
Associations between Coronavirus and Immune Response, Cardiorespiratory Fitness Rehabilitation and Physical Activity: A Brief Report


 , ,
, ,  ,
,  , and
, and 
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
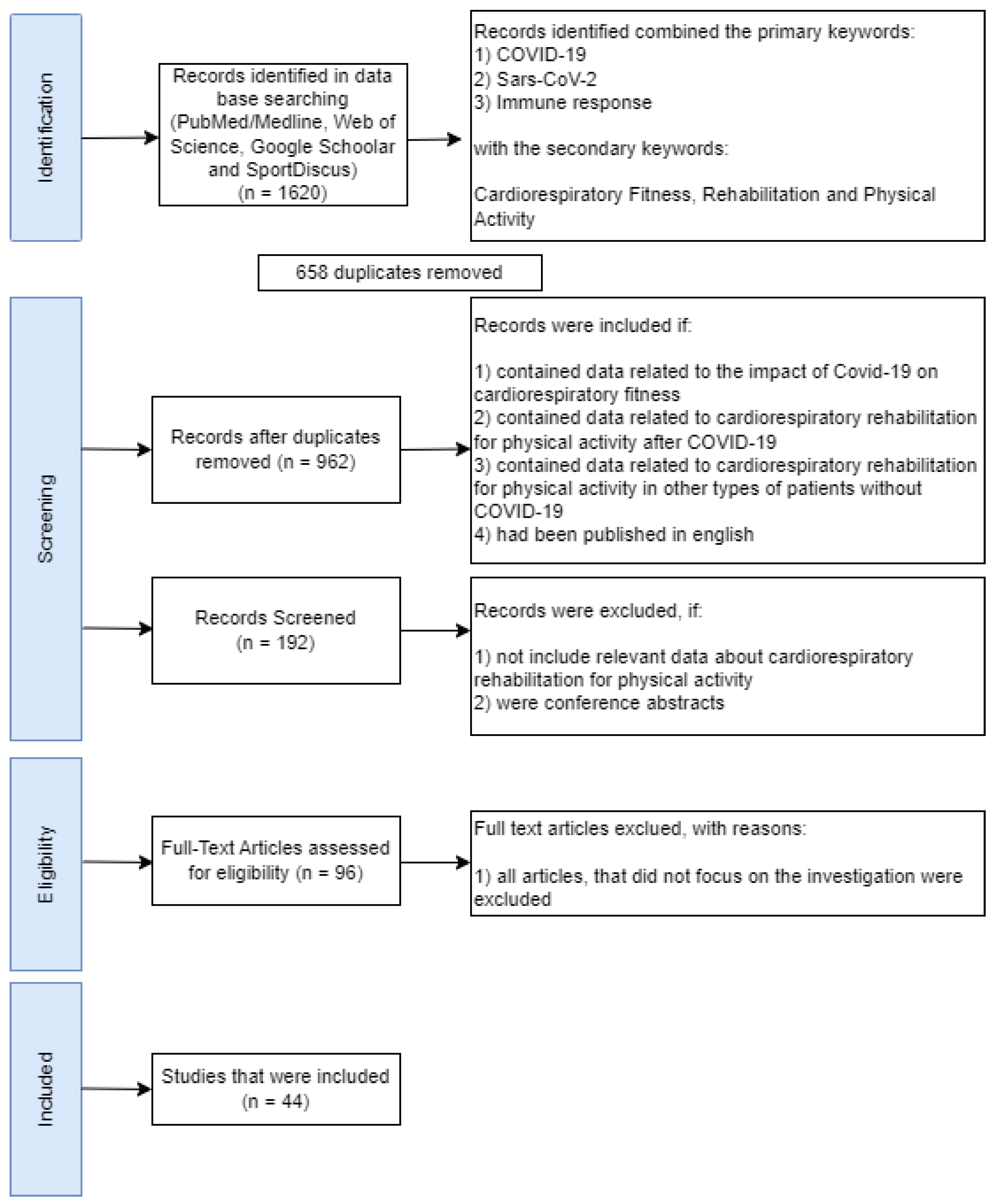
2.1. Literature Search Strategy and Selection Criteria
2.2. Selection Criteria
3. Results
3.1. The Associations between COVID-19 Symptoms and Physical Activity
3.2. COVID-19, Cardiorespiratory Fitness and Immune Response
3.3. Cardiorespiratory Fitness Rehabilitation and Physical Activity
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Menter, T.; Haslbauer, J.D.; Nienhold, R.; Savic, S.; Hopfer, H.; Deigendesch, N.; Frank, S.; Turek, D.; Willi, N.; Pargger, H.; et al. Postmortem Examination of COVID-19 Patients Reveals Diffuse Alveolar Damage with Severe Capillary Congestion and Variegated Findings in Lungs and Other Organs Suggesting Vascular Dysfunction. Histopathology 2020, 77, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Nienhold, R.; Ciani, Y.; Koelzer, V.H.; Tzankov, A.; Haslbauer, J.D.; Menter, T.; Schwab, N.; Henkel, M.; Frank, A.; Zsikla, V.; et al. Two Distinct Immunopathological Profiles in Autopsy Lungs of COVID-19. Nat. Commun. 2020, 11, 5086. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Marietta, M.; Coluccio, V.; Luppi, M. More on: ‘COVID-19 Coagulopathy in Caucasian Patients’. Br. J. Haematol. 2020, 189, 1059–1060. [Google Scholar] [CrossRef] [PubMed]
- Sittichai, N.; Parasin, N.; Saokaew, S.; Kanchanasurakit, S.; Kayod, N.; Praikaew, K.; Phisalprapa, P.; Prasannarong, M. Effects of Physical Activity on the Severity of Illness and Mortality in COVID-19 Patients: A Systematic Review and Meta-Analysis. Front. Physiol. 2022, 13, 2347. [Google Scholar] [CrossRef]
- Wang, Y.; Dong, C.; Hu, Y.; Li, C.; Ren, Q.; Zhang, X.; Shi, H.; Zhou, M. Temporal Changes of CT Findings in 90 Patients with COVID-19 Pneumonia: A Longitudinal Study. Radiology 2020, 296, E55–E64. [Google Scholar] [CrossRef] [Green Version]
- Mo, X.; Jian, W.; Su, Z.; Chen, M.; Peng, H.; Peng, P.; Lei, C.; Chen, R.; Zhong, N.; Li, S. Abnormal Pulmonary Function in COVID-19 Patients at Time of Hospital Discharge. Eur. Respir. J. 2020, 55, 2001217. [Google Scholar] [CrossRef]
- Anastasio, F.; Barbuto, S.; Scarnecchia, E.; Cosma, P.; Fugagnoli, A.; Rossi, G.; Parravicini, M.; Parravicini, P. Medium-Term Impact of COVID-19 on Pulmonary Function, Functional Capacity and Quality of Life. Eur. Respir. J. 2021, 58, 2004015. [Google Scholar] [CrossRef]
- Mitchell, B.L.; Lock, M.J.; Davison, K.; Parfitt, G.; Buckley, J.P.; Eston, R.G. What Is the Effect of Aerobic Exercise Intensity on Cardiorespiratory Fitness in Those Undergoing Cardiac Rehabilitation? A Systematic Review with Meta-Analysis. Br. J. Sports Med. 2019, 53, 1341–1352. [Google Scholar] [CrossRef]
- Gloeckl, R.; Leitl, D.; Jarosch, I.; Schneeberger, T.; Nell, C.; Stenzel, N.; Vogelmeier, C.F.; Kenn, K.; Koczulla, A.R. Benefits of Pulmonary Rehabilitation in COVID-19—A Prospective Observational Cohort Study. ERJ Open Res. 2021, 7, 00108–2021. [Google Scholar] [CrossRef] [PubMed]
- Barman, A.; Sinha, M.K.; Sahoo, J.; Jena, D.; Patel, V. Respiratory Rehabilitation in Patients Recovering from Severe Acute Respiratory Syndrome: A Systematic Review and Meta-Analysis. Heart Lung 2022, 53, 11–24. [Google Scholar] [CrossRef]
- Hatabu, H.; Ohno, Y.; Gefter, W.B.; Parraga, G.; Madore, B.; Lee, K.S.; Altes, T.A.; Lynch, D.A.; Mayo, J.R.; Seo, J.B. Expanding Applications of Pulmonary MRI in the Clinical Evaluation of Lung Disorders: Fleischner Society Position Paper. Radiology 2020, 297, 286–301. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C.; Akl, E.A.; Comerota, A.J.; Prandoni, P.; Bounameaux, H.; Goldhaber, S.Z.; Nelson, M.E.; Wells, P.S.; Gould, M.K.; Dentali, F.; et al. Antithrombotic Therapy for VTE Disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th Ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141, e419S–e496S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaff, M.R.; McMurtry, M.S.; Archer, S.L.; Cushman, M.; Goldenberg, N.; Goldhaber, S.Z.; Jenkins, J.S.; Kline, J.A.; Michaels, A.D.; Thistlethwaite, P.; et al. Management of Massive and Submassive Pulmonary Embolism, Iliofemoral Deep Vein Thrombosis, and Chronic Thromboembolic Pulmonary Hypertension: A Scientific Statement from the American Heart Association. Circulation 2011, 123, 1788–1830. [Google Scholar] [CrossRef] [Green Version]
- Amoury, M.; Noack, F.; Kleeberg, K.; Stoevesandt, D.; Lehnigk, B.; Bethge, S.; Heinze, V.; Schlitt, A. Prognosis of Patients with Pulmonary Embolism after Rehabilitation. Vasc. Health Risk Manag. 2018, 14, 183–187. [Google Scholar] [CrossRef] [Green Version]
- Al-Qahtani, M.; AlAli, S.; AbdulRahman, A.K.; Salman Alsayyad, A.; Otoom, S.; Atkin, S.L. The Prevalence of Asymptomatic and Symptomatic COVID-19 in a Cohort of Quarantined Subjects. Int. J. Infect. Dis. 2021, 102, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Wang, Y.; Shao, C.; Huang, J.; Gan, J.; Huang, X.; Bucci, E.; Piacentini, M.; Ippolito, G.; Melino, G. COVID-19 Infection: The Perspectives on Immune Responses. Cell Death Differ. 2020, 27, 1451–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonelli, M.; Donelli, D. Respiratory Rehabilitation for Post-COVID-19 Patients in Spa Centers: First Steps from Theory to Practice. Int. J. Biometeorol. 2020, 64, 1811–1813. [Google Scholar] [CrossRef]
- Medrinal, C.; Combret, Y.; Prieur, G.; Robledo Quesada, A.; Bonnevie, T.; Gravier, F.E.; Dupuis Lozeron, E.; Frenoy, E.; Contal, O.; Lamia, B. Comparison of Exercise Intensity during Four Early Rehabilitation Techniques in Sedated and Ventilated Patients in ICU: A Randomised Cross-over Trial. Crit. Care 2018, 22, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaw, D.M.; Merien, F.; Braakhuis, A.; Dulson, D. T-Cells and Their Cytokine Production: The Anti-Inflammatory and Immunosuppressive Effects of Strenuous Exercise. Cytokine 2018, 104, 136–142. [Google Scholar] [CrossRef]
- Schmidt, F.M.; Weschenfelder, J.; Sander, C.; Minkwitz, J.; Thormann, J.; Chittka, T.; Mergl, R.; Kirkby, K.C.; Faßhauer, M.; Stumvoll, M.; et al. Inflammatory Cytokines in General and Central Obesity and Modulating Effects of Physical Activity. PLoS ONE 2015, 10, e0121971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antunes, B.M.; Campos, E.Z.; dos Santos, R.V.T.; Rosa-Neto, J.C.; Franchini, E.; Bishop, N.C.; Lira, F.S. Anti-Inflammatory Response to Acute Exercise Is Related with Intensity and Physical Fitness. J. Cell. Biochem. 2019, 120, 5333–5342. [Google Scholar] [CrossRef] [Green Version]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global Trends in Insufficient Physical Activity among Adolescents: A Pooled Analysis of 298 Population-Based Surveys with 1·6 Million Participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Dickins, K.A.; Braun, L.T. Promotion of Physical Activity and Cardiac Rehabilitation for the Management of Cardiovascular Disease. J. Nurse Pract. 2017, 13, 47–53.e2. [Google Scholar] [CrossRef]
- Bostancı, Ö.; Karaduman, E.; Çolak, Y.; Yılmaz, A.K.; Kabadayı, M.; Bilgiç, S. Respiratory Muscle Strength and Pulmonary Function in Unvaccinated Athletes before and after COVID-19 Infection: A Prospective Cohort Study. Respir. Physiol. Neurobiol. 2023, 308, 103983. [Google Scholar] [CrossRef]
- Severin, R.; Franz, C.K.; Farr, E.; Meirelles, C.; Arena, R.; Phillips, S.A.; Bond, S.; Ferraro, F.; Faghy, M. The Effects of COVID-19 on Respiratory Muscle Performance: Making the Case for Respiratory Muscle Testing and Training. Eur. Respir. Rev. 2022, 31, 220006. [Google Scholar] [CrossRef]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Connor Gorber, S.; Tremblay, M. A Comparison of Direct versus Self-Report Measures for Assessing Physical Activity in Adults: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef] [Green Version]
- Gervasi, S.F.; Pengue, L.; Damato, L.; Monti, R.; Pradella, S.; Pirronti, T.; Bartoloni, A.; Epifani, F.; Saggese, A.; Cuccaro, F.; et al. Is Extensive Cardiopulmonary Screening Useful in Athletes with Previous Asymptomatic or Mild SARS-CoV-2 Infection? Br. J. Sports Med. 2021, 55, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Hur, J.; Chang, M.C. Usefulness of an Online Preliminary Questionnaire under the COVID-19 Pandemic. J. Med. Syst. 2020, 44, 116. [Google Scholar] [CrossRef] [PubMed]
- Zens, M.; Brammertz, A.; Herpich, J.; Südkamp, N.; Hinterseer, M. App-Based Tracking of Self-Reported COVID-19 Symptoms: Analysis of Questionnaire Data. J. Med. Internet Res. 2020, 22, e21956. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Syst. Rev. 2021, 10, 105906. [Google Scholar] [CrossRef] [PubMed]
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 Pathophysiology: A Review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, M.W.; Cheng, Y.; Zhang, J.; Jiang, X.M.; Wang, L.; Deng, J.; Wang, P.H. Increasing Host Cellular Receptor—Angiotensin-Converting Enzyme 2 Expression by Coronavirus May Facilitate 2019-NCoV (or SARS-CoV-2) Infection. J. Med. Virol. 2020, 92, 2693–2701. [Google Scholar] [CrossRef]
- Lee, D.H.; de Rezende, L.F.M.; Eluf-Neto, J.; Wu, K.; Tabung, F.K.; Giovannucci, E.L. Association of Type and Intensity of Physical Activity with Plasma Biomarkers of Inflammation and Insulin Response. Int. J. Cancer 2019, 145, 360–369. [Google Scholar] [CrossRef]
- Campbell, J.P.; Turner, J.E. Debunking the Myth of Exercise-Induced Immune Suppression: Redefining the Impact of Exercise on Immunological Health across the Lifespan. Front. Immunol. 2018, 9, 648. [Google Scholar] [CrossRef] [Green Version]
- Hojman, P. Exercise Protects from Cancer through Regulation of Immune Function and Inflammation. Biochem. Soc. Trans. 2017, 45, 905–911. [Google Scholar] [CrossRef]
- Jones, A.W.; Davison, G. Exercise, Immunity, and Illness. In Muscle and Exercise Physiology; Elsevier Inc.: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Miles, M.P.; Wilson, S.; Yeoman, C.J. Physical Activity and Inflammation Phenotype Conversion. J. Clin. Exerc. Physiol. 2019, 8, 64–73. [Google Scholar] [CrossRef]
- Walsh, N.P.; Gleeson, M.; Shephard, R.J.; Gleeson, M.; Woods, J.A.; Bishop, N.C.; Fleshner, M.; Green, C.; Pedersen, B.K.; Hoffman-Goetz, L.; et al. Position Statement Part One: Immune Function and Exercise. Exerc. Immunol. Rev. 2011, 17, 6–63. [Google Scholar]
- Martin, S.A.; Pence, B.D.; Woods, J.A. Exercise and Respiratory Tract Viral Infections. Exerc. Sport Sci. Rev. 2009, 37, 157–164. [Google Scholar] [CrossRef]
- Nieman, D.C.; Wentz, L.M. The Compelling Link between Physical Activity and the Body’s Defense System. J. Sport Health Sci. 2019, 8, 201–217. [Google Scholar] [CrossRef]
- Simpson, R.J.; Kunz, H.; Agha, N.; Graff, R. Exercise and the Regulation of Immune Functions. Prog. Mol. Biol. Transl. Sci. 2015, 135, 355–380. [Google Scholar] [CrossRef]
- Li, F. Receptor Recognition and Cross-Species Infections of SARS Coronavirus. Antiviral Res. 2013, 100, 246–254. [Google Scholar] [CrossRef]
- Chen, J.; Xie, Y.-Q.; Zhang, H.-T.; Wan, J.-W.; Wang, D.-T.; Lu, Z.-H.; Wang, Q.-Z.; Xue, X.-H.; Si, W.-X.; Luo, Y.-F.; et al. Lung Pathology of Severe Acute Respiratory Syndrome. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2003, 25, 360–362. [Google Scholar] [PubMed]
- Powell, K.E.; King, A.C.; Buchner, D.M.; Campbell, W.W.; DiPietro, L.; Erickson, K.I.; Hillman, C.H.; Jakicic, J.M.; Janz, K.F.; Katzmarzyk, P.T.; et al. The Scientific Foundation for the Physical Activity Guidelines for Americans, 2nd Edition. J. Phys. Act. Health 2019, 16, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Reis, R.S.; Salvo, D.; Ogilvie, D.; Lambert, E.V.; Goenka, S.; Brownson, R.C. Scaling up Physical Activity Interventions Worldwide: Stepping up to Larger and Smarter Approaches to Get People Moving. Lancet 2016, 388, 1337–1348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heitzman, J. Impact of COVID-19 Pandemic on Mental Health. Psychiatr. Pol. 2020, 54, 187–198. [Google Scholar] [CrossRef]
- Lakhan, R.; Agrawal, A.; Sharma, M. Prevalence of Depression, Anxiety, and Stress during COVID-19 Pandemic. J. Neurosci. Rural Pract. 2020, 11, 519–525. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of Stress, Anxiety, Depression among the General Population during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Global. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Al Maqbali, M.; Al Sinani, M.; Al-Lenjawi, B. Prevalence of Stress, Depression, Anxiety and Sleep Disturbance among Nurses during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. J. Psychosom. Res. 2021, 141, 110343. [Google Scholar] [CrossRef]
- Basso, J.C.; Suzuki, W.A. The Effects of Acute Exercise on Mood, Cognition, Neurophysiology, and Neurochemical Pathways: A Review. Brain Plast. 2017, 2, 127–152. [Google Scholar] [CrossRef] [Green Version]
- Daniela, M.; Catalina, L.; Ilie, O.; Paula, M.; Daniel-Andrei, I.; Ioana, B. Effects of Exercise Training on the Autonomic Nervous System with a Focus on Anti-Inflammatory and Antioxidants Effects. Antioxidants 2022, 11, 350. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Wang, Q.; Shen, J. The Impact of Physical Activity on Mental Health during COVID-19 Pandemic in China: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 6584. [Google Scholar] [CrossRef]
- Sallis, R.; Young, D.R.; Tartof, S.Y.; Sallis, J.F.; Sall, J.; Li, Q.; Smith, G.N.; Cohen, D.A. Physical Inactivity Is Associated with a Higher Risk for Severe COVID-19 Outcomes: A Study in 48 440 Adult Patients. Br. J. Sports Med. 2021, 55, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H.M.; Blaha, M.J.; Nasir, K.; Rivera, J.J.; Blumenthal, R.S. Effects of Physical Activity on Cardiovascular Disease. Am. J. Cardiol. 2012, 109, 288–295. [Google Scholar] [CrossRef]
- Bailly, M.; Pélissier, L.; Coudeyre, E.; Evrard, B.; Bingula, R.; Rochette, C.; Mériade, L.; Blavignac, C.; Fournier, A.-C.; Bignon, Y.-J.; et al. Systematic Review of COVID-19-Related Physical Activity-Based Rehabilitations: Benefits to Be Confirmed by More Robust Methodological Approaches. Int. J. Environ. Res. Public Health 2022, 19, 9025. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Li, X.; He, T.; Ju, F.; Qiu, Y.; Tian, Z. Impact of Physical Activity on COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 14108. [Google Scholar] [CrossRef]
- Ekblom-Bak, E.; Väisänen, D.; Ekblom, B.; Blom, V.; Kallings, L.V.; Hemmingsson, E.; Andersson, G.; Wallin, P.; Salier Eriksson, J.; Holmlund, T.; et al. Cardiorespiratory Fitness and Lifestyle on Severe COVID-19 Risk in 279,455 Adults: A Case Control Study. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 1–16. [Google Scholar] [CrossRef]
- Zbinden-Foncea, H.; Francaux, M.; Deldicque, L.; Hawley, J.A. Does High Cardiorespiratory Fitness Confer Some Protection Against Proinflammatory Responses After Infection by SARS-CoV-2? Obesity 2020, 28, 1378–1381. [Google Scholar] [CrossRef] [PubMed]
- Harber, M.P.; Peterman, J.E.; Imboden, M.; Kaminsky, L.; Ashton, R.E.M.; Arena, R.; Faghy, M.A. Cardiorespiratory Fitness as a Vital Sign of CVD Risk in the COVID-19 Era. Prog. Cardiovasc. Dis. 2023, in press. [Google Scholar] [CrossRef]
- Dayton, J.D.; Ford, K.; Carroll, S.J.; Flynn, P.A.; Kourtidou, S.; Holzer, R.J. The Deconditioning Effect of the COVID-19 Pandemic on Unaffected Healthy Children. Pediatr. Cardiol. 2021, 42, 554–559. [Google Scholar] [CrossRef]
- Skjørten, I.; Andre Wathne Ankerstjerne, O.; Trebinjac, D.; Brønstad, E.; Rasch-Halvorsen, Ø.; Einvik, G.; Vigeland Lerum, T.; Stavem, K.; Edvardsen, A.; Björk Ingul, C. Cardiopulmonary Exercise Capacity and Limitations 3 Months after COVID-19 Hospitalisation. Eur Respir J 2021, 58, 2100996. [Google Scholar] [CrossRef]
- Peçanha, T.; Goessler, K.F.; Roschel, H.; Gualano, B. Social Isolation during the COVID-19 Pandemic Can Increase Physical Inactivity and the Global Burden of Cardiovascular Disease. Am. J. Physiol. Circ. Physiol. 2020, 318, H1441–H1446. [Google Scholar] [CrossRef] [PubMed]
- Ragab, D.; Salah Eldin, H.; Taeimah, M.; Khattab, R.; Salem, R. The COVID-19 Cytokine Storm; What We Know so Far. Front. Immunol. 2020, 11, 1446. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W.; Crouch, R.H. Two-Minute Step Test of Exercise Capacity: Systematic Review of Procedures, Performance, and Clinimetric Properties. J. Geriatr. Phys. Ther. 2019, 42, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Sykes, K.; Roberts, A. The Chester Step Test—A Simple yet Effective Tool for the Prediction of Aerobic Capacity. Physiotherapy 2004, 90, 183–188. [Google Scholar] [CrossRef]
- Murray, J.M.; Brennan, S.F.; French, D.P.; Patterson, C.C.; Kee, F.; Hunter, R.F. Effectiveness of Physical Activity Interventions in Achieving Behaviour Change Maintenance in Young and Middle Aged Adults: A Systematic Review and Meta-Analysis. Soc. Sci. Med. 2017, 192, 125–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baert, I.; Vanlandewijck, Y.; Feys, H.; Vanhees, L.; Beyens, H.; Daly, D. Determinants of Cardiorespiratory Fitness at 3, 6 and 12 Months Poststroke. Disabil. Rehabil. 2012, 34, 1835–1842. [Google Scholar] [CrossRef]
- Paolucci, T.; Patrizio, G.; Pietrantonio, D.; Rapacchiale, G.; Spacone, A.; Parruti, G.; Graziani, G.; Damiani, M.; Liotti, V.; D’Aurizio, C. Utility of High Flow Nasal Cannula during Pulmonary Rehabilitation in COVID-19 Patients in Acute Respiratory Failure. Appl. Sci. 2022, 12, 4637. [Google Scholar] [CrossRef]
- Gosselink, R.; Kovacs, L.; Ketelaer, P.; Carton, H.; Decramer, M. Respiratory Muscle Weakness and Respiratory Muscle Training in Severely Disabled Multiple Sclerosis Patients. Arch. Phys. Med. Rehabil. 2000, 81, 747–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, H.-M.; Xie, Y.-X.; Wang, C.; Chinese Association of Rehabilitation Medicine; Respiratory Rehabilitation Committee of Chinese Association of Rehabilitation Medicine; Cardiopulmonary Rehabilitation Group of Chinese Society of Physical Medicine and Rehabilitation. Recommendations for Respiratory Rehabilitation in Adults with Coronavirus Disease 2019. Chin. Med. J. 2020, 133, 1595–1602. [Google Scholar] [CrossRef] [PubMed]
- Hermann, M.; Pekacka-Egli, A.-M.; Witassek, F.; Baumgaertner, R.; Schoendorf, S.; Spielmanns, M. Feasibility and Efficacy of Cardiopulmonary Rehabilitation Following COVID-19. Am. J. Phys. Med. Rehabil. 2020. published online. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva-Santos, S.; Monteiro, A.M.; Barbosa, T.M.; Teixeira, J.E.; Branquinho, L.; Ferraz, R.; Forte, P. Associations between Coronavirus and Immune Response, Cardiorespiratory Fitness Rehabilitation and Physical Activity: A Brief Report. Int. J. Environ. Res. Public Health 2023, 20, 4651. https://doi.org/10.3390/ijerph20054651
Silva-Santos S, Monteiro AM, Barbosa TM, Teixeira JE, Branquinho L, Ferraz R, Forte P. Associations between Coronavirus and Immune Response, Cardiorespiratory Fitness Rehabilitation and Physical Activity: A Brief Report. International Journal of Environmental Research and Public Health. 2023; 20(5):4651. https://doi.org/10.3390/ijerph20054651
Chicago/Turabian StyleSilva-Santos, Sandra, António M. Monteiro, Tiago M. Barbosa, José E. Teixeira, Luís Branquinho, Ricardo Ferraz, and Pedro Forte. 2023. "Associations between Coronavirus and Immune Response, Cardiorespiratory Fitness Rehabilitation and Physical Activity: A Brief Report" International Journal of Environmental Research and Public Health 20, no. 5: 4651. https://doi.org/10.3390/ijerph20054651
APA StyleSilva-Santos, S., Monteiro, A. M., Barbosa, T. M., Teixeira, J. E., Branquinho, L., Ferraz, R., & Forte, P. (2023). Associations between Coronavirus and Immune Response, Cardiorespiratory Fitness Rehabilitation and Physical Activity: A Brief Report. International Journal of Environmental Research and Public Health, 20(5), 4651. https://doi.org/10.3390/ijerph20054651