
Saturday Night Fever: Interpersonal Violence as a Reason for Presentation in a University Emergency Department

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Statistical Analysis
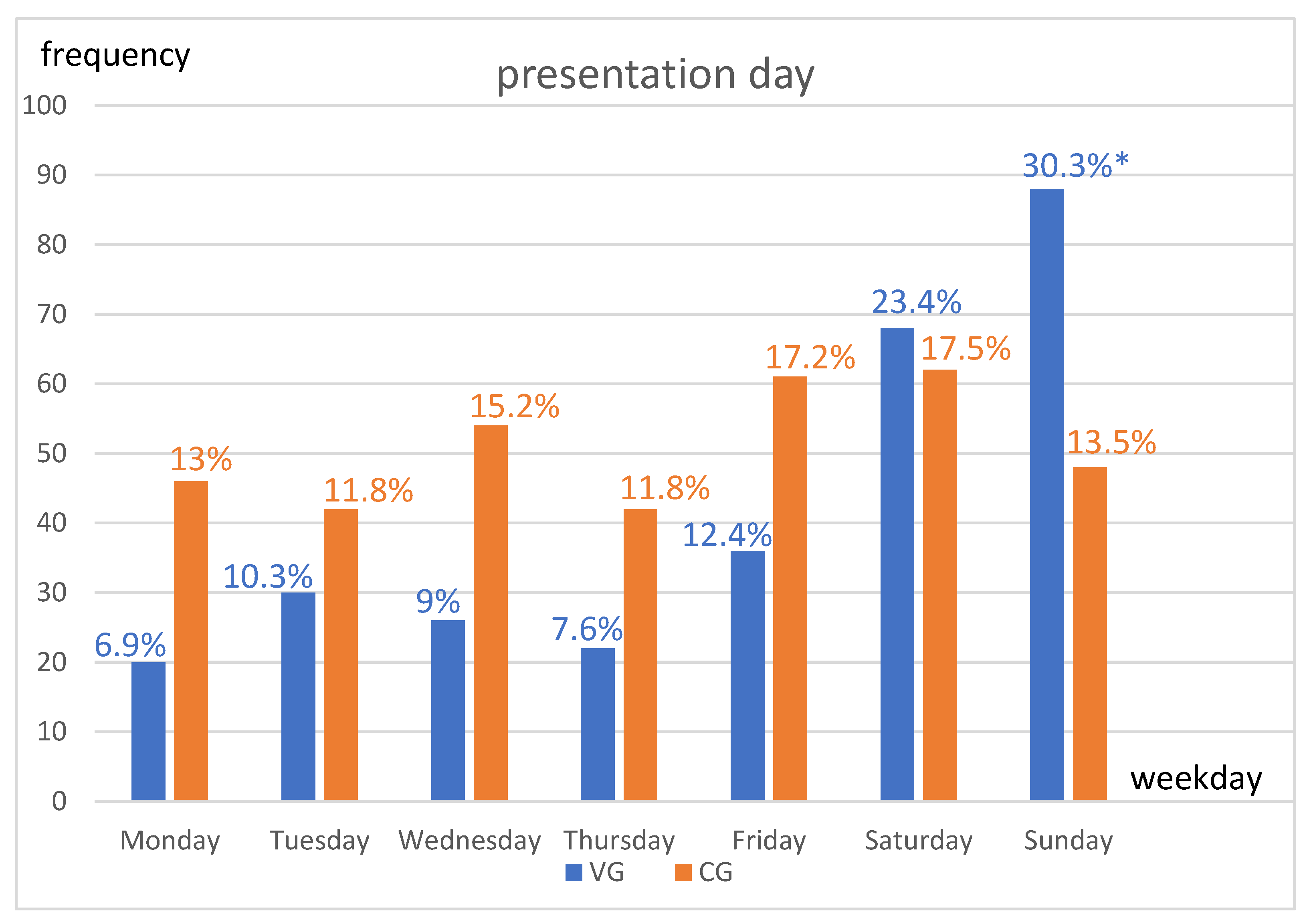
2.2. Graphical Presentation of the Results
3. Results
3.1. Reason for Presentation
3.2. Demographics
3.3. Presentation Time
3.4. Pre-Clinical and Clinical Assessment
3.5. Injury Pattern and Discharge Diagnosis
3.6. Correlation
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Biberthaler, P.; Förschner, L.; Gehring, C.; Trentzsch, H.; Kanz, K.-G.; Prückner, S. Stellenwert der Unfallchirurgie für die Notaufnahmen einer deutschen Millionenstadt—Eine Auswertung von 524.716 Notfallpatienten. Unfallchirurg 2019, 122, 44–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. World Report on Violence and Health: Summary; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Boyle, A. Domestic violence in emergency medicine patients. Emerg. Med. J. 2004, 21, 9–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oram, S.; Khalifeh, H.; Howard, L.M. Violence against women and mental health. Lancet Psychiatry 2017, 4, 159–170. [Google Scholar] [CrossRef] [Green Version]
- Pitzele, H.Z.; Tolia, V.M. Twenty per Hour: Altered Mental State Due to Ethanol Abuse and Withdrawal. Emerg. Med. Clin. N. Am. 2010, 28, 683–705. [Google Scholar] [CrossRef] [PubMed]
- Wagner, N.; Akbarpour, A.; Mörs, K.; Voth, M.; Störmann, P.; Auner, B.; Lehnert, M.; Marzi, I.; Relja, B. Alcohol Intoxication Reduces Systemic Interleukin-6 Levels and Leukocyte Counts After Severe TBI Compared With Not Intoxicated TBI Patients. Shock 2016, 46, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, G.; Jennett, B. Assessment of Coma and Impaired Consciousness. Lancet 1974, 304, 81–84. [Google Scholar] [CrossRef]
- Rundhaug, N.P.; Moen, K.G.; Skandsen, T.; Schirmer-Mikalsen, K.; Lund, S.B.; Hara, S.; Vik, A. Moderate and severe traumatic brain injury: Effect of blood alcohol concentration on Glasgow Coma Scale score and relation to computed tomography findings. J. Neurosurg. 2015, 122, 211–218. [Google Scholar] [CrossRef] [Green Version]
- Stuke, L.; Diaz-Arrastia, R.; Gentilello, L.M.; Shafi, S. Effect of Alcohol on Glasgow Coma Scale in Head-Injured Patients. Ann. Surg. 2007, 245, 651–655. [Google Scholar] [CrossRef]
- Weber, C.D.; Schmitz, J.K.; Garving, C.; Horst, K.; Pape, H.-C.; Hildebrand, F.; Kobbe, P. The alcohol-intoxicated trauma patient: Impact on imaging and radiation exposure. Eur. J. Trauma Emerg. Surg. 2019, 45, 871–876. [Google Scholar] [CrossRef]
- Paul, A.B.; Oklu, R.; Saini, S.; Prabhakar, A.M. How Much Is That Head CT? Price Transparency and Variability in Radiology. J. Am. Coll. Radiol. 2015, 12, 453–457. [Google Scholar] [CrossRef]
- Godbout, B.J.; Lee, J.; Newman, D.H.; Bodle, E.E.; Shah, K. Yield of head CT in the alcohol-intoxicated patient in the emergency department. Emerg. Radiol. 2011, 18, 381–384. [Google Scholar] [CrossRef] [PubMed]
- Easter, J.S.; Haukoos, J.S.; Claud, J.; Wilbur, L.; Hagstrom, M.T.; Cantrill, S.; Mestek, M.; Symonds, D.; Bakes, K. Traumatic Intracranial Injury in Intoxicated Patients With Minor Head Trauma. Acad. Emerg. Med. 2013, 20, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Hörauf, J.-A.; Nau, C.; Mühlenfeld, N.; Verboket, R.D.; Marzi, I.; Störmann, P. Injury Patterns after Falling down Stairs—High Ratio of Traumatic Brain Injury under Alcohol Influence. J. Clin. Med. 2022, 11, 697. [Google Scholar] [CrossRef]
- Stiell, I.G.; Wells, G.A.; Vandemheen, K.; Clement, C.; Lesiuk, H.; Laupacis, A.; McKnight, R.D.; Verbeek, R.; Brison, R.; Cass, D.; et al. The Canadian CT Head Rule for patients with minor head injury. Lancet 2001, 357, 1391–1396. [Google Scholar] [CrossRef] [PubMed]
- Mower, W.R.; Hoffman, J.R.; Herbert, M.; Wolfson, A.B.; Pollack, C.V.; Zucker, M.I. Developing a Decision Instrument to Guide Computed Tomographic Imaging of Blunt Head Injury Patients. J. Trauma Inj. Infect. Crit. Care 2005, 59, 954–959. [Google Scholar] [CrossRef] [Green Version]
- Schindler, C.R.; Lustenberger, T.; Marzi, I.; Verboket, R.D. Kostenfaktor “ambulante Wundversorgung” in der Notaufnahme: Kosten-Erlös-Defizit der ambulanten Wundversorgung in einer deutschen Universitätsklinik. Unfallchirurg 2021, 124, 40–47. [Google Scholar] [CrossRef]
- Mühlenfeld, N.; Schindler, C.R.; Sterz, J.; Thönissen, P.; Störmann, P.; Marzi, I.; Verboket, R.D. Kosten-Erlös-Defizit der ambulanten Versorgung von Kopfplatzwunden in der Notaufnahme. Der Chir. 2021, 92, 274–280. [Google Scholar] [CrossRef]
- Verboket, R.; Verboket, C.; Schöffski, O.; Tlatlik, J.; Marzi, I.; Nau, C. Kosten und Erlöse von über den Schockraum eingelieferten Patienten mit leichtem Schädel-Hirn-Trauma. Unfallchirurg 2019, 122, 618–625. [Google Scholar] [CrossRef]
- Staniloiu, A.; Markowitsch, H. Gender differences in violence and aggression—A neurobiological perspective. Procedia—Soc. Behav. Sci. 2012, 33, 1032–1036. [Google Scholar] [CrossRef] [Green Version]
- Kanny, D.; Naimi, T.S.; Liu, Y.; Lu, H.; Brewer, R.D. Annual Total Binge Drinks Consumed by U.S. Adults, 2015. Am. J. Prev. Med. 2018, 54, 486–496. [Google Scholar] [CrossRef]
- Crane, C.A.; Godleski, S.A.; Przybyla, S.M.; Schlauch, R.C.; Testa, M. The Proximal Effects of Acute Alcohol Consumption on Male-to-Female Aggression: A Meta-Analytic Review of the Experimental Literature. Trauma Violence Abus. 2016, 17, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Verboket, R.; Söhling, N.; Schmitz, L.; Lustenberger, T.; Nau, C.; Marzi, I. Gewalt in der Notaufnahme eines Maximalversorgers. Chir. 2019, 90, 570–575. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, S.; Jamshed, N.; Aggarwal, P.; Kashyap, S. Perception of workplace violence in the emergency department. J. Emerg. Trauma Shock 2019, 12, 179. [Google Scholar] [CrossRef]
- Gates, D.M.; Ross, C.S.; McQueen, L. Violence against emergency department workers. J. Emerg. Med. 2006, 31, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Pourshaikhian, M.; Abolghasem Gorji, H.; Aryankhesal, A.; Khorasani-Zavareh, D.; Barati, A. A Systematic Literature Review: Workplace Violence Against Emergency Medical Services Personnel. Arch. Trauma Res. 2016, in press. [Google Scholar] [CrossRef] [Green Version]
- Ramacciati, N.; Cecagnoli, A.; Addey, B.; Lumini, E.; Rasero, L. Interventions to reduce the risk of violence toward emergency department staff: Current approaches. Open Access Emerg. Med. 2016, 8, 17–27. [Google Scholar] [CrossRef] [Green Version]
- Gerdtz, M.F.; Daniel, C.; Dearie, V.; Prematunga, R.; Bamert, M.; Duxbury, J. The outcome of a rapid training program on nurses’ attitudes regarding the prevention of aggression in emergency departments: A multi-site evaluation. Int. J. Nurs. Stud. 2013, 50, 1434–1445. [Google Scholar] [CrossRef]
- Duncan, G.; Schabbing, M.; Gable, B.D. A Novel Simulation-Based Multidisciplinary Verbal De-escalation Training. Cureus 2021, 13, e20849. [Google Scholar] [CrossRef]
- Gillespie, G.L.; Gates, D.M.; Miller, M.; Howard, P.K. Emergency department workers’ perceptions of security officers’ effectiveness during violent events. Work 2012, 42, 21–27. [Google Scholar] [CrossRef]
- Vogt, I. Drug problems, community reactions and policy changes in Frankfurt/Main. Drugs Educ. Prev. Policy 2009, 16, 512–526. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Reason for Presentation | Frequency n (Total n = 355) |
|---|---|
| wound | n = 25 (7.0%) |
| impact trauma | n = 37 (10.4%) |
| distortion trauma | n = 81 (22.8%) |
| bruising trauma | n = 25 (7.0%) |
| domestic fall | n = 37 (10.4%) |
| outdoor fall | n = 57 (16.1%) |
| bicycle fall | n = 15 (4.2%) |
| traffic accident | n = 26 (7.3%) |
| redness/swelling (limb) | n = 12 (3.4%) |
| pain without trauma | n = 20 (5.6%) |
| other | n = 20 (5.6%) |
| Violence Group (n = 290) | Comparison Group (n = 355) | p-Value | |
|---|---|---|---|
| age (years) | 32.1 (±SD 10.4) | 35 (±SD 20.9) | 0.107 |
| sex (male) | n = 240 (82.8%) | n = 191 (53.8%) | <0.000 * |
| ambulance service | n = 196 (67.6%) | n = 82 (23.1%) | <0.000 * |
| trauma room | n = 30 (10.3%) | n = 6 (1.7%) | <0.000 * |
| weekend | n = 182 (62.8%) | n = 132 (37.2%) | <0.000 * |
| presentation at night | n = 220 (75.9%) | n = 40 (11.3%) | <0.000 * |
| imaging performed | n = 216 (74.5%) | n = 281 (79.2%) | 0.254 |
| CT performed | n = 120 (41.4%) | n = 32 (9%) | <0.000 * |
| wound care | n = 142 (49%) | n = 52 (14.7%) | <0.000 * |
| inpatient admission | n = 36 (12.4%) | n = 28 (7.9%) | 0.112 |
| operation | n = 14 (4.8%) | n = 19 (5.4%) | 0.811 |
| alcohol | n = 146 (50.3%) | no data |
| Violence Group (n = 290) | Comparison Group (n = 355) | p-Value | |
|---|---|---|---|
| wound | n = 136 (46.9%) | n = 28 (7.9%) | <0.000 * |
| contusion | n = 122 (42.1%) | n = 108 (30.4%) | 0.012 * |
| fracture | n = 14 (4.8%) | n = 67 (18.9%) | <0.000 * |
| dislocation | n = 2 (0.7%) | n = 8 (2.3%) | 0.233 |
| TBI | n = 16 (5.5%) | n = 6 (1.7%) | 0.019 * |
| distortion | n = 0 (0%)) | n = 78 (22%) | <0.000 * |
| other | n = 60 (16.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hörauf, J.-A.; Franz, J.-N.; Zabel, J.; Hartmann, F.; Störmann, P.; Marzi, I.; Janko, M.; Verboket, R.D. Saturday Night Fever: Interpersonal Violence as a Reason for Presentation in a University Emergency Department. Int. J. Environ. Res. Public Health 2023, 20, 4552. https://doi.org/10.3390/ijerph20054552
Hörauf J-A, Franz J-N, Zabel J, Hartmann F, Störmann P, Marzi I, Janko M, Verboket RD. Saturday Night Fever: Interpersonal Violence as a Reason for Presentation in a University Emergency Department. International Journal of Environmental Research and Public Health. 2023; 20(5):4552. https://doi.org/10.3390/ijerph20054552
Chicago/Turabian StyleHörauf, Jason-Alexander, Jan-Niklas Franz, Julian Zabel, Frederik Hartmann, Philipp Störmann, Ingo Marzi, Maren Janko, and René D. Verboket. 2023. "Saturday Night Fever: Interpersonal Violence as a Reason for Presentation in a University Emergency Department" International Journal of Environmental Research and Public Health 20, no. 5: 4552. https://doi.org/10.3390/ijerph20054552