
Visual Characteristics of Adults with Long-Standing History of Dietary Exposure to Mercury in Grassy Narrows First Nation, Canada
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Oculo–Visual Examination
2.3. Statistical Analyses
2.4. Ethics and Informed Consent
3. Results
3.1. Visual Acuity
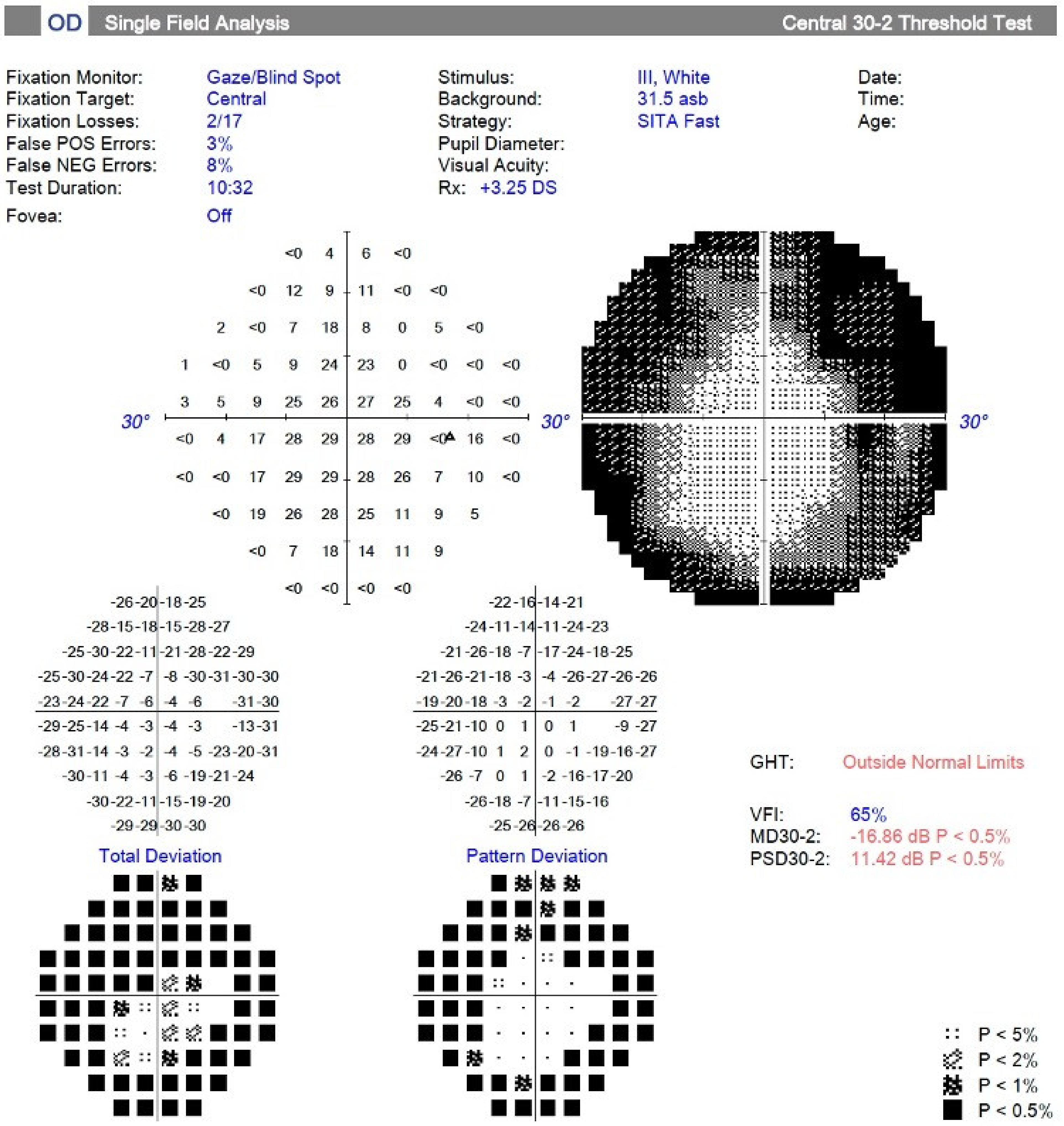
3.2. Automated Visual Field
3.3. Optical Coherence Tomography
3.4. Color Vision
3.5. Cataracts
3.6. Contrast Sensitivity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuhnlein, H.V.; Erasmus, B.; Spigelski, D.; Burlingame, B. Indigenous Peoples’ Food Systems and Well-Being: Interventions and Policies for Healthy Communities; Food and agriculture Organization of the United Nations (FAO): Rome, Italy, 2013. [Google Scholar]
- Marushka, L.; Batal, M.; Tikhonov, C.; Sadik, T.; Schwartz, H.; Ing, A.; Fediuk, K.; Chan, H.M. Importance of fish for food and nutrition security among First Nations in Canada. Can. J. Public Health 2021, 112, 64–80. [Google Scholar] [CrossRef] [PubMed]
- Roe, A. Fishing for Identity: Mercury Contamination and Fish Consumption Among Indigenous Groups in the United States. Bull. Sci. Technol. Soc. 2003, 23, 368–375. [Google Scholar] [CrossRef]
- McMillan, L.J.; Prosper, K. Remobilizing netukulimk: Indigenous cultural and spiritual connections with resource stewardship and fisheries management in Atlantic Canada. Rev. Fish Biol. Fish. 2016, 26, 629–647. [Google Scholar] [CrossRef]
- Kuhnlein, H.V.; Chotiboriboon, S. Why and How to Strengthen Indigenous Peoples’ Food Systems With Examples From Two Unique Indigenous Communities. Front. Sustain. Food Syst. Policy Pract. Rev. 2022, 6, 173. [Google Scholar] [CrossRef]
- Poirier, B.; Sethi, S.; Haag, D.; Hedges, J.; Jamieson, L. The impact of neoliberal generative mechanisms on Indigenous health: A critical realist scoping review. Glob. Health 2022, 18, 61. [Google Scholar] [CrossRef]
- Lavoie, R.A.; Jardine, T.D.; Chumchal, M.M.; Kidd, K.A.; Campbell, L.M. Biomagnification of Mercury in Aquatic Food Webs: A Worldwide Meta-Analysis. Environ. Sci. Technol. 2013, 47, 13385–13394. [Google Scholar] [CrossRef]
- Chen, J.; Jayachandran, M.; Bai, W.; Xu, B. A critical review on the health benefits of fish consumption and its bioactive constituents. Food Chem. 2022, 369, 130874. [Google Scholar] [CrossRef]
- Shahidi, F.; Ambigaipalan, P. Omega-3 Polyunsaturated Fatty Acids and Their Health Benefits. Annu. Rev. Food Sci. Technol. 2018, 9, 345–381. [Google Scholar] [CrossRef]
- Chan, H.M.; Receveur, O. Mercury in the traditional diet of indigenous peoples in Canada. Environ. Pollut. 2000, 110, 1–2. [Google Scholar] [CrossRef]
- Moriarity, R.J.; Liberda, E.N.; Tsuji, L.J.S. Subsistence fishing in the Eeyou Istchee (James Bay, Quebec, Canada): A regional investigation of fish consumption as a route of exposure to methylmercury. Chemosphere 2020, 258, 127413. [Google Scholar] [CrossRef]
- Usher, P.J. The Economic and Social Impact of Mercury Pollution on the Whitedog and Grassy Narrows Indian Reserves, Ontario; P.J. Usher Consulting Services: Ottawa, ON, Canada, 1979. [Google Scholar]
- Wheatley, B.; Paradis, S. Balancing human exposure, risk and reality: Questions raised by the Canadian aboriginal methylmercury program. Neurotoxicology 1996, 17, 241–249. [Google Scholar]
- Philibert, A.; Fillion, M.; Mergler, D. Mercury exposure and premature mortality in the Grassy Narrows First Nation community: A retrospective longitudinal study. Lancet Planet Health 2020, 4, e141–e148. [Google Scholar] [CrossRef]
- Neff, M.R.; Bhavsar, S.P.; Arhonditsis, G.B.; Fletcher, R.; Jackson, D.A. Long-term changes in fish mercury levels in the historically impacted English-Wabigoon River system (Canada). J. Environ. Monit. 2012, 14, 2327–2337. [Google Scholar] [CrossRef]
- Rudd, J.W.M.; Kelly, C.A.; Sellers, P.; Flett, R.J.; Townsend, B.E. Why the English–Wabigoon river system is still polluted by mercury 57 years after its contamination. FACETS 2021, 6, 2002–2027. [Google Scholar] [CrossRef]
- Clarkson, T.W.; Magos, L.; Myers, G.J. The toxicology of mercury--current exposures and clinical manifestations. N. Engl. J. Med. 2003, 349, 1731–1737. [Google Scholar] [CrossRef] [Green Version]
- Jackson, A.C. Chronic Neurological Disease Due to Methylmercury Poisoning. Can. J. Neurol. Sci. 2018, 45, 620–623. [Google Scholar] [CrossRef] [Green Version]
- Fox, D.A. Retinal and visual system: Occupational and environmental toxicology. Handb. Clin. Neurol. 2015, 131, 325–340. [Google Scholar] [CrossRef]
- Eto, K. Minamata disease. Neuropathol. Off. J. Jpn. Soc. Neuropathol. 2000, 20 (Suppl. S1), S14–S19. [Google Scholar] [CrossRef]
- Ekino, S.; Susa, M.; Ninomiya, T.; Imamura, K.; Kitamura, T. Minamata disease revisited: An update on the acute and chronic manifestations of methyl mercury poisoning. J. Neurol. Sci. 2007, 262, 131–144. [Google Scholar] [CrossRef]
- Uchino, M.; Tanaka, Y.; Ando, Y.; Yonehara, T.; Hara, A.; Mishima, I.; Okajima, T.; Ando, M. Neurologic features of chronic minamata disease (organic mercury poisoning) and incidence of complications with aging. J. Environ. Sci. Health B 1995, 30, 699–715. [Google Scholar] [CrossRef]
- Korogi, Y.; Takahashi, M.; Sumi, M.; Hirai, T.; Okuda, T.; Shinzato, J.; Okajima, T. MR imaging of minamata disease: Qualitative and quantitative analysis. Radiat. Med. 1994, 12, 249–253. [Google Scholar] [PubMed]
- Korogi, Y.; Takahashi, M.; Hirai, T.; Ikushima, I.; Kitajima, M.; Sugahara, T.; Shigematsu, Y.; Okajima, T.; Mukuno, K. Representation of the visual field in the striate cortex: Comparison of MR findings with visual field deficits in organic mercury poisoning (Minamata disease). AJNR Am. J. Neuroradiol. 1997, 18, 1127–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korogi, Y.; Takahashi, M.; Okajima, T.; Eto, K. MR findings of Minamata disease—Organic mercury poisoning. J. Magn. Reason. Imaging 1998, 8, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Holmes, G. The organization of the visual cortex in man. Proc. R. Soc. B Biol. Sci. 1945, 132, 348–361. [Google Scholar]
- Mukuno, K.; Ishikawa, S.; Okamura, R. Grating test of contrast sensitivity in patients with Minamata disease. Br. J. Ophthalmol. 1981, 65, 284–290. [Google Scholar] [CrossRef] [Green Version]
- Fillion, M.; Lemire, M.; Philibert, A.; Frenette, B.; Weiler, H.A.; Deguire, J.R.; Guimarães, J.R.D.; Larribe, F.; Barbosa, F., Jr.; Mergler, D. Toxic risks and nutritional benefits of traditional diet on near visual contrast sensitivity and color vision in the Brazilian Amazon. Neurotoxicology 2013, 37, 173–181. [Google Scholar] [CrossRef]
- Fillion, M.; Lemire, M.; Philibert, A.; Frenette, B.; Weiler, H.A.; Deguire, J.R.; Guimarães, J.R.D.; Larribe, F.; Barbosa, F.; Mergler, D. Visual acuity in fish consumers of the Brazilian Amazon: Risks and benefits from local diet. Public Health Nutr. 2011, 14, 2236–2244. [Google Scholar] [CrossRef] [Green Version]
- Feitosa-Santana, C.; Souza, G.D.S.; Sirius, E.V.P.; Rodrigues, A.R.; Cortes, M.I.T.; Silveira, L.C.D.L.; Ventura, D.F. Color vision impairment with low-level methylmercury exposure of an Amazonian population—Brazil. Neurotoxicology 2018, 66, 179–184. [Google Scholar] [CrossRef]
- Lemire, M.; Fillion, M.; Frenette, B.; Mayer, A.; Philibert, A.; Passos, C.J.S.; Guimaraes, J.R.D.; Barbosa, F.; Mergler, N. Selenium and mercury in the Brazilian Amazon: Opposing influences on age-related cataracts. Environ. Health Perspect. 2010, 118, 1584–1589. [Google Scholar] [CrossRef]
- Eto, K.; Takeuchi, T. Pathological changes of human sural nerves in Minamato disease (methylmercury poisoning). Light and electron microscopic studies. Virchows Arch. B Cell Pathol. 1977, 23, 109–128. [Google Scholar] [CrossRef]
- Murata, K.; Weihe, P.; Renzoni, A.; Debes, F.; Vasconcelos, R.; Zino, F.; Araki, S.; Jørgensen, P.J.; White, R.F.; Grandjean, P. Delayed evoked potentials in children exposed to methylmercury from seafood. Neurotoxicol. Teratol. 1999, 21, 343–348. [Google Scholar] [CrossRef]
- Polevoy, C.; Arbuckle, T.E.; Oulhote, Y.; Lanphear, B.P.; Cockell, K.A.; Muckle, G.; Saint-Amour, D. Prenatal exposure to legacy contaminants and visual acuity in Canadian infants: A maternal-infant research on environmental chemicals study (MIREC-ID). Environ. Health A Glob. Access Sci. Source 2020, 19, 1. [Google Scholar] [CrossRef] [Green Version]
- Saint-Amour, D.; Roy, M.-S.; Bastien, C.; Ayotte, P.; Dewailly, E.; Després, C.; Gingras, S.; Muckle, G. Alterations of visual evoked potentials in preschool Inuit children exposed to methylmercury and polychlorinated biphenyls from a marine diet. NeuroToxicology 2006, 27, 567–578. [Google Scholar] [CrossRef]
- Yorifuji, T.; Murata, K.; Bjerve, K.S.; Choi, A.L.; Weihe, P.; Grandjean, P. Visual evoked potentials in children prenatally exposed to methylmercury. NeuroToxicology 2013, 37, 15–18. [Google Scholar] [CrossRef] [Green Version]
- Korbas, M.; Lai, B.; Vogt, S.; Gleber, S.-C.; Karunakaran, C.; Pickering, I.; Krone, P.H.; George, G.N. Methylmercury targets photoreceptor outer segments. ACS Chem. Biol. 2013, 8, 2256–2263. [Google Scholar] [CrossRef]
- Goto, Y.; Shigematsu, J.; Tobimatsu, S.; Sakamoto, T.; Kinukawa, N.; Kato, M. Different vulnerability of rat retinal cells to methylmercury exposure. Curr. Eye Res. 2001, 23, 171–178. [Google Scholar] [CrossRef]
- Mela, M.; Grötzner, S.R.; Legeay, A.; Mesmer-Dudons, N.; Massabuau, J.-C.; Ventura, D.F.; Ribeiro, C.A.D.O. Morphological evidence of neurotoxicity in retina after methylmercury exposure. Neurotoxicology 2012, 33, 407–415. [Google Scholar] [CrossRef]
- Finocchio, D.V.; Luschei, E.S.; Mottet, N.K.; Body, R. Effects of methylmercury on the visual system of rhesus macaque (Macaca Mulatta). I. Pharmacokinetics of chronic methylmercury related to changes in vision and behavior. Neurotox. Vis. Syst. 1980, 11, 113. [Google Scholar]
- Rice, D.C.; Gilbert, S.G. Early chronic low-level methylmercury poisoning in monkeys impairs spatial vision. Science 1982, 216, 759–761. [Google Scholar] [CrossRef]
- Rice, D.C.; Gilbert, S.G. Effects of developmental exposure to methyl mercury on spatial and temporal visual function in monkeys. Toxicol. Appl. Pharmacol. 1990, 102, 151–163. [Google Scholar] [CrossRef]
- Philibert, A.; Fillion, M.; Da Silva, J.; Lena, T.S.; Mergler, D. Past mercury exposure and current symptoms of nervous system dysfunction in adults of a First Nation community (Canada). Environ. Health 2022, 21, 34. [Google Scholar] [CrossRef] [PubMed]
- Ferris, F.L., 3rd; Kassoff, A.; Bresnick, G.H.; Bailey, I. New visual acuity charts for clinical research. Am. J. Ophthalmol. 1982, 94, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Thylefors, B.; Chylack, L.T., Jr.; Konyama, K.; Sasaki, K.; Sperduto, R.; Taylor, H.R.; West4, S. A simplified cataract grading system. Ophthalmic. Epidemiol. 2002, 9, 83–95. [Google Scholar] [CrossRef]
- Cole, B.L.; Lian, K.Y.; Lakkis, C. The new Richmond HRR pseudoisochromatic test for colour vision is better than the Ishihara test. Clin. Exp. Optom. 2006, 89, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Huna-Baron, R.; Glovinsky, Y.; Habot-Wilner, Z. Comparison between Hardy-Rand-Rittler 4th edition and Ishihara color plate tests for detection of dyschromatopsia in optic neuropathy. Graefes. Arch. Clin. Exp. Ophthalmol. 2013, 251, 585–589. [Google Scholar] [CrossRef]
- Foote, K.G.; Neitz, M.; Neitz, J. Comparison of the Richmond HRR 4th edition and Farnsworth-Munsell 100 Hue Test for quantitative assessment of tritan color deficiencies. J. Opt. Soc. Am. A Opt. Image Sci. Vis. 2014, 31, A186–A188. [Google Scholar] [CrossRef]
- Bowman, K.J. A method for quantitative scoring of the Farnsworth Panel D-15. Acta Ophthalmol. Copenh. 1982, 60, 907–916. [Google Scholar] [CrossRef]
- Stamler, C.J.; Mergler, D.; Abdelouahab, N.; Vanier, C.; Chan, H.M. Associations between platelet monoamine oxidase-B activity and acquired colour vision loss in a fish-eating population. Neurotoxicol. Teratol. 2006, 28, 446–452. [Google Scholar] [CrossRef]
- Dougherty, B.E.; Flom, R.E.; Bullimore, M.A. An evaluation of the Mars Letter Contrast Sensitivity Test. Optom. Vis. Sci. 2005, 82, 970–975. [Google Scholar] [CrossRef] [Green Version]
- Hepworth, L.R.; Rowe, F.J. Programme choice for perimetry in neurological conditions (PoPiN): A systematic review of perimetry options and patterns of visual field loss. BMC Ophthalmol. 2018, 18, 241. [Google Scholar] [CrossRef]
- Zhang, H.G.; Ying, G.S. Statistical approaches in published ophthalmic clinical science papers: A comparison to statistical practice two decades ago. Br. J. Ophthalmol. 2018, 102, 1188–1191. [Google Scholar] [CrossRef]
- Armstrong, R.A. Statistical guidelines for the analysis of data obtained from one or both eyes. Ophthalmic. Physiol. Opt. 2013, 33, 7–14. [Google Scholar] [CrossRef]
- FNIGC. The First Nations Principles of OCAP®. Available online: https://fnigc.ca/ocap-training/ (accessed on 11 August 2022).
- Hirasawa, K.; Shoji, N.; Morita, T.; Shimizu, K. A modified glaucoma staging system based on visual field index. Graefes. Arch. Clin. Exp. Ophthalmol. 2013, 251, 2747–2752. [Google Scholar] [CrossRef]
- Rustam, H.; Hamdi, T. Methyl mercury poisoning in Iraq. A neurological study. Brain 1974, 97, 500–510. [Google Scholar] [CrossRef]
- Wheatley, B.; Barbeau, A.; Clarkson, T.W.; Lapham, L.W. Methylmercury poisoning in Canadian Indians--the elusive diagnosis. Can. J. Neurol. Sci. 1979, 6, 417–422. [Google Scholar] [CrossRef] [Green Version]
- Harada, M. Minamata Disease: Methylmercury Poisoning in Japan Caused by Environmental Pollution AU—Harada, Masazumi. Crit. Rev. Toxicol. 1995, 25, 1–24. [Google Scholar] [CrossRef]
- Harada, M.; Fujino, T.; Oorui, T.; Nakachi, S.; Nou, T.; Kizaki, T.; Hitomi, Y.; Nakano, N.; Ohno, H. Followup Study of Mercury Pollution in Indigenous Tribe Reservations in the Province of Ontario, Canada, 1975–2002. Bull. Environ. Contam. Toxicol. 2005, 74, 689–697. [Google Scholar] [CrossRef]
- Harada, M.; Hanada, M.; Tajiri, M.; Inoue, Y.; Hotta, N.; Fujino, T.; Takaoka, S.; Ueda, K. Mercury Poisoning in First Nations Groups in Ontario, Canada 35 years of Minamata Disease in Canada. J. Minamata Stud. 2011, 3, 3–30. [Google Scholar]
- Takaoka, S.; Kawakami, Y.; Fujino, T.; Oh-Ishi, F.; Motokura, F.; Kumagai, Y.; Miyaoka, T. Somatosensory disturbance by methylmercury exposure. Environ. Res. 2008, 107, 6–19. [Google Scholar] [CrossRef]
- Takaoka, S.; Fujino, T.; Hotta, N.; Ueda, K.; Hanada, M.; Tajiri, M.; Inoue, Y. Signs and symptoms of methylmercury contamination in a First Nations community in Northwestern Ontario, Canada. Sci. Total Environ. 2014, 468–469, 950–957. [Google Scholar] [CrossRef]
- Lacerda, E.M.D.C.B.; Souza, G.D.S.; Cortes, M.I.T.; Rodrigues, A.R.; Pinheiro, M.C.N.; Silveira, L.C.D.L.; Ventura, D.F. Comparison of Visual Functions of Two Amazonian Populations: Possible Consequences of Different Mercury Exposure. Front. Neurosci. 2019, 13, 1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takaoka, S.; Fujino, T.; Kawakami, Y.; Shigeoka, S.I.; Yorifuji, T. Survey of the Extent of the Persisting Effects of Methylmercury Pollution on the Inhabitants around the Shiranui Sea, Japan. Toxics 2018, 6, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeuchi, T.; Eto, K.; Oyanag, S.; Miyajima, H. Ultrastructural changes of human sural nerves in the neuropathy induced by intrauterine methylmercury poisoning (so-called fetal Minamata disease). Virchows Arch. B Cell Pathol. 1978, 27, 137–154. [Google Scholar] [CrossRef] [PubMed]
- Eto, K. Pathology of Minamata disease. Toxicol. Pathol. 1997, 25, 614–623. [Google Scholar] [CrossRef] [Green Version]
- Sihota, R.; Gupta, V.; Tuli, D.; Sharma, A.; Sony, P.; Srinivasan, G. Classifying patterns of localized glaucomatous visual field defects on automated perimetry. J. Glaucoma. 2007, 16, 146–152. [Google Scholar] [CrossRef]
- Hamel, C. Retinitis pigmentosa. Orphanet. J. Rare Dis. 2006, 1, 40. [Google Scholar] [CrossRef]
- Fillion, M.; Philibert, A.; Mertens, F.; Lemire, M.; Passos, C.J.S.; Frenette, B.; Guimarães, J.R.D.; Mergler, D. Neurotoxic sequelae of mercury exposure: An intervention and follow-up study in the Brazilian Amazon. Ecohealth 2011, 8, 210–222. [Google Scholar] [CrossRef]
- Pamphlett, R.; Jew, S.K.; Cherepanoff, S. Mercury in the retina and optic nerve following prenatal exposure to mercury vapor. PLoS ONE 2019, 14, e0220859. [Google Scholar] [CrossRef] [Green Version]
- Warfvinge, K.; Bruun, A. Mercury distribution in the squirrel monkey retina after in utero exposure to mercury vapor. Environ. Res. 2000, 83, 102–109. [Google Scholar] [CrossRef]
- Uludag, G.; Ekinci, M.; Ceylan, E.; Keleş, S.; Çağatay, H.H.; Apil, A.; Tanyıldız, B. Toxic effects of chronic mercury exposure on the retinal nerve fiber layer and macular and choroidal thickness in industrial mercury battery workers. Med. Sci. Monit. 2014, 20, 1284–1290. [Google Scholar] [CrossRef] [Green Version]
- Bilak, Ş.; Önderci, M.; Şimşek, A. Evaluation of amalgam-related retinal neurotoxicity with optical coherence tomography findings. Hum. Exp. Toxicol. 2019, 38, 814–822. [Google Scholar] [CrossRef]
- Alasil, T.; Wang, K.; Yu, F.; Field, M.G.; Lee, H.; Baniasadi, N.; de Boer, J.F.; Coleman, A.L.; Chen, T.C. Correlation of retinal nerve fiber layer thickness and visual fields in glaucoma: A broken stick model. Am. J. Ophthalmol. 2014, 157, 953–959. [Google Scholar] [CrossRef] [Green Version]
- Knight, O.J.; Girkin, C.A.; Budenz, D.L.; Durbin, M.K.; Feuer, W.J. Effect of race, age, and axial length on optic nerve head parameters and retinal nerve fiber layer thickness measured by Cirrus HD-OCT. Arch. Ophthalmol. 2012, 130, 312–318. [Google Scholar] [CrossRef]
- Mehta, N.; Waheed, N.K. Diversity in optical coherence tomography normative databases: Moving beyond race. Int. J. Retina Vitreous 2020, 6, 5. [Google Scholar] [CrossRef]
- Ho, H.; Tham, Y.-C.; Chee, M.L.; Shi, Y.; Tan, N.Y.; Wong, K.-H.; Majithia, S.; Cheung, C.Y.; Aung, T.; Wong, T.Y.; et al. Retinal Nerve Fiber Layer Thickness in a Multiethnic Normal Asian Population: The Singapore Epidemiology of Eye Diseases Study. Ophthalmology 2019, 126, 702–711. [Google Scholar] [CrossRef] [Green Version]
- Fareed, M.; Anwar, M.A.; Afzal, M. Prevalence and gene frequency of color vision impairments among children of six populations from North Indian region. Genes Dis. 2015, 2, 211–218. [Google Scholar] [CrossRef] [Green Version]
- Freitas, J.D.S.; Lacerda, E.M.D.C.B.; Martins, I.C.V.D.S.; Rodrigues, D.; Bonci, D.M.O.; Cortes, M.I.T.; Corvelo, T.C.O.; Ventura, D.F.; Silveira, L.C.D.L.; Pinheiro, M.D.C.N.; et al. Cross-sectional study to assess the association of color vision with mercury hair concentration in children from Brazilian Amazonian riverine communities. Neurotoxicology 2018, 65, 60–67. [Google Scholar] [CrossRef]
- Lebel, J.; Mergler, D.; Lucotte, M.; Amorim, M.; Dolbec, J.; Miranda, D.; Arantes, G.; Rheault, I.; Pichet, P. Evidence of early nervous system dysfunction in Amazonian populations exposed to low-levels of methylmercury. Neurotoxicology 1996, 17, 157–167. [Google Scholar]
- Rodrigues, A.; Souza, C.; Braga, A.; Rodrigues, P.; Silveira, A.; Damin, E.; Côrtes, M.; Castro, A.; Mello, G.; Vieira, J.; et al. Mercury toxicity in the Amazon: Contrast sensitivity and color discrimination of subjects exposed to mercury. Braz. J. Med. Biol. Res. 2007, 40, 415–424. [Google Scholar] [CrossRef] [Green Version]
- Lebel, J.; Mergler, D.; Branches, F.; Lucotte, M.; Amorim, M.; Larribe, F.; Dolbec, J. Neurotoxic effects of low-level methylmercury contamination in the Amazonian Basin. Environ. Res. 1998, 79, 20–32. [Google Scholar] [CrossRef]
- Breitmeyer, B.G.; Tripathy, S.P.; Brown, J.M. Can Contrast-Response Functions Indicate Visual Processing Levels? Vision 2018, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avidan, G.; Harel, M.; Hendler, T.; Ben-Bashat, D.; Zohary, E.; Malach, R. Contrast sensitivity in human visual areas and its relationship to object recognition. J. Neurophysiol. 2002, 87, 3102–3116. [Google Scholar] [CrossRef] [Green Version]
- Baker, C.L., Jr.; Mareschal, I. Processing of second-order stimuli in the visual cortex. Prog. Brain Res. 2001, 134, 171–191. [Google Scholar] [CrossRef]

{kind=link}
| N | Median logMAR (IQR) | |
|---|---|---|
| Distance visual acuity (presenting) | ||
| Crude monocular (without pinhole) | 78 | 0.2 (0.1–0.27) |
| Optimized monocular (adjusted with pinhole for n = 32) | 80 | 0.1 (0–0.2) |
| Binocular | 80 | 0.1 (0–0.2) |
| Near visual acuity (presenting) | ||
| Binocular | 80 | 0.3 (0.3–0.5) |
| Visual Field Indices/Analyses | N | Median (IQR)/n (%) |
|---|---|---|
| Mean Deviation (MD) | 68 | −5.59 (−17.3; −2.36) |
| MD < −12 dB | 68 | 21 (31%) |
| MD P < 0.5% | 68 | 34 (50%) |
| Pattern Standard Deviation (PSD) | 70 | 5 (2.27–7.81) |
| PSD P < 0.5% | 70 | 37 (53.6%) |
| Visual Field Index VFI (%) | 70 | 92 (63–98) |
| VFI > 81% | 48 (64%) | |
| VFI < 62% | 18 (25.7%) | |
| VFI < 15% | 6 (8.57%) | |
| Glaucoma Hemifield Test (GHT) | 75 | |
| Within normal limits | 17 (24%) | |
| Borderline | 5 (7%) | |
| Outside normal limits | 48 (69%) | |
| Qualitative assessment (based on pattern deviation plot) | 68 | |
| Normal | 16 (23.5%) | |
| Mild scattered defects | 8 (17.8%) | |
| Moderate concentric constriction | 12 (17.6%) | |
| End-stage concentric constriction | 12 (17.6%) | |
| Complex defects | 15 (23.5%) | |
| Central defects | 1 (1.47%) | |
| Other localized scotomas | 3 (4.41%) | |
| Scotomas (more than three contiguous points with P < 0.5%) | ||
| Total deviation plot | 68 | 45 (66%) |
| Pattern deviation plot | 54 | 27 (51%) |
| OCT Scans | N | Median Thickness μm (IQR) | Measurement in Green/Normal Range n (%) |
|---|---|---|---|
| Optic Disc Cube | |||
| Average RNFL thickness | 70 | 86.5 (79–92) | 52 (74.3%) |
| Thickness (by quadrant) | |||
| Superior | 70 | 103 (94–114) | 57 (81.4%) |
| Nasal | 70 | 70.5 (62.8–77) | 62 (88.5%) |
| Inferior | 70 | 102 (103–125) | 56 (80%) |
| Temporal | 70 | 54 (46–61) | 56 (80%) |
| Macular Cube | |||
| Average GCL + IPL thickness | 68 | 78 (72–82) | 51 (75%) |
| Minimum GCL + IPL thickness | 68 | 74.5 (66.3–79) | 48 (70.6%) |
| Thickness (by section) | |||
| Superior | 68 | 78 (72.3–83.8) | 52 (76.5%) |
| Superior nasal | 68 | 79 (74.3–85.8) | 56 (82.3%) |
| Inferior nasal | 68 | 77 (72–83) | 54 (79.4%) |
| Inferior | 68 | 76 (70–81) | 54 (79.4%) |
| Inferior temporal | 68 | 78 (72–83) | 55 (80.8%) |
| Superior temporal | 68 | 77 (72–83) | 54 (79.4%) |
| Color Vision Test | N | n (%)/Median (IQR) |
|---|---|---|
| HRR testing (monocular) | ||
| B–Y defect | 77 | 27 (37.1%) |
| R–G defect | 77 | 29 (37.7%) |
| Color defect categories | 77 | |
| B–Y normal and R–G normal | 46 (49.7%) | |
| B–Y normal and R–G defect | 4 (5.20%) | |
| B–Y defect and R–G normal | 2 (2.60%) | |
| B–Y defect and R–G defect | 25 (32.5%) | |
| D-15 testing | ||
| Saturated, CCI (binocular) | 80 | 1.17 (1–1.46) |
| CCI > 1.2 | 44 (55%) | |
| Desaturated, CCI (monocular) | 77 | 1.59 (1.32–1.96) |
| CCI > 1.2 | 67 (87%) |
| N | Median (IQR)/n (%) | |
|---|---|---|
| 20 cm (high spatial frequencies) | 76 | |
| log CS | 1.48 (1.36–1.64) | |
| Categories | ||
| Normal | 8 (10.5%) | |
| Moderate | 65 (85.5%) | |
| Severe | 3 (3.95%) | |
| 40 cm (medium spatial frequencies) | 76 | |
| log CS | 1.48 (1.32–1.67) | |
| Categories | ||
| Normal | 10 (13.2%) | |
| Moderate | 63 (82.9%) | |
| Severe | 3 (3.9%) | |
| 80 cm (low spatial frequencies) | 76 | |
| log CS | 1.44 (1.29–1.56) | |
| Categories | ||
| Normal | 7 (9.2%) | |
| Moderate | 63 (82.9%) | |
| Severe | 6 (7.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tousignant, B.; Chatillon, A.; Philibert, A.; Da Silva, J.; Fillion, M.; Mergler, D. Visual Characteristics of Adults with Long-Standing History of Dietary Exposure to Mercury in Grassy Narrows First Nation, Canada. Int. J. Environ. Res. Public Health 2023, 20, 4827. https://doi.org/10.3390/ijerph20064827
Tousignant B, Chatillon A, Philibert A, Da Silva J, Fillion M, Mergler D. Visual Characteristics of Adults with Long-Standing History of Dietary Exposure to Mercury in Grassy Narrows First Nation, Canada. International Journal of Environmental Research and Public Health. 2023; 20(6):4827. https://doi.org/10.3390/ijerph20064827
Chicago/Turabian StyleTousignant, Benoit, Annie Chatillon, Aline Philibert, Judy Da Silva, Myriam Fillion, and Donna Mergler. 2023. "Visual Characteristics of Adults with Long-Standing History of Dietary Exposure to Mercury in Grassy Narrows First Nation, Canada" International Journal of Environmental Research and Public Health 20, no. 6: 4827. https://doi.org/10.3390/ijerph20064827