1. Introduction
Health and economics are unrelated concepts. However, this does not imply that the two most crucial components of a nation’s existence cannot be simultaneously improved. If a country is concerned about maximizing its economy, it must prioritize improving its inhabitants’ healthcare standards. One of the most important things a nation can do for its citizens and its growth on the world stage is to improve its health. A nation’s economic development may be maximized by prioritizing healthcare.
Although there is no unique health index to measure health outcomes, many indicators are used to measure health outcomes [
1]. Kindig and Stoddart [
2] indicated expected lifespan and the quality of wellbeing as indicators of health outcomes, whereas Erickson et al. [
3] emphasized the years of a healthy life. The Canadian National Population Health Survey uses the Health Utilities Index to measure health outcomes [
4]. Or [
1] used gender-specific potential years of life lost (PYLL) as an indicator, meanwhile also including the mortality rate and the infant or premature mortality rate as some indicators of health outcomes. Well [
5] noted that some measurements of health outcomes are life expectancy at birth, anemia, low birth weight, etc. Health outcomes are a key component of human resources; they are crucial in measuring economic progress [
6]. Similarly, health outcomes depend on the income of a people and their surrounding environment, along with other factors [
7]. Consequently, health outcomes, economic growth, and energy consumption are organically related. Better health outcomes not only induce population expansion; they also boost the working abilities of the labor force, thus accelerating economic growth. Again, population expansion will require more energy to sustain the population’s growth pace. In contrast to economic development, industry flourishes, resulting in many environmental pollutants such as CO
2 emissions, waste, etc. [
8].
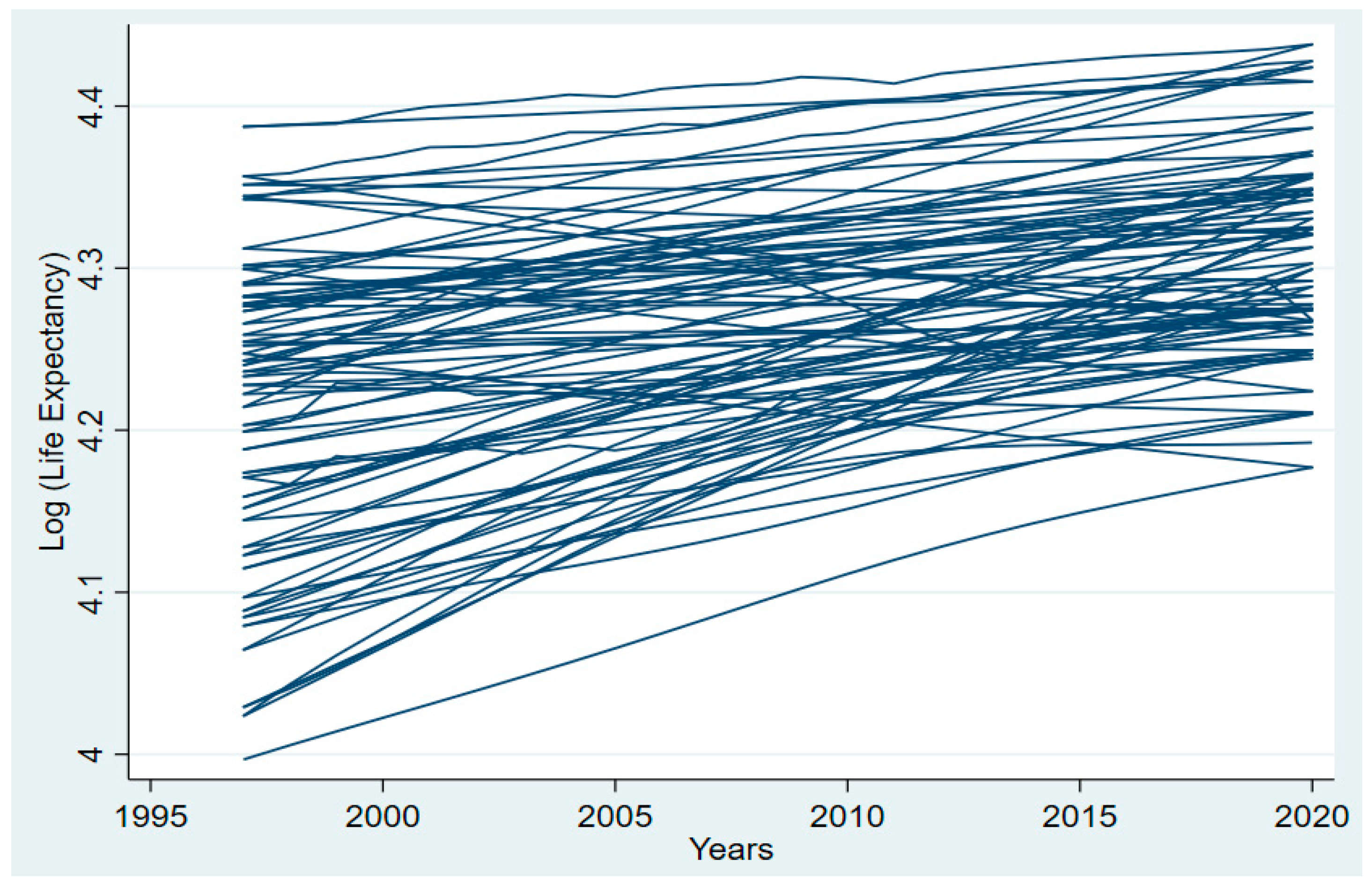
Figure 1 shows that increases in both longevity and health have contributed to a dramatic increase in life expectancy in recent decades across Asia. In 1997, health outcomes were 4.2, and in 2019, the log of health outcomes improved to 4.3 in Asia. Improved healthcare infrastructure, wider availability of medical technologies and pharmaceuticals, and progress in medical research are all contributing factors to these outcomes. Higher incomes have led to better nutrition and living circumstances, as well as expanded access to energy consumption, all of which have contributed significantly to economic growth and development. Social progress has helped to increase life expectancy by encouraging people to lead healthier lives, decreasing their use of cigarettes and alcohol, and enhancing public health policy. If the trend of rising life expectancy in Asia continues, it will be a welcome sign of the region’s prosperity and future potential.
The 46 nations and territories of the Asia Pacific Region of the World Health Organization (WHO) cover a huge, densely inhabited land region and an equally enormous, sparsely populated ocean. The area encompasses 21% of the earth’s surface and is home to 53% of the global population. The list of Asian nations where the study was conducted can be found in
Appendix A. Even though the region has had impressive economic growth in recent years, the advantages of such growth are not equally dispersed, with several nations and a worryingly sizable portion of the people being left behind in the development process, living in poverty and deteriorating health [
9]. The Asia Pacific region has more impoverished people than the rest of the globe combined [
10]. Although the area has some significant historical and cultural linkages, it is not uniform. The huge differences between and within Asia Pacific nations present a major public health problem. Annually, hundreds of millions of people are at risk from epidemics and natural catastrophes, and in some fast-emerging countries, health disparities are widening. Environmental, economic, and metabolic illnesses have accompanied economic expansion [
11]. Consequently, it is vital to assess the state of health of the Asian continent and to determine the variables that influence health outcomes.
Health and economic growth are important in Asian nations considering their geographic location [
12]. In terms of both nominal GDP and PPP, Asia has the world’s biggest regional economy [
13]. According to figures provided using IMF [
14] data, the nominal size of the 46-nation Asian economy in 2021 was estimated to be approximately USD 36.8 trillion. Asia is responsible for 39% of the global GDP. Its shares are over 47.5% of the global USD 68.7 trillion in PPP terms. After surpassing Europe in 2010, Asia has had the biggest regional economy [
13]. In nominal terms, Asia outranks North America, which is placed second by USD 10 trillion. Asia’s GDP is twice as large as Europe’s, ranked second in PPP terms. Whereas the economies of a few Asian nations have expanded rapidly in recent years, most of the continent’s inhabitants have not shared in these benefits [
15]. According to the World Bank [
16], 36% of South Asians and 14% of East Asian and Pacific residents earn less than USD 1.25 a day. Historically, three main factors—better nutrition, improved infrastructure for public health (such as improved sanitation and the quality of freshwater resources), and enhanced medical technology—have all been linked to economic development in the long term [
17]. Numerous research findings demonstrate this well-known connection between income and health within and across countries [
18,
19]. People live longer and endure fewer years of impairment while living in countries with higher average wages [
20]. Anemia is less prevalent among women in countries with higher incomes. The birth weights of infants in these nations are higher. People with greater earnings have a longer lifespan within nations. Children from wealthy backgrounds tend to have better health. Infant and child mortality rates, in addition to child disease, are decreasing [
17]. Even if economic development and health have a substantial relationship, there is very little research in Asia that is related to this issue. As such, it is important to figure out how economic growth impacts health outcomes in Asia.
Together, the Asia Pacific region makes up a sizable, varied, and energetic area that is home to 4.7 billion people who reside in nations that span from the largest energy consumer to island countries that are the most susceptible to climate change’s consequences [
21]. The area consumes more than half of the energy used globally, with fossil fuels making up 85% of total consumption [
16]. Over the previous ten years, electrification rates have increased significantly, reaching 96.6 percent in the region in 2019 [
21]. Alternative and renewable energy’s percentage in global final energy consumption is growing quickly, achieving more than 8.5% in 2018 [
22]. The greatest improvements were seen in power generation, where renewable energy made up 22.1% of all electricity produced in 2018, up gradually from 16.1% in 2010 [
21]. Creating power and heat via the combustion of fossil fuels—gas, coal, or oil—results in significant emissions of GHG, such as CO
2 and NO
2 [
23]. Numerous adverse consequences on health have been attributed to prolonged exposure to CO
2. Low cognitive function, difficulty making decisions, fatigue, nausea, vomiting, and tingling feelings are among the symptoms that may arise [
24]. Thus, it is important to analyze how energy consumption is related to health outcomes in the Asia region.
In this work, we have concentrated on finding the linkage between economic progress, energy usage, and health in selected Asian countries. The objectives of this study are to determine (i) the effect of economic growth on health outcomes; (ii) the effect of energy usage on health outcomes; and (iii) whether CO2 emissions have a meaningful impact on health outcomes.
Not only does energy consumption increase economic activity, but it also increases CO
2 emissions. Even though the impact of energy growth on health outcomes in this region has been identified, many previous studies still need to pay attention to the linkage between energy usage, economic development, and health outcomes. Specifically in Asian nations, there are no recognized works on this topic. Evidentially, a healthy population is positively and significantly associated with economic expansion. In their seminal research, Bloom et al. [
25] looked at how people’s health impacts their country’s GDP. Rarely has the causality between economic growth and health outcomes been examined. Furthermore, the linkage between energy usage and health effects still needs to be proven. Evaluating the impacts of energy usage and economic expansion on health outcomes in Asian countries is consequently of utmost importance. The subsequent sections of this paper provide a literature review and statistical analysis relating to the relevant data, and the remaining sections discuss methodology, the empirical findings, and conclusions.
The countries of Asia are competing to become the world’s economic leaders. Economic output, population, healthcare spending, and energy use are all rising in these nations [
26]. Therefore, it is crucial to assess the effect of these variables on health outcomes. In light of these presumptions, this paper makes the following contributions to the current literature. The first part of the study looks at how population, income, health expenditure, and energy consumption have affected life expectancy in Asia between 1997 and 2019. Second, there is a great deal of interaction between Asian countries due to trade, religion, bilateral cooperation, and cultural exchange. There is evidence of CSD and SH issues in the data. Therefore, the paper uses cointegration tests, a cross-sectional unit root test, and CS-ARDL of the second generation to deal with data issues. To check the robustness the paper, we applied AMG and CCEMG estimators. The theoretical framework of this research is an application of Smith’s [
27] health production model to determine the effect on health outcomes. Finally, the study provides recommendations for how policymakers may approach policymaking in light issues related to income, CO
2 emissions, population, and energy usage.
2. Literature Review
Several investigations have been undertaken on the links between health, economic growth, and energy usage. These studies proceed country by country or worldwide.
Mankiw et al. [
28] used health as a human resource factor in their economic development analysis. Barro [
6] presented a growth model that used health capital, physical capital inputs, hours worked, and education level. Therefore, based on Mankiw et al. [
28], health capital is considered to be a regular production indicator. Lucas [
29] discovered a similar finding. Energy use and economic growth have been studied extensively. Granger’s causality and mediation model was employed by Gyimah et al. [
30] to explore the connection between the utilization of sustainable energy and economic expansion for the scenario of Ghana. The research findings indicated that the use of sustainable energy sources can have a sizeable and beneficial influence on economic growth [
31]. Tutak and Brodny [
32] discovered that using energy from sustainable energy sources has a favorable impact on economic development, lowering GHG emissions and minimizing traditional energy usage in almost all European Union nations [
33]. Renewable energy consumption (REC) and economic growth (EG) have a bidirectional, unidirectional, or no causal link, according to empirical studies. Ocal and Aslan [
34] studied EG and REC in Turkey. Using data from 1990 to 2010, they found that EG causes REC. Sadorsky [
35] and Salim et al. [
36] found unidirectional causation from EG to REC for 18 developing nations, Romania, and OECD countries. Numerous studies, including those of Apergis and Payne [
37], Ito [
38], Magazzino [
39], Fotourehchi [
40], and Khobai and Le Roux [
41], have observed a unidirectional causality from REC to EG.
Mujtabe and Sahazad [
42] conducted a study in OECD nations and discovered that a causality exists in the long term between renewable energy and healthcare spending. Majeed et al. [
43] examined the connection between renewable energy consumption and health outcomes in 155 economies using panel approaches such as two-stage least squares, random effects, fixed effects, pooled OLS, and the generalized method of moment (GMM). It has been empirically demonstrated that using renewable energy is beneficial to health. Using sustainable energy has been shown to prolong the average life span and decrease fatality rates. The favorable association between sustainable energy and public health indicates that sustainable energy assists in managing chronic illnesses, increases life expectancy, and reduces mortality and tuberculosis rates. Using the GMM methodology, Hanif [
44] explored the association between different patterns of energy use and the state of human health in Sub-Saharan Africa. The use of solid fuels (wood pellets, peat, charcoal, wood, agricultural waste) for cooking and the consumption of fossil fuels (gas, coal, oil) is dramatically raising the incidence of TB, according to the study’s findings. Moreover, the data demonstrate that the usage of both fossil and solid fuels has negative impacts on the expected life span in Sub-Saharan African nations by increasing the death rate. The findings suggest that economic growth and the use of renewable energy sources such as wind, sun, and water (which can prevent residents from overexposure to particulate matter and toxic pollutants) contribute to reducing mortality and managing tuberculosis.
Using time series data from Turkey, Essen and Çelik Keçili [
45] assessed the ways in which the development of an economy and health spending are related. The study found a substantial positive linkage between economic expansion and healthcare spending, employing the Granger causality and Johansen cointegration test. Chen et al. [
46] researched the ways in which factors related to economic development and the environment influence life expectancy in 20 different emerging and developed economies. The correlation coefficients between the variables were evaluated using the Pearson correlation coefficient, and the influence of each indicator on LE was determined using multiple regression models. The research found that the per capita income had a considerable favorable effect on life span in developed and developing nations. Using a full information maximum likelihood model, Miladinov [
47] explored the linkage between GDP growth and life expectancy at birth in the five EU membership candidate nations (Albania, Bosnia and Macedonia, Montenegro and Herzegovina, and Serbia). The research results demonstrated that longer life expectancy is associated with greater levels of income and lower neonatal mortality rates. Applying time series data from Pakistan, Wang et al. [
48] researched the correlation between life expectancy and economic expansion. Utilizing the ARDL bound testing method, the research found that economic growth is positively related to life expectancy.
Youssef et al. [
49] used the SUR technique to determine the causal linkage between energy usage and health outcomes. The study’s results showed that health and energy consumption have a healthy relationship. Wang [
50] examined the influence of energy usage on public health and the environment using the exposure-response approach. The findings exhibited that energy use impacts both beneficial and harmful health considerations. Arawomo et al. [
51] evaluated the dynamic connection between economic development, energy use, and health in Sub-Saharan Africa. The results of the analysis exhibited that neither energy use nor economic growth has a substantial effect on health outcomes. Smith et al. [
52] showed a unilateral causation for the association between energy use and health outcomes, but Youssef et al. [
49] found a bidirectional causality. Smith et al. [
52] found a positive and inverse linkage between energy use and health outcomes. As such, it is evident that the association between health and economic growth has been thoroughly examined under the structure of growth theories, as shown in the above literature review.
Our assessment of the literature reveals that no research has examined how energy consumption, health expenditure, and income affect health outcomes for a panel of Asian countries, and those studies on the linkage between energy use and health outcomes are scant and inconsistent, often ignoring potential CSD and SH in panel data, leading to erroneous estimations. Previous research ignored CSD and SH problems. It is important to fill this massive gap in the literature. Because of the lack of data, the conflicting results, and the methodological flaws in the existing studies, the authors opted to investigate the connection between energy use, GDP growth, and health outcomes in a sample of Asian nations.
4. Results
Table 3 demonstrates the outcomes of the CSD and indicates the interdependence between the variables. The research applied four CSD tests, so that the findings are robust. In other words, the findings of the Pesaran CSD test, the Frees test, the Friedman test, and the Pesaran abs test are shown, and there is no CSD assumed as the null hypothesis. The results of the CSD test indicate that the null hypothesis should have been rejected at the 1% significance level. This verifies that the dataset contains CSD. Similar social and economic policies account for this cross-sectional dependence.
The results of the slope homogeneity [
58] test are shown in
Table 4. For the sake of this test, we will assume that slope values are uniform continuously. The findings are shown in
Table 4, which reveals that delta tidle is significant at the 5% significance level, and delta tidle adjusted is significant at the 1% significance level. As a consequence, the model is concerned with heterogeneity, and the null hypothesis of homogeneity for slope values is rejected.
Table 5 summarizes the outcomes of the cross-sectionally augmented IPS (CIPS) unit root test. The empirical result of the CIPS unit root test exhibits that lnH, lnEC, lnCO
2, and lnPOP have unit root problems at the level. After taking the first difference, variables become significant at a 1% significance level, and they are integrated into I(1). The results also depict that lnGDP and lnHEX are significant at a 1% significance level in both the level and first difference. Therefore, the result is that lnGDP and lnHEX are integrated into I (0).
Bootstrap
p-values are taken into account while analyzing the findings of the ECM test provided by Westerland [
56] to determine whether there is a cross-sectional dependence between the series used in the analysis. The findings are interpreted taking into consideration the Group tau (G
t), Group alpha (G
a), Panel tau (P
t), and Panel alpha (P
a) critical values because of the heterogeneity between the series [
64]. The findings of the cointegration test are shown in
Table 6. The null hypothesis is that there is no long-term cointegration between the dependent variable and the independent variables. The outcome presented in
Table 6 indicates that the null hypothesis should be rejected, because the p values for G
t and P
t are highly significant at the 1% level of significance. As a consequence, there is long-term cointegration between health outcomes and other independent variables reported in this analysis in the Asian region.
The outcomes of the CS-ARDL are presented in
Table 7. The validity of CS-ARDL results has been confirmed by the CCEMG and AMG test results presented in
Table 8. The findings of the CS-ARDL results show that energy consumption has a significant positive relationship with health outcomes. The coefficients of lnEC are 0.0019 and 0.00015 in the long and short run, respectively, which means at a 1% level of significance, an increase in energy consumption of 1% will lead to an increase in health outcomes by 0.0019% in the long term and 0.00015% in short term. The results are also validated by the AMG and CCEMG tests. The findings demonstrate that countries in the Asian region consume more eco-friendly resources and renewable energy, and this is why energy consumption has a significant positive impact on health outcomes.
The results reveal a positive relationship between economic growth and health outcomes, but it is insignificant in the long run. Especially the coefficient of lnGDP is positive at 0.0018. Therefore, a 1% increase in GDP per capita will increase health outcomes by 0.0018% in the long run at a significance level of 5%. In the short term, the coefficient of lnGDP exhibits that a 1% increase in GDP will lead to an increase in health outcomes by 0.00062%. CCEMG test results confirm these results. In addition, these results are consistent with the existing research [
65,
66]. These findings suggest that as the economy grows faster, it will increase the per capita income, and higher-income people can spend more on healthcare. Thus, this study finds a positive correlation between economic growth and health outcomes in the Asian region.
The coefficients of lnHEX are 0.0012 and 0.00034 in the long and short term, respectively, which means that at a 1% significance level, a 1% increase in health expenditures will increase the health outcome by 0.0025% in the long term and 0.00034% in the short term. The test results of AMG and CCEMG confirms the results. The findings suggest that the government’s increase in general health expenditure and growth in health-related services such as hospitals, clinics, and healthcare services will positively impact public health.
The population has no significant relationship with health outcomes in the long and short term. The results were also confirmed by the AMG and CCEMG test results. This means there is no evidence of a significant relationship between health outcomes and population. The CS-ARDL, AMG, and CCEMG results show that CO2 emissions have an important negative relationship with health outcomes in the short and long term. The coefficient of lnCO2 is −0.0028 in the long term and −0.00119 in the short term and significant at a 1% significance level. The results mean that a 1% increase in CO2 will lead to declining health outcomes by 0.0028% in the long term and 0.00119% in the short run. CO2 emissions are one of the main reasons for air pollution and adversely affect public health. With the speed adjustment, the coefficient of ECT is −0.5689, indicating that the life expectancy rate converges to its long-run equilibrium by 56.89%.
The robustness results show similarity with our baseline CS-ARDL findings (
Table 8). All directions are the same except for the impact of the population in the AMG estimator. The impacts of GDP are positive and significant in both the short and long run in the CS-ARDL model. However, the impact of GDP is insignificant in the AMG estimator. On the other hand, the population impact is insignificant in the CS-ARDL model but significant in AMG estimation.
5. Discussion
Figure 2 graphically shows the influencing factors’ signs on health outcomes. The figure shows that health expenditure, energy consumption, and GDP per capita positively impact life expectancy in all estimators. On the other hand, CO
2 harms life expectancy in all estimators. Population impacts positively on life expectancy in the AMG estimator and negatively on life expectancy in the CCEMG estimator.
The observations of this study support the notion that overall energy consumption positively influences human health. Energy generated from fossil fuels generates significant CO
2 emissions and has negative health effects. In contrast, alternative energy sources benefit the environment and human health [
46,
67,
68,
69]. Thus, the practical impact of overall energy consumption on health in the Asian area indicates that renewable energy consumption outperforms nonrenewable energy consumption in this region [
70]. Renewable energy enhances life expectancy, lowers infant mortality, prevents TB cases by replacing traditional energy sources, and, as a result, enhances environmental quality. In addition, it enhances health outcomes by improving availability, cost, supply, food quality, and nutrition. The study’s findings align with Alharthi et al. [
71], Kadria et al. [
72], Sasmaz et al. [
73], and Majeed et al. [
43].
The outcome of this study has found that CO
2 emissions have a significant negative impact on health outcomes both in the short and long term. Smog, the more obvious type of air pollution, is indirectly caused by carbon dioxide. The production of smog, which is detrimental to respiratory health, is facilitated by the increased warmth and humidity caused by carbon dioxide emissions. The effects of carbon dioxide pollution on the environment and human health are multifaceted and occur in both immediate and delayed ways. These findings are consistent with Emodi et al. [
74], Oyedele [
75], and Farooq [
76].
The findings of this study have also demonstrated that health outcomes are positively influenced by economic growth and health expenditures. A high GDP (gross domestic product) typically corresponds to a large government budget and taxable income. If the government is intelligent, it should allocate a significant portion of the budget to healthcare, cleanliness, and research and development. Countries with excellent management and governance and a high GDP per capita have great food security. This indicates that the people’s food and water are wholesome and do not cause ailments such as food poisoning, diarrhea, etc. More investment in facilities that maintain cleanliness eradicates illnesses such as malaria from the nation. Water and cleanliness indicate that individuals are also healthy. Healthcare is extremely important. It should be cutting-edge, accessible, inexpensive, and continually advancing. Research and development are very important. Modern research and development have enhanced healthcare services. These findings are in line with Hlafa et al. [
77], Arthur and Oaikhenan [
78], and Oluwatoyin et al. [
79].






{kind=link}
{kind=link}