

Physicians’ Distress Related to Moral Issues and Mental Health In-Between Two Late Waves of COVID-19 Contagions

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Participants
- 23 medical specialists holding a staff position, who were aged 29 to 45 years (37.3 ± 4.8 years), with a mean in-hospital experience of 112 ± 58 months;
- 85 medical residents aged 26 to 44 years (28.6 ± 3.0 years), with a mean in-hospital experience of 30 ± 21 months. According to their experience during the pandemic, they were categorized into two groups: 58 residents who have been at the forefront of the medical care of patients with COVID-19 since the first wave of contagions (before vaccination started), who were aged 26 to 44 years (29.0 ± 3.3 years), and had a mean in-hospital experience of 38.7 ± 21.4 months; and 27 residents who participated in patient care since the third wave of contagions (after vaccination), in a variety of institutional hospitals, who were aged 26 to 33 years (27.2 ± 1.75 years), and had a mean in-hospital experience of 12.6 ± 0.9 months.
2.3. Procedures
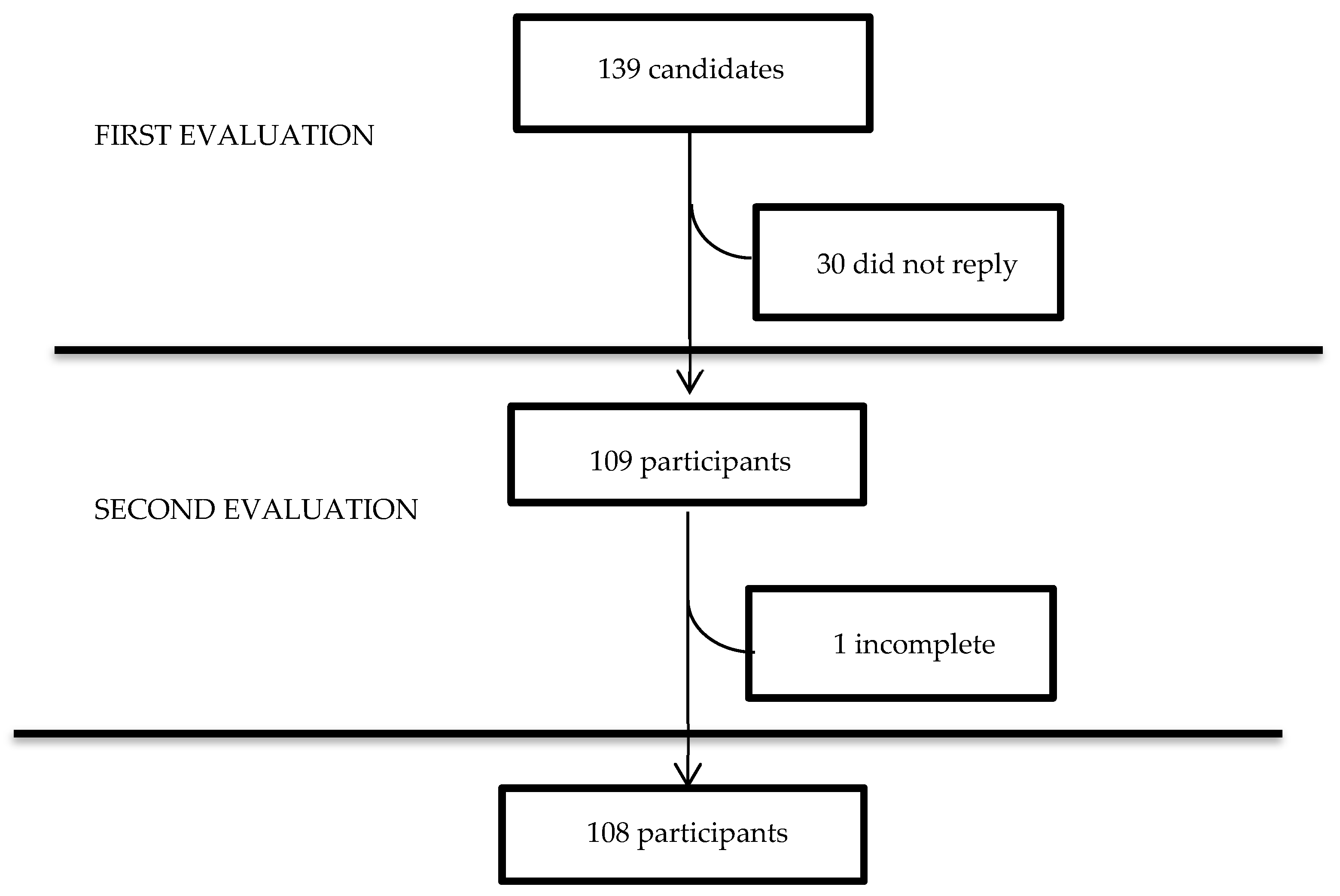
- The first evaluation was performed at the end of the fourth wave of contagions (April–May 2022), by the beginning of the residents’ academic year.
- The second evaluation was performed three months later, at the beginning of the fifth wave of contagions (July–August 2022).
- Sleep quality by the Pittsburg Sleep Quality Index [39];
- State Anxiety by the short version of the State-Trait Anxiety Inventory (STAI) [40];
- Burnout by the short version of the Burnout Measure [5];
- Sense of coherence by the short version of the Orientation to Life Questionnaire [27],
- Clinical empathy by the Jefferson Scale of Empathy [10];
- Moral sensitivity, moral distress, and moral injury by the Moral Sensitivity Questionnaire [43]; the seven top-ranking situations in intensive health care [44] of the revised Moral Distress Scale [45], with four additional situations reflecting COVID-19 context [16]; and the Moral Injury Event Scale [46].
2.4. Instruments
- -
- The Hospital Anxiety and Depression Scale [35] comprises 14 items, 7 for anxiety and 7 for depression, which are rated on a 4-point scale (0 to 4). A total score is calculated by summing the ratings for all the items, and by summing the ratings for the seven items of each subscale to yield two separate sub-scores, which range from 0 to 21, with a cut-off of ≥8 [47]; the internal consistency has shown Cronbach alpha coefficients from 0.67 to 0.93 [48]. The Spanish version has shown a Cronbach alpha of 0.86, for both anxiety and depression, and test–retest reliability with coefficients >0.85 [49].
- -
- -
- The Moral sensitivity questionnaire [43] comprises 9 items worded as assumptions related to patient care, which are rated on a 6-point scale (1 to 6). These nine items are grouped into three factors: Moral strength (3 items); Sense of moral burden (4 items); and Moral responsibility (2 items). The ratings of the items are added, and a higher total score indicates higher sensitivity. It has shown a Cronbach’s alpha coefficient >0.7 [50].
- -
- The seven top ranking situations in intensive health care [44] of the revised Moral Distress Scale [45], with four additional situations reflecting COVID-19 context [16]: “caring for patients who: must experience hospitalization without family presence; die during a hospitalization without family and/or clergy present; present transmission risk to your family/household and …being assigned/floated to a new unit, requiring unfamiliar skills or procedures”. Each situation was rated for both frequency and intensity of disturbance, using a 4-point Likert scale (from 0 to 4). The total score for each instrument was calculated by summing the products of the two scores for each item; in the original study, a psychometric evaluation showed two factors (traditional moral distress and COVID-19-specific moral distress), and a Cronbach’s alpha ≥ 0.74 [16].
- -
- The Moral injury Event Scale comprises 9 items that are rated using a 6-point Likert-type scale (1 = strongly disagree, 6 = strongly agree) [46]. The psychometric evaluation showed favorable internal validity, temporal stability, initial discriminant, and concurrent validity; the factor analysis indicated a two-factor solution (perceived transgressions and perceived betrayal), while the internal consistency estimate was 0.90 [46]. The scale has been used in health workers in the context of the COVID-19 pandemic [23,31], with an internal consistency of α = 0.87 [23]. For the current study, the original instructions were adapted to ask the respondent to recall his/her individual experiences during the COVID-19 pandemic, which were revised by five psychiatrists until absolute agreement.
- -
- The Pittsburg Sleep Quality Index [39] comprises 19 items, with 7 components on subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. A total score is calculated by the sum of all the components, and a cut-off >5 is used to distinguish good from poor sleepers. Cronbach’s alpha coefficient has varied from 0.70 to 0.83 [51]. The Spanish version has shown an alpha coefficient of 0.80 and a Spearman correlation coefficient of 0.77 [52].
- -
- The Jefferson Scale of Empathy [10] is used to measure empathy in health professionals. The instrument was developed for administration to practicing health professionals. It comprises 20 items that include three factors: perspective-taking, compassionate care, and walking in patient’s shoes. Items are rated using a 7-point Likert-type scale (1 = strongly disagree to 7 = strongly agree), half of them are positively worded, and the other half are negatively worded (reverse scored). A total score is calculated by summing the ratings for all the items (range 7–140). It has been translated into 56 languages, with adequate construct validity, criterion-related validity, and internal consistency reliability (Cronbach’s alpha range 0.80 to 0.85) [10].
- -
- The Resilience Scale by Connor and Davidson (2003) [34] comprises 25 items, where each one is rated on a 4-point scale (0 to 4). A total score is calculated by summing the ratings for all the items (range 0 to 100). It has good ratings on content validity, internal consistency, validity, reproducibility, agreement, and reliability [53]. The Spanish version has shown a Cronbach alpha coefficient of 0.86 [54].
- -
- The short version of the Orientation to Life Questionnaire [27] comprises 13 items to measure comprehensibility, manageability, and meaningfulness. Comprehensibility refers to the extent to which one perceives internal and external stimuli as rationally understandable; manageability is defined as the resources at one’s disposal that can be used to meet the requirements of the stimuli; and meaningfulness, refers to the feeling that life has an emotional meaning. The responses are provided using a semantic scale of 1 to 7 points (extreme feelings). A total score is calculated by summing the ratings for all the items (range 13 to 91 points). Antonovsky intended the use of a single total score and not of component scores [26]. The instrument has been used in 49 languages in 48 countries. The scale has shown internal consistency with a Cronbach’s alpha of 0.70 to 0.92 [55].
- -
- The short version of the State-Trait Anxiety Inventory [40] comprises 6 items coded on a 4-point scale (from 0 to 3). A total score is calculated by the sum of all the components (range 0 to 18). It has shown similar scores to those produced with the full form across subject groups [40]. The internal consistency when administered repeatedly was <0.80 [56].
- -
- The Dissociative Experiences Scale [41] comprises 28 items including: disturbances in memory, identity, and cognition, and feelings of derealization, depersonalization, absorption, and imaginative involvement. Scores on each item may range from 0% to 100% by multiples of ten (10%, 20%, 30%, etc.); a total score is calculated as an average of the individual scores (range from 0% to 100%); the low normal range has been considered by a cut-off point of 8. The Spanish version has shown a Cronbach alpha of 0.96 [57].
- -
- The Depersonalization/Derealization Inventory by Cox & Swinson (2002) [42] comprises 28 items rated on a 4-point scale (0 to 4). It was designed for the assessment of clinical anxiety states, rather than in the context of dissociative disorders. A total score is obtained by the sum of the individual scores (range 0 to 112), with an internal consistency coefficient of 0.95 [40]. The Spanish version has been used in the general population and in patients with sensory deficits [58].
- -
- The Stanford Acute Stress Reaction Questionnaire II (SASRQ-II) [36,37]. At first, the respondent is asked to describe the stressful event and how much disturbance it caused. The second part of the instrument contains 30 statements with answers on a 6-point scale (from 0 = not experienced to 5 = very often experienced). The third part of the instrument includes four questions about the duration of symptoms, degree of functional impairment, and whether the respondent suffers from any mental illness. The range of scores is 0–150. In nurses, it has shown an alpha Cronbach of 0.97 [37].
- -
- The Posttraumatic Stress Disorder Symptom Severity Scale-Revised by Echeburúa (2016) [36] is a 21-item structured interview based on DSM-5 criteria. It has shown high internal consistency with a Cronbach alpha of 0.91), as well as good discriminant and concurrent validity; and a diagnostic efficacy of 82.48%, using a cut-off point of 20 [38].
2.5. Statistical Analysis
3. Results
3.1. Psychological Screening
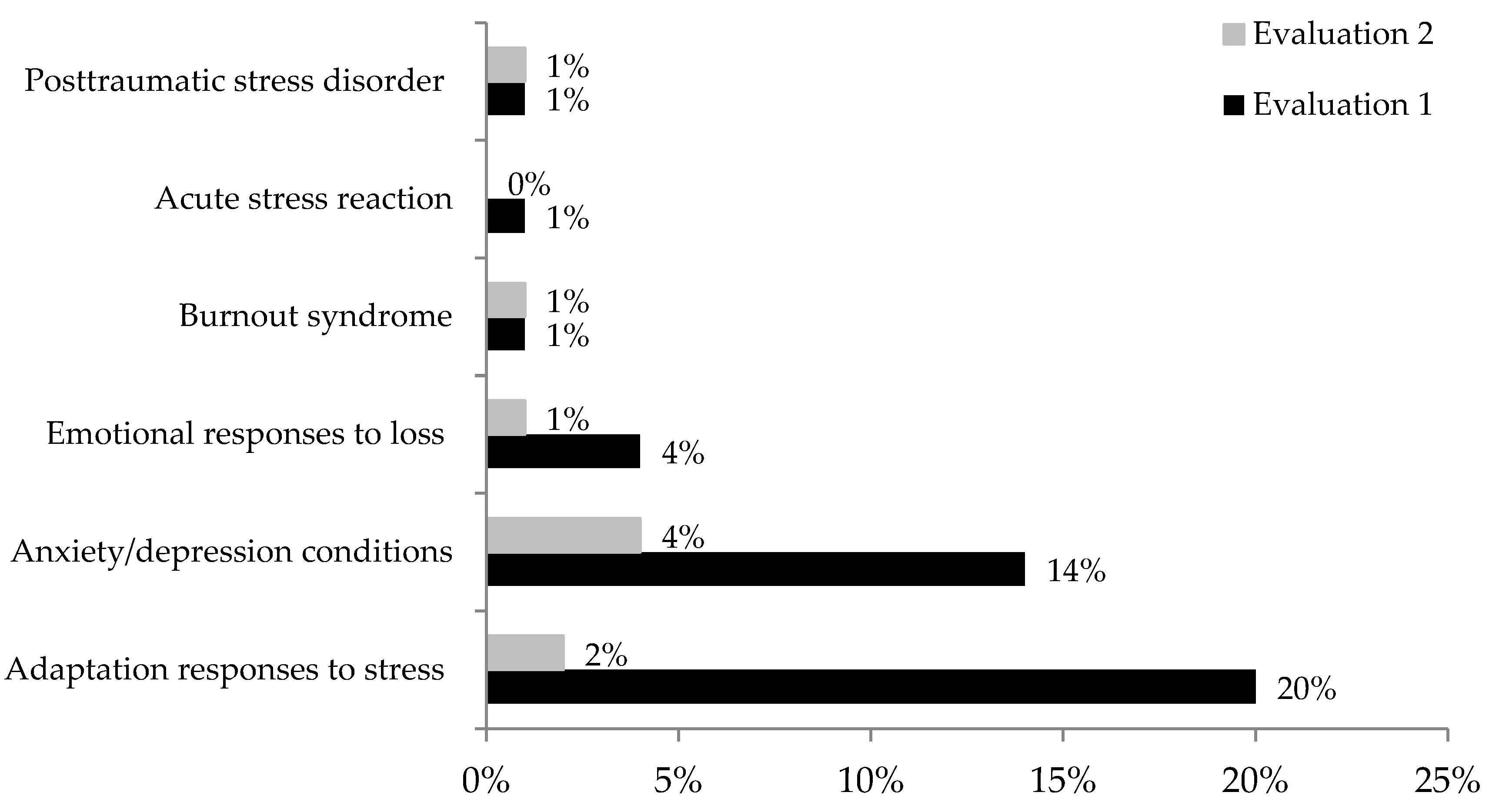
- In the first evaluation, which was performed at the end of the fourth wave of contagions, 44 (41%) participants were experiencing adverse emotional reactions, comprising:
- -
- Anxiety/depression conditions in 15 (14%) participants (2 staff specialist/13 residents);
- -
- Emotional responses to loss in four (4%) residents;
- -
- Burnout syndrome in one (1%) resident;
- -
- Adaptation responses to stress in 22 (20%) participants (4 staff specialist/18 residents);
- -
- Acute stress reaction in one (1%) staff specialist;
- -
- Posttraumatic stress disorder in one (1%) staff specialist.
- In the second evaluation three months later, 10 (9%) participants were experiencing adverse emotional reactions, comprising:
- -
- Anxiety/depression conditions in 5 (4%) participants (1 staff specialist/4 residents), including four with persistent depression/anxiety and one with persistent anxiety;
- -
- Emotional responses to loss in one (1%) resident;
- -
- Persistent burnout syndrome in one (1%) resident;
- -
- Adaptation responses to stress in two (2%) residents;
- -
- Posttraumatic stress disorder in resolution in one (1%) staff specialist.
3.2. Bivariate Analysis
3.3. Multivariate Analysis on the Moral Distress Instruments
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Cénat, J.M.; Blais-Rochette, C.; Kokou-Kpolou, C.K.; Noorishad, P.G.; Mukunzi, J.N.; McIntee, S.E.; Dalexis, R.D.; Goulet, M.A.; Labelle, P.R. Prevalence of symptoms of depression, anxiety, insomnia, posttraumatic stress disorder, and psychological distress among populations affected by the COVID-19 pandemic: A systematic review and meta-analysis. Psychiatry Res. 2021, 295, 113599. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Ripoll, M.J.; Zamanillo-Campos, R.; Castro, A.; Fiol-de Roque, M.A.; Ricci-Cabello, I. Insomnia and sleep quality in healthcare workers fighting against COVID-19: A systematic review of the literature and meta-analysis. Actas Esp. Psiquiatr. 2021, 49, 155–179. [Google Scholar] [PubMed]
- McCall, W.V.; Mensah-Bonsu, D.; Withers, A.; Gibson, R.W. Short-term insomnia disorder in health care workers in an academic medical center before and during COVID-19: Rates and predictive factors. J. Clin. Sleep Med. 2021, 17, 749–755. [Google Scholar] [CrossRef] [PubMed]
- Leiter, M.P.; Schaufeli, W.B. Consistency of the burnout construct across occupations. Anxiety Stress Coping 1996, 9, 229–243. [Google Scholar] [CrossRef]
- Malach-Pines, A. The Burnout Measure, Short Version. Int. J. Stress Manag. 2005, 12, 78–88. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; West, C.P.; Sinsky, C.; Trockel, M.; Tutty, M.; Satele, D.V.; Carlasare, L.E.; Dyrbye, L.N. Changes in Burnout and Satisfaction With Work-Life Integration in Physicians and the General US Working Population Between 2011 and 2017. Mayo Clin. Proc. 2019, 94, 1681–1694. [Google Scholar] [CrossRef]
- Prasad, K.; McLoughlin, C.; Stillman, M.; Poplau, S.; Goelz, E.; Taylor, S.; Nankivil, N.; Brown, R.; Linzer, M.; Cappelucci, K.; et al. Prevalence and correlates of stress and burnout among U.S. healthcare workers during the COVID-19 pandemic: A national cross-sectional survey study. EClinicalMedicine 2021, 35, 100879. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; West, C.P.; Sinsky, C.; Trockel, M.; Tutty, M.; Wang, H.; Carlasare, L.E.; Dyrbye, L.N. Changes in Burnout and Satisfaction With Work-Life Integration in Physicians and the General US Working Population Between 2011 and 2020. Mayo Clin. Proc. 2022, 97, 491–506. [Google Scholar] [CrossRef]
- Kapil, V.; Collett, G.; Godec, T.; Gupta, J.; Maniero, C.; Ng, S.M.; McIntosh, I.; Kumar, A.; Nair, S.; Kotecha, A.; et al. Longitudinal comparisons of mental health, burnout and well-being in patient-facing, non-patient-facing healthcare professionals and non-healthcare professionals during the COVID-19 pandemic: Findings from the CoPE-HCP study. BJPsych Open 2022, 8, E173. [Google Scholar] [CrossRef]
- Hojat, M.; Mangione, S.; Nasca, T.J.; Cohen, M.J.M.; Gonnella, J.S.; Erdmann, J.B.; Veloski, J.; Magee, M. The Jefferson Scale of Physician Empathy: Development and preliminary psychometric data. Educ. Psychol. Meas. 2001, 61, 349–365. [Google Scholar] [CrossRef]
- Epstein, E.G.; Whitehead, P.B.; Prompahakul, C.; Thacker, L.R.; Hamric, A.B. Enhancing Understanding of Moral Distress: The Measure of Moral Distress for Health Care Professionals. AJOB Empir. Bioeth. 2019, 10, 113–124. [Google Scholar] [CrossRef] [PubMed]
- Jameton, A. Nursing Practice: The Ethical Issues, 1st ed.; Prentice Hall: Hoboken, NJ, USA, 1984. [Google Scholar]
- Lützén, K.; Dahlqvist, V.; Eriksson, S.; Norberg, A. Developing the concept of moral sensitivity in health care practice. Nurs. Ethics. 2006, 13, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Epstein, E.G.; Hamric, A.B. Moral distress, moral residue, and the crescendo effect. J. Clin. Ethics 2009, 20, 330–342. [Google Scholar] [CrossRef] [PubMed]
- Norman, S.B.; Feingold, J.H.; Kaye-Kauderer, H.; Kaplan, C.A.; Hurtado, A.; Kachadourian, L.; Feder, A.; Murrough, J.W.; Charney, D.; Southwick, S.M.; et al. Moral distress in frontline healthcare workers in the initial epicenter of the COVID-19 pandemic in the United States: Relationship to PTSD symptoms, burnout, and psychosocial functioning. Depress. Anxiety 2021, 38, 1007–1017. [Google Scholar] [CrossRef]
- Lake, E.T.; Narva, A.M.; Holland, S.; Smith, J.G.; Cramer, E.; Rosenbaum, K.E.F.; French, R.; Clark, R.R.S.; Rogowski, J.A. Hospital nurses’ moral distress and mental health during COVID-19. J. Adv. Nurs. 2022, 78, 799–809. [Google Scholar] [CrossRef]
- Wilson, C.A.; Metwally, H.; Heavner, S.; Kennedy, A.B.; Britt, T.W. Chronicling moral distress among healthcare providers during the COVID-19 pandemic: A longitudinal analysis of mental health strain, burnout, and maladaptive coping behaviours. Int. J. Ment. Health Nurs. 2022, 31, 111–127. [Google Scholar] [CrossRef]
- Donkers, M.A.; Gilissen, V.J.H.S.; Candel, M.J.J.M.; van Dijk, N.M.; Kling, H.; Heijnen-Panis, R.; Pragt, E.; van der Horst, I.; Pronk, S.A.; van Mook, W.N.K.A. Moral distress and ethical climate in intensive care medicine during COVID-19: A nationwide study. BMC Med. Ethics 2021, 22, 73. [Google Scholar] [CrossRef]
- Shay, J. Moral injury. Psychoanal. Psychol. 2014, 31, 182–191. [Google Scholar] [CrossRef]
- Fani, N.; Currier, J.M.; Turner, M.D.; Guelfo, A.; Kloess, M.; Jain, J.; Mekawi, Y.; Kuzyk, E.; Hinrichs, R.; Bradley, B.; et al. Moral injury in civilians: Associations with trauma exposure, PTSD, and suicide behavior. Eur. J. Psychotraumatol. 2021, 12, 1965464. [Google Scholar] [CrossRef]
- Mantri, S.; Lawson, J.M.; Wang, Z.; Koenig, H.G. Identifying Moral Injury in Healthcare Professionals: The Moral Injury Symptom Scale-HP. J. Relig. Health 2020, 59, 2323–2340. [Google Scholar] [CrossRef]
- Hines, S.E.; Chin, K.H.; Glick, D.R.; Wickwire, E.M. Trends in Moral Injury, Distress, and Resilience Factors among Healthcare Workers at the Beginning of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 488. [Google Scholar] [CrossRef]
- Amsalem, D.; Lazarov, A.; Markowitz, J.C.; Naiman, A.; Smith, T.E.; Dixo, L.B.; Neria, Y. Psychiatric symptoms and moral injury among US healthcare workers in the COVID-19 era. BMC Psychiatry 2021, 21, 546. [Google Scholar] [CrossRef] [PubMed]
- Zerach, G.; Levi-Belz, Y. Moral injury and mental health outcomes among Israeli health and social care workers during the COVID-19 pandemic: A latent class analysis approach. Eur. J. Psychotraumatol. 2021, 12, 1945749. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, B.L. The role of positive emotions in positive psychology. The broaden-and-build theory of positive emotions. Am. Psychol. 2001, 56, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. Unraveling the Mystery of Health. How People Manage Stress and Stay Well, 1st ed.; Jossey-Bass Publishers: San Francisco, CA, USA, 1987. [Google Scholar]
- Eriksson, M.; Mittelmark, M.B. The sense of coherence and its measurement. In The Handbook of Salutogenesis, 1st ed.; Mittelmark, M.B., Sagy, S., Eriksson, M., Bauer, G.F., Pelikan, J.M., Lindström, B., Espnes, G.A., Eds.; Chapter 12; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Di Trani, M.; Mariani, R.; Ferri, R.; De Berardinis, D.; Frigo, M.G. From Resilience to Burnout in Healthcare Workers During the COVID-19 Emergency: The Role of the Ability to Tolerate Uncertainty. Front. Psychol. 2021, 12, 646435. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, M.; Nepa, G.; Prout, T.A.; Albertini, F.; Marcelli, S.; Orrù, G.; Conversano, C. Stress, Burnout, and Resilience among Healthcare Workers During the COVID-19 Emergency: The Role of Defense Mechanisms. Int. J. Environ. Res. Public Health 2021, 18, 5258. [Google Scholar] [CrossRef]
- Gómez-Salgado, J.; Domínguez-Salas, S.; Romero-Martín, M.; Ortega-Moreno, M.; García-Iglesias, J.J.; Ruiz-Frutos, C. Sense of Coherence and Psychological Distress among Healthcare Workers During the COVID-19 Pandemic in Spain. Sustainability 2020, 12, 6855. [Google Scholar] [CrossRef]
- Litam, S.D.A.; Balkin, R.S. Moral injury in health-care workers during COVID-19 pandemic. Traumatology 2021, 27, 14–19. [Google Scholar] [CrossRef]
- Lamiani, G.; Biscardi, D.; Meyer, E.C.; Giannini, A.; Vegni, E. Moral Distress Trajectories of Physicians 1 Year after the COVID-19 Outbreak: A Grounded Theory Study. Int. J. Environ. Res. Public Health 2021, 18, 13367. [Google Scholar] [CrossRef]
- American Psychiatric Association. DSM-5. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R.T.; Lee, L.-C. Spirituality, resilience, and anger in survivors of violent trauma: A community survey. J. Trauma. Stress 2003, 16, 487–494. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Cardeña, E.; Koopman, C.; Classen, C.; Waelde, L.C.; Spiegel, D. Psychometric properties of the Stanford Acute Stress Reaction Questionnaire (SASRQ): A valid and reliable measure of acute stress. J. Trauma. Stress 2000, 13, 719–734. [Google Scholar] [CrossRef] [PubMed]
- Palmborg, Å.; Lötvall, R.; Cardeña, E. Acute Stress among Nurses in Sweden during the COVID-19 Pandemic. Eur. J. Trauma Dissociation 2022, 6, 100283. [Google Scholar] [CrossRef]
- Echeburúa, E.; Amor, P.J.; Sarasua, B.; Zubizarreta, I.; Holgado-Tello, F.P.; Muñoz, J.M. Posttraumatic Stress Disorder Symptom Severity Scale-Revised (EGS-R) according to DSM-5 criteria: Psychometric Properties. Ter. Psicol. 2016, 34, 111–128. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Marteau, T.M.; Bekker, H. The development of a six-item short-form of the state scale of the Spielberger State-Trait Anxiety Inventory (STAI). Br. J. Clin. Psychol. 1992, 31, 301–306. [Google Scholar] [CrossRef]
- Bernstein, E.M.; Putnam, F.W. Development, reliability, and validity of a dissociation scale. J. Nerv. Ment. Dis. 1986, 174, 727–735. [Google Scholar] [CrossRef]
- Cox, B.J.; Swinson, R.P. Instrument to assess depersonalization-derealization in panic disorder. Depress. Anxiety 2002, 15, 172–175. [Google Scholar] [CrossRef]
- Lützén, K.; Nordin, C. Modifying autonomy a concept grounded in nurses’ experiences of moral decision-making in psychiatric practice. J. Med. Ethics 1994, 20, 101–107. [Google Scholar] [CrossRef]
- Colville, G.A.; Dawson, D.; Rabinthiran, S.; Chaudry-Daley, Z.; Perkins-Porras, L. A survey of moral distress in staff working in intensive care in the UK. J. Intensive Care Soc. 2019, 20, 196–203. [Google Scholar] [CrossRef]
- Hamric, A.B. Empirical research on moral distress: Issues, challenges, and opportunities. HEC Forum 2012, 24, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Nash, W.P.; Marino Carper, T.L.; Mills, M.A.; Au, T.; Goldsmith, A.; Litz, B.T. Psychometric evaluation of the Moral Injury Events Scale. Mil. Med. 2013, 178, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Olssøn, I.; Mykletun, A.; Dahl, A.A. The Hospital Anxiety and Depression Rating Scale: A cross-sectional study of psycho-726 metrics and case finding abilities in general practice. BMC Psychiatry 2005, 5, 46. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Quintana, J.M.; Padierna, A.; Esteban, C.; Arostegui, I.; Bilbao, A.; Ruiz, I. Evaluation of the psychometric characteristics of the Spanish version of the Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 2003, 107, 216–221. [Google Scholar] [CrossRef]
- Lützén, K.; Blom, T.; Ewalds-Kvist, B.; Winch, S. Moral stress, moral climate and moral sensitivity among psychiatric professionals. Nurs. Ethics 2010, 17, 213–224. [Google Scholar] [CrossRef]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef]
- Hita-Contreras, F.; Martínez-López, E.; Latorre-Román, P.A.; Garrido, F.; Santos, M.A.; Martínez-Amat, A. Reliability and validity of the Spanish version of the Pittsburgh Sleep Quality Index (PSQI) in patients with fibromyalgia. Rheumatol. Int. 2014, 34, 929–936. [Google Scholar] [CrossRef]
- Windle, G.; Bennett, K.M.; Noyes, J. A methodological review of resilience measurement scales. Health Qual. Life Outcomes 2011, 9, 8. [Google Scholar] [CrossRef]
- García-León, M.A.; González-Gómez, A.; Robles-Ortega, H.; Padilla, J.L.; Peralta-Ramirez, M.I. Propiedades psicométricas de la Escala de Resiliencia de Connor y Davidson (CD-RISC) en población española. Anal. Psicol. 2019, 35, 33–40. [Google Scholar] [CrossRef]
- Eriksson, M.; Lindström, B. Validity of Antonovsky’s sense of coherence scale: A systematic review. J Epidemiol. Community Health 2005, 59, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Bayrampour, H.; McDonald, S.; Fung, T.; Tough, S. Reliability and validity of three shortened versions of the State Anxiety Inventory scale during the perinatal period. J. Psychosom. Obstet. Gynecol. 2014, 35, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Robles García, R.; Garibay Rico, S.E.; Páez Agráz, F. Evaluación de trastornos disociativos en población psiquiátrica mexicana: Prevalencia, comorbilidad y características psicométricas de la Escala de Experiencias Disociativas. Salud Ment. 2006, 29, 38–43. [Google Scholar]
- Jáuregui-Renaud, K.; Ramos-Toledo, V.; Aguilar-Bolaños, M.; Montaño-Velázquez, B.; Pliego-Maldonado, A. Symptoms of detachment from the self or from the environment in patients with an acquired deficiency of the special senses. J. Vestib. Res. 2008, 18, 129–137. [Google Scholar] [CrossRef]
- Holm, S. A Simple Sequentially Rejective Multiple Test Procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Cohen, J. Statistical Power Analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Di Monte, C.; Monaco, S.; Mariani, R.; Di Trani, M. From Resilience to Burnout: Psychological Features of Italian General Practitioners During COVID-19 Emergency. Front. Psychol. 2020, 11, 567201. [Google Scholar] [CrossRef]
- Čartolovni, A.; Stolt, M.; Scott, P.A.; Suhonen, R. Moral injury in healthcare professionals: A scoping review and discussion. Nurs. Ethics 2021, 28, 590–602. [Google Scholar] [CrossRef]
- Rodriguez-Ruiz, E.; Campelo-Izquierdo, M.; Boga Veiras, P.; Mansilla Rodríguez, M.; Estany-Gestal, A.; Blanco Hortas, A.; Rodríguez-Calvo, M.S.; Rodríguez-Núñez, A. Impact of the Coronavirus Disease 2019 Pandemic on Moral Distress among Nurses and Physicians in Spanish ICUs. Crit. Care Med. 2022, 50, e487–e497. [Google Scholar] [CrossRef]
- Lamiani, G.; Dordoni, P.; Vegni, E.; Barajon, I. Caring for Critically Ill Patients: Clinicians’ Empathy Promotes Job Satisfaction and Does Not Predict Moral Distress. Front. Psychol. 2020, 10, 2902. [Google Scholar] [CrossRef]
- Stratta, E.C.; Riding, D.M.; Baker, P. Ethical erosion in newly qualified doctors: Perceptions of empathy decline. Int. J. Med. Educ. 2016, 7, 286–292. [Google Scholar] [CrossRef]
- Liu, L.X.; Goldszmidt, M.; Calvert, S.; Burm, S.; Torti, J.; Cristancho, S.; Sukhera, J. From distress to detachment: Exploring how providing care for stigmatized patients influences the moral development of medical trainees. Adv. Health Sci. Educ. Theory Pract. 2022, 27, 1003–1019. [Google Scholar] [CrossRef] [PubMed]
- Del-Pino-Casado, R.; Espinosa-Medina, A.; López-Martínez, C.; Orgeta, V. Sense of coherence, burden and mental health in caregiving: A systematic review and meta-analysis. J. Affect. Disord. 2019, 242, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, M.; Lindström, B. Antonovsky’s sense of coherence scale and the relation with health: A systematic review. J. Epidemiol. Community Health 2006, 60, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Dȩbska, G.; Pasek, M.; Wilczek-Rużyczka, E. Sense of Coherence vs. Mental Load in Nurses Working at a Chemotherapy Ward. Cent. Eur. J. Public Health 2017, 25, 35–40. [Google Scholar] [CrossRef]
- Sun, D.; Phillips, R.D.; Mulready, H.L.; Zablonski, S.T.; Turner, J.A.; Turner, M.D.; McClymond, K.; Nieuwsma, J.A.; Morey, R.A. Resting-state brain fluctuation and functional connectivity dissociate moral injury from posttraumatic stress disorder. Depress. Anxiety 2019, 36, 442–452. [Google Scholar] [CrossRef]
- Stewart, N.H.; Arora, V.M. The Impact of Sleep and Circadian Disorders on Physician Burnout. Chest 2019, 156, 1022–1030. [Google Scholar] [CrossRef]
- Serrano, J.; Hassamal, S.; Hassamal, S.; Hassamal, S.; Dong, F.; Neeki, M. Depression and anxiety prevalence in nursing staff during the COVID-19 pandemic. Nurs. Manag. 2021, 52, 24–32. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Instruments | Evaluation 1 Median (Q1–Q3) | Evaluation 2 Median (Q1–Q3) | p (Z) |
|---|---|---|---|
| Hospital Anxiety and Depression Scale | |||
| 6 (2.5–9) | - | - |
| Women | 5 (2–9) | - | - |
| Men | 6 (3–9) | - | - |
| 3 (1–4) | - | - |
| Women | 3 (1–4) | - | - |
| Men | 3 (1–4) | - | - |
| 8 (4–13) | - | - |
| Women | 8.5 (4–13) | - | - |
| Men | 8 (4–13) | - | - |
| Resilience Scale (all) | 78.5 (71–87) | - | - |
| Women | 78 (72–87) | - | - |
| Men | 78.5 (69–88) | - | - |
| Pittsburg Sleep Quality Index (all) | 8.5 (6–11) | 7 (5–10) | 0.06 (1.851) |
| Women | 9 (7–11) | 7 (6–10) | 0.003 (2.954) |
| Men | 7 (5–9) | 7 (5–9) | 0.72 (0.355) |
| State-Trait Anxiety Inventory (all) | 4 (2–6.5) | 3 (1–6) | 0.08 (1.748) |
| Women | 4 (2–7) | 4 (2–6) | 0.48 (0.697) |
| Men | 4 (2–6) | 2 (1–5) | 0.06 (1.827) |
| Burnout Measure (all) | 2.5 (1.8–3.2) | 2.2 (1.8–2.9) | 0.003 (2.895) |
| Women | 2.6 (1.9–3.4) | 2.4 (2.0–3.1) | 0.08 (1.720) |
| Men | 2.4 (1.8–3.0) | 2.1 (1.6–2.6) | 0.01 (2.385) |
| Dissociative Experiences Scale (all) | 3.9 (1.4–8.2) | 2.6 (0.7–5.5) | 0.003 (2.878) |
| Women | 4.4 (1.0–7.8) | 2.8 (0.7–5.0) | 0.01(2.345) |
| Men | 3.9 (1.7–10) | 2.5 (0.3–5.7) | 0.12 (1.552) |
| Depersonalization/derealization (all) | 7 (2–14) | 5 (1.5–10) | 0.001(3.232) * |
| Women | 6.5 (2–14) | 5.5 (3–10) | 0.09 (1.666) |
| Men | 7 (3–14) | 4 (1–9) | 0.003 (2.949) |
| Orientation to Life Questionnaire (all) | 68 (60.5–77.5) | 72.5 (63.5–80) | 0.007 (2.666) |
| Women | 67 (71–77) | 72 (62–80) | 0.03 (2.142) |
| Men | 68.5 (60–78) | 73 (66–81) | 0.10 (1.642) |
| Jefferson Scale of Empathy (all) | 116 (106–127) | 116 (105–127) | 0.79 (0.254) |
| Women | 119 (110–128) | 118 (108–128) | .0.53 (0.627) |
| Men | 111 (109–122) | 114 (96–123) | 1 (0) |
| Moral Sensitivity Questionnaire (all) | 38.5 (34–43) | 39 (35–41) | 0.42 (0.792) |
| Women | 39 (34–43) | 39 (34–41) | 0.43 (0.787) |
| Men | 37.5 (35–42) | 38.5 (35–41) | 0.68 (0.402) |
| Items of Moral Distress Scale-R (all) | 16 (8–35.3) | 11.5 (3.0–23.5) | 0.0004(3.508) * |
| Women | 24.5 (10–40) | 13 (7–27) | 0.004 (2.828) |
| Men | 13.5 (6–24) | 9 (2–16) | 0.03 (2.167) |
| Additional COVID-19 situations (all) | 12 (4–18.5) | 6 (1.5–12.5) | <0.0001(4.910) * |
| Women | 13.5 (5–21) | 7 (2–14) | <0.0001 (4.637) * |
| Men | 8 (2–15) | 4 (1–12) | 0.03 (2.168) |
| Moral Injury Event Scale (all) | 15 (10–20) | 13 (9–19) | 0.15 (1.412) |
| Women | 15 (11–21) | 13.5 (9–19) | 0.55 (0.596) |
| Men | 14 (10–19) | 12.5 (9–21) | 0.4 (.840) |
| Instruments | Staff Physicians | Residents Since Wave 1 | Residents Since Wave 3 | p (H) |
|---|---|---|---|---|
| Median (Q1–Q3) | Median (Q1–Q3) | Median (Q1–Q3) | ||
| Hospital Anxiety and Depression Scale | ||||
| 3 (1–8) | 6 (3–10) | 6 (2–9) | 0.27 (2.567) |
| 2 (0–3) | 3 (2–5) | 2 (1–5) | 0.28 (2.507) |
| 6 (3–10) | 10 (5–16) | 8 (4–13) | 0.18 (3.358) |
| Resilience Scale | 87 (81–90) | 76 (67–83) | 80 (73–85) | 0.08 (5.004) |
| Pittsburg Sleep Quality Index | ||||
| Evaluation 1 | 9 (4–11) | 9 (6–11) | 7 (5–9) | 0.25 (2.724) |
| Evaluation 2 | 7 (6–9) | 7 (5–10) | 7 (5–11) | 0.16 (3.620) |
| State-Trait Anxiety Inventory | ||||
| Evaluation 1 | 3 (1–5) | 4 (2–7) | 4 (3–6) | 0.24 (2.822) |
| Evaluation 2 | 2 (1–4) | 4 (2–7) | 4 (1–6) | 0.66 (0.828) |
| Burnout Measure | ||||
| Evaluation 1 | 2.3 (1.7–3.0) | 2.6 (1.9–3.2) | 2.6 (2–3) | 0.29 (2.43) |
| Evaluation 2 | 1.9 (1.5–2.6) | 2.4 (2.0–3.2) | 2.3 (1.9–2.6) | 0.10 (4.459) |
| Dissociative Experiences Scale | ||||
| Evaluation 1 | 2.5 (0.3–6.4) | 4.6 (2.1–8.2) | 3.9 (1.8–10.3) | 0.19 (3.229) |
| Evaluation 2 | 2.5 (0.3–5.0) | 3.0 (0.7–5.0) | 2.1 (0.4–10.3) | 0.90 (0.200) |
| Depersonalization/derealization | ||||
| Evaluation 1 | 2 (1–10) | 8.5 (3–14) | 7 (2–16) | 0.07 (5.241) |
| Evaluation 2 | 3 (0–6) | 6 (2–11) | 6 (3–10) | 0.18 (3.416) |
| Orientation to Life Questionnaire | ||||
| Evaluation 1 | 77 (67–82) | 66 (57–72) | 68 (61–78) | 0.10 (4.518) |
| Evaluation 2 | 80 (72–86) | 71 (59–79) | 71 (65–79) | 0.17 (3.500) |
| Jefferson Scale of Empathy | ||||
| Evaluation 1 | 120 (107–128) | 115 (110–125) | 118 (100–127) | 0.77 (0.504) |
| Evaluation 2 | 118 (106–122) | 115 (107–128) | 115 (91–129) | 0.93 (0.145) |
| Moral Sensitivity Questionnaire | ||||
| Evaluation 1 | 39 (34–47) | 39 (35–43) | 38 (33–43) | 0.69 (0.74) |
| Evaluation 2 | 39 (34–41) | 39 (36–41) | 39 (32–40) | 0.39 (1.840) |
| Items of Moral Distress Scale-R | ||||
| Evaluation 1 | 22 (5–41) | 16 (10–32) | 15/8–33) | 0.85 (0.316) |
| Evaluation 2 | 10 (1–18) | 13 (5–30) | 10 (2–17) | 0.52 (1.261) |
| Additional COVID-19 situations | ||||
| Evaluation 1 | 10 (3–18) | 12 (5–18) | 14 (4–22) | 0.58 (1.068) |
| Evaluation 2 | 5 (0–9) | 7 (2–16) | 3 (1–12) | 0.65 (0.848) |
| Moral Injury Event Scale | ||||
| Evaluation 1 | 14 (12–23) | 15 (10–19) | 17 (9–25) | 0.93 (0.125) |
| Evaluation 2 | 13 (9–18) | 13 (9–19) | 14 (10–23) | 0.23 (2.931) |
| Items | Staff Physicians | Residents Since Wave 1 | Residents Since Wave 3 | p (H) |
|---|---|---|---|---|
| Median (Q1–Q3) | Median (Q1–Q3) | Median (Q1–Q3) | ||
| Caring for patients who must experience hospitalization without family presence | ||||
| Evaluation1 | 0 (0–4) | 0.5 (0–4) | 1 (0–6) | 0.83 (0.349) |
| Evaluation 2 | 0 (0–1) | 0.5 (0–2) | 0 (0–1) | 0.45 (1.555) |
| Caring for patients who die during a hospitalization without family and/or clergy present | ||||
| Evaluation 1 | 1 (0–4) | 1.5 (0–4) | 2 (0–4) | 0.19 (3.273) |
| Evaluation 2 | 0 (0–2) | 1.5 (0–4) | 0 (0–2) | 0.34 (2.113) |
| Being assigned/floated to a new unit, requiring unfamiliar skills or procedures | ||||
| Evaluation 1 | 0 (0–1) | 3 (1–6) | 4 (1–6) | 0.0007 (9.880) * |
| Evaluation 2 | 0 (0–0) | 3 (0–4) | 2 (0–2) | 0.11 (4.327) |
| Caring for patients who present transmission risk to your family/household | ||||
| Evaluation 1 | 6 (1–9) | 2 (0–8) | 4 (1–9) | 0.84 (0.339) |
| Evaluation 2 | 1 (0–6) | 2 (0–6) | 1 (0–6) | 0.87 (0.264) |
| Instrument | ||||
| Between Evaluations | ||||
| Gamma | p (Z) | |||
| Items of the Moral Distress Scale-R | 0.224 | 0.0008(3.339) | - | - |
| Moral Distress COVID-19 situations | 0.402 | <0.0001 (5.906) | - | - |
| Moral Injury Event Scale Transgressions | 0.348 | <0.0001 (4.634) | - | - |
| Moral Injury Event Scale Betrayal. | 0.245 | 0.002 (3.031) | - | - |
| Moral Injury Event Scale Total score | 0.273 | 0.0001 (3.843) | - | - |
| Within each evaluation | Evaluation 1 | Evaluation 2 | ||
| Gamma | p (Z) | Gamma | p (Z) | |
| Items of the Moral Distress Scale-R and | ||||
| 0.261 | 0.0002 (3.678) | 0.345 | <0.0001 (4.767) |
| 0.364 | <0.0001 (5.057) | 0.230 | 0.002 (3.000) |
| 0.361 | <0.0001 (5.298) | 0.327 | <0.0001 (4.666) |
| COVID-19 situations and | ||||
| 0.320 | <0.0001 (4.499) | 0.292 | <0.0001 (3.988) |
| 0.353 | <0.0001 (4.890) | 0.319 | <0.0001 (4.145) |
| 0.363 | <0.0001 (5.312) | 0.344 | <0.0001 (4.869) |
| Items of the Moral Distress Scale-R | ||||
|---|---|---|---|---|
| Within Each Evaluation | Evaluation 1 | Evaluation 2 | ||
| F | p | F | p | |
| Intercept | 4.846 | 0.029 * | 0.779 | 0.379 |
| Resilience Scale | 0.439 | 0.508 | 6.055 | 0.015 * |
| Jefferson Scale of Empathy | 6.869 | 0.010 * | 4.290 | 0.040 * |
| Burnout Measure | 18.952 | <0.0001 * | 1.66 | 0.199 |
| COVID-19 sick leave | 7.067 | 0.009 * | 0.013 | 0.906 |
| Repeated measure | 6.113 | 0.015 * | - | - |
| Resilience Scale | 5.200 | 0.024 * | - | - |
| Jefferson Scale of Empathy | 0.577 | 0.449 | - | - |
| Burnout Measure | 7.648 | 0.006 * | - | - |
| COVID-19 sick leave | 4.654 | 0.033 * | - | - |
| Moral Injury Event Scale | Evaluation 1 | Evaluation 2 | ||
|---|---|---|---|---|
| Total Score | Estimate (95% C.I.) | p (Wald Statistic) | Estimate (95% C.I.) | p (Wald Statistic) |
| Intercept | 3.170 (2.610–3.730) | <0.0001 (123.01) | 2.960 (2.399–3.522) | <0.0001 (106.79) |
| Orientation to Life Question. | −0.009 (−0.016–−0.002) | 0.012 (6.258) | −0.005 (−0.012–0.002) | 0.144 (2.134) |
| State-Trait Anxiety Inventory | −0.033 (−0.056–−0.009) | 0.006 (7.420) | −0.035 (−0.060–−0.010) | 0.005 (7.697) |
| Dissociative Experiences Scale | 0.019 (0.007–0.031) | 0.002 (9.026) | 0.011 (0.001–0.021) | 0.028 (4.803) |
| Moral Distress Scale-R | 0.005 (0.001–0.010) | 0.019 (5.444) | 0.007 (0.002–0.013) | 0.011 (6.430) |
| COVID-19 situations | 0.012 (0.005–0.019) | 0.0005 (12.123) | 0.016 (0.006–0.026) | 0.001 (10.617) |
| GROUP I (^residents 1/staff) | −0.055 (−0.151–0.041) | 0.260 (1.268) | −0.053 (−0.148–0.042) | 0.272 (1.203) |
| GROUP II (^residents 2/staff) | −0.044 (−0.151–0.063) | 0.416 (0.660) | 0.038 (−0.066–0.141) | 0.474 (0.512) |
| Sick leave due to COVID-19 | 0.022 (−0.053–0.097) | 0.563 (0.334) | 0.099 (0.029–0.169) | 0.005 (7.707) |
| GROUP I* COVID-19 sick leave | 0.051 (−0.042–0.144) | 0.285 (1.141) | 0.074 (−0.015–0.163) | 0.102 (2.672) |
| GROUP II* COVID-19 sick leave | −0.128 (−0.235–−0.021) | 0.019 (5.486) | −0.088 (−0.192–0.017) | 0.099 (2.718) |
| Transgression score | ||||
| Intercept | 2.322 (1.645–3.000) | <0.0001 (3.000) | 2.393 (1.773–3.014) | <0.0001 (57.093) |
| Orientation to Life Question. | −0.003 (−0.011–0.005) | 0.49 (0.475) | −0.003 (−0.011–0.004) | 0.407 (0.686) |
| State-Trait Anxiety Inventory | −0.028 (−0.056–0.000) | 0.053 (3.740) | −0.034 (−0.062–0.007) | 0.15 (5.899) |
| Dissociative Experiences Scale | 0.013 (−0.002–0.028) | 0.095 (2.788) | 0.006 (−0.005–0.017) | 0.273 (1.198) |
| Moral Distress Scale-R | 0.004 (−0.001–0.010) | 0.127 (2.326) | 0.010 (0.004–0.016) | 0.001 (10.439) |
| COVID-19 situations | 0.014 (0.005–0.022) | 0.001 (10.432) | 0.012 (0.001–0.023) | 0.029 (4.731) |
| GROUP I (^residents 1/staff) | −0.006 (−0.123–0.110) | 0.913 (0.012) | −0.052 (−0.157–−0.053) | 0.331 (0.944) |
| GROUP II (^residents 2/staff) | 0.034 (−0.095–0.164) | 0.604 (0.269) | 0.127 (0.012–0.241) | 0.030 (4.706) |
| Sick leave due to COVID-19 | 0.025 (−0.066–0.116) | 0.587 (0.294) | 0.114 (0.036–0.191) | 0.004 (8.279) |
| GROUP I* COVID-19 sick leave | 0.051 (−0.062–0.163) | 0.378 (0.776) | 0.074 (−0.024–0.173) | 0.139 (2.184) |
| GROUP II* COVID-19 sick leave | −0.154 (−0.283–−0.024) | 0.019 (5.417) | −0.109 (−0.224–0.006) | 0.063 (3.444) |
| Betrayal score | ||||
| Intercept | 2.700 (2.026–3.375) | <0.0001 (61.572) | 2.166 (1.361–2.971) | <0.0001 (27.81) |
| Orientation to Life Question. | −0.017 (−0.026–−0.009) | <0.0001 (16.640) | −0.009 (−0.018–0.001) | 0.079 (3.085) |
| State-Trait Anxiety Inventory | −0.038 (−0.067–−0.010) | 0.007 (7.041) | −0.037 (−0.073–−0.002) | 0.040 (4.193) |
| Dissociative Experiences Scale | 0.029 (0.015–0.044) | 0.0001 (15.073) | 0.020 (0.006–0.034) | 0.004 (8.008) |
| Moral Distress Scale-R | 0.005 (0.000–0.010) | 0.07 (3.279) | 0.001 (−0.007–0.009) | 0.872 (0.026) |
| COVID-19 situations | 0.013 (0.005–0.021) | 0.002 (9.322) | 0.024 (0.010–0.038) | 0.0006 (11.752) |
| GROUP I (^residents 1/staff) | −0.124 (−0.239–−0.008) | 0.036 (4.380) | −0.037 (−0.173–0.099) | 0.591 (0.288) |
| GROUP II (^residents 2/staff) | −0.177 (−0.306–−0.048) | 0.0071 (7.232) | −0.140 (−0.288–0.009) | 0.065 (3.391) |
| Sick leave due to COVID-19 | 0.015 (−0.075–0.106) | 0.738 (0.112) | 0.077 (−0.023–0.177) | 0.132 (2.265) |
| GROUP I* COVID-19 sick leave | 0.051 (−0.062–0.163) | 0.376 (0.781) | 0.062 (−0.066–0.190) | 0.543 (0.904) |
| GROUP II* COVID-19 sick leave | −0.086 (−0.215–0.043) | 0.189 (1.718) | −0.044 (−0.194–0.105) | 0.563 (0.334) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cooper-Bribiesca, D.; Rascón-Martínez, D.M.; Miguel-Puga, J.A.; Juárez-Carreón, M.K.; Sánchez-Hurtado, L.A.; Colin-Martinez, T.; Anda-Garay, J.C.; Espinosa-Poblano, E.; Jáuregui-Renaud, K. Physicians’ Distress Related to Moral Issues and Mental Health In-Between Two Late Waves of COVID-19 Contagions. Int. J. Environ. Res. Public Health 2023, 20, 3989. https://doi.org/10.3390/ijerph20053989
Cooper-Bribiesca D, Rascón-Martínez DM, Miguel-Puga JA, Juárez-Carreón MK, Sánchez-Hurtado LA, Colin-Martinez T, Anda-Garay JC, Espinosa-Poblano E, Jáuregui-Renaud K. Physicians’ Distress Related to Moral Issues and Mental Health In-Between Two Late Waves of COVID-19 Contagions. International Journal of Environmental Research and Public Health. 2023; 20(5):3989. https://doi.org/10.3390/ijerph20053989
Chicago/Turabian StyleCooper-Bribiesca, Davis, Dulce María Rascón-Martínez, José Adan Miguel-Puga, María Karen Juárez-Carreón, Luis Alejandro Sánchez-Hurtado, Tania Colin-Martinez, Juan Carlos Anda-Garay, Eliseo Espinosa-Poblano, and Kathrine Jáuregui-Renaud. 2023. "Physicians’ Distress Related to Moral Issues and Mental Health In-Between Two Late Waves of COVID-19 Contagions" International Journal of Environmental Research and Public Health 20, no. 5: 3989. https://doi.org/10.3390/ijerph20053989
APA StyleCooper-Bribiesca, D., Rascón-Martínez, D. M., Miguel-Puga, J. A., Juárez-Carreón, M. K., Sánchez-Hurtado, L. A., Colin-Martinez, T., Anda-Garay, J. C., Espinosa-Poblano, E., & Jáuregui-Renaud, K. (2023). Physicians’ Distress Related to Moral Issues and Mental Health In-Between Two Late Waves of COVID-19 Contagions. International Journal of Environmental Research and Public Health, 20(5), 3989. https://doi.org/10.3390/ijerph20053989