
Pain and Clinical Presentation: A Cross-Sectional Study of Patients with New-Onset Chronic Pain in Long-COVID-19 Syndrome
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
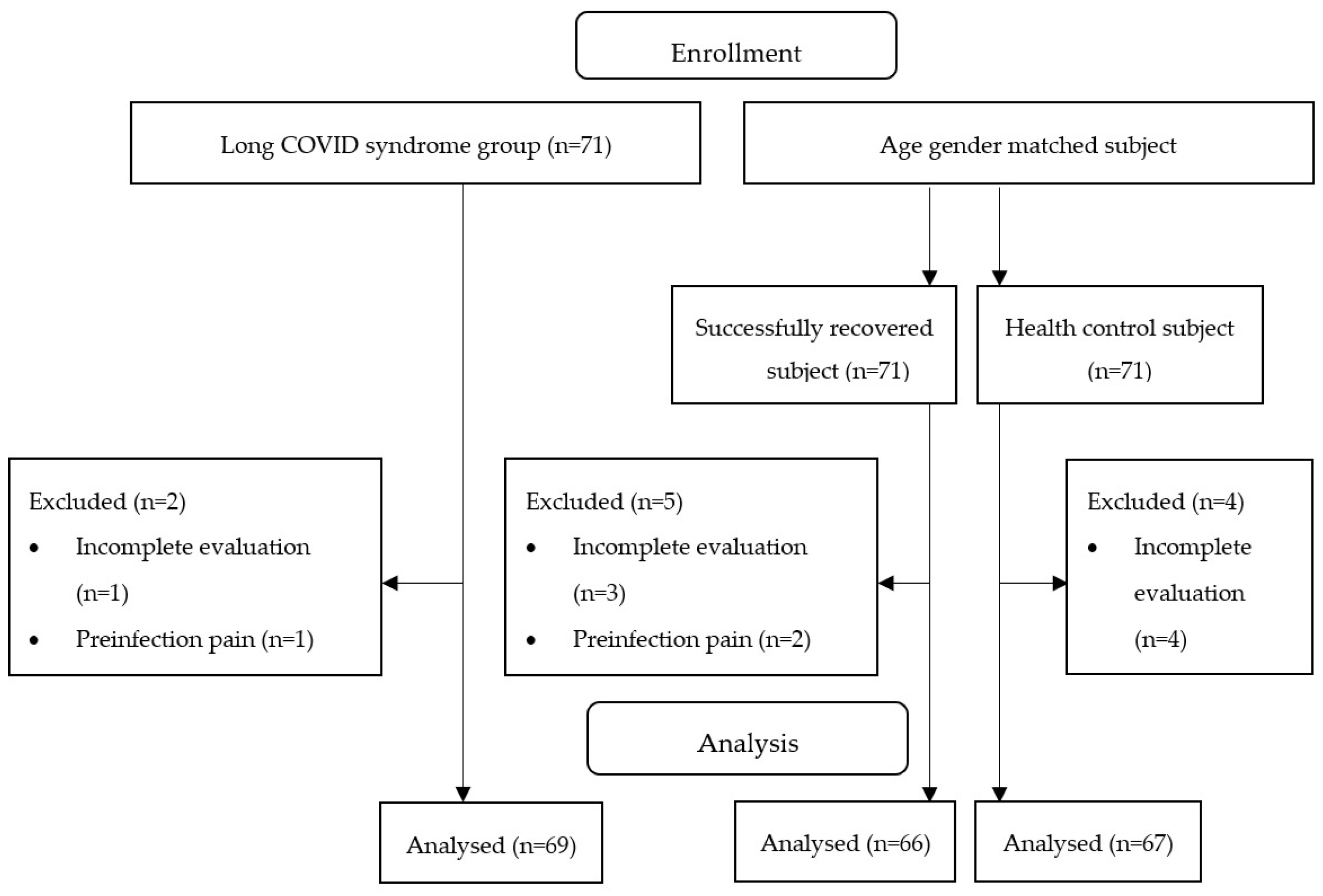
2.1. Study Design and Participants
2.2. Outcome Measures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haleem, A.; Javaid, M.; Vaishya, R. Effects of COVID-19 pandemic in daily life. Curr. Med. Res. Pract. 2020, 10, 78. [Google Scholar] [CrossRef]
- Yong, E. COVID-19 Can Last for Several Months; The Atlantic: Washington, DC, USA, 2020. [Google Scholar]
- Nabavi, N. Long covid: How to define it and how to manage it. BMJ 2020, 370, m3489. [Google Scholar] [CrossRef] [PubMed]
- Aiyegbusi, O.L.; Hughes, S.E.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S.; Haroon, S.; Price, G.; Davies, E.H.; Nirantharakumar, K.; et al. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef] [PubMed]
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 869–875. [Google Scholar] [CrossRef] [PubMed]
- What Might Long COVID Mean for the Nation’s Health? The Health Foundation. Available online: https://www.health.org.uk/news-and-comment/blogs/what-might-long-covid-mean-for-the-nations-health (accessed on 16 January 2023).
- Office for National Statistics. Prevalence of Ongoing Symptoms following Coronavirus (COVID-19) Infection in the UK. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/1july2021 (accessed on 16 January 2023).
- Babnik, K.; Staresinic, C.; Lep, Ž. Some of the workforce face post COVID after the acute phase of the illness: The employer’s supportive role. Hum. Syst. Manag. 2022, 41, 257–275. [Google Scholar] [CrossRef]
- Giorgi, G.; Lecca, L.I.; Alessio, F.; Finstad, G.L.; Bondanini, G.; Lulli, L.G.; Arcangeli, G.; Mucci, N. COVID-19-related mental health effects in the workplace: A narrative review. Int. J. Environ. Res. Public Health 2020, 17, 7857. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. Job demands-resources theory: Taking stock and looking forward. J. Occup. Health Psychol. 2017, 22, 273–285. [Google Scholar] [CrossRef]
- Bileviciute-Ljungar, I.; Norrefalk, J.R.; Borg, K. Pain Burden in Post-COVID-19 Syndrome following Mild COVID-19 Infection. J. Clin. Med. 2022, 11, 771. [Google Scholar] [CrossRef]
- Clauw, D.J.; Häuser, W.; Cohen, S.P.; Fitzcharles, M.A. Considering the potential for an increase in chronic pain after the COVID-19 pandemic. Pain 2020, 161, 1694–1697. [Google Scholar] [CrossRef]
- Su, S.; Cui, H.; Wang, T.; Shen, X.; Ma, C. Pain: A potential new label of COVID-19. Brain Behav. Immun. 2020, 87, 159–160. [Google Scholar] [CrossRef]
- Nicholas, M.K.; Linton, S.J.; Watson, P.J.; Main, C.J. “Decade of the Flags” Working Group. Early identification and management of psychological risk factors (“yellow flags”) in patients with low back pain: A reappraisal. Phys. Ther. 2011, 91, 737–753. [Google Scholar] [CrossRef]
- Gatchel, R.J.; Peng, Y.B.; Peters, M.L.; Fuchs, P.N.; Turk, D.C. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol. Bull. 2007, 133, 581–624. [Google Scholar] [CrossRef] [PubMed]
- Soares, F.H.C.; Kubota, G.T.; Fernandes, A.M.; Hojo, B.; Couras, C.; Costa, B.V.; Lapa, J.D.D.S.; Braga, L.M.; Almeida, M.M.D.; Cunha, P.H.M.D.; et al. Prevalence and characteristics of new-onset pain in COVID-19 survivours, a controlled study. Eur. J. Pain 2021, 25, 1342–1354. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. World Medical Association declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA—J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Buhr, R.G.; Jackson, N.J.; Kominski, G.F.; Dubinett, S.M.; Ong, M.K.; Mangione, C.M. Comorbidity and thirty-day hospital readmission odds in chronic obstructive pulmonary disease: A comparison of the Charlson and Elixhauser comorbidity indices. BMC Health Serv. Res. 2019, 19, 701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groll, D.L.; Heyland, D.K.; Caeser, M.; Wright, J.G. Assessment of long-term physical function in acute respiratory distress syndrome (ARDS) patients: Comparison of the Charlson Comorbidity Index and the Functional Comorbidity Index. Am. J. Phys. Med. Rehabil. 2006, 85, 574–581. [Google Scholar] [CrossRef] [PubMed]
- Tuty Kuswardhani, R.A.; Henrina, J.; Pranata, R.; Anthonius Lim, M.; Lawrensia, S.; Suastika, K. Charlson comorbidity index and a composite of poor outcomes in COVID-19 patients: A systematic review and meta-analysis. Diabetes Metab. Syndr. 2020, 14, 2103–2109. [Google Scholar] [CrossRef] [PubMed]
- Keller, S.; Bann, C.M.; Dodd, S.L.; Schein, J.; Mendoza, T.R.; Cleeland, C.S. Validity of the brief pain inventory for use in documenting the outcomes of patients with noncancer pain. Clin. J. Pain 2004, 20, 309–318. [Google Scholar] [CrossRef]
- Tan, G.; Jensen, M.P.; Thornby, J.I.; Shanti, B.F. Validation of the brief pain inventory for chronic nonmalignant pain. J. Pain 2004, 5, 133–137. [Google Scholar] [CrossRef]
- Chen, Y.W.; HajGhanbari, B.; Road, J.D.; Coxson, H.O.; Camp, P.G.; Reid, W.D. Reliability and validity of the Brief Pain Inventory in individuals with chronic obstructive pulmonary disease. Eur. J. Pain 2018, 22, 1718–1726. [Google Scholar] [CrossRef]
- HajGhanbari, B.; Holsti, L.; Road, J.D.; Darlene Reid, W. Pain in people with chronic obstructive pulmonary disease (COPD). Respir. Med. 2012, 106, 998–1005. [Google Scholar] [CrossRef] [Green Version]
- Melzack, R. The McGill Pain Questionnaire: Major properties and scoring methods. Pain 1975, 1, 277–299. [Google Scholar] [CrossRef]
- Melzack, R. The short-form McGill pain questionnaire. Pain 1987, 30, 191–197. [Google Scholar] [CrossRef]
- Mason, S.T.; Arceneaux, L.L.; Abouhassan, W.; Lauterbach, D.; Seebach, C.; Fauerbach, J.A. Confirmatory factor analysis of the Short Form McGill Pain Questionnaire with burn patients. Eplasty 2008, 8, e54. [Google Scholar]
- Reading, A.E.; Everitt, B.S.; Sledmere, C.M. The McGill Pain Questionnaire: A replication of its construction. Br. J. Clin. Psychol. 1982, 21 Pt 4, 339–349. [Google Scholar] [CrossRef]
- HajGhanbari, B.; Garland, S.J.; Road, J.D.; Reid, W.D. Pain and physical performance in people with COPD. Respir. Med. 2013, 107, 1692–1699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clauw, D.J. Fibromyalgia: A clinical review. JAMA—J. Am. Med. Assoc. 2014, 311, 1547–1555. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [Green Version]
- Dudeney, J.; Law, E.F.; Meyyappan, A.; Palermo, T.M.; Rabbitts, J.A. Evaluating the psychometric properties of the Widespread Pain Index and the Symptom Severity scale in youth with painful conditions. Can. J. Pain 2019, 3, 137–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galvez-Sánchez, C.M.; de la Coba, P.; Duschek, S.; Reyes Del Paso, G.A. Reliability, Factor Structure and Predictive Validity of the Widespread Pain Index and Symptom Severity Scales of the 2010 American College of Rheumatology Criteria of Fibromyalgia. J. Clin. Med. 2020, 9, 2460. [Google Scholar] [CrossRef]
- Barbero, M.; Moresi, F.; Leoni, D.; Gatti, R.; Egloff, M.; Falla, D. Test-retest reliability of pain extent and pain location using a novel method for pain drawing analysis. Eur. J. Pain 2015, 19, 1129–1138. [Google Scholar] [CrossRef]
- Falla, D.; Peolsson, A.; Peterson, G.; Ludvigsson, M.L.; Soldini, E.; Schneebeli, A.; Barbero, M. Perceived pain extent is associated with disability, depression and self-efficacy in individuals with whiplash-associated disorders. Eur. J. Pain 2016, 20, 1490–1501. [Google Scholar] [CrossRef] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Nolan, C.M.; Longworth, L.; Lord, J.; Canavan, J.L.; Jones, S.E.; Kon, S.S.; Man, W.D. The EQ-5D-5L health status questionnaire in COPD: Validity, responsiveness and minimum important difference. Thorax 2016, 71, 493–500. [Google Scholar] [CrossRef] [Green Version]
- Arab-Zozani, M.; Hashemi, F.; Safari, H.; Yousefi, M.; Ameri, H. Health-Related Quality of Life and its Associated Factors in COVID-19 Patients. Osong Public Health Res. Perspect. 2020, 11, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Meys, R.; Delbressine, J.M.; Goërtz, Y.M.; Vaes, A.W.; Machado, F.V.; Van Herck, M.; Burtin, C.; Posthuma, R.; Spaetgens, B.; Franssen, F.M.; et al. Generic and Respiratory-Specific Quality of Life in Non-Hospitalized Patients with COVID-19. J. Clin. Med. 2020, 9, 3993. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Navarro-Santana, M.; Plaza-Manzano, G.; Palacios-Ceña, D.; Arendt-Nielsen, L. Time course prevalence of post-COVID pain symptoms of musculoskeletal origin in patients who had survived severe acute respiratory syndrome coronavirus 2 infection: A systematic review and meta-analysis. Pain 2022, 163, 1220–1231. [Google Scholar] [CrossRef] [PubMed]
- Seang, S.; Itani, O.; Monsel, G.; Abdi, B.; Marcelin, A.G.; Valantin, M.A.; Palich, R.; Fayçal, A.; Pourcher, V.; Katlama, C.; et al. Long COVID-19 symptoms: Clinical characteristics and recovery rate among non-severe outpatients over a six-month follow-up. Infect. Dis. Now 2022, 52, 165–169. [Google Scholar] [CrossRef]
- Pelà, G.; Goldoni, M.; Solinas, E.; Cavalli, C.; Tagliaferri, S.; Ranzieri, S.; Frizzelli, A.; Marchi, L.; Mori, P.A.; Majori, M.; et al. Sex-Related Differences in Long-COVID-19 Syndrome. J. Women’s Health 2022, 31, 620–630. [Google Scholar] [CrossRef]
- Muus, C.; Luecken, M.D.; Eraslan, G.; Sikkema, L.; Waghray, A.; Heimberg, G.; Kobayashi, Y.; Vaishnav, E.D.; Subramanian, A.; Smillie, C.; et al. Single-cell meta-analysis of SARS-CoV-2 entry genes across tissues and demographics. Nat. Med. 2021, 27, 546–559. [Google Scholar] [CrossRef]
- Bilgin, A.; Kesik, G.; Özdemir, L. Biopsychosocial Factors Predicting Pain Among Individuals Experiencing the Novel Coronavirus Disease (COVID-19). Pain Manag. Nurs. Off. J. Am. Soc. Pain Manag. Nurs. 2022, 23, 79–86. [Google Scholar] [CrossRef]
- Vahidy, F.S.; Pan, A.P.; Ahnstedt, H.; Munshi, Y.; Choi, H.A.; Tiruneh, Y.; Nasir, K.; Kash, B.A.; Andrieni, J.D.; McCullough, L.D. Sex differences in susceptibility, severity, and outcomes of coronavirus disease 2019: Cross-sectional analysis from a diverse US metropolitan area. PLoS ONE 2021, 16, e0245556. [Google Scholar] [CrossRef]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Sharma, G.; Volgman, A.S.; Michos, E.D. Sex Differences in Mortality From COVID-19 Pandemic: Are Men Vulnerable and Women Protected? JACC Case Rep. 2020, 2, 1407–1410. [Google Scholar] [CrossRef]
- Stewart, S.; Newson, L.; Briggs, T.A.; Grammatopoulos, D.; Young, L.; Gill, P. Long COVID risk—A signal to address sex hormones and women’s health. Lancet Reg. Health–Eur. 2021, 11, 100242. [Google Scholar] [CrossRef]
- Klein, S.L. Sex influences immune responses to viruses, and efficacy of prophylaxis and treatments for viral diseases. Bioessays 2012, 34, 1050–1059. [Google Scholar] [CrossRef] [Green Version]
- Spini, A.; Giudice, V.; Brancaleone, V.; Morgese, M.G.; De Francia, S.; Filippelli, A.; Ruggieri, A.; Ziche, M.; Ortona, E.; Cignarella, A.; et al. Sex-tailored pharmacology and COVID-19: Next steps towards appropriateness and health equity. Pharmacol. Res. 2021, 173, 105848. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Rodríguez-Jiménez, J.; Fuensalida-Novo, S.; Palacios-Ceña, M.; Gómez-Mayordomo, V.; Florencio, L.L.; Hernández-Barrera, V.; Arendt-Nielsen, L. Myalgia as a symptom at hospital admission by severe acute respiratory syndrome coronavirus 2 infection is associated with persistent musculoskeletal pain as long-term post-COVID sequelae: A case-control study. Pain 2021, 162, 2832–2840. [Google Scholar] [CrossRef]
- Goërtz, Y.M.; Van Herck, M.; Delbressine, J.M.; Vaes, A.W.; Meys, R.; Machado, F.V.; Houben-Wilke, S.; Burtin, C.; Posthuma, R.; Franssen, F.M.; et al. Persistent symptoms 3 months after a SARS-CoV-2 infection: The post-COVID-19 syndrome? ERJ Open Res. 2020, 6, 00542-2020. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, K.B.; Rao, M.; Bonilla, H.; Subramanian, A.; Hack, I.; Madrigal, M.; Singh, U.; Jagannathan, P.; Grant, P. Patients with Uncomplicated Coronavirus Disease 2019 (COVID-19) Have Long-Term Persistent Symptoms and Functional Impairment Similar to Patients with Severe COVID-19: A Cautionary Tale during a Global Pandemic. Clin. Infect. Dis. 2021, 73, e826–e829. [Google Scholar] [CrossRef]
- Iqbal, A.; Iqbal, K.; Ali, S.A.; Azim, D.; Farid, E.; Baig, M.D.; Arif, T.B.; Raza, M. The COVID-19 Sequelae: A Cross-Sectional Evaluation of Post-recovery Symptoms and the Need for Rehabilitation of COVID-19 Survivors. Cureus 2021, 13, e13080. [Google Scholar] [CrossRef]
- Stavem, K.; Ghanima, W.; Olsen, M.K.; Gilboe, H.M.; Einvik, G. Persistent symptoms 1.5-6 months after COVID-19 in non-hospitalised subjects: A population-based cohort study. Thorax 2021, 76, 405–407. [Google Scholar] [CrossRef] [PubMed]
- Havervall, S.; Rosell, A.; Phillipson, M.; Mangsbo, S.M.; Nilsson, P.; Hober, S.; Thålin, C. Symptoms and Functional Impairment Assessed 8 Months after Mild COVID-19 among Health Care Workers. JAMA—J. Am. Med. Assoc. 2021, 325, 2015–2016. [Google Scholar] [CrossRef]
- Graham, E.L.; Clark, J.R.; Orban, Z.S.; Lim, P.H.; Szymanski, A.L.; Taylor, C.; DiBiase, R.M.; Jia, D.T.; Balabanov, R.; Ho, S.U.; et al. Persistent neurologic symptoms and cognitive dysfunction in non-hospitalized Covid-19 “long haulers”. Ann. Clin. Transl. Neurol. 2021, 8, 1073–1085. [Google Scholar] [CrossRef]
- Adnan, J.W.; Saleemi, H.; Shafqat, A.; Arif, M.; Hamid, K. Tendency of post COVID muscle and joint pains. Med. Forum Mon. 2021, 32, 161–163. [Google Scholar]
- Taquet, M.; Dercon, Q.; Luciano, S.; Geddes, J.R.; Husain, M.; Harrison, P.J. Incidence, co-occurrence, and evolution of long-COVID features: A 6-month retrospective cohort study of 273,618 survivors of COVID-19. PLoS Med. 2021, 18, e1003773. [Google Scholar] [CrossRef]
- Kayaaslan, B.; Eser, F.; Kalem, A.K.; Kaya, G.; Kaplan, B.; Kacar, D.; Hasanoglu, I.; Coskun, B.; Guner, R. Post-COVID syndrome: A single-center questionnaire study on 1007 participants recovered from COVID-19. J. Med. Virol. 2021, 93, 6566–6574. [Google Scholar] [CrossRef]
- Bittencourt, J.V.; Reis, F.J.J.; Nogueira, L.A.C. Pain in COVID-19 patients: A call to action for physical therapists to provide pain management after an episode of COVID-19. Braz. J. Phys. Ther. 2021, 25, 367–368. [Google Scholar] [CrossRef]
- Mulchandani, R.; Lyngdoh, T.; Kakkar, A.K. Deciphering the COVID-19 cytokine storm: Systematic review and meta-analysis. Eur. J. Clin. Investig. 2021, 51, e13429. [Google Scholar] [CrossRef] [PubMed]
- Disser, N.P.; De Micheli, A.J.; Schonk, M.M.; Konnaris, M.A.; Piacentini, A.N.; Edon, D.L.; Toresdahl, B.G.; Rodeo, S.A.; Casey, E.K.; Mendias, C.L. Musculoskeletal Consequences of COVID-19. J. Bone Jt. Surg. Am. Vol. 2020, 102, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Danda, D.; Kavadichanda, C.; Das, S.; Adarsh, M.B.; Negi, V.S. Autoimmune and rheumatic musculoskeletal diseases as a consequence of SARS-CoV-2 infection and its treatment. Rheumatol. Int. 2020, 40, 1539–1554. [Google Scholar] [CrossRef]
- Ramakrishnan, R.K.; Kashour, T.; Hamid, Q.; Halwani, R.; Tleyjeh, I.M. Unraveling the Mystery Surrounding Post-Acute Sequelae of COVID-19. Front. Immunol. 2021, 12, 686029. [Google Scholar] [CrossRef] [PubMed]
- Maamar, M.; Artime, A.; Pariente, E.; Fierro, P.; Ruiz, Y.; Gutiérrez, S.; Tobalina, M.; Díaz-Salazar, S.; Ramos, C.; Olmos, J.M.; et al. Post-COVID-19 syndrome, low-grade inflammation and inflammatory markers: A cross-sectional study. Curr. Med. Res. Opin. 2022, 38, 901–909. [Google Scholar] [CrossRef]
- Kemp, H.I.; Corner, E.; Colvin, L.A. Chronic pain after COVID-19: Implications for rehabilitation. Br. J. Anaesth. 2020, 125, 436–440. [Google Scholar] [CrossRef]
- Sykes, D.L.; Holdsworth, L.; Jawad, N.; Gunasekera, P.; Morice, A.H.; Crooks, M.G. Post-COVID-19 Symptom Burden: What is Long-COVID and How Should We Manage It? Lung 2021, 199, 113–119. [Google Scholar] [CrossRef]
- van Isselt, E.F.V.D.; Groenewegen-Sipkema, K.H.; Spruit-van Eijk, M.; Chavannes, N.H.; De Waal, M.W.; Janssen, D.J.; Achterberg, W.P. Pain in patients with COPD: A systematic review and meta-analysis. BMJ Open 2014, 4, e005898. [Google Scholar] [CrossRef] [Green Version]
- Bentsen, S.B.; Rustøen, T.; Miaskowski, C. Prevalence and characteristics of pain in patients with chronic obstructive pulmonary disease compared to the Norwegian general population. J. Pain 2011, 12, 539–545. [Google Scholar] [CrossRef]
- Murat, S.; Dogruoz Karatekin, B.; Icagasioglu, A.; Ulasoglu, C.; İçten, S.; Incealtin, O. Clinical presentations of pain in patients with COVID-19 infection. Ir. J. Med. Sci. 2021, 190, 913–917. [Google Scholar] [CrossRef] [PubMed]
- Oguz-Akarsu, E.; Gullu, G.; Kilic, E.; Dinc, Y.; Ursavas, A.; Yilmaz, E.; Zarifoglu, M.; Karli, N.; Pandemic Study Team; Akalın, H.; et al. Insight into pain syndromes in acute phase of mild-to-moderate COVID-19: Frequency, clinical characteristics, and associated factors. Eur. J. Pain 2022, 26, 492–504. [Google Scholar] [CrossRef] [PubMed]
- Tuzun, S.; Keles, A.; Okutan, D.; Yildiran, T.; Palamar, D. Assessment of musculoskeletal pain, fatigue and grip strength in hospitalized patients with COVID-19. Eur. J. Phys. Rehabil. Med. 2021, 57, 653–662. [Google Scholar] [CrossRef]
- Bakılan, F.; Gökmen, İ.G.; Ortanca, B.; Uçan, A.; Eker Güvenç, Ş.; Şahin Mutlu, F.; Gökmen, H.M.; Ekim, A. Musculoskeletal symptoms and related factors in postacute COVID-19 patients. Int. J. Clin. Pract. 2021, 75, e14734. [Google Scholar] [CrossRef]
- Karaarslan, F.; Demircioğlu Güneri, F.; Kardeş, S. Postdischarge rheumatic and musculoskeletal symptoms following hospitalization for COVID-19: Prospective follow-up by phone interviews. Rheumatol. Int. 2021, 41, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Karaarslan, F.; Güneri, F.D.; Kardeş, S. Long COVID: Rheumatologic/musculoskeletal symptoms in hospitalized COVID-19 survivors at 3 and 6 months. Clin. Rheumatol. 2022, 41, 289–296. [Google Scholar] [CrossRef]
- Wahlgren, C.; Divanoglou, A.; Larsson, M.; Nilsson, E.; Balkhed, Å.Ö.; Niward, K.; Thornberg, U.B.; Gudmundsson, E.L.; Levi, R. Rehabilitation needs following COVID-19: Five-month post-discharge clinical follow-up of individuals with concerning self-reported symptoms. EClinicalMedicine 2022, 43, 101219. [Google Scholar] [CrossRef]
- Bai, F.; Tomasoni, D.; Falcinella, C.; Barbanotti, D.; Castoldi, R.; Mulè, G.; Augello, M.; Mondatore, D.; Allegrini, M.; Cona, A.; et al. Female gender is associated with long COVID syndrome: A prospective cohort study. Clin. Microbiol. Infect. 2022, 28, 611.e9–611.e16. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Palacios-Cena, D.; Florencio, L.L.; Guerrero, A.L.; García-Azorín, D.; Hernández-Barrera, V.; Arendt-Nielsen, L. The presence of headache at onset in SARS-CoV-2 infection is associated with long-term post-COVID headache and fatigue: A case-control study. Cephalalgia 2021, 41, 1332–1341. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Arnold, D.T.; Hamilton, F.W.; Milne, A.; Morley, A.J.; Viner, J.; Attwood, M.; Noel, A.; Gunning, S.; Hatrick, J.; Hamilton, S.; et al. Patient outcomes after hospitalisation with COVID-19 and implications for follow-up: Results from a prospective UK cohort. Thorax 2021, 76, 399–401. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Logue, J.K.; Franko, N.M.; McCulloch, D.J.; McDonald, D.; Magedson, A.; Wolf, C.R.; Chu, H.Y. Sequelae in Adults at 6 Months after COVID-19 Infection. JAMA Netw. Open 2021, 4, e210830. [Google Scholar] [CrossRef]
- Gonzalez-Martinez, A.; Fanjul, V.; Ramos, C.; Serrano Ballesteros, J.; Bustamante, M.; Villa Marti, A.; Álvarez, C.; Garcia del Alamo, Y.; Vivancos, J.; Gago-Veiga, A.B. Headache during SARS-CoV-2 infection as an early symptom associated with a more benign course of disease: A case-control study. Eur. J. Neurol. 2021, 28, 3426–3436. [Google Scholar] [CrossRef]
- Bobker, S.M.; Robbins, M.S. COVID-19 and headache: A primer for trainees. Headache 2020, 60, 1806–1811. [Google Scholar] [CrossRef]
- Bohmwald, K.; Gálvez, N.M.S.; Ríos, M.; Kalergis, A.M. Neurologic Alterations Due to Respiratory Virus Infections. Front. Cell. Neurosci. 2018, 12, 386. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Chhabra, N.; Grill, M.F.; Singh, R.B.H. Post-COVID Headache: A Literature Review. Curr. Pain Headache Rep. 2022, 26, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Kang, H.; Li, S.; Zhao, X. Understanding the neurotropic characteristics of SARS-CoV-2: From neurological manifestations of COVID-19 to potential neurotropic mechanisms. J. Neurol. 2020, 267, 2179–2184. [Google Scholar] [CrossRef]
- Tamariz, L.; Bast, E.; Abad, M.; Klimas, N.; Caralis, P.; Palacio, A. Post COVID-19 joint pain: Preliminary report of the relationship with antinuclear antibodies and inflammation. J. Med. Virol. 2022, 94, 3479–3481. [Google Scholar] [CrossRef] [PubMed]
- Joshi, D.; Gyanpuri, V.; Pathak, A.; Chaurasia, R.N.; Mishra, V.N.; Kumar, A.; Singh, V.K.; Dhiman, N.R. Neuropathic Pain Associated with COVID-19: A Systematic Review of Case Reports. Curr. Pain Headache Rep. 2022, 26, 595–603. [Google Scholar] [CrossRef]
- El-Tallawy, S.N.; Nalamasu, R.; Pergolizzi, J.V.; Gharibo, C. Pain Management During the COVID-19 Pandemic. Pain Ther. 2020, 9, 453–466. [Google Scholar] [CrossRef]
- Lacasse, A.; Pagé, M.G.; Dassieu, L.; Sourial, N.; Janelle-Montcalm, A.; Dorais, M.; Nguefack, H.L.N.; Godbout-Parent, M.; Hudspith, M.; Moor, G.; et al. Impact of the COVID-19 pandemic on the pharmacological, physical, and psychological treatments of pain: Findings from the Chronic Pain & COVID-19 Pan-Canadian Study. Pain Rep. 2021, 6, e891. [Google Scholar] [CrossRef] [PubMed]
- Şahin, T.; Ayyildiz, A.; Gencer-Atalay, K.; Akgün, C.; Özdemir, H.M.; Kuran, B. Pain Symptoms in COVID-19. Am. J. Phys. Med. Rehabil. 2021, 100, 307–312. [Google Scholar] [CrossRef]
- Muñoz-Corona, C.; Gutiérrez-Canales, L.G.; Ortiz-Ledesma, C.; Martínez-Navarro, L.J.; Macías, A.E.; Scavo-Montes, D.A.; Guaní-Guerra, E. Quality of life and persistence of COVID-19 symptoms 90 days after hospital discharge. J. Int. Med. Res. 2022, 50, 3000605221110492. [Google Scholar] [CrossRef]
- Korkut, S.; Ülker, T. The Effect of Pain Experienced During the COVID-19 Infection on the Fear of Pain and Quality of Life. Pain Manag. Nurs. Off. J. Am. Soc. Pain Manag. Nurs. 2022, 23, 31–37. [Google Scholar] [CrossRef]
- Pires, R.E.; Reis, I.G.N.; Waldolato, G.S.; Pires, D.D.; Bidolegui, F.; Giordano, V. What Do We Need to Know About Musculoskeletal Manifestations of COVID-19?: A Systematic Review. JBJS Rev. 2022, 10, e22. [Google Scholar] [CrossRef] [PubMed]
- Galli, U.; Ettlin, D.A.; Palla, S.; Ehlert, U.; Gaab, J. Do illness perceptions predict pain-related disability and mood in chronic orofacial pain patients? A 6-month follow-up study. Eur. J. Pain 2010, 14, 550–558. [Google Scholar] [CrossRef] [Green Version]
- Leventhal, H.; Leventhal, E.A.; Breland, J.Y. Cognitive science speaks to the “common-sense” of chronic illness management. Ann. Behav. Med. 2011, 41, 152–163. [Google Scholar] [CrossRef] [PubMed]
- Petrie, K.J.; Weinman, J. Patients’ perceptions of their illness: The dynamo of volition in health care. Curr. Dir. Psychol. Sci. 2012, 21, 60–65. [Google Scholar] [CrossRef]
- O’Connor, D.P. Comparison of two psychometric scaling methods for ratings of acute musculoskeletal pain. Pain 2004, 110, 488–494. [Google Scholar] [CrossRef]
- Silva, O.F.D.; da Silva, J.M.N.; Silva, L.K.D.; Lima, T.D.F.M.; Bornia, A.C.; Souza, L.A.H.D.; Leite, W.K.D.S.; Vieira, E.M.D.A. Do men and women have different musculoskeletal symptoms at the same musculoskeletal discomfort level? Ergonomics 2022, 65, 1486–1508. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | Long-COVID-19 Syndrome Group (n = 69) | Successfully Recovered COVID-19 Group (n = 66) | Healthy Control Group (n = 67) | F |
|---|---|---|---|---|
| Age | 44.99 ± 2.79 | 44.90 ± 2.94 | 44.67 ± 3.11 | 0.144 |
| Sex (% female) | 75.26 | 75.79 | 75.51 | 0.973 |
| Weeks since infection | 104.23 ± 11.36 | 103.26 ± 8.96 | 0.300 | |
| BMI (kg/m2) | 25.16 ± 3.07 | 25.19 ± 3.19 | 25.38 ± 3.6 | 0.052 |
| Smoker (%) | 13.0 | 22.9 | 17.2 | 0.432 |
| Other diseases (%) | 31.5 | 22.9 | 24.1 | 0.497 |
| Charlson index | 0.17 ± 0.38 | 0.15 ± 0.41 | 0.24 ± 0.51 | 0.488 |
| Non-pharmacological treatment (%) | 39.2 | 24.6 | 20 | 0.056 |
| Physiotherapy | 76.32 | 64.29 | 83.33 | |
| Psychology | 23.68 | 35.71 | 16.66 | |
| Pharmacological treatment for pain (%) | 74.2 | 14 | 13.3 | <0.001 ** |
| NSAIDs | 31.9 | 50 | 25 | |
| Paracetamol | 19.4 | 37.5 | 50 | |
| Muscle relaxants | 13.9 | 12.5 | 25 | |
| Tramadol | 12.5 | 0 | 0 | |
| Codeine | 2.8 | 0 | 0 | |
| Metamizole | 19.4 | 0 | 0 |
| Variables | Long-COVID-19 Syndrome Group (n = 69) | Successfully Recovered COVID-19 Group (n = 66) | Healthy Control Group (n = 67) | F |
|---|---|---|---|---|
| Pain prevalence (%) | 69.5 | 26.3 | 23.3 | <0.001 * |
| BPI-intensity | 5.12 ± 2.28 | 0.93 ± 1.74 | 0.75 ± 1.48 | 101.88 bc |
| BPI-interference | 5.78 ± 2.77 | 0.82 ± 1.87 | 0.51 ± 1.41 | 107.73 bc |
| SF-MPQ-sensory subscale | 15.99 ± 6.89 | 2.94 ± 4.43 | 2.8 ± 5.54 | 108.79 bc |
| SF-MPQ-affective subscale | 5.75 ± 3.33 | 0.83 ± 1.29 | 0.67 ± 1.84 | 81.54 bc |
| SF-MPQ-overall score | 21.74 ± 9.51 | 3.77 ± 5.62 | 3.47 ± 6.96 | 114.46 bc |
| SF-MPQ-VAS | 65.11 ± 22.8 | 15.75 ± 22.92 | 11.62 ± 21.14 | 115.41 bc |
| SF-MPQ-PPI | 2.53 ± 1.35 | 0.49 ± 0.89 | 0.31 ± 0.66 | 78.36 bc |
| Variables | Long-COVID-19 Syndrome Group (n = 69) | Successfully Recovered COVID-19 Group (n = 66) | Healthy Control Group (n = 67) | F |
|---|---|---|---|---|
| WPI | 10.02 ± 5.93 | 1.16 ± 2.52 | 0.9 ± 1.68 | 86.297 bc |
| EQ-5D-mobility | 2.36 ± 1.07 | 1.00 ± 0.00 | 1.17 ± 0.46 | 65.61 bc |
| EQ-5D-self-care | 1.80 ± 0.98 | 1.00 ± 0.00 | 1.03 ± 0.18 | 31.82 bc |
| EQ-5D-usual activities | 3.24 ± 0.95 | 1.04 ± 0.29 | 1.14 ± 0.44 | 225.40 bc |
| EQ-5D-anxiety or depression | 3.43 ± 0.76 | 1.26 ± 0.53 | 1.48 ± 0.68 | 216.35 bc |
| EQ-5D-pain or discomfort | 2.20 ± 1.17 | 1.47 ± 0.62 | 1.34 ± 0.61 | 18.98 bc |
| EQ-5D VAS | 42.05 ± 21.67 | 74.62 ± 28.31 | 70.76 ± 31.70 | 31.49 bc |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calvache-Mateo, A.; López-López, L.; Martín-Núñez, J.; Heredia-Ciuró, A.; Granados-Santiago, M.; Ortiz-Rubio, A.; Valenza, M.C. Pain and Clinical Presentation: A Cross-Sectional Study of Patients with New-Onset Chronic Pain in Long-COVID-19 Syndrome. Int. J. Environ. Res. Public Health 2023, 20, 4049. https://doi.org/10.3390/ijerph20054049
Calvache-Mateo A, López-López L, Martín-Núñez J, Heredia-Ciuró A, Granados-Santiago M, Ortiz-Rubio A, Valenza MC. Pain and Clinical Presentation: A Cross-Sectional Study of Patients with New-Onset Chronic Pain in Long-COVID-19 Syndrome. International Journal of Environmental Research and Public Health. 2023; 20(5):4049. https://doi.org/10.3390/ijerph20054049
Chicago/Turabian StyleCalvache-Mateo, Andrés, Laura López-López, Javier Martín-Núñez, Alejandro Heredia-Ciuró, María Granados-Santiago, Araceli Ortiz-Rubio, and Marie Carmen Valenza. 2023. "Pain and Clinical Presentation: A Cross-Sectional Study of Patients with New-Onset Chronic Pain in Long-COVID-19 Syndrome" International Journal of Environmental Research and Public Health 20, no. 5: 4049. https://doi.org/10.3390/ijerph20054049