta, I.R.; Velasco, Á.; Campano-Laborda, M.; Jiménez, E. Assessment of indoor air quality and risk of COVID-19 infection in Spanish secondary school and university classrooms. Build. Environ. 2022, 226, 109717. [Google Scholar] [CrossRef] [PubMed]
- Scheff, P.A.; Paulius, V.K.; Huang, S.W.; Conroy, L.M. Indoor air quality in a middle school, Part I: Use of CO2 as a tracer for effective ventilation. Appl. Occup. Environ. Hyg. 2000, 15, 824–834. [Google Scholar] [CrossRef] [PubMed]
- Canha, N.; Mandin, C.; Ramalho, O.; Wyart, G.; Riberon, J.; Dassonville, C.; Hanninen, O.; Almeida, S.M.; Derbez, M. Assessment of ventilation and indoor air pollutants in nursery and elementary schools in France. Indoor Air 2016, 26, 350–365. [Google Scholar] [CrossRef] [PubMed]
- Canha, N.; Almeida, S.M.; Freitas, M.C.; Täubel, M.; Hänninen, O. Winter ventilation rates at primary schools: Comparison between Portugal and Finland. J. Toxicol. Environ. Health. A 2013, 76, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Duill, F.F.; Schulz, F.; Jain, A.; Krieger, L.; van Wachem, B.; Beyrau, F. The Impact of Large Mobile Air Purifiers on Aerosol Concentration in Classrooms and the Reduction of Airborne Transmission of SARS-CoV-2. Int. J. Environ. Res. Public Health 2021, 18, 11523. [Google Scholar] [CrossRef] [PubMed]
- Stein-Zamir, C.; Abramson, N.; Shoob, H.; Libal, E.; Bitan, M.; Cardash, T.; Cayam, R.; Miskin, I. A large COVID-19 outbreak in a high school 10 days after schools’ reopening, Israel, May 2020. Eurosurveillance 2020, 25, 2–6. [Google Scholar] [CrossRef]
- Rosbach, J.T.; Vonk, M.; Duijm, F.; van Ginkel, J.T.; Gehring, U.; Brunekreef, B. A ventilation intervention study in classrooms to improve indoor air quality: The FRESH study. Environ. Health 2013, 12, 110. [Google Scholar] [CrossRef]
- McNeill, V.F.; Corsi, R.; Huffman, J.A.; King, C.; Klein, R.; Lamore, M.; Maeng, D.Y.; Miller, S.L.; Ng, N.L.; Olsiewski, P.; et al. Room-level ventilation in schools and universities. Atmos. Environ. X 2022, 13, 100152. [Google Scholar] [CrossRef]
- Villanueva, F.; Notario, A.; Cabañas, B.; Martín, P.; Salgado, S.; Gabriel, M.F. Assessment of CO(2) and aerosol (PM(2.5), PM(10), UFP) concentrations during the reopening of schools in the COVID-19 pandemic: The case of a metropolitan area in Central-Southern Spain. Environ. Res. 2021, 197, 111092. [Google Scholar] [CrossRef]
- Alonso, A.; Llanos, J.; Escandón, R.; Sendra, J.J. Effects of the COVID-19 Pandemic on Indoor Air Quality and Thermal Comfort of Primary Schools in Winter in a Mediterranean Climate. Sustainability 2021, 13, 2699. [Google Scholar] [CrossRef]
- Curtius, J.; Granzin, M.; Schrod, J. Testing mobile air purifiers in a school classroom: Reducing the airborne transmission risk for SARS-CoV-2. Aerosol. Sci. Technol. 2021, 55, 586–599. [Google Scholar] [CrossRef]
- Gillespie, D.L.; Meyers, L.A.; Lachmann, M.; Redd, S.C.; Zenilman, J.M. The Experience of 2 Independent Schools with In-Person Learning During the COVID-19 Pandemic. J. Sch. Health 2021, 91, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Baumgarte, S.; Hartkopf, F.; Hölzer, M.; von Kleist, M.; Neitz, S.; Kriegel, M.; Bollongino, K. Investigation of a Limited but Explosive COVID-19 Outbreak in a German Secondary School. Viruses 2022, 14, 87. [Google Scholar] [CrossRef] [PubMed]
- Vouriot, C.V.M.; Burridge, H.C.; Noakes, C.J.; Linden, P.F. Seasonal variation in airborne infection risk in schools due to changes in ventilation inferred from monitored carbon dioxide. Indoor Air 2021, 31, 1154–1163. [Google Scholar] [CrossRef]
- Schibuola, L.; Chiara, T. High energy efficiency ventilation to limit COVID-19 contagion in school environments. Energy Build. 2021, 240, 110882. [Google Scholar] [CrossRef]
- Park, S.; Choi, Y.; Song, D.; Kim, E.K. Natural ventilation strategy and related issues to prevent coronavirus disease 2019 (COVID-19) airborne transmission in a school building. Sci. Total Environ. 2021, 789, 147764. [Google Scholar] [CrossRef]
- Gettings, J.; Czarnik, M.; Morris, E.; Haller, E.; Thompson-Paul, A.M.; Rasberry, C.; Lanzieri, T.M.; Smith-Grant, J.; Aholou, T.M.; Thomas, E.; et al. Mask Use and Ventilation Improvements to Reduce COVID-19 Incidence in Elementary Schools—Georgia, November 16-December 11, 2020. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 779–784. [Google Scholar] [CrossRef]
- Xu, Y.; Cai, J.; Li, S.; He, Q.; Zhu, S. Airborne infection risks of SARS-CoV-2 in U.S. schools and impacts of different intervention strategie. Sustain. Cities Soc. 2021, 74, 103188. [Google Scholar] [CrossRef]
- Shen, J.; Kong, M.; Dong, B.; Birnkrant, M.J.; Zhang, J. A systematic approach to estimating the effectiveness of multi-scale IAQ strategies for reducing the risk of airborne infection of SARS-CoV-2. Build. Environ. 2021, 200, 107926. [Google Scholar] [CrossRef]
- Dai, H.; Zhao, B. Association of the infection probability of COVID-19 with ventilation rates in confined spaces. Build. Simul. 2020, 13, 1321–1327. [Google Scholar] [CrossRef] [PubMed]
- Kurnitski, J.; Kiil, M.; Wargocki, P.; Boerstra, A.; Seppänen, O.; Olesen, B.; Morawska, L. Respiratory infection risk-based ventilation design method. Build. Environ. 2021, 206, 108387. [Google Scholar] [CrossRef] [PubMed]
- Stabile, L.; Pacitto, A.; Mikszewski, A.; Morawska, L.; Buonanno, G. Ventilation procedures to minimize the airborne transmission of viruses in classrooms. Build. Environ. 2021, 202, 108042. [Google Scholar] [CrossRef] [PubMed]
- Azimi, P.; Keshavarz, Z.; Cedeno Laurent, J.G.; Allen, J.G. Estimating the nationwide transmission risk of measles in US schools and impacts of vaccination and supplemental infection control strategies. BMC Infect. Dis. 2020, 20, 497. [Google Scholar]
- Clements-Croome, D.J.; Awbi, H.B.; Bakó-Biró, Z.; Kochhar, N.; Williams, M. Ventilation rates in schools. Build. Environ. 2008, 43, 362–367. [Google Scholar] [CrossRef]
- REHVA. CO₂ Monitoring and Indoor Air Quality. 2021. Available online: https://www.rehva.eu/rehva-journal/chapter/co2-monitoring-and-indoor-air-quality (accessed on 13 December 2022).
- The_Lancet_COVID-19_Commission. Proposed Non-infectious Air Delivery Rates (NADR) for Reducing Exposure to Airborne Respiratory Infectious Diseases. 2022. Available online: https://covid19commission.org/safe-work-travel (accessed on 18 January 2023).
- Umweltbundesamt. Anforderungen an Lüftungskonzeptionen in Gebäuden Teil I: Bildungseinrichtungen. 2017. Available online: https://www.umweltbundesamt.de/sites/default/files/medien/1410/publikationen/uba_empfehlungspapier_lueftung_unterrichtsgebaeude_final_bf.pdf (accessed on 18 January 2023).
- Bakó-Biró, Z.; Clements-Croome, D.J.; Kochhar, N.; Awbi, H.B.; Williams, M.J. Ventilation rates in schools and pupils’ performance. Build. Environ. 2012, 48, 215–223. [Google Scholar] [CrossRef]
- Haverinen-Shaughnessy, U.; Moschandreas, D.J.; Shaughnessy, R.J. Association between substandard classroom ventilation rates and students’ academic achievement. Indoor Air 2011, 21, 121–131. [Google Scholar] [CrossRef]
- Miranda, M.T.; Romero, P.; Valero-Amaro, V.; Arranz, J.I.; Montero, I. Ventilation conditions and their influence on thermal comfort in examination classrooms in times of COVID-19. A case study in a Spanish area with Mediterranean climate. Int. J. Hyg. Env. Health 2022, 240, 113910. [Google Scholar] [CrossRef]
- Kienbaum, T. Hygienemanagement in Gesundheitseinrichtungen Teil 4: Effektives Lüften während der Pandmie. Hygienemanagement 2020, 10, 47–58. [Google Scholar]
- Ferrari, S.; Blázquez, T.; Cardelli, R.; Puglisi, G.; Suárez, R.; Mazzarella, L. Ventilation strategies to reduce airborne transmission of viruses in classrooms: A systematic review of scientific literature. Build. Environ. 2022, 222, 109366. [Google Scholar] [CrossRef]
- REHVA. REHVA COVID19 Guidance version 4.1 How to operate HVAC and Other Building Service Systems to Prevent the Spread of the Coronavirus (SARS-CoV-2) Disease (COVID-19) in Workplaces. 2021. Available online: https://www.rehva.eu/fileadmin/user_upload/REHVA_COVID-19_guidance_document_V4.1_15042021.pdf (accessed on 10 November 2022).
- Laurent, M.R.; Frans, J. Monitors to improve indoor air carbon dioxide concentrations in the hospital: A randomized crossover trial. Sci. Total Environ. 2022, 806, 151349. [Google Scholar] [CrossRef] [PubMed]
- de la Hoz-Torres, M.L.; Aguilar, A.J.; Ruiz, D.P.; Martínez-Aires, M.D. Analysis of Impact of Natural Ventilation Strategies in Ventilation Rates and Indoor Environmental Acoustics Using Sensor Measurement Data in Educational Buildings. Sensors 2021, 21, 6122. [Google Scholar] [CrossRef] [PubMed]
- Korsavi, S.S.; Montazami, A.; Mumovic, D. Ventilation rates in naturally ventilated primary schools in the UK.; Contextual, Occupant and Building-related (COB) factors. Build. Environ. 2020, 181, 107061. [Google Scholar] [CrossRef]
- Aguilar, A.J.; de la Hoz-Torres, M.L.; Costa, N.; Arezes, P.; Martínez-Aires, M.D.; Ruiz, D.P. Assessment of ventilation rates inside educational buildings in Southwestern Europe: Analysis of implemented strategic measures. J. Build. Eng. 2022, 51, 104204. [Google Scholar] [CrossRef]
- Burgmann, S.; Janoske, U. Transmission and reduction of aerosols in classrooms using air purifier systems. Phys. Fluids 2021, 33, 033321. [Google Scholar] [CrossRef]
- Asadi, S.; Wexler, A.S.; Cappa, C.D.; Barreda, S.; Bouvier, N.M.; Ristenpart, W.D. Aerosol emission and superemission during human speech increase with voice loudness. Sci. Rep. 2019, 9, 2348. [Google Scholar] [CrossRef]
- Fleischer, M.; Schumann, L.; Hartmann, A.; Walker, R.S.; Ifrim, L.; von Zadow, D.; Luske, J.; Seybold, J.; Kriegel, M.; Murbe, D. Pre-adolescent children exhibit lower aerosol particle volume emissions than adults for breathing, speaking, singing and shouting. J. R. Soc. Interface 2022, 19, 20210833. [Google Scholar] [CrossRef]
- Murbe, D.; Kriegel, M.; Lange, J.; Schumann, L.; Hartmann, A.; Fleischer, M. Aerosol emission of adolescents voices during speaking, singing and shouting. PLoS ONE 2021, 16, e0246819. [Google Scholar] [CrossRef]
- Euser, S.; Aronson, S.; Manders, I.; van Lelyveld, S.; Herpers, B.; Sinnige, J.; Kalpoe, J.; van Gemeren, C.; Snijders, D.; Jansen, R.; et al. SARS-CoV-2 viral-load distribution reveals that viral loads increase with age: A retrospective cross-sectional cohort study. Int. J. Epidemiol. 2022, 50, 1795–1803. [Google Scholar] [CrossRef]
- Thompson, H.A.; Mousa, A.; Dighe, A.; Fu, H.; Arnedo-Pena, A.; Barrett, P.; Bellido-Blasco, J.; Bi, Q.; Caputi, A.; Chaw, L.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Setting-specific Transmission Rates: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2021, 73, e754–e764. [Google Scholar] [CrossRef]
- Viner, R.M.; Mytton, O.T.; Bonell, C.; Melendez-Torres, G.J.; Ward, J.; Hudson, L.; Waddington, C.; Thomas, J.; Russell, S.; van der Klis, F.; et al. Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared with Adults: A Systematic Review and Meta-analysis. JAMA Pediatr. 2021, 175, 143–156. [Google Scholar] [CrossRef]
- Zafarnejad, R.-G.; Paul, M. Assessing school-based policy actions for COVID-19: An agent-based analysis of incremental infection risk. Comput. Biol. Med. 2021, 134, 104518. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Li, Y.; Nielsen, P.V.; Wei, J.; Jensen, R.L. Short-range airborne transmission of expiratory droplets between two people. Indoor Air 2017, 27, 452–462. [Google Scholar] [CrossRef] [PubMed]
- Makris, R.; Tawackolian, K.; Lausch, K.; Kopic, C.; Kriegel, M. Near-Field Exposure of Pathogen-Laden Respiratory Particles Based on Statistical Evaluation of One Emitting Person Indoors. 2022. Available online: https://www.researchgate.net/publication/361312085_Near-field_exposure_of_pathogen-laden_respiratory_particles_based_on_statistical_evaluation_of_one_emitting_person_indoors (accessed on 17 June 2022).
- Gold, J.A.W.; Gettings, J.R.; Kimball, A.; Franklin, R.; Rivera, G.; Morris, E.; Scott, C.; Marcet, P.L.; Hast, M.; Swanson, M.; et al. Clusters of SARS-CoV-2 Infection Among Elementary School Educators and Students in One School District—Georgia, December 2020-January 2021. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.A.; Saliba, V.; Lopez Bernal, J.; Ramsay, M.E.; Ladhani, S.N. SARS-CoV-2 infection and transmission in educational settings: A prospective, cross-sectional analysis of infection clusters and outbreaks in England. Lancet Infect Dis. 2021, 21, 344–353. [Google Scholar] [CrossRef]
- Du, C.R.; Wang, S.C.; Yu, M.C.; Chiu, T.F.; Wang, J.Y.; Chuang, P.C.; Jou, R.; Chan, P.C.; Fang, C.T. Effect of ventilation improvement during a tuberculosis outbreak in underventilated university buildings. Indoor Air 2020, 30, 422–432. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jendrossek, S.N.; Jurk, L.A.; Remmers, K.; Cetin, Y.E.; Sunder, W.; Kriegel, M.; Gastmeier, P. The Influence of Ventilation Measures on the Airborne Risk of Infection in Schools: A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 3746. https://doi.org/10.3390/ijerph20043746
Jendrossek SN, Jurk LA, Remmers K, Cetin YE, Sunder W, Kriegel M, Gastmeier P. The Influence of Ventilation Measures on the Airborne Risk of Infection in Schools: A Scoping Review. International Journal of Environmental Research and Public Health. 2023; 20(4):3746. https://doi.org/10.3390/ijerph20043746
Chicago/Turabian StyleJendrossek, Sandra N., Lukas A. Jurk, Kirsten Remmers, Yunus E. Cetin, Wolfgang Sunder, Martin Kriegel, and Petra Gastmeier. 2023. "The Influence of Ventilation Measures on the Airborne Risk of Infection in Schools: A Scoping Review" International Journal of Environmental Research and Public Health 20, no. 4: 3746. https://doi.org/10.3390/ijerph20043746
APA StyleJendrossek, S. N., Jurk, L. A., Remmers, K., Cetin, Y. E., Sunder, W., Kriegel, M., & Gastmeier, P. (2023). The Influence of Ventilation Measures on the Airborne Risk of Infection in Schools: A Scoping Review. International Journal of Environmental Research and Public Health, 20(4), 3746. https://doi.org/10.3390/ijerph20043746