
COVID-19 Public Health Measures and Patient and Public Involvement in Health and Social Care Research: An Umbrella Review

 , , , , , , , , , , , ,
, , , , , , , , , , , ,  and
and 
Abstract
:1. Introduction
2. Aim, Objectives and Research Questions
- Explore the scientific evidence of incorporating PPI.
- Summarize the current evidence on COVID-19, including PPI, and determine where and when the research was conducted.
- Identify the members of the public and the types of patients who participated.
- Identify any gaps in the literature or study designs that should be further explored and emphasized in future public health measures (PHM) and PPI research.
- Have systematic reviews of PHM during the COVID-19 pandemic reported on assessed PPI activities?
- What were the PPI activities, and who/what populations were likely to be left out?
- What are the similarities and differences in the effectiveness of PHM between the systematic review studies?
3. Research Design
3.1. Search Stratgey
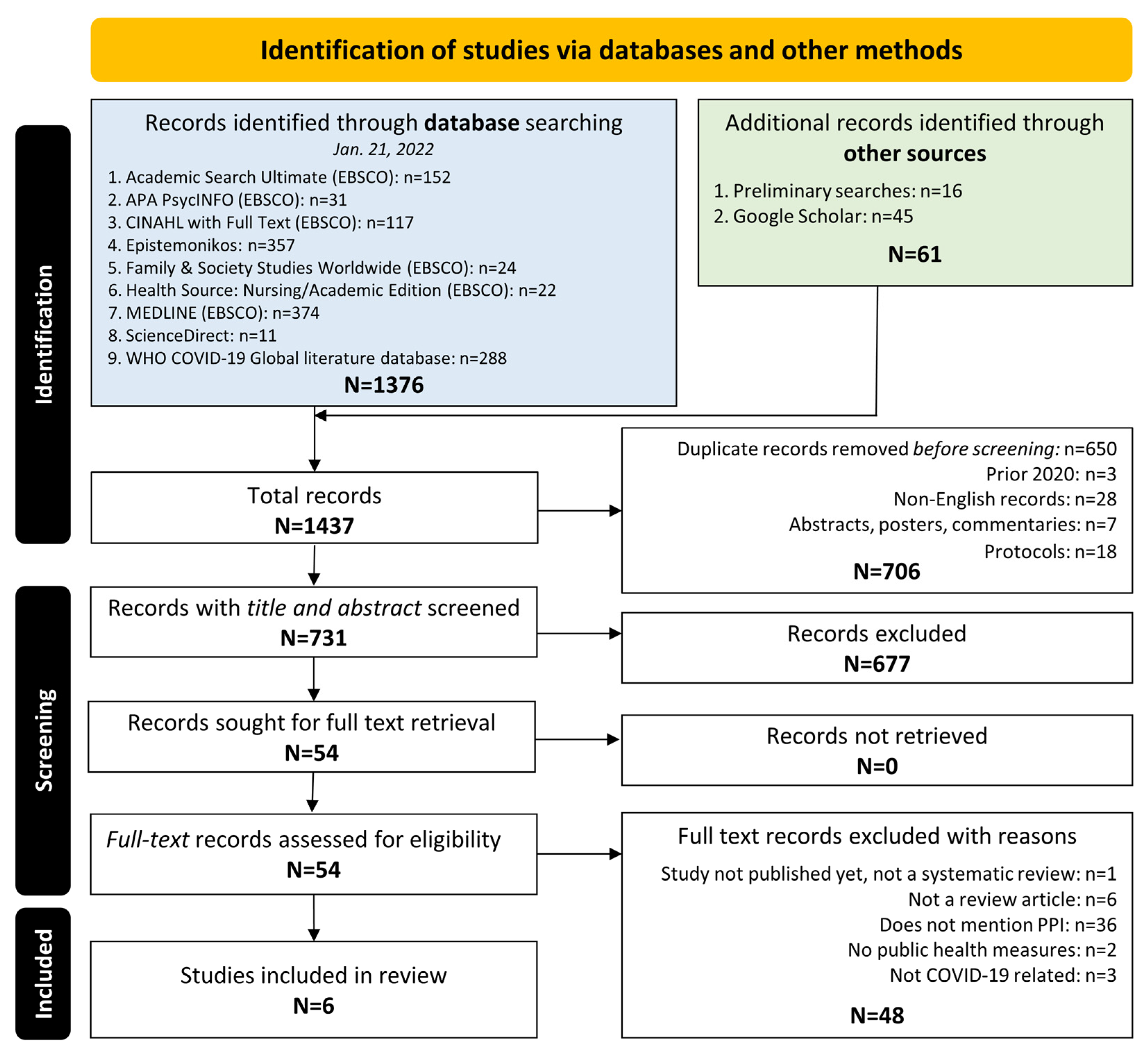
- We conducted preliminary searches to find published reviews in the literature on patient and public involvement (PPI) and public health measures (PHM) during the pandemic. Among the databases searched were the 3iE Database, BMC Systematic Reviews, Campbell Collaboration, Centre for Reviews and Dissemination, Cochrane Library, JBI Evidence Synthesis, PROSPERO, and Google Scholar.
- In the next stage of the search, nine databases (EBSCO interface—Academic Search Ultimate, APA PsycINFO, CINAHL, Family & Society Studies Worldwide, Health Source: Nursing/Academic Edition, MEDLINE; Epistemonikos, ScienceDirect and WHO COVID-19 Global Literature) were searched on 21 January 2022.
- Finally, a Google Scholar search was again conducted with the included studies identified from the title/abstract stage. Using the cited by feature, reference lists were checked to identify additional studies that could be appropriate for inclusion.
3.2. Inclusion and Exclusion Criteria
- Qualitative studies include designs such as grounded theory, ethnography, phenomenology, action research, and qualitative descriptive.
- Quantitative studies include both experimental (e.g., randomized trials, non-randomized trials) and observational (e.g., cohort, cross-sectional) study designs.
- We also considered case series, individual case reports, health intervention, or service development.
3.3. Study Screening and Selection
3.4. Assessment of Methodological Quality/Critical Appraisal of the Included Systematic Reviews
3.5. Data Extraction
3.6. Data Summary
4. Results
4.1. Study Inclusion
4.2. Methodological Quality of Included Systematic Reviews
4.3. Characteristics of Included Studies
4.4. Findings of the Review
5. Summary of Evidence
5.1. Benefits of Patient and Public Involvement (PPI)
5.2. Public Health Measures (PHM) Approaches
5.3. Patient and Public Involvement (PPI) Population and Engagement Strategies
5.4. Challenges to Patient and Public Involvement (PPI) and Public Health Measures (PHM) during the COVID-19 Pandemic
6. Discussion
7. Limitations
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Murphy, E.; Tierney, E.; Shé, É.N.; Killilea, M.; Donaghey, C.; Daly, A.; Roche, M.; Loughlin, D.M.; Dinneen, S. COVID-19: Public and Patient Involvement, Now More than Ever. HRB Open Res. 2020, 3, 35. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Research. What Is Patient and Public Involvement and Public Engagement? Available online: https://www.spcr.nihr.ac.uk/PPI/what-is-patient-and-public-involvement-and-engagement (accessed on 8 March 2023).
- National Institute for Health and Care Research Annual Report 2020/2021. Available online: https://www.nihr.ac.uk/documents/annual-report-20202021/30206 (accessed on 20 June 2022).
- Brett, J.; Staniszewska, S.; Mockford, C.; Herron-Marx, S.; Hughes, J.; Tysall, C.; Suleman, R. Mapping the Impact of Patient and Public Involvement on Health and Social Care Research: A Systematic Review. Health Expect. 2014, 17, 637–650. [Google Scholar] [CrossRef] [PubMed]
- Staniszewska, S.; Brett, J.; Simera, I.; Seers, K.; Mockford, C.; Goodlad, S.; Altman, D.G.; Moher, D.; Barber, R.; Denegri, S.; et al. GRIPP2 Reporting Checklists: Tools to Improve Reporting of Patient and Public Involvement in Research. BMJ 2017, 358, j3453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PPI Ignite Network. Promoting Excellence and Inspiring Innovation. Available online: https://ppinetwork.ie/ (accessed on 17 January 2023).
- Dotto, L.; Kinalski, M.D.A.; Machado, P.S.; Pereira, G.K.R.; Sarkis-Onofre, R.; dos Santos, M.B.F. The Mass Production of Systematic Reviews about COVID-19: An Analysis of PROSPERO Records. J. Evid. Based Med. 2021, 14, 56–64. [Google Scholar] [CrossRef] [PubMed]
- McKenna, H. Perspectives: Patient and Public Involvement and Research Impact: A Reciprocal Relationship. J. Res. Nurs. 2015, 20, 723–728. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control Guide to Public Health Measures to Reduce the Impact of Influenza Pandemics in Europe—‘The ECDC Menu’. Available online: https://www.ecdc.europa.eu/en/publications-data/guide-public-health-measures-reduce-impact-influenza-pandemics-europe-ecdc-menu (accessed on 17 January 2023).
- World Health Organization. Tracking Public Health and Social Measures: Taxonomy and Glossary. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/phsm (accessed on 23 March 2022).
- Michie, S.; West, R. Behavioural, Environmental, Social, and Systems Interventions against Covid-19. BMJ 2020, 370, m2982. [Google Scholar] [CrossRef] [PubMed]
- Talic, S.; Shah, S.; Wild, H.; Gasevic, D.; Maharaj, A.; Ademi, Z.; Li, X.; Xu, W.; Mesa-Eguiagaray, I.; Rostron, J.; et al. Effectiveness of Public Health Measures in Reducing the Incidence of COVID-19, SARS-CoV-2 Transmission, and Covid-19 Mortality: Systematic Review and Meta-Analysis. BMJ 2021, 375, e068302. [Google Scholar] [CrossRef] [PubMed]
- Pizzo, E.; Doyle, C.; Matthews, R.; Barlow, J. Patient and Public Involvement: How Much Do We Spend and What Are the Benefits? Health Expect. 2015, 18, 1918–1926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adeyemi, I.; Sanders, C.; Ong, B.N.; Howells, K.; Quinlivan, L.; Gorman, L.; Giles, S.; Amp, M.; Monaghan, E.; Naseem, S.; et al. Challenges and Adaptations to Public Involvement with Marginalised Groups during the COVID-19 Pandemic: Commentary with Illustrative Case Studies in the Context of Patient Safety Research. Res. Involv. Engag. 2022, 8, 13. [Google Scholar] [CrossRef] [PubMed]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing Systematic Reviews: Methodological Development, Conduct and Reporting of an Umbrella Review Approach. JBI Evid. Implement. 2015, 13, 132–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aromataris, E.; Fernandez, R.; Godfrey, C.; Holly, C.; Khalil, H.; Tungpunkom, P. Chapter 10: Umbrella Reviews. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://jbi-global-wiki.refined.site/space/MANUAL (accessed on 8 March 2023).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fouladi, N.; Tchangalova, N.; Ajayi, D.; Bonilla, L.; Lovett, C.; Liggett, S.; Manukulasuriya, M.; Millwee, E.; Munoz, A.; Njonkou, C.; et al. COVID-19 Public Health Measures and Patient and Public Involvement (PPI) in Health and Social Care Research: An Umbrella Review Protocol. PROSPERO. 2022. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022307608 (accessed on 8 March 2023).
- Lockwood, C.; Munn, Z.; Porritt, K. Qualitative Research Synthesis: Methodological Guidance for Systematic Reviewers Utilizing Meta-Aggregation. Int. J. Evid. Based Healthc. 2015, 13, 179–187. [Google Scholar] [CrossRef] [PubMed]
- National Library of Medicine Search Strategy Used to Create the Pubmed Systematic Reviews Filter. Available online: https://www.nlm.nih.gov/bsd/pubmed_subsets/sysreviews_strategy.html (accessed on 6 February 2023).
- Puckett, J. Zotero: A Guide for Librarians, Researchers, and Educators; Association of College and Research Libraries: Chicago, IL, USA, 2011; ISBN 978-0-8389-8589-2. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan: A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adebisi, Y.A.; Rabe, A.; Lucero-Prisno III, D.E. Risk Communication and Community Engagement Strategies for COVID-19 in 13 African Countries. Health Promot. Perspect. 2021, 11, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, A.; Pasea, L.; Manohar, S.; Lai, A.G.; Hemingway, E.; Sofer, I.; Katsoulis, M.; Sood, H.; Morris, A.; Cake, C.; et al. ‘What Is the Risk to Me from COVID-19?’: Public Involvement in Providing Mortality Risk Information for People with ‘High-Risk’ Conditions for COVID-19 (OurRisk.CoV). Clin. Med. 2021, 21, e620–e628. [Google Scholar] [CrossRef] [PubMed]
- Ernawati, K.; Cantika, I.B.; Isaputri, R.R.; Andari, A.W.; Ramadhan, M.F.; Nathasia, S.K.; Rifqatussa’adah, R.; Hasibuan, H.S.; Astuti, L.T.M.; Ismail, Y. Community Knowledge, Attitudes and Behaviors in Prevention of COVID-19 Transmission: A Systematic Review. Int. J. Public Health Sci. 2021, 10, 16–26. [Google Scholar] [CrossRef]
- Mao, G.; Fernandes-Jesus, M.; Ntontis, E.; Drury, J. What Have We Learned about COVID-19 Volunteering in the UK? A Rapid Review of the Literature. BMC Public Health 2021, 21, 1470. [Google Scholar] [CrossRef] [PubMed]
- Pegollo, L.; Maggioni, E.; Gaeta, M.; Odone, A. Characteristics and Determinants of Population Acceptance of COVID-19 Digital Contact Tracing: A Systematic Review. Acta Biomed. 2021, 92, e2021444. [Google Scholar] [CrossRef] [PubMed]
- Raymond, C.B.; Ward, P.R. Community-Level Experiences, Understandings, and Responses to COVID-19 in Low- and Middle-Income Countries: A Systematic Review of Qualitative and Ethnographic Studies. Int. J. Environ. Res. Public Health 2021, 18, 12063. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Interventions/Phenomena of Interest | Author/Year | Number of Studies/Participants | Results/Findings | Heterogeneity |
|---|---|---|---|---|
| Risk Communication and Community Engagement (RCCE) Strategies | Adebisi et al., 2021 [23] | Participants from 13 African Countries | PPI measures consisted of in-depth conversations with stakeholders, written feedback, and social media responses. Distrust in the government, weak healthcare systems, widespread rumors and misinformation, the exclusion of some vulnerable groups, and resistance and inertia were challenges to implementing RCCE strategies in African countries. Based on the results, researchers recommend strengthening the strategic mapping of partners, investing in proper coordination structures, resources, training, improving public trust through effective leaderships, ensuring adequate planning, and strengthening the documentation and reporting of activities and experiences for RCCE in Africa. | N/A |
| COVID-19 Risk Prediction Tools | Banerjee et al., 2021 [24] | 53/29.1 million | PPI measures consisted of written feedback from patient and public panels, informal and structured written feedback from stakeholders, user and media feedback on prototype patient portals, and virtual focus groups. Research engagement results have identified a lack of public and patient engagement in COVID-19 risk tools to date and a lack of mortality risk information designs for patients with underlying conditions. Throughout the pandemic, a sustained patient, public interest, and engagement in the development of a risk information tool during and beyond the pandemic was demonstrated. The feasibility to create an online portal containing mortality information with PPI and other healthcare stakeholders was also considered. | N/A |
| Knowledge, Attitudes, and Behaviors of Communities for the Prevention of COVID-19 Transmission | Ernawati et al., 2021 [25] | 10 | PPI measures consisted of using community participation to collect data regarding socio-demographic features, knowledge attitudes, and behaviors. Sociodemographic features: older respondents had better attitudes and behaviors towards COVID-19. Women were more likely to perform infection control behavior. Higher-educated respondents had healthier behaviors and unemployed persons had the least healthy behaviors. Knowledge: Increased knowledge leads to increased adherence to public health measures the majority of the time. Increased knowledge led to optimism, limited access to health services, and information affects attitudes/motivation. Attitudes: Self efficacy, view of COVID-19, the government’s idea for handling the pandemic, and social stigma had the most effect on attitudes. Practices: The most utilized practices included washing hands with soap and water, social distancing/self-isolation, and wearing a mask. | High |
| Volunteering in the UK in the Context of COVID-19 | Mao et al., 2021 [26] | 27 | PPI measures consisted of surveys, interviews, and conversations with volunteers. Volunteer activities consisted of the delivery of essentials, social isolation, support, and supporting improved social determinants of health such as housing. Online volunteering was developed. The expansion of formal volunteering, social action volunteering, and neighborhood support were developed but many models lacked structure and leadership. Middle-aged adults comprised most of the volunteer workforce. A total of 95% of council leaders and chief executives found expanded volunteering to be significant or very significant to their COVID-19 response. | High |
| Digital Contact Tracing | Pegollo et al., 2021 [27] | 41/186,144 | PPI consists of user experiences of DCT apps. Accessibility, communication, privacy, cybersecurity, and self-efficacy translated to successful policies. | N/A |
| Government Mandated Restrictions in Relation to Social and Public Health Adaptive Measures | Raymond & Ward, 2021 [28] | 26 | PPI consist of intersectoral collaboration, building upon previous epidemic and outbreak experiences, and the establishment of health policy infrastructure, with a focus on community-level engagement. Under-resourced health systems, misinformation, and structural weaknesses contributed to emotional destabilization. Local and contextual strategies including traditional explanatory models and spiritual technologies created resilience. | N/A |
| Phenomena of Interest/Context | Author/Year | Synthesized Finding | Details of Strategies |
|---|---|---|---|
| Risk Communication and Community Engagement (RCCE) Strategies | Adebisi et al., 2021 [23] | The study aimed at identifying the risk communication and community engagement (RCCE) strategies in 13 African countries. The WHO interim guidance on COVID-19 RCCE, which focused on risk communication systems, coordination among internal personnel and partners, communication and engagement with the public, training, capacity building, and addressing infodemic. Although the African countries utilized support from the WHO. The RCCE response activities were not without challenges. Many of the challenges that were experienced included distrust in the government due to corruption practices, weak healthcare systems caused by limited resources, widespread rumors and misinformation, excluding the specific needs of vulnerable groups, as well as cultural, social, and religious resistance, and inertia. | PPI Measures: engagement with risk communication strategies such as creating operational teams and working groups, engaging with all levels of government, creating risk communication plans, and RCCE budgets. Identifying and establishing relationships with partner organizations and national health authorities to create RCCE coordination and operating strategies. Utilizing community engagement through community leaders and media to understand opinions and beliefs regarding RCCE. Communicating through traditional and non-traditional methods. Training the public on RCCE strategies. Using IT to address infodemic concerns. Face-to-Face: community health organizers, youth-led and women-led movements, home visits, engaging the community, and religious leaders. Media: posters, billboards, radio and television ads, podcasts, social media, WhatsApp Government: Daily press briefings, translation into local languages, contract tracing, hotlines, official websites |
| COVID-19 Risk Prediction Tools | Banerjee et al., 2021 [24] | The study analyzed mortality risk information for people with ‘high-risk’ conditions for COVID-19. Three themes were identified in the pre- and post prototype release. The three themes are as follows: the information needs of patients, the usability of the information, and shared decision making with healthcare professionals. The findings suggest that there is a lack of public and patient engagement when it comes to COVID-19 risk tools as well as a lack of mortality risk information that is designed for patients with underlying conditions. Another finding showed that there had been sustained patient and public interest and engagement when developing such information during and post-pandemic. The last finding demonstrated the feasibility and utility of one online portal used for mortality information, covering a wide range of conditions, which was informed by patients and the public, ultimately giving context for decision-making and allowing for discussions between health professionals, family members, and caretakers. The findings suggest that multiple stakeholders, methods, and ongoing patient and public involvement and engagement (PPIE) are prerequisites, perhaps requiring a dedicated organization, (such as the Institute for Health Metrics and Evaluation for the Global Burden of Disease Study). Doctors are required to provide ‘all material risks’ when consenting patients, underscoring the need to find new ways to generate and communicate risk information. Second, there is a role for charities, patient organizations, and patients to collaborate and articulate a framework for better risk information across disease silos. | PPI Measures: users assisted in the development and publication of the prototype portal as well as providing feedback for further improvements once the prototype patient portal was published. Informing prototype (March–May 2020) Information Needs: Data were not collected from the tool due to patient concerns about data use and privacy. Usability for Patients: Initial reservations around usability, requiring a further need for dialogue in order to make the tool more useful to patients and the public. Shared decision making: Interest in using mortality risk data in discussions with health professionals was expressed by patients, but there were concerns about how the information would link to COVID-19 advice, and the potential for unintended consequences where the risk could be low. Informing the subsequent development of the public-facing version (May 2020–November 2020) Information needs:
|
| Knowledge, Attitudes and Behaviors, of Communities for the Prevention of COVID-19 Transmission | Ernawati et al., 2021 [25] | Knowledge, attitude, and practice factors (KAP) were evaluated in community participation for the prevention of COVID-19 transmission. Knowledge of the COVID-19 pandemic, specifically on modes of transmission, common symptoms, and the prevention of transmission, was found to encourage the public’s participation in preventing transmission. Preventive behavior correlates with the knowledge and attitudes of each community, showing a positive relationship among the three aspects of KAP. Additionally, the results of a good KAP aspect can provide a direct output and, namely, a reduction in the incidence of COVID-19 in each country in a specific time and in the long term. | PPI Measures: data were collected from respondents in individual communities from each country. Findings and conclusions were generalized but also tabulated for specific communities. Knowledge affecting community participation in the prevention of COVID-19 transmission: initial introductory information about COVID-19, information about transmission, how to identify general symptoms, and how to prevent transmission. Attitudes affecting community participation in the prevention of COVID-19 transmission: attitudes describe the government’s view on handling COVID-19, along with individual views which include self-isolation, mask usage, and social distancing. Practices affecting community participation in the prevention of COVID-19 transmission: washing hands properly and appropriately, maintaining physical distance, social distancing, avoiding crowded places, mask usage, and self-isolation. |
| Volunteering in the UK in the Context of COVID-19 | Mao et al., 2021 [26] | Overall, the review suggests that there were diverse models of organization and coordination in COVID-19 volunteering and that community support groups adjusted their activities and scope of action to the perceived needs and challenges. Social networks and connections, local knowledge, and social trust were key dimensions associated with community organizing and volunteering. | PPI Measures: Volunteer profiles, models of a vertical or horizontal organization, volunteer focus, and perceptions and realities of challenges and successes were indicated through the use of qualitative research measures such as surveys, interviews, and conversations. Volunteering Activities: the delivery of essentials such as food and prescriptions, activities to provide support during social isolation, employment assistance, social benefits, mental health, domestic abuse, homelessness, and housing and eviction assistance. Ways to Connect: online activities, Facebook social clubs, youth-led web groups, zoom meetings, WhatsApp, Skype, google docs, and offline activities such as handing out leaflets. Volunteering Models: formal volunteering through already established organizations, social action volunteering through fundraising and donation campaigns, and neighborhood support or grassroot movements. Volunteers: a shift from the traditional elderly population to middle aged adults, primarily women, volunteers who had lower SES, attitudes that included compassion, and trust in others and the government Sustainability: established organizations had lengthy processes to certify new volunteers and often the excitement to volunteer would dissipate before the organizations could process applications, grassroot movements lacked leadership, successful models included giving volunteers the option to decline assignments, giving social recognition, trusting relationships with volunteers, access to funds, and community-led groups that had a positive relationship with the local government with a mutual give-and-take style oversight. |
| Digital Contact Tracing | Pegollo et al., 2021 [27] | Digital health technologies have the capacity to bring healthcare services to everyone, helping those more vulnerable to feel safe and meaningfully helped while also contributing to public health. | PPI Measures: user interactions, experiences, attitudes, and beliefs were measured by observing and communicating with users. Practicalities: knowledge of the app did not correlate with downloads, a willingness to download the app varied widely across countries, a lack of accessibility, and disproportionately affected vulnerable groups mainly due to SES, education, and the digital divide. Adoption: downloads ranged from 37.3% to 87% and refused or missed downloads ranged from 27.7% to 94.8% across countries, adherence and continued use of the app declined over time, and continued use of the app was more likely to occur amongst people who felt self-efficacy or if their use of the app kept them or their loved ones safe. Participants were more likely to adopt the app with a higher SES, if they lived in affluent neighborhoods, were more educated, had trust in authority, more internet use, more use of pandemic safety measures and coping skills, and if they were men. Effectiveness and Trust: privacy was often considered to be more important than the common social good; a lack of trust in the government prevented effectiveness, concerns about the rapid development of the app and cybersecurity, social media impacted the trust of users whether informed or not, poor communication from the government about the app and its purpose caused barriers to usage whereas governments who educated citizenry showed positive effects. |
| Government Mandated Restrictions in Relation to Social and Public Health Adaptive Measures | Raymond & Ward 2021 [28] | Innovations and adaptations, through the syntheses of traditional and biomedical discourses and practice, illustrated community resilience and provided models for successful engagement to improve public health outcomes. | PPI Measures: interacting with local leaders, developing a COVID-19 task force, community engagement in contact tracing, “social surveillance”, and volunteerism. Community Cohesion: the management and disbursement of funds/resources became a communal affair, promoting trust, and transparency, and providing much-needed economic relief to families. Adaptive Leadership: A patron-client theory was used to approach the way that local leaders were regarded during the pandemic. The researchers found that the village heads shaped public opinion and that perceptions of COVID-19 served as a consolidating center for volunteers and a conduit for information, and facilitated social assistance. |
| Author/Year | PPI Definition | Type of PHM | Approaches Used | Groups Included | Settings | Outcomes | Benefits/Gaps |
|---|---|---|---|---|---|---|---|
| Adebisi et al., 2021 [23] | Various forms of verbal and written communication | Risk communication and community engagement (RCCE) strategies, such as training and capacity building, risk communication systems, internal and partners’ coordination, community engagement, public communication, contending with uncertainties, addressing misperceptions, and managing misinformation. | The key categories of COVID-19 RCCE based on WHO interim guidance were risk communication systems, internal and partner coordination, community engagement, public communication, addressing infodemic, and training and capacity building. | Community influencers, community health workers and religious leaders, community spokespersons, health professionals, and community health workers. | Ethiopia, Ghana, Kenya, Algeria, Angola, Cote d’Ivoire, the Democratic Republic of the Congo, Mauritius, Nigeria, South Africa, Tanzania, Uganda, and Zambia. | RCCE Strategies to address COVID-19 pandemic in 13 African countries. | Benefits: Given the common RCCE approaches and interventions seen across the continent, it is clear that countries are learning from each other and from global health organizations to develop RCCE programs for COVID-19. Gaps: Challenges with response activities included distrust in the government, cultural, social, and religious resistance, and inertia, as well as widespread fake news and rumors, the exclusion of vulnerable populations, and longstanding issues of weak healthcare systems. |
| Banerjee et al., 2021 [24] | Including patients and the public in all phases of research development and implementation | Developing a mortality risk calculator, informed by patients and the public, for 87 underlying conditions in the COVID-19 context | Systematic review of published risk tools for the prognosis, provision, and patient testing of new mortality risk estimates for people with high-risk conditions, iterative PPI, and engagement with qualitative analysis. | Patients older than 30 years of age registered with a general practice between 1-1-97 and 1-1-17 with ≥1 year of follow-up data. | Population-based primary care electronic health records. | The study showed a lack of public and patient engagement in COVID-19 risk tools to date and a lack of mortality risk information designed for patients with underlying conditions. | Benefits: Throughout the pandemic, the study demonstrated sustained PPI interest and engagement in the development of risk information tools. The study showed the feasibility and utility of a single online portal for the mortality information of a wide range of conditions, informed by patients and the public. Gaps: Despite research engagement, the results identified a lack of public and patient engagement in COVID-19 risk tools to date and a lack of mortality risk information design for patients with underlying conditions. |
| Ernawati et al., 2021 [25] | Community participation and willingness to help with disease management activities in respective regions. | Community participation to raise awareness of social distancing and self-isolation. | Systematic review and meta-analysis to determine community knowledge, attitudes, and behavior in preventing the transmission of COVID-19. | Members of the community with varying demographics. | Global review (all regions) | The results of a good knowledge, attitude, and practice aspect can provide a direct output, namely a reduction in the incidence of COVID-19 in each country over a specific time and in the long term. | Benefits: Community knowledge determines how people will behave as it relates to the pandemic. |
| Mao et al., 2021 [26] | COVID-19 volunteering including both informal and formal volunteering. | Volunteering and community support to aid support self-isolation. | A rapid review of the literature to assess the impact of volunteering at national and local community levels. | Groups including community volunteers. | United Kingdom | The review showed diverse models of organization and coordination in COVID-19 volunteering and that community support groups adjusted their activities and scope of action to perceived needs and challenges. Social networks and connections, local knowledge, and social trust were key dimensions associated with community organizing and volunteering. | Benefits: Community support groups seem to adjust their activities and scope of action to the current needs and challenges. Gaps: Despite the efforts of a few official public institutions and councils, there has been limited community engagement and collaboration with volunteering groups and other community-based organizations. |
| Pegollo et al., 2021 [27] | Population acceptance and participation in the use of digital contact tracing | Uptake, usage, interaction, and general sentiment or perception of digital contact tracing. | Systematic review of studies reporting on DCT acceptance and indicators, such as knowledge of technology, a willingness to download the DCT app, and the accessibility of the technology. | No age or region-specific limitations were in place. | Global review (all regions). | Adherence and continued use of DCT app declined over time, except among certain groups (individuals who felt self-efficacy, those that felt app usage kept loved ones safe, and those with higher SES). | Benefits: Digital health technologies have the capacity to bring healthcare services to all, helping vulnerable populations feel safe and overall contributing to public health. Gaps: Late adopters are individuals that need the most protection but often lack the equipment and understanding of technology. |
| Raymond & Ward 2021 [28] | Interacting with local leaders, the development of a COVID-19 task force, community engagement in contact tracing, “social surveillance”, and volunteerism. | Government mandated restrictions on movements to reduce transmission rates in lower/middle income nations. | Systematic review to evaluate the context and construction of community responses, social and psychological effects, the impacts of social and mobility restrictions, health system challenges, and adaptive responses. | No age nor region-specific limitations were in place. | Low- and middle-income countries of the Global South. | Communities worldwide reacted in multiple and complex ways and were influenced by social ruptures, restrictions in social and physical mobility, and ever-looming uncertainties of infection, financial insecurity, stigma, and loss, communities worldwide reacted in multiple and complex ways. | Benefits: Innovations and adaptations, through the syntheses of traditional and biomedical discourses and practice, leading to community resilience and providing models for successful engagement to improve public health outcomes. Gaps: Widespread misinformation and fear of social renunciations resulted in noncooperation with pandemic regulations, aversions, and heightened isolation, allowing the spread of the virus. |
| Author/Year | Interventions/Phenomena of Interest | Types of Studies Included in the Synthesis | Synthesized Findings |
|---|---|---|---|
| Adebisi et al., 2021 [23] | Risk Communication and Community Engagement (RCCE) strategies | Peer reviewed articles, reports, newsletters, government documents. | The majority of African countries have implemented risk communication and community engagement (RCCE) strategies to decrease the prevalence of COVID-19. |
| Banerjee et al., 2021 [24] | COVID-19 risk prediction tools | Living systematic reviews | Even though the public has shown interest in the development of risk information tools, there has been a lack of public and patient involvement in the development of risk prediction tools. There is an urgent need to better understand the specific risk information that patients and the public want overall. |
| Ernawati et al., 2021 [25] | Knowledge, attitudes, and behaviors, of communities in the prevention of COVID-19 transmission. | Quantitative research, primary data, open access articles, peer-reviewed work. | Evaluation of society awareness around the knowledge, attitudes, practice (KAP) for the prevention of COVID-19 has been found to be an effective transmission prevention strategy. |
| Mao et al., 2021 [26] | Volunteering in the UK in the context of COVID-19. | Published peer-reviewed articles, reports, briefings, blog posts, newspaper articles, and online media. | Community engagement and adaptation to change during volunteering efforts were essential in the public’s response to COVID-19 in the UK. |
| Pegollo et al., 2021 [27] | Digital contact tracing | Cross-sectional, population-based controlled experiment, surveys, interviews, text analysis, readability, experiments, longitudinal, comparative mixed methods, app review analysis, app usability, hybrid, and prospective. | Digital health technologies may bring healthcare services to a large population, which can help individuals feel safe while helping contribute to public health. The acceptance of digital contact tracing (DCT) is mainly centered around knowledge, willingness/adherence, usefulness, accessibility, community empowerment, and the concerns of privacy. |
| Raymond & Ward 2021 [28] | Government mandated restrictions in relation to social and public health adaptive measures. | Empirical, qualitative, field-based, and/or participatory research | Misinformation and fear of being socially chastised resulted in pandemic sanctions, resistance, higher rates of isolation, and increased prevalence rates of the virus. Synthesizing traditional and scientific/medical discourse and practices allowed for innovations and adaptations to communities’ reactions to the pandemic, resulting in community strength and providing methods for successful interactions to improve public health outcomes. |
| COVID-19 Public Health Measures | PPI Approach and Mechanisms | Diversity of PPI Stakeholder Groups | Benefits of Efficacy of Using PPI Strategies |
|---|---|---|---|
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fouladi, N.; Tchangalova, N.; Ajayi, D.; Millwee, E.; Lovett, C.; Del Sordi, A.; Liggett, S.; De Silva, M.; Bonilla, L.; Nkwonta, A.; et al. COVID-19 Public Health Measures and Patient and Public Involvement in Health and Social Care Research: An Umbrella Review. Int. J. Environ. Res. Public Health 2023, 20, 4887. https://doi.org/10.3390/ijerph20064887
Fouladi N, Tchangalova N, Ajayi D, Millwee E, Lovett C, Del Sordi A, Liggett S, De Silva M, Bonilla L, Nkwonta A, et al. COVID-19 Public Health Measures and Patient and Public Involvement in Health and Social Care Research: An Umbrella Review. International Journal of Environmental Research and Public Health. 2023; 20(6):4887. https://doi.org/10.3390/ijerph20064887
Chicago/Turabian StyleFouladi, Negin, Nedelina Tchangalova, Damilola Ajayi, Elizabeth Millwee, Corinne Lovett, Alana Del Sordi, Samantha Liggett, Malki De Silva, Laura Bonilla, Angel Nkwonta, and et al. 2023. "COVID-19 Public Health Measures and Patient and Public Involvement in Health and Social Care Research: An Umbrella Review" International Journal of Environmental Research and Public Health 20, no. 6: 4887. https://doi.org/10.3390/ijerph20064887
APA StyleFouladi, N., Tchangalova, N., Ajayi, D., Millwee, E., Lovett, C., Del Sordi, A., Liggett, S., De Silva, M., Bonilla, L., Nkwonta, A., Ramnarine, L., Munoz, A., Frazer, K., & Kroll, T. (2023). COVID-19 Public Health Measures and Patient and Public Involvement in Health and Social Care Research: An Umbrella Review. International Journal of Environmental Research and Public Health, 20(6), 4887. https://doi.org/10.3390/ijerph20064887