
Exhaled Carbon Monoxide Level and Practices among Tobacco and Nicotine Adult Users in Klang Valley, Malaysia


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Socio-Demographic and Smoking Status
3.2. Comparison of Practices and Nicotine Dependency Profile
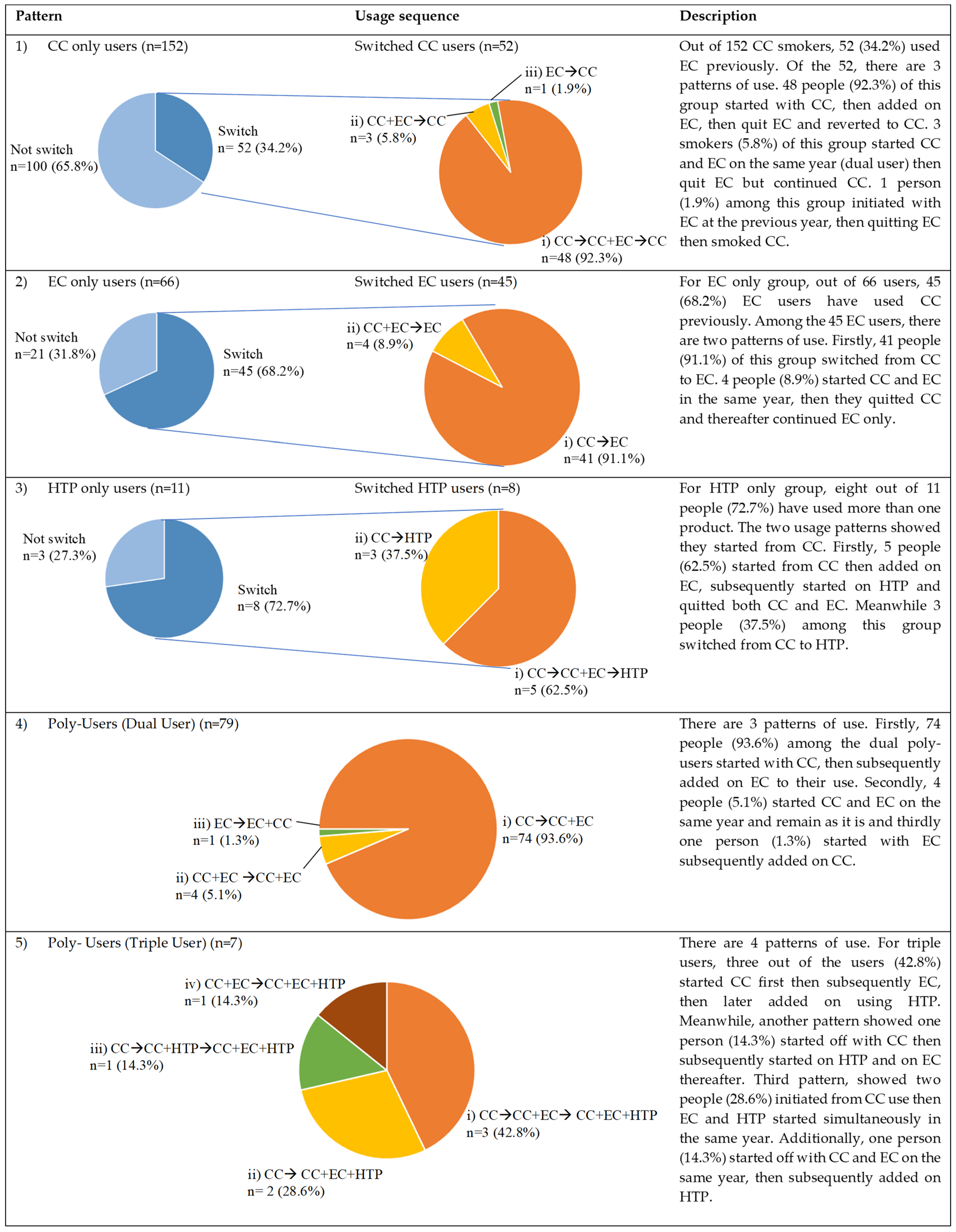
3.3. Switching Patterns
3.3.1. Single Product User
3.3.2. Poly-User Group
3.4. Comparison of Exhaled Carbon Monoxide Level between Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tobacco. Available online: https://www.who.int/news-room/fact-sheets/detail/tobacco (accessed on 23 August 2022).
- Cigarette. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/cigarette (accessed on 20 August 2022).
- IQOS Heated Tobacco Products. Available online: https://www.pmi.com/smoke-free-products/iqos-our-tobacco-heating-system (accessed on 20 August 2022).
- Grana, R.; Benowitz, N.; Glantz, S.A. E-cigarettes: A scientific review. Circulation 2014, 129, 1972–1986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNeill, A.; Calder, R.; Bauld, L.; Robson, D. Vaping in England: An evidence update February 2019. In A Report Commissioned by Public Health England; Public Health England: London, UK, 2019. [Google Scholar]
- E-Cigarettes: An Emerging Category; Ernst & Young: London, UK, 2016.
- World Health Organization. WHO Global Report on Trends in Prevalence of Tobacco Use 2000–2025; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Institute for Public Health. National Health and Morbidity Survey (NHMS) 2019: Vol. I: NCDs—Non-Communicable Diseases: Risk Factors and other Health Problems; National Institutes of Health, Ministry of Health Malaysia: Putrajaya, Malaysia, 2020.
- U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; U.S. Department of Health and Human: Atlanta, GA, USA, 2014.
- Electronic Non-Nicotine Delivery Systems (ENDS/ENNDS). Available online: https://www.who.int/publications/m/item/electronic-nicotine-delivery-systems-and-electronic-non-nicotine-delivery-systems-(ends-ennds) (accessed on 21 August 2022).
- Yun, W.J.; Rhee, J.A.; Kim, S.A.; Kweon, S.S.; Lee, Y.H.; Ryu, S.Y.; Park, S.W.; Kim, D.H.; Shin, M.H. Household and area income levels are associated with smoking status in the Korean adult population. BMC Public Health 2015, 15, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widome, R.; Joseph, A.M.; Hammett, P.; Van Ryn, M.; Nelson, D.B.; Nyman, J.A.; Fu, S.S. Associations between smoking behaviors and financial stress among low-income smokers. Prev. Med. Rep. 2015, 2, 911–915. [Google Scholar] [CrossRef] [Green Version]
- Samsudin, H.; Nadzrulizam, A. Relationship between B40 Household Income and Demographic Factors in Malaysia. Int. J. Innov. Technol. Explor. Eng. 2020, 10, 113–117. [Google Scholar] [CrossRef]
- Fallahia, M.; Mohamed Nor, N.; Bui, W. The Impact of Human Development on Cigarettes Consumption in Malaysia. Int. J. Econ. Manag. 2015, 9, 356–368. [Google Scholar]
- Wadgave, U.; Nagesh, L. Nicotine Replacement Therapy: An Overview. Int. J. Health Sci. 2016, 10, 425–435. [Google Scholar] [CrossRef]
- Ellerbeck, E.F.; Nollen, N.; Hutcheson, T.D.; Phadnis, M.; Fitzgerald, S.A.; Vacek, J.; Sharpe, M.R.; Salzman, G.A.; Richter, K.P. Effect of Long-term Nicotine Replacement Therapy vs Standard Smoking Cessation for Smokers With Chronic Lung Disease: A Randomized Clinical Trial. JAMA Netw. Open 2018, 1, e181843. [Google Scholar] [CrossRef] [Green Version]
- OpenEpi: Open Source Epidemiologic Statistics for Public Health. Available online: www.OpenEpi.com (accessed on 10 July 2021).
- Igarashi, A.; Aida, J.; Kusama, T.; Tabuchi, T.; Tsuboya, T.; Sugiyama, K.; Yamamoto, T.; Osaka, K. Heated Tobacco Products Have Reached Younger or More Affluent People in Japan. J. Epidemiol. 2021, 31, 187–193. [Google Scholar] [CrossRef] [Green Version]
- Carrilero, N.; Dalmau-Bueno, A.; García-Altés, A. Comorbidity Patterns and Socioeconomic Inequalities in Children under 15 with Medical Complexity: A Population-Based Study. BMC Pediatr. 2020, 20, 358. [Google Scholar] [CrossRef]
- Chetty, R.; Stepner, M.; Abraham, S.; Lin, S.; Scuderi, B.; Turner, N.; Bergeron, A.; Cutler, D. The Association between Income and Life Expectancy in the United States, 2001-2014. JAMA 2016, 315, 1750–1766. [Google Scholar] [CrossRef]
- Lenhart, O. The Effects of Income on Health: New Evidence from the Earned Income Tax Credit. Rev. Econ. Househ. 2019, 17, 377–410. [Google Scholar] [CrossRef] [Green Version]
- Kosendiak, A.; Król, M.; Ściskalska, M.; Kepinska, M. The Changes in Stress Coping, Alcohol Use, Cigarette Smoking and Physical Activity during COVID-19 Related Lockdown in Medical Students in Poland. Int. J. Environ. Res. Public Health 2021, 19, 302. [Google Scholar] [CrossRef]
- Koopmann, A.; Georgiadou, E.; Reinhard, I.; Müller, A.; Lemenager, T.; Kiefer, F.; Hillemacher, T. The Effects of the Lockdown during the COVID-19 Pandemic on Alcohol and Tobacco Consumption Behavior in Germany. Eur. Addict. Res. 2021, 27, 242–256. [Google Scholar] [CrossRef]
- Zhu, J.; Shi, F.; Xu, G.; Li, N.; Li, J.; He, Y.; Yu, J. Conventional Cigarette and E-Cigarette Smoking among School Personnel in Shanghai, China: Prevalence and Determinants. Int. J. Environ. Res. Public Health 2019, 16, 3197. [Google Scholar] [CrossRef] [Green Version]
- Johnson, A.L.; Collins, L.K.; Villanti, A.C.; Pearson, J.L.; Niaura, R.S. Patterns of Nicotine and Tobacco Product Use in Youth and Young Adults in the United States, 2011–2015. Nicotine Tob. Res. 2018, 20 (Suppl. S1), S48–S54. [Google Scholar] [CrossRef]
- Cho, M.S. Factors Associated with Cigarette, E-Cigarette, and Dual Use among South Korean Adolescents. Healthcare 2021, 9, 1252. [Google Scholar] [CrossRef]
- Mattingly, D.T.; Hart, J.L.; Wood, L.A.; Walker, K.L. Sociodemographic differences in single, dual, and poly tobacco use among Appalachian youth. Tob. Prev. Cessat. 2020, 6, 45. [Google Scholar] [CrossRef]
- Sung, H.Y.; Wang, Y.; Yao, T.; Lightwood, J.; Max, W. Polytobacco Use of Cigarettes, Cigars, Chewing Tobacco, and Snuff Among US Adults. Nicotine Tob. Res. 2016, 18, 817–826. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.Y.; Paek, Y.J.; Seo, H.G.; Cheong, Y.S.; Lee, C.M.; Park, S.M.; Park, D.W.; Lee, K. Dual use of electronic and conventional cigarettes is associated with higher cardiovascular risk factors in Korean men. Sci. Rep. 2020, 10, 5612. [Google Scholar] [CrossRef] [Green Version]
- Kim, M. Philip Morris International introduces new heat-not-burn product, IQOS, in South Korea. Tob. Control 2018, 27, e76. [Google Scholar] [CrossRef]
- Jankowski, M.; Krzystanek, M.; Zejda, J.E.; Majek, P.; Lubanski, J.; Lawson, J.A.; Brozek, G. E-Cigarettes are More Addictive than Traditional Cigarettes-A Study in Highly Educated Young People. Int. J. Environ. Res. Public Health 2019, 16, 2279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huh, Y.; Lee, C.M.; Cho, H.-J. Comparison of nicotine dependence between single and multiple tobacco product users among South Korean adults. Tob. Induc. Dis. 2022, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, S.; Kimm, H.; Lee, J.-A.; Lee, C.-M.; Cho, H.-J. Heated tobacco product use and its relationship to quitting combustible cigarettes in Korean adults. PLoS ONE 2021, 16, e0251243. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.M.; Kim, C.Y.; Lee, K.; Kim, S. Are Heated Tobacco Product Users Less Likely to Quit than Cigarette Smokers? Findings from THINK (Tobacco and Health IN Korea) Study. Int. J. Environ. Res. Public Health 2020, 17, 8622. [Google Scholar] [CrossRef] [PubMed]
- Berry, K.M.; Reynolds, L.M.; Collins, J.M.; Siegel, M.B.; Fetterman, J.L.; Hamburg, N.M.; Bhatnagar, A.; Benjamin, E.J.; Stokes, A. E-cigarette initiation and associated changes in smoking cessation and reduction: The Population Assessment of Tobacco and Health Study, 2013-2015. Tob. Control 2019, 28, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Evans, A.T.; Henderson, K.C.; Geier, A.; Weaver, S.R.; Spears, C.A.; Ashley, D.L.; Fritz, M.; John, L.; Pechacek, T.F. What Motivates Smokers to Switch to ENDS? A Qualitative Study of Perceptions and Use. Int. J. Environ. Res. Public Health 2020, 17, 8865. [Google Scholar] [CrossRef]
- Barufaldi, L.A.; Guerra, R.L.; Rita de Cássia, R.; Nascimento, A.; Chança, R.D.; de Souza, M.C.; de Almeida, L.M. Risk of smoking relapse with the use of electronic cigarettes: A systematic review with meta-analysis of longitudinal studies. Tob. Prev. Cessat. 2021, 29, 29. [Google Scholar] [CrossRef]
- Martínez, Ú.; Martínez-Loredo, V.; Simmons, V.N.; Meltzer, L.R.; Drobes, D.J.; Brandon, K.O.; Palmer, A.M.; Eissenberg, T.; Bullen, C.R.; Harrell, P.T.; et al. How Does Smoking and Nicotine Dependence Change After Onset of Vaping? A Retrospective Analysis of Dual Users. Nicotine Tob. Res. 2020, 22, 764–770. [Google Scholar] [CrossRef]
- Brose, L.S.; Bowen, J.; McNeill, A.; Partos, T.R. Associations between vaping and relapse to smoking: Preliminary findings from a longitudinal survey in the UK. Harm. Reduct. J. 2019, 16, 76. [Google Scholar] [CrossRef] [Green Version]
- Price, A.D.; Coffey, M.; Houston, L.; Cook, P.A. Evaluation of a pharmacy supported e-cigarette smoking cessation intervention in Northwest England. BMC Public Health 2022, 22, 1326. [Google Scholar] [CrossRef]
- Hung, J.; Lin, C.H.; Wang, J.D.; Chan, C.C. Exhaled carbon monoxide level as an indicator of cigarette consumption in a workplace cessation program in Taiwan. J. Formos. Med. Assoc. 2006, 105, 210–213. [Google Scholar] [CrossRef] [Green Version]
- Maclaren, D.J.; Conigrave, K.M.; Robertson, J.A.; Ivers, R.G.; Eades, S.; Clough, A.R. Using breath carbon monoxide to validate self-reported tobacco smoking in remote Australian Indigenous communities. Popul. Health Metr. 2010, 8, 2. [Google Scholar] [CrossRef] [Green Version]
- Nikkholgh, A.; Soleimani, M.; Torkaman-Boutorabi, A.; Valizadeh, B. Evaluation of smoking status: Comparison of self-reports with exhaled carbon monoxide analysis in university students in the Islamic Republic of Iran. East Mediterr. Health J. 2021, 27, 321–326. [Google Scholar] [CrossRef]
- Sugavanesh, P.; Pushpanjali, K. Nicotine Dependence, Its Risk Indicators, and Exhaled Carbon Monoxide Levels among the Smokers in Bengaluru, India. Indian J. Community Med. 2018, 43, 220–223. [Google Scholar]
- Herath, P.; Wimalasekera, S.W.; Amarasekara, T.D.; Fernando, M.S.; Turale, S. Adverse effects of cigarette smoking on exhaled breath carbon monoxide, blood carboxyhemoglobin, and hematological parameters amongst Sri Lankan adult tobacco smokers: A descriptive study. Popul. Med. 2021, 3, 1–10. [Google Scholar] [CrossRef]
- Brinkman, G.L.; Coates, E.O., Jr. The effect of bronchitis, smoking, and occupation on ventilation. Am. Rev. Respir. Dis. 1963, 87, 684–693. [Google Scholar]
- Park, M.-B.; Choi, J.-K. Differences between the effects of conventional cigarettes, e-cigarettes and dual product use on urine cotinine levels. Tob. Induc. Dis. 2019, 17, 12. [Google Scholar] [CrossRef]
- Cancelada, L.; Sleiman, M.; Tang, X.; Russell, M.L.; Montesinos, V.N.; Litter, M.I.; Gundel, L.A.; Destaillats, H. Heated Tobacco Products: Volatile Emissions and Their Predicted Impact on Indoor Air Quality. Environ. Sci. Technol. 2019, 53, 7866–7876. [Google Scholar] [CrossRef]
- Zhang, Q.; Li, L.; Smith, M.; Guo, Y.; Whitlock, G.; Bian, Z.; Kurmi, O.; Collins, R.; Chen, J.; Lv, S.; et al. Exhaled carbon monoxide and its associations with smoking, indoor household air pollution and chronic respiratory diseases among 512,000 Chinese adults. Int. J. Epidemiol. 2013, 42, 1464–1475. [Google Scholar] [CrossRef] [Green Version]
- Nga, J.D.L.; Hakim, S.L.; Bilal, S. Comparison of End Tidal Carbon Monoxide Levels between Conventional Cigarette, Electronic Cigarette and Heated Tobacco Product among Asiatic Smokers. Subst. Use Misuse 2020, 55, 1943–1948. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables (n = 657) | Overall n (%) | Non-Smokers | CCs | PUs | ECs | HTPs | p-Value |
|---|---|---|---|---|---|---|---|
| (n = 342) n (%) | (n = 152) n (%) | (n = 86) n (%) | (n = 66) n (%) | (n = 11) n (%) | |||
| Age (years) | <0.001 *a <0.001 *b | ||||||
| Mean (±SD) | 34.4 (±0.37) | 34.85 (±9.78) | 36.20 (±9.47) | 31.89 (±8.09) | 30.32 (±7.36) | 39.18 (±7.39) | |
| 18–30 | 250 (38.1) | 120 (48.0) | 48 (19.2) | 42 (16.8) | 39 (15.6) | 1 (0.4) | |
| 31–60 | 407 (61.9) | 222 (54.5) | 104 (25.6) | 44 (10.8) | 27 (6.6) | 10 (2.5) | |
| Gender | <0.001 *b | ||||||
| Male | 462 (70.3) | 173 (37.4) | 146 (31.4) | 82 (17.6) | 52 (11.2) | 9 (1.9) | |
| Female | 195 (29.7) | 169 (86.7) | 6 (3.1) | 4 (2.1) | 14 (7.3) | 2 (1.0) | |
| Ethnicity | <0.001 *b | ||||||
| Malay | 577 (87.8) | 298 (51.6) | 138 (23.9) | 79 (13.7) | 59 (10.2) | 3 (0.5) | |
| Others | 80 (12.2) | 44 (55.0) | 14 (17.5) | 7 (8.8) | 7 (8.8) | 8 (10.0) | |
| Marital status | 0.047 *b | ||||||
| Married | 407 (61.9) | 210 (51.6) | 108 (26.5) | 45 (11.1) | 38 (9.3) | 6 (1.5) | |
| Non-married | 250 (38.1) | 132 (52.8) | 44 (17.6) | 41 (16.4) | 28 (11.2) | 5 (2.0) | |
| Education level | <0.001 *b | ||||||
| Tertiary | 285 (43.4) | 189 (66.3) | 24 (8.4) | 34 (11.9) | 30 (10.5) | 8 (2.8) | |
| Non-tertiary | 372 (56.6) | 153 (41.1) | 128 (34.4) | 52 (14.0) | 36 (9.7) | 3 (0.8) | |
| Occupation | <0.001 *b | ||||||
| Government staff | 326 (49.6) | 204 (62.6) | 62 (19.0) | 34 (10.4) | 26 (8.0) | 0 (0.0) | |
| Private sector | 235 (35.8) | 67 (28.5) | 77 (32.8) | 45 (19.1) | 35 (14.9) | 11 (4.7) | |
| Unemployed/Student | 96 (14.6) | 71 (74.0) | 13 (13.5) | 7 (7.3) | 5 (5.2) | 0 (0.0) | |
| Income group | <0.001 *b | ||||||
| B40 | 482 (73.4) | 213 (44.2) | 138 (28.6) | 73 (15.1) | 56 (11.6) | 2 (0.4) | |
| Non B40 | 175 (26.6) | 129 (73.7) | 14 (8.0) | 13 (7.4) | 10 (5.7) | 9 (5.1) | |
| Co-morbidity | <0.001 *b | ||||||
| Absent | 507 (77.2) | 251 (49.5) | 113 (22.3) | 72 (14.2) | 61 (12.0) | 10 (2.0) | |
| Present | 150 (22.8) | 91 (60.7) | 39 (26.0) | 14 (9.3) | 5 (3.3) | 1 (0.7) | |
| Weight (kg) | 0.347 *a | ||||||
| Mean (±SD) | 73.52 (±16.36) | 72.35 (±16.03) | 74.67 (±18.23) | 75.21 (±17.65) | 75.38 (±18.23) | 70.00 (±11.66) | |
| Height (m) | <0.001 *a | ||||||
| Mean (±SD) | 1.68 (±0.0784) | 1.63 (±0.084) | 1.68 (±0.070) | 1.69 (±0.067) | 1.69 (±0.087) | 1.70 (±0.088) | |
| BMI (kg/m2) | 0.144 a | ||||||
| Mean (±SD) | 26.00(±5.22) | 27.18 (±5.63) | 26.27 (±5.67) | 26.15 (±5.57) | 26.18 (±5.43) | 24.22 (±3.80) |
| Variables | CCs (n = 152) | ECs (n = 66) | HTPs (n = 11) | Poly-Users (n = 86) | p-Value | ||
|---|---|---|---|---|---|---|---|
| CCs (n = 86) | ECs (n = 86) | HTPs (n = 7) | |||||
| Age start (years) | <0.001 *a <0.001 *b | ||||||
| Mean (±SD) | 17.41 (±3.84) | 26.65 (±8.09) | 35.00 (±7.47) | 17.16 (±3.66) | 27.20 (±8.29) | 27.00 (±9.79) | |
| Range | (10–31) | (13–47) | (22–46) | (10–29) | (15–52) | (18–48) | |
| ≤18 | 110 (72.4) | 11 (16.7) | 0 (0.0) | 56 (65.1) | 8 (9.3) | 1 (14.3) | |
| >18 | 42 (27.6) | 55 (83.3) | 11 (100.0) | 30 (34.9) | 78 (90.7) | 6 (85.7) | |
| Duration smoking (years) | <0.001 *a <0.001 *b | ||||||
| Mean (±SD) | 17.58 (±9.74) | 4.20 (±3.61) | 4.32 (±1.76) | 13.93 (±7.76) | 4.20 (±3.13) | 3.43 (±1.51) | |
| Range | (2–45) | (1–22) | (1–8) | (1–36) | (1–19) | (2–6) | |
| 0–5 | 17 (11.2) | 51 (77.3) | 9 (81.8) | 13 (15.1) | 66 (76.7) | 6 (85.7) | |
| ≥5 | 135 (88.8) | 15 (22.7) | 2 (18.2) | 73 (84.9) | 20 (23.3) | 1 (14.3) | |
| Cost/month (MYR) | <0.001 *a <0.001 *b | ||||||
| Mean (±SD) | 197.61 (±139.98) | 81.86 (±96.30) | 330.64 (±195.56) | 187.66 (±128.53) | 82.49 (±97.86) | 152.14 (±122.13) | |
| Range | (10–700) | (7.5–700) | (28–630) | (15–600) | (15–600) | (15–300) | |
| ≤100 | 50 (32.9) | 54 (81.8) | 2 (18.2) | 32 (37.2) | 70 (81.4) | 3 (42.9) | |
| >100 | 102 (67.1) | 12 (18.2) | 9 (81.8) | 54 (62.8) | 16 (18.6) | 4 (57.1) | |
| Fagerström score | 0.109 a 0.195 b | ||||||
| Mean (±SD) | 3.66 (±2.19) | 4.12 (±2.39) | 2.55 (±2.21) | 3.38 (±2.27) | 3.81 (±2.20) | 4.00 (±1.41) | |
| Range | (0–9) | (0–10) | (0–6) | (0–9) | (0–9) | (1–5) | |
| <4 | 73 (48.0) | 29 (43.9) | 7 (63.6) | 41 (47.7) | 45 (52.3) | 1 (14.3) | |
| 4–6 | 62 (40.8) | 25 (37.9) | 4 (36.4) | 38 (44.2) | 29 (33.7) | 6 (85.7) | |
| 7–10 | 17 (11.2) | 12 (18.2) | 0 (0) | 7 (8.1) | 12 (14.0) | 0 (0) | |
| Attempt to quit | <0.001 *b | ||||||
| Yes | 85 (55.9) | 23 (34.8) | 1 (9.1) | 74 (86.0) | 41 (47.7) | 2 (28.6) | |
| No | 67 (44.1) | 43 (65.2) | 10 (90.9) | 12 (14.0) | 45 (52.3) | 5 (71.4) | |
| Smoking Status | Mean Duration Use (Years) | Minimum–Maximum (ppm) | Median (IQR) (ppm) | p-Value |
|---|---|---|---|---|
| <0.001 a | ||||
| CCs only (n = 152) | 17.58 (±9.74) | 2–50 | 13.00 (9.00–19.75) | |
| PUs (n = 86) | 13.93(±7.76) b, 4.20 (±3.13) c, and 3.43(±1.51) d | 1–39 | 7.00 (3.00–12.25) | |
| ECs only (n = 66) | 4.20 (±3.61) | 1–12 | 2.00 (1.00–3.00) | |
| HTPs only (n = 11) | 4.32 (±1.76) | 1–3 | 2.00 (1.00–3.00) | |
| Non-smokers (n = 342) | Not applicable | 0–7 | 1.00 (1.00–2.00) |
| Smoking Status | Mean Duration Use (Years) | eCO Level (ppm) | p-Value | ||
|---|---|---|---|---|---|
| 0–6 n (%) (n = 481) | 7–10 n (%) (n = 50) | >10 n (%) (n = 126) | |||
| <0.001 a | |||||
| Non-smokers (n = 342) | Not applicable | 337 (98.5) | 5 (1.5) | 0 (0) | |
| CCs only (n = 152) | 17.58 (±9.74) | 28 (18.4) | 23 (15.1) | 101 (66.4) | |
| PUs (n = 86) | 13.93(±7.76) b, 4.20 (±3.13) c, and 3.43 (±1.51) d | 42 (48.8) | 20 (23.3) | 24 (27.9) | |
| ECs only (n = 66) | 4.20 (±3.61) | 63 (95.5) | 2 (3.0) | 1 (1.5) | |
| HTPs only (n = 11) | 4.32 (±1.76) | 11 (100.0) | 0 (0) | 0 (0) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wan Puteh, S.E.; Mohd Ismail, N.; Md Isa, Z.; Ban, A.Y.-L. Exhaled Carbon Monoxide Level and Practices among Tobacco and Nicotine Adult Users in Klang Valley, Malaysia. Int. J. Environ. Res. Public Health 2023, 20, 4443. https://doi.org/10.3390/ijerph20054443
Wan Puteh SE, Mohd Ismail N, Md Isa Z, Ban AY-L. Exhaled Carbon Monoxide Level and Practices among Tobacco and Nicotine Adult Users in Klang Valley, Malaysia. International Journal of Environmental Research and Public Health. 2023; 20(5):4443. https://doi.org/10.3390/ijerph20054443
Chicago/Turabian StyleWan Puteh, Sharifa Ezat, Norayuni Mohd Ismail, Zaleha Md Isa, and Andrea Yu-Lin Ban. 2023. "Exhaled Carbon Monoxide Level and Practices among Tobacco and Nicotine Adult Users in Klang Valley, Malaysia" International Journal of Environmental Research and Public Health 20, no. 5: 4443. https://doi.org/10.3390/ijerph20054443
APA StyleWan Puteh, S. E., Mohd Ismail, N., Md Isa, Z., & Ban, A. Y.-L. (2023). Exhaled Carbon Monoxide Level and Practices among Tobacco and Nicotine Adult Users in Klang Valley, Malaysia. International Journal of Environmental Research and Public Health, 20(5), 4443. https://doi.org/10.3390/ijerph20054443