1. Introduction
The number and frequency of disasters increased by a factor of five in the last 50 years [
1]. Disasters are defined as events that can cause human suffering and infrastructure damage [
2]. One aspect of human suffering following a disaster is the potential long-term health impacts that often disproportionately affect women and the most marginalized [
3]. From the 9/11 air particulates to wildfires to Zika to the Flint water crisis, health impacts endure after the immediate crisis [
4,
5]. The full extent of the long-term health impacts of COVID-19 is currently unknown, but the evidence is growing that COVID-19 can have long-term health consequences [
6]. Furthermore, disasters are inherently stressful events that are part of the typical chronology of the onset of chronic disease after a disaster [
7]. While we do not treat diabetes (DM) the same as we treat hypertension (HTN), the National Response Framework uses an all-hazards generalized approach to the disasters [
8]. Different health outcomes for different types of disasters would question the approach as it relates to healthcare.
This study addresses gaps in existing research related to new onset metabolic and anxiety disorders following disasters and identifies the impact of the disasters on persons living with these disorders. An emphasis on linking data to social determinants of health (SDOH) and Census data in areas that received federal disaster declarations is included. It was established that the percentage of individuals who live with metabolic and anxiety disorders increased steadily. Among the increased conditions, this study addresses HTN, DM, and anxiety [
9].
Like other public health emergencies, African Americans, Latinx, Native Americans, Alaska Natives, and those with low income are disproportionately impacted. An analysis of the Federal Emergency Management Agency (FEMA) National Risk Index Score indicated that U.S. indigenous people are at the greatest risk from natural hazards, including hurricanes, volcanic activity, avalanches, extreme cold, drought, flooding, wildfires, and ice storms. The analysis also showed that Black or African Americans have the lowest overall risk from natural disasters, but they have the highest risk of negative impacts based on expected annual loss, social vulnerability, and community resilience [
10,
11]. Following Hurricane Katrina, survivors who stayed in a shelter and had a chronic disease requiring medications were twice as likely to present with acute symptoms [
12]. Additionally, there is a “differential recognition of medical need as a function of ethnicity” [
13]. This raises the question, when linked with the impacts of HTN and DM, is the disaster impact even greater?
The number of people diagnosed with DM also grew from 6.4 million to 26.8 million from 1990 to 2018 [
14], with 80% of those diagnosed with DM visiting an emergency department (ED) [
15]. Rural patients had higher rates of ED visits than urban patients. Medicare and Medicaid patients were more likely to use EDs for DM-related care [
14]. Likewise, more than 40% of adults in rural and 29.4% in urban areas reported HTN, with a 17% higher rate of DM in rural areas. Following Hurricane Sandy, an increase in ER visits by persons with diabetes was found, with the greatest increase by non-Hispanic White individuals [
16]. Lee et al. found a statistically significant increase in both primary and secondary diagnosis of DM in ED visits in New York City in the weeks after Hurricane Sandy but did not find changes in the proportion of female, non-Hispanic Black Hispanic, privately or uninsured patients, but there was an increase in Medicaid patients [
17]. Most studies that examined chronic disease after disasters found an association with outcomes [
7,
18,
19,
20,
21].
It was documented that after 9/11, major earthquakes, and Hurricane Katrina, there was an increase in cardiovascular disease and deaths [
20]. Two separate review studies of post-disaster elevated BP and DM found that, in most cases, BP returns to normal within six months. However, those with DM were likelier to have sustained HTN [
7,
20]. Gohardehi et al. found only five U.S. studies that examined disaster survivors specific to HTN and DM, and all focused on 9/11 and Hurricane Katrina [
17]. The studies compared disaster survivors to the general population rather than longitudinal studies of individuals diagnosed with HTN or DM before and after a disaster. They consistently found a higher prevalence of HTN and DM among survivors of major disasters than in the general population.
Anxiety disorders are characterized by “unpleasant feelings of stress, uneasiness, tension, and worry [and] is either the predominate disturbance or is expected in confronting a dreaded object or situation or is resisting obsessions or compulsions” [
22]. The impact of natural disasters on the development of anxiety disorders was difficult to assess. Many studies used broad definitions of psychological stress rather than specific diagnoses [
23,
24] or included anxiety, depression, and PTSD [
25,
26]. Other researchers used large population and Census data for Bayesian modeling to compare mental health outcomes between regions that were impacted and those not impacted by disasters [
27,
28]. Other studies were reported to oversample people over 60 or required excessive anxiety for 6–9 months [
29]. As with HTN and DM, there was no longitudinal study specific to the diagnosis of anxiety before and after a disaster, rather an
a priori belief that because disasters are inherently stressful events, anxiety would rise.
A frequent concern for people with non-communicable diseases is difficulty obtaining prescribed medications in the aftermath of a disaster. This may be exacerbated by the just-in-time resupply of medications and individuals not having more than a week of medication before the insurance company will pay for a refill. Jimmez-Mangual found that 77% of people in their study of Hurricane Maria survivors reported problems with medications, and 47.7% reported difficulty getting to the pharmacy [
30]. In addition to problems with obtaining medications, there are also gender, age, ethnicity, and educational and socio-economic status factors that play a role in inequalities that may exacerbate the universal problem across all disaster types of maintaining medication for chronic conditions [
31].
Preliminary studies of mapping capabilities related to disaster risks indicated there is considerable publicly available data on environmental hazards and natural disasters, but a lack of knowledge of the risks and necessary response by healthcare providers [
32,
33,
34]. For example, Veenema et al. [
34] identified a full list of U.S. nuclear power sites, including nuclear power reactors and nuclear research and test reactors. [US Nuclear Regulatory Commission]. In that study, the 99 active nuclear power reactors were combined with the five research/test sites that generated the highest amount of power. The sites were layered in ArcGIS with nursing schools, and then, nursing schools were surveyed to determine their perceived risk and related training offered as part of the curriculum. The results showed 75.1% of respondents teach ≤1 h of content on radiation/nuclear care, with 11.5% saying the primary reason for this was a lack of qualified faculty. The faculty (18%) said they would teach it if there were content developed by experts. A total of 53% of respondents answered incorrectly when asked if they were within an emergency planning zone of a nuclear reactor [
34].
The United Nations Office on Disaster Risk Reduction (UNDRR) noted the increased risk of disaster resulting from climate change and the growing number of deaths and persons impacted by disasters. “Between 2000 and 2019, 510,837 deaths and 3.9 billion people were affected by 6681 climate-related disasters” [
35]. This may further burden the 43.5 million caregivers who provide care to an adult or child in the average year [
36]. Caregivers can be either family members or friends who assist a person with health-related task, medications, and medical appointments, usually without compensation [
36]. The goal of the research was threefold: (1) to determine the independent and joint impacts of federally declared disasters on the diagnosis and medication changes for a person with HTN, DM, and anxiety six months before and six months after a disaster, (2) link the findings with available FEMA and Census data, and (3) make recommendations for education and practice. Our central hypothesis is that the incidence of long-term metabolic and anxiety disorders following disasters are associated with region-specific conditions disasters and SDOH. This first stage of research involves hurricanes in Louisiana.
Aim 1. Determine the independent and joint impacts of federally declared disasters on metabolic and anxiety disorders 6 months after a disaster. The change will be evaluated to determine the impact of disasters on outcomes for patients with HTN, DM, and/or anxiety. We hypothesize, based on preliminary data, that disaster survivors will show an increased rate of metabolic and anxiety disorders 6 months after the disaster.
Aim 2. Determine the independent and joint impacts of federally declared disasters on the medications prescribed for metabolic and anxiety disorders 6 months after a disaster. The change will be evaluated to determine the impact of disasters on medications. Using the medications prescribed, we hypothesize that disaster survivors diagnosed with metabolic or anxiety disorders have more medications ordered than controls.
Aim 3. Examine regional (local) environmental hazard risk integrating hazard data and data about population vulnerabilities that would affect healthcare workers’ treatment approach. Begin to develop recommendations for provider and community education to mitigate potential disaster health-related risks.
2. Materials and Methods
2.1. Study Design
This longitudinal, population-based cohort study used electronic health records data reported in MarketScan® (Ann Arbor, MI, USA) from patients seen in zip codes that received a federal disaster declaration because of either Hurricane Gustave or Ike and attempts to answer the proposed research questions. MarketScan® was selected because it has patient-level longitudinal data that maintain the exact date of service. Because pre- and post-disaster data were being compared, the precise dates of service were essential. Additionally, because their data included the lifespan, there was not an overrepresentation of those over 60 years old, which usually occurs with Medicare data.
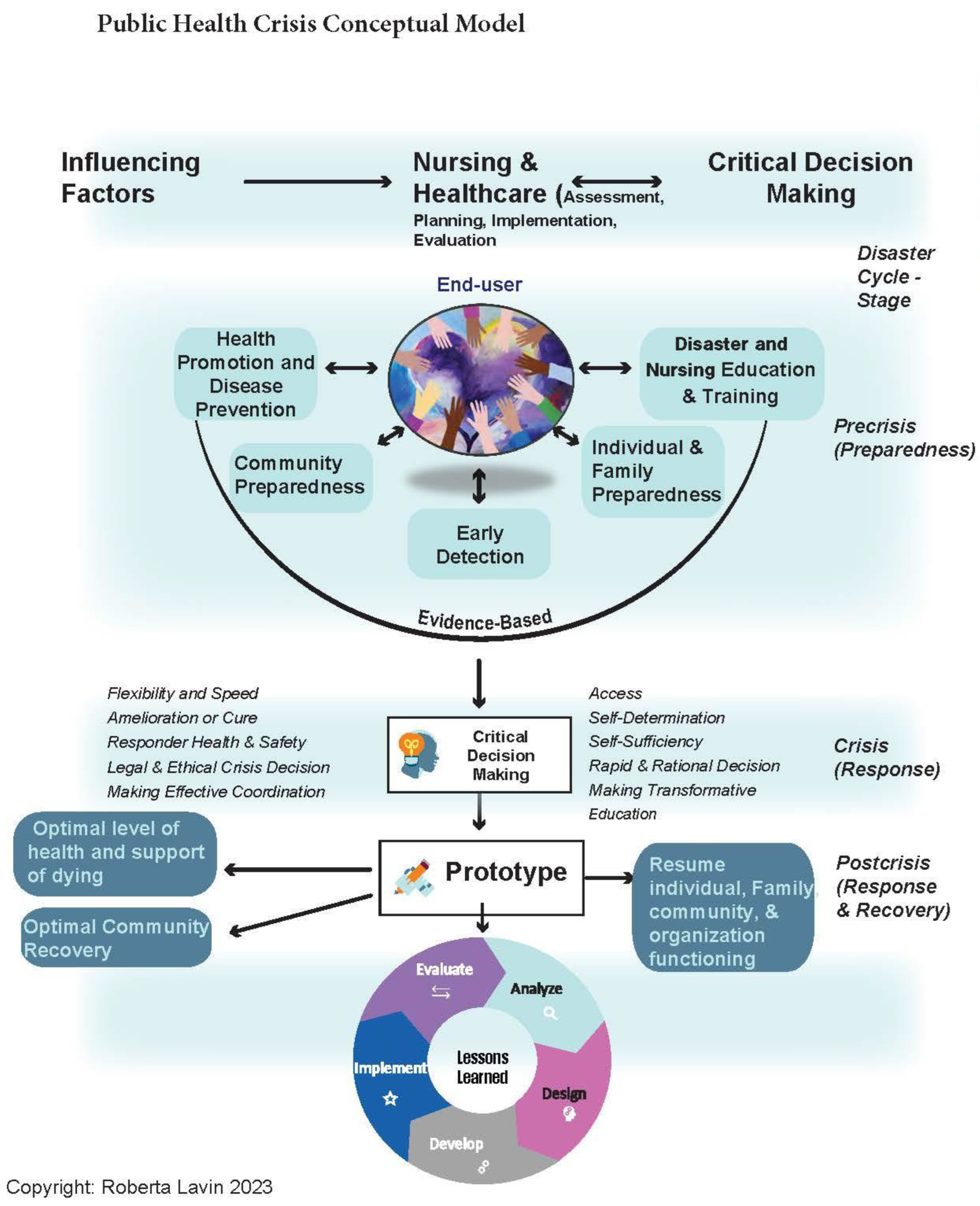
The conceptual framework of this study was based on the public health crisis conceptual model that was adapted from the crisis conceptual model and the social justice in nursing and public health preparedness human-centered structured analytical approach (
Figure 1) [
33,
37]. The approach was to take the “as is” data specific to the region of the declared disaster in the pre-crisis stage and compare it to the crisis and post-crisis stages. The data and analysis formed the evidence to propose a “to be” educational approach and tools to mitigate the impact on health presented in this article. The process of building an appropriate education component is a continuous cycle of design, development, implementation, evaluation, and analysis that is beyond the scope of this stage of the research.
2.2. Data Collection and Sample
In 2008, Hurricane Gustave (
Figure 2a) made landfall on 1 September 2008, in Louisiana and Hurricane Ike (
Figure 2b) made landfall in Texas on 8 September 2008, with the storm surge impacting Louisiana and causing significant damage. Publicly available FEMA data on federally declared disasters were used to identify areas impacted by the two disasters. Areas were identified by county as having received individual assistance, public assistance, or both.
MarketScan® data comes primarily from large employers; small employers may be underrepresented, and it does not include Medicare (except for those for retirees with employer-paid Medicare supplements). The study included individuals ≥18 who had a documented diagnosis of HTN, DM, or anxiety, with at least one visit to a primary care provider 6 months before and 6 months after a federally declared disaster, were treated in one of the declared regions in Louisiana, and whose healthcare data were captured in MarketScan®. As such, the sample was a convenience sample of those whose information is captured in the MarketScan® dataset.
Using the MarketScan® databases of de-identified patient-level health data, ICD-9 codes for HTN, DM, and anxiety were used to identify patients who were diagnosed with HTN, DM, or anxiety 6 months before and after the disasters. Working with the Center for Translational Science Center at the University of New Mexico, SAS Analytical Software was used to collect data from MarketScan®. Data were provided to the research team in Excel and imported into SPSS 26 for analysis.
There was a total of 13,681 patients who met the criteria of having a diagnosis of HTN, DM, or anxiety six months before (4 March 2008, to 31 August 2008) or after (14 September to 13 March 2009) Hurricanes Gustave and Ike, and who received care in an area that received a federal disaster designation.
2.3. Measures and Analysis
Noncommunicable chronic conditions (HTN, DM, anxiety) and medication data were analyzed, and trends were identified, looking for previously unidentified evidence that disaster can cause or exacerbate health conditions. Changes in disease-specific diagnosis and medication use rates were assessed between the pre-disaster and the post-disaster. This is significant because much of the policy related to disaster relief is specific to events caused by a disaster and does not cover events only exacerbated by a disaster.
Demographic characteristics of patients were compared using Pearson’s chi-squared test for categorical variables and a t-test or Mann–Whitney U test for continuous variables. A patient diagnosis was included if their visit occurred within six months before or six months after the disaster. Individual patients could have more than one diagnosis.
A binary logistic regression was conducted. Association between exposure to disaster (post-disaster) and diagnoses are shown as odds ratios (ORs) with 95% confidence intervals (CIs). No collinearity between variables was observed. The regression models showed an overall statistical significance of α < 0.05 and the goodness-of-fit of α > 0.05 (Hosmer–Lemeshow test). Therefore, the assumptions to conduct the analysis were met. All analyses were conducted using SPSS 26 (IBM, Armonk, NY, USA).
Study 22–215 was submitted to the University of New Mexico, Health Sciences Center IRB, and determined not to be human subjects research.
Census estimates for 2008 for Louisiana were used to estimate the total population and population characteristics. FEMA disaster declarations were mapped for the USA from 2012 to 2022 as an estimate of the disaster by region and type. All mapped data were shared on GitHub. Additionally, declared counties were identified and mapped for comparison with the 10-year average.
4. Discussion
The first aim explored metabolic and anxiety disorders 6 months after a disaster. The change was evaluated to determine the impact of disasters on outcomes for patients with HTN, DM, and/or anxiety after Hurricanes Gustave and Ike. The number of unique patients diagnosed with HTN, DM, and/or anxiety was similar before (49.5%) and after (50.5%) the disaster. Likewise, the patients’ characteristics were similar in the two periods. The only statistically significant association was the post-disaster diagnosis of hypertension, X
2 (1,
n = 19,328) = 3.985,
p = 0.04. The finding of a significant difference in the post-disaster diagnosis of HTN is inconsistent with the work of Kairo [
7] who found that at 6 months, the BP returned to normal except for those that also had DM but consistent with Gohardehi et al. [
20], who found a higher incidence of both HTN and DM from disaster survivors. While there were studies that showed increased ED visits for both primary and secondary diagnoses of DM, we did not find studies that showed an increase in the diagnosis of DM, which is consistent with our findings.
The second aim was to determine the independent and joint impacts of federally declared disasters on the medications prescribed for metabolic and anxiety disorders 6 months after a disaster. There was no statistically significant difference in medications before and after the disaster. Still, there was an increase in the number of medications started post-disaster for those diagnosed with HTN, DM, and anxiety. This is consistent with a new diagnosis and not unexpected. The study did not examine difficulties obtaining the medications as our data were related to the prescription.
The third aim examined regional (local) environmental hazard risks integrating hazard data and data about population vulnerabilities that would affect healthcare workers’ treatment approach. The study began a preliminary examination of existing FEMA and Census data to begin to identify interconnections with the post-disaster diagnosis of HTN, DM, and anxiety. The data clearly indicated that Louisiana is among the states most heavily impacted by hurricanes and with the most statewide impact. Because it is 48th in HTN and 44th in DM, their rate of HTN and DM was above the national average before the disaster. While the MarketScan
® data did not include information on race and ethnicity, the Census data demonstrated that Louisiana is a highly diverse state, with 32.8% of the population being Black or African American, 1.2% American Indian and Alaska Native, and 1.8% Asian. Because there is a “differential recognition of medical need as a function of ethnicity” [
13] it should be expected that healthcare needs following a disaster could vary based on population characteristics and environmental characteristics. Such characteristics should be considered in the precrisis phase planning and decision-making.
We are beginning to develop recommendations for provider education and practice and community education to mitigate potential disaster health-related risks. Clinicians should know the potential hazards in their community and be familiar with community resources to help patients access care, including medications. Recommendations for education and practice include the importance of identifying disaster and health hazards in a region and region specific characteristics. In addition to helping patients prepare for disasters, clinicians must also be alert to potential health hazards resulting from the disaster and aftereffects, e.g., mental health issues, inability to assess medications, and increased risk of non-communicable diseases. With the knowledge that there is a statistically significant association between the six months before and after a disaster and a diagnosis of hypertension, steps can be taken to educate clinicians to screen for hypertension after a disaster and monitor medication compliance, as well as other potential health issues. Additionally, because exposure to the disaster was significantly associated with increased odds of being diagnosed with HTN, DM, and anxiety after adjusting for age and sex, it is recommended that there be increased screening in the primary care setting for these conditions in areas impacted by a disaster.
The Public Health Crisis Conceptual Model (
Figure 1) provides a framework for a holistic focus on studying the impact of disasters. Rather than one temporal slice of the disaster, it examines the precrisis, crisis, and postcrisis phases leading to recommendations for education and practice: design, development, implementation, evaluation, and analysis that consider regional disaster and health hazard risks. Using the framework can help ensure local and national data are used, which then facilitates incorporating demographics and potential hazards of the community into provider and student education and training. Emergency planners can use the information in their processes for assessing risk and developing appropriate response and recovery plans. Faculty at health professions schools can incorporate information on the increased risk of HTN, DM, and anxiety into existing content and emphasize the need for added screening following a disaster.
6. Conclusions
This research has two important implications for science and practice. First, it was determined that there was a statically significant increase in the diagnosis of HTN but no statically significant changes in the diagnosis of DM, and anxiety after a disaster. It is important to note that there is a key distinction between statistical significance and clinical significance. Although there was no statistically significant increase in the diagnoses of diabetes, anxiety, or prescribed medications, the management of these chronic conditions and the ability to acquire the necessary medication remains critical to the health and well-being of patients, especially during a disaster when people may have been displaced from their homes. Until there is more evidence, it is recommended that increased screening for HTN occur in the 6 months after a disaster. Further studies to evaluate the clinical and statistical significance of different types of disasters in different geographic location on persons living with chronic conditions such as DM, HTN, and anxiety are needed. Further research is ongoing to assess five different types of disasters in five different geographic locations and whether medications were obtained by patients when prescribed.
Second, non-communicable chronic diseases and access to medications are essential considerations for clinicians, educators, and emergency planners in disaster-prone areas. This study illuminated the need to provide guidance and training for healthcare providers, health professions students, and emergency planners ensure that primary care needs, including non-communicable chronic diseases, are addressed in response plans, especially related to long-term health impacts of disasters. The findings related to medications identified a gap in the literature. Specifically, do patients prescribed new medications after a disaster have access to them?
Although the study specifically addressed the impact of natural disasters on HTN, DM, and anxiety, there may be policy implications for implementing primary care screening for metabolic and anxiety disorders following a disaster and changing policy related to what is considered “caused by” a disaster.


 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}