
Acetylsalicylic Acid Effect in Colorectal Cancer Taking into Account the Role of Tobacco, Alcohol and Excess Weight

 ,
,  , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
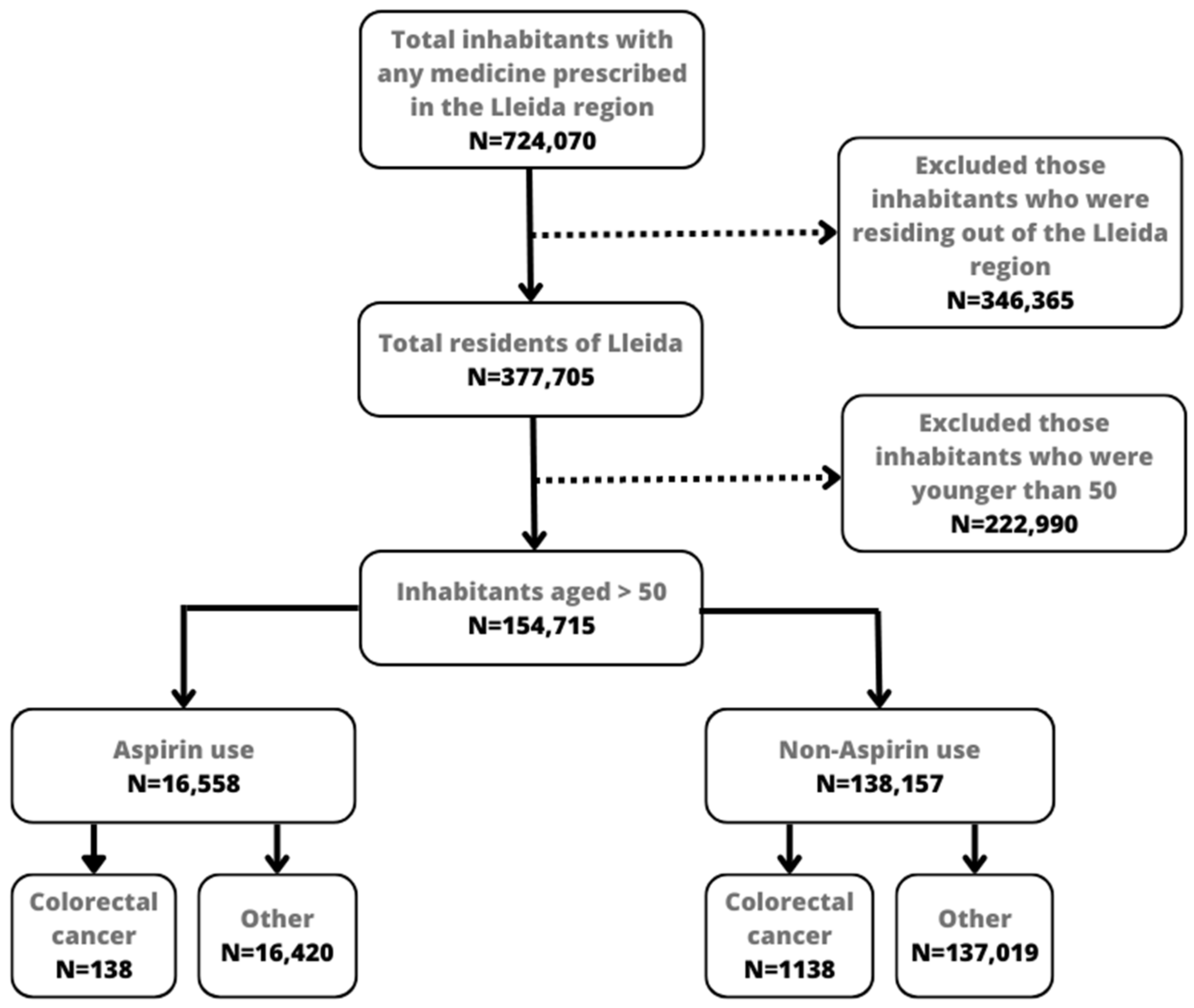
2.1. Study Population
2.2. Data Collection
2.3. Exposure
2.4. Statistical Analysis
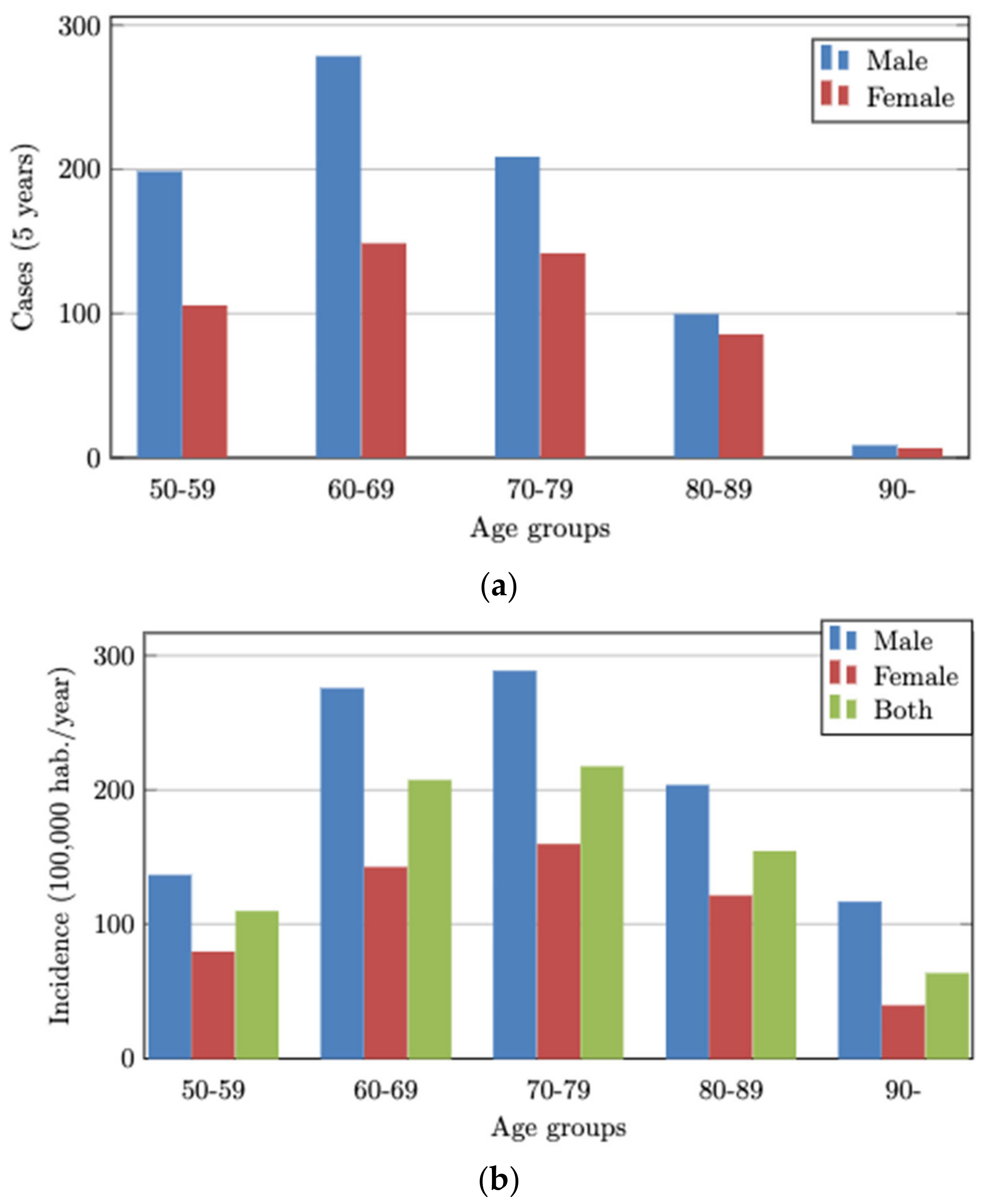
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Barsouk, A. Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Gastroenterol. Rev. Przegląd Gastroenterol. 2019, 14, 89–103. [Google Scholar] [CrossRef]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020; Available online: https://gco.iarc.fr/today (accessed on 15 February 2023).
- Cardoso, R.; Guo, F.; Heisser, T.; Hackl, M.; Ihle, P.; De Schutter, H.; Van Damme, N.; Valerianova, Z.; Atanasov, T.; Májek, O.; et al. Colorectal cancer incidence, mortality, and stage distribution in European countries in the colorectal cancer screening era: An international population-based study. Lancet Oncol. 2021, 22, 1002–1013. [Google Scholar] [CrossRef]
- Aleksandrova, K.; Pischon, T.; Jenab, M.; Bueno-de-Mesquita, H.B.; Fedirko, V.; Norat, T.; Romaguera, D.; Knüppel, S.; Boutron-Ruault, M.C.; Dossus, L.; et al. Combined impact of healthy lifestyle factors on colorectal cancer: A large European cohort study. BMC Med. 2014, 12, 168. [Google Scholar] [CrossRef] [PubMed]
- Burn, J.; Sheth, H.; Elliott, F.; Reed, L.; Macrae, F.; Mecklin, J.-P.; Möslein, G.; McRonald, F.E.; Bertario, L.; Evans, D.G.; et al. Cancer prevention with aspirin in hereditary colorectal cancer (Lynch syndrome), 10-year follow-up and registry-based 20-year data in the CAPP2 study: A double-blind, randomised, placebo-controlled trial. Lancet 2020, 395, 1855–1863. [Google Scholar] [CrossRef] [PubMed]
- Serrano, D.; Patrignani, P.; Stigliano, V.; Turchetti, D.; Sciallero, S.; Roviello, F.; D’Arpino, A.; Grattagliano, I.; Testa, S.; Oliani, C.; et al. Aspirin Colorectal Cancer Prevention in Lynch Syndrome: Recommendations in the Era of Precision Medicine. Genes 2022, 13, 460. [Google Scholar] [CrossRef] [PubMed]
- Shaukat, A.; Dostal, A.; Menk, J.; Church, T.R. BMI Is a Risk Factor for Colorectal Cancer Mortality. Dig. Dis. Sci. 2017, 62, 2511–2517. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Boakye, D.; Chen, X.; Hoffmeister, M.; Brenner, H. Association of Body Mass Index With Risk of Early-Onset Colorectal Cancer: Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2021, 116, 2173–2183. [Google Scholar] [CrossRef] [PubMed]
- Dashti, S.G.; Buchanan, D.D.; Jayasekara, H.; Ouakrim, D.A.; Clendenning, M.; Rosty, C.; Winship, I.M.; MacRae, F.A.; Giles, G.G.; Parry, S.; et al. Alcohol consumption and the risk of colorectal cancer for mismatch repair gene mutation carriers. Cancer Epidemiol. Biomarkers Prev. 2017, 26, 366–375. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Wang, X.; Huang, C.H.; Yuan, W.J.; Chen, Z.H. Passive Smoking and Risk of Colorectal Cancer: A Meta-analysis of Observational Studies. Asia Pac. J. Public Health 2016, 28, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Coyle, C.; Cafferty, F.H.; Langley, R.E. Aspirin and Colorectal Cancer Prevention and Treatment: Is It for Everyone? Curr. Colorectal Cancer Rep. 2016, 12, 27–34. [Google Scholar] [CrossRef]
- Ma, S.; Han, T.; Sun, C.; Cheng, C.; Zhang, H.; Qu, G.; Bhan, C.; Yang, H.; Guo, Z.; Yan, Y.; et al. Does aspirin reduce the incidence, recurrence, and mortality of colorectal cancer? A meta-analysis of randomized clinical trials. Int. J. Colorectal Dis. 2021, 36, 1653–1666. [Google Scholar] [CrossRef]
- Guo, C.G.; Ma, W.; Drew, D.A.; Cao, Y.; Nguyen, L.H.; Joshi, A.D.; Ng, K.; Ogino, S.; Meyerhardt, J.A.; Song, M.; et al. Aspirin Use and Risk of Colorectal Cancer Among Older Adults. JAMA Oncol. 2021, 7, 428–435. [Google Scholar] [CrossRef]
- Friis, S.; Riis, A.H.; Erichsen, R.; Baron, J.A.; Sørensen, H.T. Low-Dose Aspirin or Nonsteroidal Anti-inflammatory Drug Use and Colorectal Cancer Risk. Ann. Intern. Med. 2015, 163, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.H.; Yoo, T.G.; Jeong, S.M.; Shin, D.W. Association of Aspirin, Metformin, and Statin use with gastric cancer incidence and mortality: A nationwide cohort study. Cancer Prev. Res. 2021, 14, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Henley, S.J.; Anderson, R.N.; Thomas, C.C.; Massetti, G.M.; Peaker, B.; Richardson, L.C. Invasive cancer incidence, 2004–2013, and deaths, 2006–2015, in nonmetropolitan and metropolitan counties—United States. MMWR Surveill. Summ. 2017, 661, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Florensa, D.; Godoy, P.; Mateo, J.; Solsona, F.; Pedrol, T.; Mesas, M.; Pinol, R. The Use of Multiple Correspondence Analysis to Explore Associations between Categories of Qualitative Variables and Cancer Incidence. IEEE J. Biomed. Health Inform. 2021, 25, 3659–3667. [Google Scholar] [CrossRef] [PubMed]
- WHO|World Health Organization. Available online: https://www.who.int/en (accessed on 18 January 2023).
- Sierosławski, J.; Foster, J.; Moskalewicz, J. Survey of European drinking surveys. Alcohol survey experiences of 22 European countries. Drugs Educ. Prev. Policy 2013, 20, 383–398. [Google Scholar] [CrossRef]
- Low Risk Alcohol Consumption Thresholds. Update on the Risks Related to Alcohol Consumption Levels, Consumption Patterns and Type of Alcoholic Beverages. Available online: https://www.sanidad.gob.es/profesionales/saludPublica/prevPromocion/Prevencion/alcohol/docs/Low_Risk_Alcohol_Consumption_Thresholds_Part1.pdf (accessed on 20 January 2023).
- Kenfield, S.A.; Stampfer, M.J.; Rosner, B.A.; Colditz, G.A. Smoking and smoking cessation in relation to mortality in women. JAMA 2008, 299, 2037–2047. [Google Scholar] [CrossRef]
- WHOCC—ATC/DDD Index. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 22 December 2022).
- Torres-Bondia, F.; Dakterzada, F.; Galván, L.; Buti, M.; Besanson, G.; Gill, E.; Buil, R.; de Batlle, J.; Piñol-Ripoll, G. Proton pump inhibitors and the risk of Alzheimer’s disease and non-Alzheimer’s dementias. Sci. Rep. 2020, 10, 21046. [Google Scholar] [CrossRef]
- Chan, A.T.; Giovannucci, E.L.; Meyerhardt, J.A.; Schernhammer, E.S.; Wu, K.; Fuchs, C.S. Aspirin Dose and Duration of Use and Risk of Colorectal Cancer in Men. Gastroenterology 2008, 134, 21–28. [Google Scholar] [CrossRef]
- Hwang, I.C.; Chang, J.; Kim, K.; Park, S.M. Aspirin Use and Risk of Hepatocellular Carcinoma in a National Cohort Study of Korean Adults. Sci. Rep. 2018, 8, 4968. [Google Scholar] [CrossRef] [PubMed]
- Thun, M.J.; Jacobs, E.J.; Patrono, C. The role of aspirin in cancer prevention. Nat. Rev. Clin. Oncol. 2012, 9, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, P.M.; Wilson, M.; Elwin, C.E.; Norrving, B.; Algra, A.; Warlow, C.P.; Meade, T.W. Long-term effect of aspirin on colorectal cancer incidence and mortality: 20-year follow-up of five randomised trials. Lancet 2010, 376, 1741–1750. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, P.M.; Fowkes, F.G.R.; Belch, J.F.; Ogawa, H.; Warlow, C.P.; Meade, T.W. Effect of daily aspirin on long-term risk of death due to cancer: Analysis of individual patient data from randomised trials. Lancet 2011, 377, 31–41. [Google Scholar] [CrossRef]
- Maniewska, J.; Jeżewska, D. Non-Steroidal Anti-Inflammatory Drugs in Colorectal Cancer Chemoprevention. Cancers 2021, 13, 594. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.J.; He, Q.; Zhang, J.M.; Fan, H.J.; Wen, Z.F.; Qin, Y.R. High-dose aspirin consumption contributes to decreased risk for pancreatic cancer in a systematic review and meta-analysis. Pancreas 2014, 43, 135–140. [Google Scholar] [CrossRef]
- Jacobo-Herrera, N.J.; Pérez-Plasencia, C.; Camacho-Zavala, E.; Figueroa González, G.; López Urrutia, E.; Garćia-Castillo, V.; Zentella-Dehesa, A. Clinical evidence of the relationship between aspirin and breast cancer risk (review). Oncol. Rep. 2014, 32, 451–461. [Google Scholar] [CrossRef]
- Liao, L.M.; Vaughan, T.L.; Corley, D.A.; Cook, M.B.; Casson, A.G.; Kamangar, F.; Abnet, C.C.; Risch, H.A.; Giffen, C.; Freedman, N.D.; et al. Nonsteroidal Anti-inflammatory Drug Use Reduces Risk of Adenocarcinomas of the Esophagus and Esophagogastric Junction in a Pooled Analysis. Gastroenterology 2012, 142, 442–452.e5. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, G.; He, J.; Ren, S.; Wu, F.; Zhang, J.; Wang, F. Gender differences in colorectal cancer survival: A meta-analysis. Int. J. Cancer 2017, 141, 1942–1949. [Google Scholar] [CrossRef]
- Favoriti, P.; Carbone, G.; Greco, M.; Pirozzi, F.; Pirozzi, R.E.M.; Corcione, F. Worldwide burden of colorectal cancer: A review. Updat. Surg. 2016, 68, 7–11. [Google Scholar] [CrossRef]
- Permanyer, I.; Scholl, N. Global trends in lifespan inequality: 1950–2015. PLoS ONE 2019, 14, e0215742. [Google Scholar] [CrossRef]
- Nolen, S.C.; Evans, M.A.; Fischer, A.; Corrada, M.M.; Kawas, C.H.; Bota, D.A. Cancer—Incidence, prevalence and mortality in the oldest-old. A comprehensive review. Mech. Ageing Dev. 2017, 164, 113–126. [Google Scholar] [CrossRef]
- Shahjehan, F.; Merchea, A.; Cochuyt, J.J.; Li, Z.; Colibaseanu, D.T.; Kasi, P.M. Body mass index and long-term outcomes in patients with colorectal cancer. Front. Oncol. 2018, 8, 620. [Google Scholar] [CrossRef]
- Liu, P.H.; Wu, K.; Ng, K.; Zauber, A.G.; Nguyen, L.H.; Song, M.; He, X.; Fuchs, C.S.; Ogino, S.; Willett, W.C.; et al. Association of Obesity With Risk of Early-Onset Colorectal Cancer Among Women. JAMA Oncol. 2019, 5, 37–44. [Google Scholar] [CrossRef]
- Sanford, N.N.; Giovannucci, E.L.; Ahn, C.; Dee, E.C.; Mahal, B.A. Obesity and younger versus older onset colorectal cancer in the United States, 1998–2017. J. Gastrointest. Oncol. 2020, 11, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Jaspan, V.; Lin, K.; Popov, V. The impact of anthropometric parameters on colorectal cancer prognosis: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2021, 159, 103232. [Google Scholar] [CrossRef]
- Bradbury, K.E.; Murphy, N.; Key, T.J. Diet and colorectal cancer in UK Biobank: A prospective study. Int. J. Epidemiol. 2020, 49, 246–258. [Google Scholar] [CrossRef] [PubMed]
- Akter, S.; Islam, Z.; Mizoue, T.; Sawada, N.; Ihira, H.; Tsugane, S.; Koyanagi, Y.N.; Ito, H.; Wang, C.; Tamakoshi, A.; et al. Smoking and colorectal cancer: A pooled analysis of 10 population-based cohort studies in Japan. Int. J. Cancer 2021, 148, 654–664. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.S.; Huang, J.; Lok, V.; Wang, J.; Fung, F.; Ding, H.; Zheng, Z.J. Differences in Incidence and Mortality Trends of Colorectal Cancer Worldwide Based on Sex, Age, and Anatomic Location. Clin. Gastroenterol. Hepatol. 2021, 19, 955–966.e61. [Google Scholar] [CrossRef] [PubMed]
- Rasool, S.; Kadla, S.A.; Rasool, V.; Ganai, B.A. A comparative overview of general risk factors associated with the incidence of colorectal cancer. Tumor Biol. 2013, 34, 2469–2476. [Google Scholar] [CrossRef]
- Siegel, R.L.; Fedewa, S.A.; Anderson, W.F.; Miller, K.D.; Ma, J.; Rosenberg, P.S.; Jemal, A. Colorectal Cancer Incidence Patterns in the United States, 1974–2013. JNCI J. Natl. Cancer Inst. 2017, 109, djw322. [Google Scholar] [CrossRef]
- Rodríguez-Miguel, A.; García-Rodríguez, L.A.; Gil, M.; Montoya, H.; Rodríguez-Martín, S.; de Abajo, F.J. Clopidogrel and Low-Dose Aspirin, Alone or Together, Reduce Risk of Colorectal Cancer. Clin. Gastroenterol. Hepatol. 2019, 17, 2024–2033.e2. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, C.; Santucci, C.; Gallus, S.; Martinetti, M.; La Vecchia, C. Aspirin and the risk of colorectal and other digestive tract cancers: An updated meta-analysis through 2019. Ann. Oncol. 2020, 31, 558–568. [Google Scholar] [CrossRef]
- Steele, C.B.; Thomas, C.C.; Henley, S.J.; Massetti, G.M.; Galuska, D.A.; Agurs-Collins, T.; Puckett, M.; Richardson, L.C. Vital Signs: Trends in Incidence of Cancers Associated with Overweight and Obesity—United States, 2005–2014. Morb. Mortal. Wkly. Rep. 2017, 66, 1052. [Google Scholar] [CrossRef]
- Park, S.Y.; Wilkens, L.R.; Setiawan, V.W.; Monroe, K.R.; Haiman, C.A.; Le Marchand, L. Alcohol Intake and Colorectal Cancer Risk in the Multiethnic Cohort Study. Am. J. Epidemiol. 2019, 188, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Lee, D.H.; Han, K.D.; Kim, H.S.; Yoon, H.; Shin, C.M.; Park, Y.S.; Kim, N. The relationship between drinking alcohol and esophageal, gastric or colorectal cancer: A nationwide population-based cohort study of South Korea. PLoS ONE 2017, 12, e0185778. [Google Scholar] [CrossRef]
- Cook, N.R.; Lee, I.M.; Zhang, S.M.; Moorthy, M.V.; Buring, J.E. Alternate-day, low-dose aspirin and cancer risk: Long-term observational follow-up of a randomized trial. Ann. Intern. Med. 2013, 159, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Brasky, T.M.; Potter, J.D.; Kristal, A.R.; Patterson, R.E.; Peters, U.; Asgari, M.M.; Thornquist, M.D.; White, E. Non-steroidal anti-inflammatory drugs and cancer incidence by sex in the VITamins and Lifestyle (VITAL) cohort. Cancer Causes Control 2012, 23, 431–444. [Google Scholar] [CrossRef]
- Kim, H.; Giovannucci, E.L. Sex differences in the association of obesity and colorectal cancer risk. Cancer Causes Control 2016, 28, 1–4. [Google Scholar] [CrossRef]
- Bentham, J.; Di Cesare, M.; Bilano, V.; Bixby, H.; Zhou, B.; Stevens, G.A.; Riley, L.M.; Taddei, C.; Hajifathalian, K.; Lu, Y.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Movahedi, M.; Bishop, D.T.; Macrae, F.; Mecklin, J.P.; Moeslein, G.; Olschwang, S.; Eccles, D.; Evans, D.G.; Maher, E.R.; Bertario, L.; et al. Obesity, aspirin, and risk of colorectal cancer in carriers of hereditary colorectal cancer: A prospective investigation in the CAPP2 study. J. Clin. Oncol. 2015, 33, 3591–3597. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.N.; Pan, J.J.; Huang, Y.W.; Tsai, H.J.; Chang, W.C. Association between nonsteroidal anti-inflammatory drugs and colorectal cancer: A population-based case-control study. Cancer Epidemiol. Biomark. Prev. 2018, 27, 737–745. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.; Kumar, D.R.; Altinoz, M.A.; Bhat, G.J. Mechanisms of Colorectal Cancer Prevention by Aspirin—A Literature Review and Perspective on the Role of COX-Dependent and -Independent Pathways. Int. J. Mol. Sci. 2020, 21, 9018. [Google Scholar] [CrossRef] [PubMed]
- Gu, Q.; Dillon, C.F.; Eberhardt, M.S.; Wright, J.D.; Burt, V.L. Preventive aspirin and other antiplatelet medication use among U.S. adults aged ≥ 40 years: Data from the national health and nutrition examination survey, 2011–2012. Public Health Rep. 2015, 130, 643–654. [Google Scholar] [CrossRef]
- Duffy, D.; Kelly, E.; Trang, A.; Whellan, D.; Mills, G. Aspirin for Cardioprotection and Strategies to Improve Patient Adherence. Postgrad. Med. 2015, 126, 18–28. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Men | Women | ||||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| Gender | ||||||
| Female | 80,865 | 52.3 | - | - | - | - |
| Male | 73,850 | 47.7 | - | - | - | - |
| Age | ||||||
| [50–59) | 46,454 | 30.0 | 24,080 | 32.6 | 22,374 | 27.7 |
| [60–69) | 35,819 | 23.2 | 17,655 | 23.9 | 18,164 | 22.5 |
| [70–79) | 28,138 | 18.2 | 12,842 | 17.4 | 15,296 | 18.9 |
| [80–89) | 23,651 | 15.3 | 10,176 | 13.8 | 13,475 | 16.7 |
| [90–) | 20,653 | 13.3 | 9097 | 12.3 | 11,556 | 14.3 |
| Aspirin | ||||||
| Non-use | 138,157 | 88.1 | 66,695 | 90.3 | 71,462 | 88.4 |
| Use | 16,558 | 11.9 | 7155 | 9.7 | 9403 | 11.6 |
| Body Mass Index | ||||||
| Normal weight | 47,761 | 30.9 | 21,088 | 28.6 | 26,673 | 33.0 |
| Overweight | 51,022 | 33.0 | 27,005 | 36.6 | 24,017 | 29.7 |
| Obesity | 55,932 | 36.1 | 25,757 | 34.9 | 30,175 | 37.3 |
| Risky drinking | ||||||
| No | 151,323 | 97.8 | 71,997 | 97.5 | 79,326 | 98.1 |
| Yes | 3392 | 2.2 | 1853 | 2.5 | 1539 | 1.9 |
| Smoking | ||||||
| No | 140,749 | 90.9 | 62,995 | 85.3 | 77,754 | 96.2 |
| Yes | 13,966 | 9.1 | 10,855 | 14.7 | 3111 | 3.8 |
| Total | n | % (n/p-y) | Crude HR 1 | 95% CI | ||
|---|---|---|---|---|---|---|
| Person-Year (p-y) | % | |||||
| Gender | ||||||
| Female | 639,455 | 53.1 | 485 | 0.8 | 1.0 | Ref. group |
| Male | 563,716 | 46.9 | 791 | 1.4 | 1.9 | 1.6–2.1 |
| Age | ||||||
| (50–59) | 393,275 | 32.7 | 303 | 0.8 | 1.0 | Ref. group |
| (60–69) | 297,538 | 24.7 | 426 | 1.4 | 1.8 | 1.6–2.1 |
| (70–79) | 215,272 | 17.9 | 349 | 1.6 | 2.0 | 1.9–2.6 |
| (80–89) | 147,817 | 12.3 | 184 | 1.2 | 1.6 | 1.3–1.9 |
| (90–) | 149,269 | 12.4 | 14 | 0.1 | 0.1 | 0.1–0.2 |
| Aspirin | ||||||
| Non-use | 1,068,470 | 88.8 | 1138 | 1.2 | 1.0 | Ref. group |
| Use | 134,701 | 11.2 | 138 | 1.0 | 0.9 | 0.8–1.1 |
| Body mass index | ||||||
| Normal weight | 350.994 | 29.2 | 169 | 0.5 | 1.0 | Ref. Group |
| Overweight | 404.905 | 33.7 | 504 | 1.2 | 2.5 | 2.2–3.1 |
| Obesity | 447,272 | 37.2 | 603 | 1.3 | 2.7 | 2.3–3.3 |
| Risky drinking | ||||||
| No | 1,177,736 | 97.9 | 1220 | 1.0 | 1.0 | Ref. Group |
| Yes | 25,435 | 2.1 | 56 | 2.2 | 2.1 | 1.6–2.7 |
| Smoking | ||||||
| No | 1,094,891 | 91.0 | 1056 | 1.0 | 1.0 | Ref. Group |
| Yes | 108,280 | 9.0 | 220 | 2.0 | 2.0 | 1.8–2.4 |
| Adjusted Hazard Ratio (aHR); 95% CI 1 | p-Value | |
|---|---|---|
| Female | - | Ref. Group |
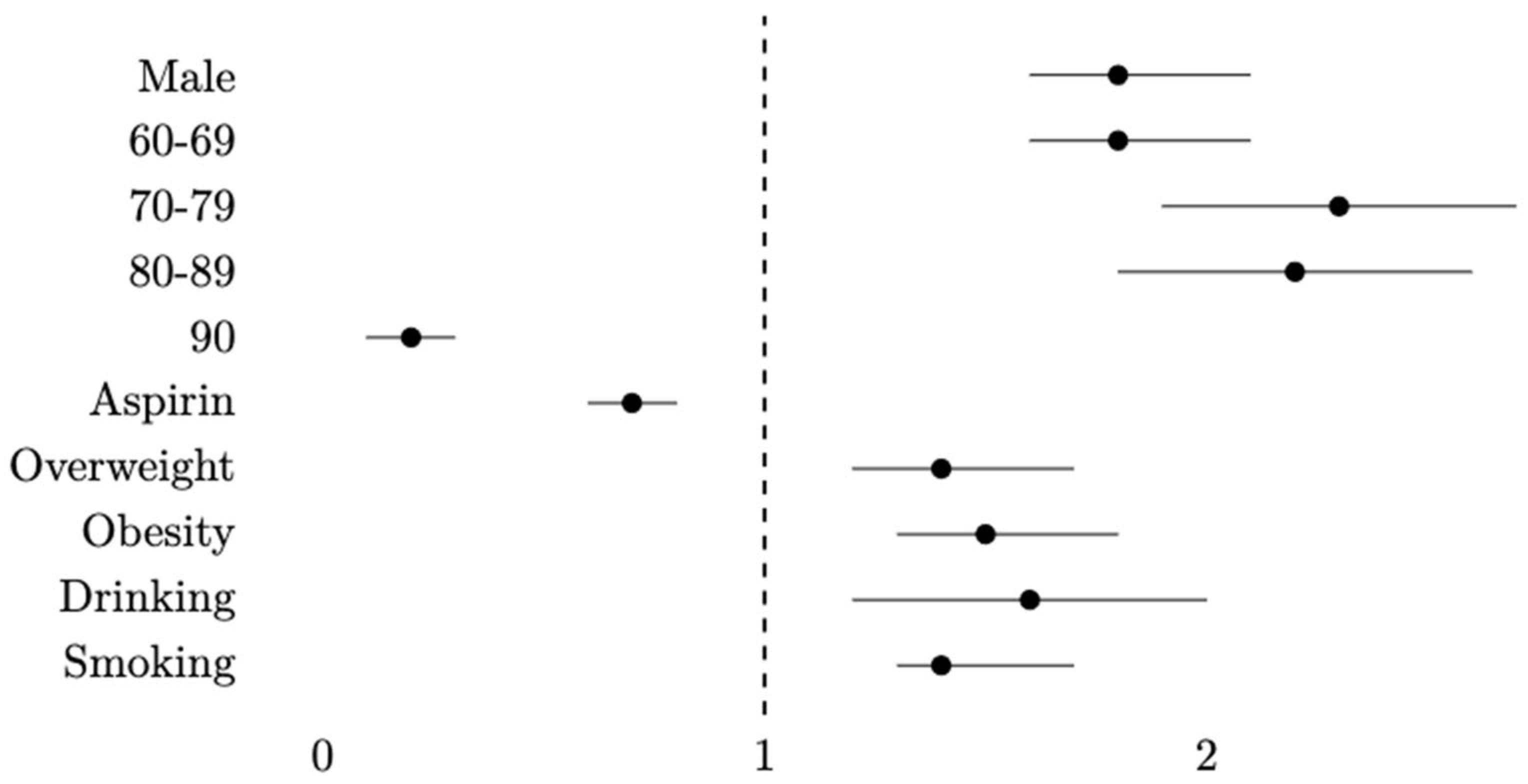
| Male | 1.8 (1.6–2.1) | <0.001 |
| (50–59) | - | Ref. Group |
| (60–69) | 1.8 (1.6–2.1) | <0.001 |
| (70–79) | 2.3 (1.9–2.7) | <0.001 |
| (80–89) | 2.2 (1.8–2.6) | 0.007 |
| (90-) | 0.2 (0.1–0.3) | <0.001 |
| Aspirin use | 0.7 (0.6–0.8) | 0.006 |
| Normal weight | - | Ref. Group |
| Overweight | 1.4 (1.2–1.7) | <0.001 |
| Obesity | 1.5 (1.3–1.8) | <0.001 |
| Risky drinking | 1.6 (1.2–2.0) | 0.006 |
| Smoking | 1.4 (1.3–1.7) | <0.001 |
| Men | Women | |||
|---|---|---|---|---|
| Adjusted Hazard Ratio (aHR); 95% CI 1 | p-Value | Adjusted Hazard Ratio (aHR); 95% CI 1 | p-Value | |
| (50–59) | - | Ref. Group | - | Ref. Group 2 |
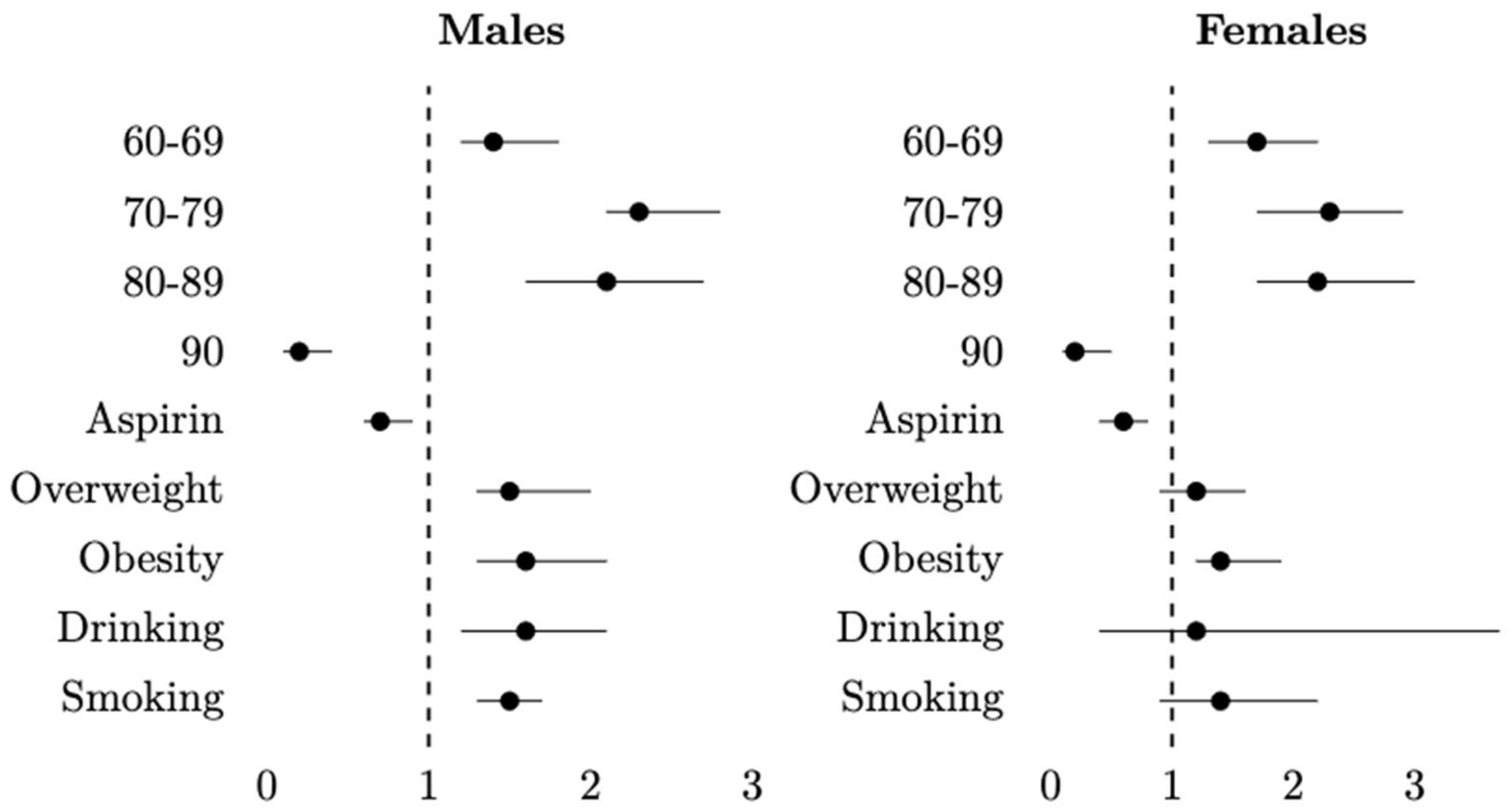
| (60–69) | 1.9 (1.7–2.3) | <0.001 | 1.7 (1.3–2.2) | <0.001 |
| (70–79) | 2.3 (1.9–2.8) | <0.001 | 2.3 (1.7–2.9) | <0.001 |
| (80–89) | 2.1 (1.6–2.7) | <0.001 | 2.2 (1.7–3.0) | <0.001 |
| (90–) | 0.2 (0.1–0.4) | <0.001 | 0.2 (0.1–0.5) | <0.001 |
| Aspirin use | 0.7 (0.6–0.9) | 0.005 | 0.6 (0.4–0.8) | 0.005 |
| Normal weight | - | Ref. Group 2 | - | Ref. Group 2 |
| Overweight | 1.5 (1.2–2.0) | <0.001 | 1.2 (0.9–1.6) | 0.1 |
| Obesity | 1.6 (1.3–2.1) | <0.001 | 1.4 (1.2–1.9) | 0.004 |
| Risky drinking | 1.6 (1.2–2.1) | 0.001 | 1.2 (0.4–3.7) | 0.7 |
| Smoking | 1.5 (1.3–1.7) | <0.001 | 1.4 (0.9–2.2) | 0.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Florensa, D.; Mateo, J.; Solsona, F.; Galván, L.; Mesas, M.; Piñol, R.; Espinosa-Leal, L.; Godoy, P. Acetylsalicylic Acid Effect in Colorectal Cancer Taking into Account the Role of Tobacco, Alcohol and Excess Weight. Int. J. Environ. Res. Public Health 2023, 20, 4104. https://doi.org/10.3390/ijerph20054104
Florensa D, Mateo J, Solsona F, Galván L, Mesas M, Piñol R, Espinosa-Leal L, Godoy P. Acetylsalicylic Acid Effect in Colorectal Cancer Taking into Account the Role of Tobacco, Alcohol and Excess Weight. International Journal of Environmental Research and Public Health. 2023; 20(5):4104. https://doi.org/10.3390/ijerph20054104
Chicago/Turabian StyleFlorensa, Didac, Jordi Mateo, Francesc Solsona, Leonardo Galván, Miquel Mesas, Ramon Piñol, Leonardo Espinosa-Leal, and Pere Godoy. 2023. "Acetylsalicylic Acid Effect in Colorectal Cancer Taking into Account the Role of Tobacco, Alcohol and Excess Weight" International Journal of Environmental Research and Public Health 20, no. 5: 4104. https://doi.org/10.3390/ijerph20054104
APA StyleFlorensa, D., Mateo, J., Solsona, F., Galván, L., Mesas, M., Piñol, R., Espinosa-Leal, L., & Godoy, P. (2023). Acetylsalicylic Acid Effect in Colorectal Cancer Taking into Account the Role of Tobacco, Alcohol and Excess Weight. International Journal of Environmental Research and Public Health, 20(5), 4104. https://doi.org/10.3390/ijerph20054104