
Households’ Practices towards Rabies Prevention and Control in Rural Nepal


Abstract
:1. Introduction
2. Materials and Methods
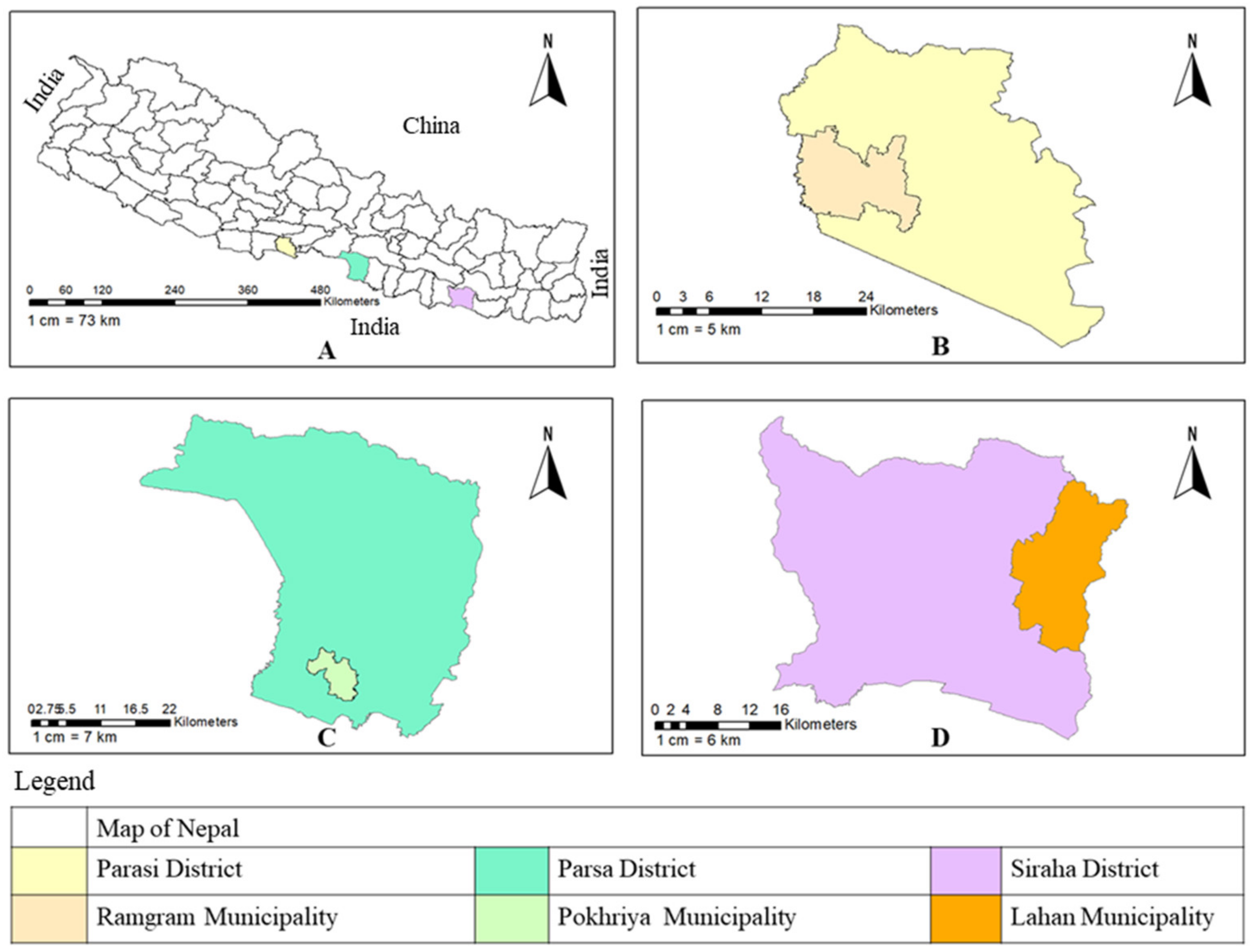
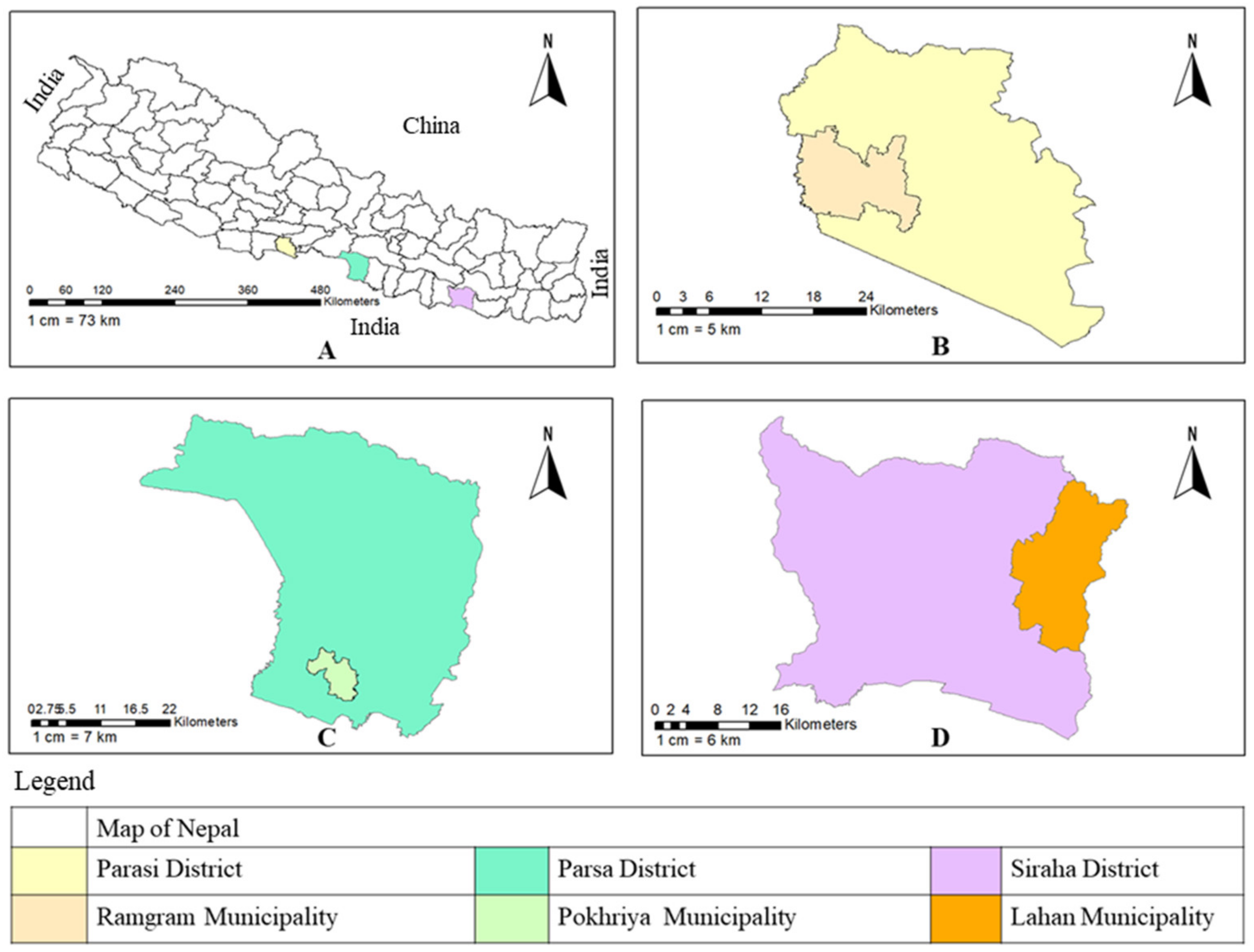
2.1. Study Design
2.2. Procedures and Data Collection Method
2.3. Measurement of Practices Score
2.4. Data Entry and Analysis
2.5. Ethics Statement
3. Results
3.1. Sociodemographic Characteristics of Respondents
3.2. Pet and Domestic Animal Ownership
3.3. Purpose of Owing Pets and Housing of Pets
4. Practices towards Rabies
4.1. Rabies Vaccination and Record Keeping
4.2. Treatment Seeking Behavior of Respondents
4.3. Actions Taken on Rabid Animals/Rabies Suspected Animals
4.4. Practice of Informing Authorities
4.5. Association between the Practice Category of Respondents and Sociodemographic Traits
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Rabies. Available online: https://www.who.int/news-room/fact-sheets/detail/rabies (accessed on 25 January 2022).
- Singh, R.; Singh, K.P.; Cherian, S.; Saminathan, M.; Kapoor, S.; Reddy, G.B.M.; Panda, S.; Dhama, K. Rabies—Epidemiology, Pathogenesis, Public Health Concerns and Advances in Diagnosis and Control: A Comprehensive Review. Vet. Q. 2017, 37, 212–251. [Google Scholar] [CrossRef] [Green Version]
- WHO. Zero by 30: The Global Strategic Plan to End Human Deaths from Dog-Mediated Rabies by 2030; WHO, OIE, FAO and GARC: Geneva, Switzerland, 2018; ISBN 0002-0729. [Google Scholar]
- FAO Towards a Rabies-Free World as Unparalleled Global Initiative Gets Underway. Available online: https://www.fao.org/news/story/en/item/1040394/icode/ (accessed on 23 January 2022).
- Wilde, H.; Lumlertdacha, B.; Meslin, F.X.; Ghai, S.; Hemachudha, T. Worldwide Rabies Deaths Prevention-A Focus on the Current Inadequacies in Postexposure Prophylaxis of Animal Bite Victims. Vaccine 2016, 34, 187–189. [Google Scholar] [CrossRef]
- FAO. The Food and Agriculture Organization and Rabies Prevention and Control; FAO: Rome, Italy, 2017. [Google Scholar]
- Annual Report Department of Health Services 2019/2020; Government of Nepal, Ministry of Health and Population: Kathmandu, Nepal, 2020.
- Acharya, K.P.; Adhikari, N.; Tariq, M. Fight against Rabies in Nepal: Immediate Need for Government Intervention. One Health 2020, 9, 100114. [Google Scholar] [CrossRef]
- EDCD. National Guideline Rabies Prophylaxis in Nepal (2019); EDCD: Kathmandu, Nepal, 2019.
- RVPL Introduction. Available online: http://www.rvpl.gov.np/ (accessed on 28 December 2022).
- Pantha, S.; Subedi, D.; Poudel, U.; Subedi, S.; Kaphle, K.; Dhakal, S. Review of Rabies in Nepal. One Health 2020, 10, 100155. [Google Scholar] [CrossRef] [PubMed]
- CDC Rabies around the World. Available online: https://www.cdc.gov/rabies/location/world/index.html (accessed on 23 January 2022).
- Mission Rabies Mission Rabies. Available online: http://www.missionrabies.com/ (accessed on 23 January 2022).
- Tiwari, H.K.; Vanak, A.T.; O’Dea, M.; Robertson, I.D. Knowledge, Attitudes and Practices (KAP) towards Rabies and Free-Roaming Dogs (FRD) in Shirsuphal Village in Western India: A Community Based Cross-Sectional Study. PLoS Negl. Trop. Dis. 2019, 13, e0007120. [Google Scholar] [CrossRef]
- Tenzin; Dhand, N.K.; Rai, B.D.; Changlo; Tenzin, S.; Tsheten, K.; Ugyen, P.; Singye, K.; Ward, M.P. Community-Based Study on Knowledge, Attitudes and Perception of Rabies in Gelephu, South-Central Bhutan. Int. Health 2012, 4, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Wolelaw, G.A.; Yalew, W.A.; Azene, A.G.; Wassie, G.T. Rabies Prevention Practices and Associated Factors among Household Heads in Bure Zuria District, North West Ethiopia. Sci. Rep. 2022, 12, 7361. [Google Scholar] [CrossRef] [PubMed]
- Akoglu, H. User’s Guide to Correlation Coefficients. Turkish J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Mapatse, M.; Sabeta, C.; Fafetine, J.; Abernethy, D. Knowledge, Attitudes, Practices (KAP) and Control of Rabies among Community Households and Health Practitioners at the Human-Wildlife Interface in Limpopo National Park, Massingir District, Mozambique. PLoS Negl. Trop. Dis. 2022, 16, e0010202. [Google Scholar] [CrossRef]
- Bihon, A.; Meresa, D.; Tesfaw, A. Rabies: Knowledge, Attitude and Practices in and Around South Gondar, North West Ethiopia. Diseases 2020, 8, 5. [Google Scholar] [CrossRef] [Green Version]
- Tenzin, T.; Ahmed, R.; Debnath, N.C.; Ahmed, G.; Yamage, M. Free-Roaming Dog Population Estimation and Status of the Dog Population Management and Rabies Control Program in Dhaka City, Bangladesh. PLOS Negl. Trop. Dis. 2015, 9, e0003784. [Google Scholar] [CrossRef] [Green Version]
- Rinzin, K.; Tenzin, T.; Robertson, I. Size and Demography Pattern of the Domestic Dog Population in Bhutan: Implications for Dog Population Management and Disease Control. Prev. Vet. Med. 2016, 126, 39–47. [Google Scholar] [CrossRef]
- CDC Rabies VIS. Available online: https://www.cdc.gov/vaccines/hcp/vis/vis-statements/rabies.html (accessed on 28 December 2022).
- Hagos, W.G.; Muchie, K.F.; Gebru, G.G.; Mezgebe, G.G.; Reda, K.A.; Dachew, B.A. Assessment of Knowledge, Attitude and Practice towards Rabies and Associated Factors among Household Heads in Mekelle City, Ethiopia. BMC Public Health 2020, 20, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widyastuti, M.D.W.; Bardosh, K.L.ᅟ; Sunandar; Basri, C.; Basuno, E.; Jatikusumah, A.; Arief, R.A.; Putra, A.A.G.; Rukmantara, A.; Estoepangestie, A.T.S.; et al. On Dogs, People, and a Rabies Epidemic: Results from a Sociocultural Study in Bali, Indonesia. Infect. Dis. Poverty 2015, 4, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabeta, T.; Deresa, B.; Tigre, W.; Ward, M.P.; Mor, S.M. Knowledge, Attitudes and Practices of Animal Bite Victims Attending an Anti-Rabies Health Center in Jimma Town, Ethiopia. PLoS Negl. Trop. Dis. 2015, 9, e0003867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sambo, M.; Lembo, T.; Cleaveland, S.; Ferguson, H.M.; Sikana, L.; Simon, C.; Urassa, H.; Hampson, K. Knowledge, Attitudes and Practices (KAP) about Rabies Prevention and Control: A Community Survey in Tanzania. PLoS Negl. Trop. Dis. 2014, 8, e3310. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, T.; Hussain, S.; Zia, U.U.R.; Rinchen, S.; Yasir, A.; Ahmed, S.; Khan, W.A.; Tahir, M.F.; Ricketson, R. Knowledge, Attitude and Practice (KAP) Survey of Canine Rabies in Khyber Pakhtunkhwa and Punjab Province of Pakistan. BMC Public Health 2020, 20, 1293. [Google Scholar] [CrossRef] [PubMed]
- Radostits, O.M.; Gay, C.; Hinchcliff, K.W.; Constable, P.D. Veterinary Medicine: A Textbook of the Diseases of Cattle, Horses, Sheep, Pigs and Goats; Elsevier Saunders: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Chaudhary, S.; Dangi, S. Awareness towards Rabies in the Residents of Kathmandu Metropolitan City, Nepal. J. Zoonotic Dis. 2021, 5, 1–8. [Google Scholar] [CrossRef]
- Ntampaka, P.; Nyaga, P.N.; Gathumbi, J.K.; Tukei, M.; Niragire, F. Knowledge, Attitudes and Practices Regarding Rabies and Its Control among Dog Owners in Kigali City, Rwanda. PLoS ONE 2019, 14, e0210044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, G.B.; Gilbert, A.; Monroe, B.; Blanton, J.; Ngam, S.N.; Recuenco, S.; Wallace, R. The Influence of Poverty and Rabies Knowledge on Healthcare Seeking Behaviors and Dog Ownership, Cameroon. PLoS ONE 2018, 13, e0197330. [Google Scholar] [CrossRef]
- Gebremeskel, A.K.; Tanga, B.M.; Getachew, A.; Eshetu, Y. Assessment of Public Knowledge, Attitude and Practices towards Rabies in the Community of Kombolcha, Southern Wollo, Amhara Reginal State, Ethiopia. J. Public Health Epidemiol. 2019, 11, 38–48. [Google Scholar] [CrossRef] [Green Version]
- Jemberu, W.T.; Molla, W.; Almaw, G.; Alemu, S. Incidence of Rabies in Humans and Domestic Animals and People’s Awareness in North Gondar Zone, Ethiopia. PLoS Negl. Trop. Dis. 2013, 7, e2216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mshelbwala, P.P.; Ogunkoya, A.B.; Maikai, B.V. Detection of Rabies Antigen in the Saliva and Brains of Apparently Healthy Dogs Slaughtered for Human Consumption and Its Public Health Implications in Abia State, Nigeria. ISRN Vet. Sci. 2013, 2013, 468043. [Google Scholar] [CrossRef] [PubMed]
- Digafe, R.T.; Kifelew, L.G.; Mechesso, A.F. Knowledge, Attitudes and Practices towards Rabies: Questionnaire Survey in Rural Household Heads of Gondar Zuria District, Ethiopia. BMC Res. Notes 2015, 8, 400. [Google Scholar] [CrossRef] [Green Version]
- Ali, A.; Yimer, E.; Sifer, D. A Study on Knowledge, Attitude and Practice of Rabies among Residents Abstract This Study Was Conducted in Addis Ababa during the Months of January and February, 2011 to Assess the Knowledge, Attitudes and Practices of the Communities on Rabies. A Cro. Ethiop. Vet. J. 2013, 17, 19–35. [Google Scholar] [CrossRef]
- Gebeyaw, S.; Teshome, D. Assessment of Knowledge, Attitude and Practice on Rabies in and Around Dessie City. Austin J. Vet. Sci. Anim. Husbandary 2016, 3, 1–5. [Google Scholar]
- Tamirat, K.; Alemayehu, L.; Mulualem, T. Community Perception towards Traditional Healers and Health Centers on Management of Dog Bites and Its Relation with Veterinary Public Health Activities. J. Vet. Sci. Anim. Husb. 2016, 4, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Pal, P.; Yawongsa, A.; Bhusal, T.N.; Bashyal, R.; Rukkwamsuk, T. Knowledge, Attitude, and Practice about Rabies Prevention and Control: A Community Survey in Nepal. Vet. World 2021, 14, 923–942. [Google Scholar] [CrossRef]
- Nejash, A.; Boru, M.; Jemal, J.; Wezir, A. Knowledge, Attitudes and Practices towards Rabies in Dedo District of Jimma Zone, Southwestern Ethiopia: A Community Based Cross-Sectional Study. Int. J. Med. Med. Sci. 2017, 9, 61–71. [Google Scholar] [CrossRef] [Green Version]
- Bouaddi, K.; Bitar, A.; Bouslikhane, M.; Ferssiwi, A.; Fitani, A.; Mshelbwala, P.P. Knowledge, Attitudes, and Practices Regarding Rabies in El Jadida Region, Morocco. Vet. Sci. 2020, 7, 29. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, S.; Chowdhury, S.; Haider, N.; Bhowmik, R.K.; Rana, M.S.; Prue Marma, A.S.; Hossain, M.B.; Debnath, N.C.; Ahmed, B.N. Awareness of Rabies and Response to Dog Bites in a Bangladesh Community. Vet. Med. Sci. 2016, 2, 161–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnamoorthy, Y.; Vijayageetha, M.; Sarkar, S. Awareness about Rabies among General Population and Treatment Seeking Behaviour Following Dog-Bite in Rural Puducherry: A Community Based Cross-Sectional Study. Int. J. Community Med. Public Health 2018, 5, 2557. [Google Scholar] [CrossRef] [Green Version]
- Rinchen, S.; Tenzin, T.T.; Hall, D.; Van Der Meer, F.; Sharma, B.; Dukpa, K.; Cork, S. A Community-Based Knowledge, Attitude, and Practice Survey on Rabies among Cattle Owners in Selected Areas of Bhutan. PLoS Negl. Trop. Dis. 2019, 13, e0007305. [Google Scholar] [CrossRef] [PubMed]
- Guadu, T.; Shite, A.; Chanie, M.; Bogale, B.; Fentahun, T. Assessment of Knowledge, Attitude and Practices about Rabies and Associated Factors: In the Case of Bahir Dar Town. Glob. Vet. 2014, 13, 348–354. [Google Scholar]

{kind=link}
| Socio-Demographics | Siraha, n = 102 | Parsa, n = 102 | Parasi, n = 104 | Total, n = 308 | |
|---|---|---|---|---|---|
| Gender | Male | 72 (70.6%) | 89 (87.3%) | 71 (68.3%) | 232 (75.3%) |
| Female | 30 (29.4%) | 13 (12.7%) | 33 (31.7%) | 76 (24.7%) | |
| Age | Lowest to 40 (≤40) | 46 (45.1%) | 45 (44.1%) | 41 (39.4%) | 132 (42.9%) |
| 41 to highest (≥41) | 56 (54.9%) | 57 (55.9%) | 63 (60.6%) | 176 (57.1%) | |
| Family Size | Mean ± SD | 6.74 ± 2.3 | 6.22 ± 2.4 | 6.18 ± 2.7 | 6.4 ± 2.5 |
| Household head gender | Male | 96 (94.1%) | 100 (98.0%) | 80 (76.9%) | 276 (89.6%) |
| Female | 6 (5.9%) | 2 (2.0%) | 24 (23.1%) | 32 (10.4%) | |
| Ethnicity | Madeshi | 58 (56.9%) | 64 (62.7%) | 37 (35.6%) | 159 (51.6%) |
| Aadibasi/Janajati | 20 (19.6%) | 17 (16.7%) | 17 (16.3%) | 54 (17.5%) | |
| Brahmin | 9 (8.8%) | 10 (9.8%) | 32 (30.8%) | 51 (16.6%) | |
| Chhetri | 6 (5.9%) | 8 (7.8%) | 10 (9.6%) | 24 (7.8%) | |
| Musalman | 9 (8.8%) | 3 (2.9%) | 8 (7.7%) | 20 (6.5%) | |
| Religion | Hinduism | 89 (87.3%) | 91 (89.2%) | 88 (84.6%) | 268 (87.0%) |
| Islam | 9 (8.8%) | 3 (2.9%) | 8 (7.7%) | 20 (6.5%) | |
| Buddhism | 4 (3.9%) | 8 (7.8%) | 7 (6.7%) | 19 (6.2%) | |
| Christianity | 0 | 0 | 1 (1.0%) | 1 (0.3%) | |
| Years of education | No formal education (0 years of education) | 25 (24.5%) | 15 (14.7%) | 22 (21.2%) | 62 (20.1%) |
| School level (1 to 10) | 45 (44.1%) | 72 (70.6%) | 49 (47.1%) | 166 (53.9%) | |
| College/University (11 to highest) | 32 (31.4%) | 15 (14.7%) | 33 (31.7%) | 80 (26.0%) | |
| Main family occupation | Self-employed/Own business | 46 (45.1%) | 31 (30.4%) | 35 (33.7%) | 112 (36.4%) |
| Agriculture | 36 (35.3%) | 35 (34.3%) | 27 (26.0%) | 98 (31.8%) | |
| Private Jobs | 8 (7.8%) | 17 (16.7%) | 12 (11.5%) | 37 (12.0%) | |
| Government Job/Public Services | 5 (4.9%) | 6 (5.9%) | 20 (19.2%) | 31 (10.1%) | |
| Others | 7 (6.9%) | 13 (12.7%) | 10 (9.6%) | 30 (9.7%) | |
| Monthly Household income of family | Lower (Rs. 10,000 to Rs. 25,000) | 61 (59.8%) | 74 (72.5%) | 41 (39.4%) | 176 (57.1%) |
| Middle/Upper (Rs. 25,001 to Rs. 60,000) | 41 (40.2%) | 28 (27.5%) | 63 (60.6%) | 132 (42.9%) | |
| Pet and/or Domestic Animals Owned | Siraha, n = 102 | Parsa, n = 102 | Parasi, n = 104 | Total, n = 308 |
|---|---|---|---|---|
| Dogs | 21 (20.6%) | 19 (18.6%) | 19 (18.3%) | 59 (19.2%) |
| Cats | 2 (2.0%) | 3 (2.9%) | 6 (5.8%) | 11 (3.6%) |
| Cattle | 22 (21.6%) | 12 (11.8%) | 4 (3.8%) | 38 (12.3%) |
| Buffalo | 35 (34.3%) | 38 (37.3%) | 17 (16.3%) | 90 (29.2%) |
| Goats | 63 (61.8%) | 56 (54.9%) | 19 (18.3%) | 138 (44.8%) |
| Poultry | 13 (12.7%) | 11 (10.8%) | 11 (10.6%) | 35 (11.4%) |
| Pigs | 3 (2.9%) | 4 (3.9%) | 1 (1.0%) | 8 (2.6%) |
| The Main Purpose of Owning a Dog/Cat | Siraha, n = 23 pets | Parsa, n = 22 pets | Parasi, n = 25 pets | Total, n = 70 |
|---|---|---|---|---|
| Guarding (n = 59, dogs) | 8/21 (38.1%) | 3/19 (15.8%) | 9/19 (47.4%) | 20/59 (33.9%) |
| Companionship | 8/23 (34.8%) | 9/22 (40.9%) | 3/25 (12%) | 20/70 (28.6%) |
| Family/children wish | 3/23 (13.0%) | 6/22 (27.3%) | 7/25 (28%) | 16/70 (22.9%) |
| Hobby | 4/23 (17.4%) | 1/22 (4.5%) | 5/25 (20%) | 10/70 (14.3%) |
| Other reasons | 0 | 3/22 (13.6%) | 1/25 (4.0%) | 4/70 (5.7%) |
| Housing for dog/cat | ||||
| Housed in cages | 6/23 (26.1%) | 4/22 (18.2%) | 10/25 (40.0%) | 20/70 (28.6%) |
| Tied outside the house (n = 59, dogs) | 9/21 (42.9%) | 9/19 (47.4%) | 2/19 (10.5%) | 20/59 (33.9%) |
| Free living inside the house | 2/23 (8.7%) | 5/22 (22.7%) | 5/25 (20.0%) | 12/70 (17.1%) |
| Free to roam around | 6/23 (26.1%) | 4/22 (18.2%) | 8/25 (32.0%) | 18/70 (25.7%) |
| Vaccination and Record Keeping | Siraha, n = 23 pets | Parsa, n = 22 pets | Parasi, n = 25 pets | Total, n = 70 |
|---|---|---|---|---|
| Do you vaccinate your dog/cat against rabies? (n = 70, respondents having pet animal) | ||||
| Yes | 20/23 (87.0%) | 19/22 (86.4%) | 19/25 (76.0%) | 58/70 (82.9%) |
| Do you keep record of rabies vaccination of your pet animals? (n = 58, respondents vaccinating their pets) | ||||
| Yes | 18/20 (90.0%) | 18/19 (94.7%) | 15/19 (78.9%) | 51/58 (87.9%) |
| Do you restrict your pet(s) to roam in the community? (n = 70, respondents having pet animal) | ||||
| Yes | 17/23 (73.9%) | 18/22 (81.8%) | 17/25 (68.0%) | 52/70 (74.3%) |
| Practices Related Questions | Siraha, n = 102 | Parsa, n = 102 | Parasi, n = 104 | Total, n = 308 |
|---|---|---|---|---|
| What immediate action(s) do you take after being bitten by rabid or rabies suspected animal? | ||||
| Washing with soap and water | 77 (75.5%) | 79 (77.5%) | 51 (49%) | 207 (67.2%) |
| Go to traditional healer | 41 (40.2%) | 11 (10.8%) | 4 (3.8%) | 56 (18.2%) |
| Visit hospital | 102 (100.0%) | 102 (100.0%) | 103 (99.0%) | 307 (99.7%) |
| Will you visit hospital if you are scratched by stray dog/cat? | ||||
| Yes | 70 (68.6%) | 91 (89.2%) | 94 (90.4%) | 255 (82.8%) |
| No | 32 (31.4%) | 11 (10.8%) | 10 (9.6%) | 53 (17.2%) |
| What action do you take on presumed rabid animal after it bites people? | ||||
| Tie/cage | 20 (19.6%) | 27 (26.5%) | 41 (39.4%) | 88 (28.6%) |
| Kill | 38 (37.3%) | 64 (62.7%) | 54 (51.9%) | 156 (50.6%) |
| Do nothing | 44 (43.1%) | 11 (10.8%) | 9 (8.7%) | 64 (20.8%) |
| Do you inform concerned authorities if you see someone bitten by a presumed rabid dog? | ||||
| Yes | 31 (30.4%) | 32 (31.4%) | 61 (58.7%) | 124 (40.3%) |
| No | 71 (69.6%) | 70 (68.6%) | 43 (41.3%) | 184 (59.7%) |
| Will you report to concerned authority if you find the behavior of dog/animal resembling to rabies? | ||||
| Yes | 31 (30.4%) | 32 (31.4%) | 61 (58.7%) | 124 (40.3%) |
| No | 71 (69.6%) | 70 (68.6%) | 43 (41.3%) | 184 (59.7%) |
| Socio-Demographics | Practice Category | X2 | df | p Value | ||
|---|---|---|---|---|---|---|
| Poor Practice | Good Practice | |||||
| Districts | Siraha | 74 | 28 | 22.562 | 2 | <0.001 *** |
| Parsa | 66 | 36 | ||||
| Parasi | 43 | 61 | ||||
| Gender | Male | 141 | 91 | 0.721 | 1 | 0.396 |
| Female | 42 | 34 | ||||
| Pet ownership | Yes | 32 | 38 | 7.052 | 1 | 0.008 ** |
| No | 151 | 87 | ||||
| Ethnicity | Brahmin | 23 | 28 | 11.409 | 4 | 0.022 * |
| Chhetri | 15 | 9 | ||||
| Adhibashi/Janajati | 27 | 27 | ||||
| Madhesi | 102 | 57 | ||||
| Mushalman | 16 | 4 | ||||
| Household head | Male | 170 | 106 | 5.299 | 1 | 0.022 * |
| Female | 13 | 19 | ||||
| Family size | Small (1 to 5) | 58 | 68 | 16.010 | 2 | <0.001 *** |
| Medium (6 to 10) | 109 | 51 | ||||
| Large (≥11) | 16 | 6 | ||||
| Religion | Hinduism | 154 | 114 | - | - | - |
| Buddhism | 13 | 6 | ||||
| Islam | 16 | 4 | ||||
| Christianity | 0 | 1 | ||||
| Main occupation | Agriculture | 65 | 33 | 17.448 | 4 | 0.002 ** |
| Government/Public Service | 8 | 23 | ||||
| Self/Own employed | 69 | 43 | ||||
| Private Jobs | 21 | 16 | ||||
| Others | 20 | 10 | ||||
| Level of education | No formal education (0 years of education) | 51 | 11 | 41.485 | 2 | <0.001 *** |
| School level (1 to 10) | 107 | 59 | ||||
| College/University (11 to highest) | 25 | 55 | ||||
| Household income | Lower (10,000 to 25,000) | 124 | 52 | 20.753 | 1 | <0.001 *** |
| Middle/Upper (25,001 to 60,000) | 59 | 73 | ||||
| Age group | Lowest to 40 (≤40) | 73 | 59 | 1.620 | 1 | 0.203 |
| 41 to highest (≥41) | 110 | 66 | ||||
| History of Animal bite (Dog/cat/fox) to you and your family | Yes | 50 | 36 | 0.081 | 1 | 0.777 |
| No | 133 | 89 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dhakal, A.; Ghimire, R.P.; Regmi, S.; Kaphle, K. Households’ Practices towards Rabies Prevention and Control in Rural Nepal. Int. J. Environ. Res. Public Health 2023, 20, 5427. https://doi.org/10.3390/ijerph20075427
Dhakal A, Ghimire RP, Regmi S, Kaphle K. Households’ Practices towards Rabies Prevention and Control in Rural Nepal. International Journal of Environmental Research and Public Health. 2023; 20(7):5427. https://doi.org/10.3390/ijerph20075427
Chicago/Turabian StyleDhakal, Alok, Ramjee P. Ghimire, Sujit Regmi, and Krishna Kaphle. 2023. "Households’ Practices towards Rabies Prevention and Control in Rural Nepal" International Journal of Environmental Research and Public Health 20, no. 7: 5427. https://doi.org/10.3390/ijerph20075427