

Neighborhood Physical and Social Environments and Social Inequalities in Health in Older Adolescents and Young Adults: A Scoping Review

Abstract
:1. Introduction
2. Objectives
3. Methods
3.1. Design
3.2. Data Collection
3.2.1. Search Strategy
3.2.2. Selection Criteria
3.2.3. Data Extraction and Synthesis
4. Results
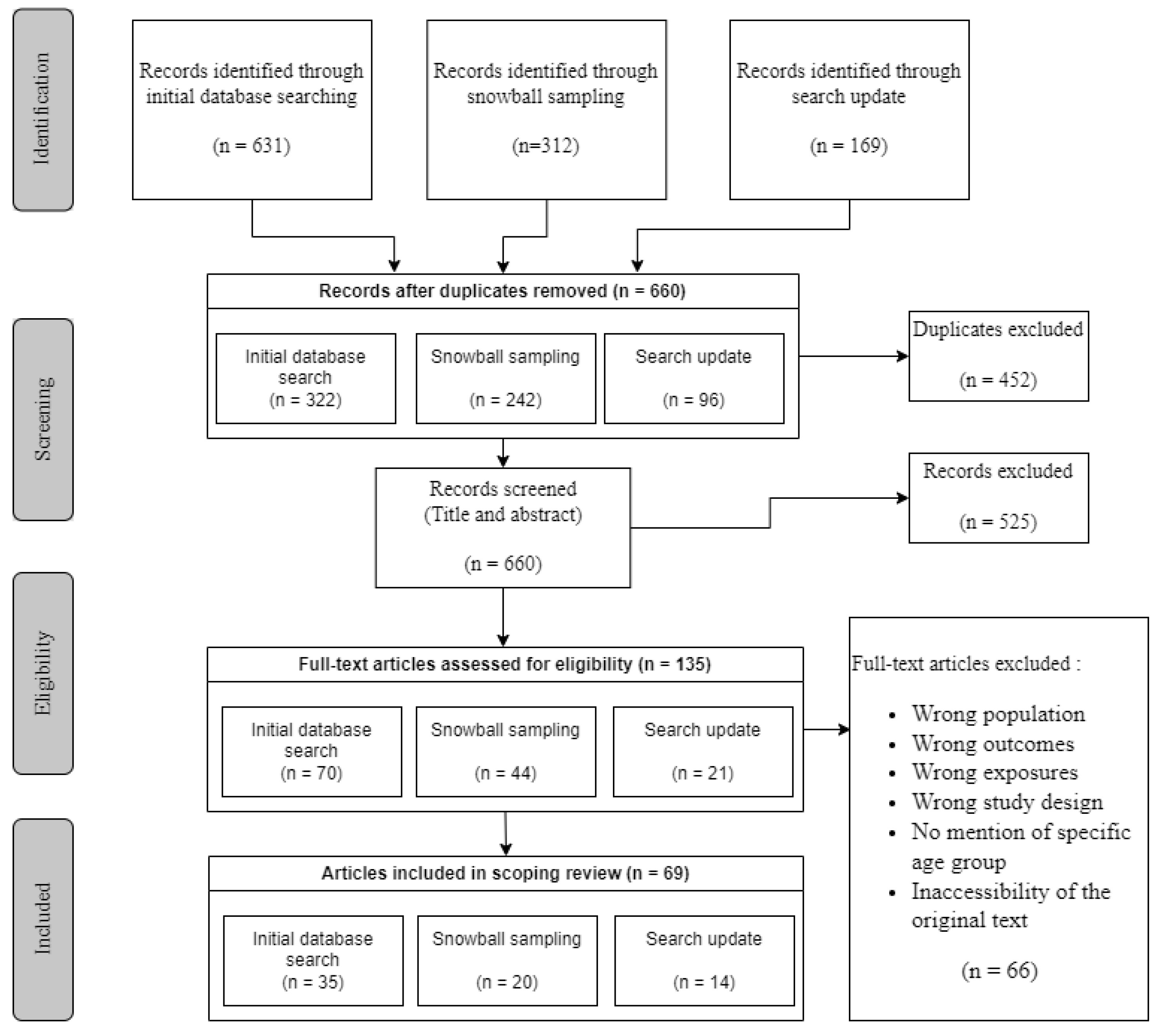
4.1. Literature Search Results
4.2. Study Characteristics
4.3. Outcome and Exposure Definition and Measurement
4.3.1. Health Outcomes
4.3.2. Environmental Exposures
4.4. Settings Definition and Inequalities Assessment
4.5. Associations Studied and Direction of Associations
4.6. Evidence on Social Inequalities in Health
5. Discussion
6. Conclusions
7. Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The Age of Adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Child, S.T.; Lawton, L. Loneliness and Social Isolation among Young and Late Middle-Age Adults: Associations with Personal Networks and Social Participation. Aging Ment. Health 2019, 23, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine and National Research Council. Improving the Health, Safety, and Well-Being of Young Adults: Workshop Summary; The National Academies Press: Washington, DC, USA, 2014. [Google Scholar]
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A Foundation for Future Health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Côté, J.; Bynner, J.M. Changes in the Transition to Adulthood in the UK and Canada: The Role of Structure and Agency in Emerging Adulthood. J. Youth Stud. 2008, 11, 251–268. [Google Scholar] [CrossRef]
- Patel, V.; Flisher, A.J.; Hetrick, S.; McGorry, P. Mental Health of Young People: A Global Public-Health Challenge. Lancet 2007, 369, 12. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Janz, K.F.; Letuchy, E.M.; Burns, T.L.; Levy, S.M. Developmental Trajectories of Physical Activity, Sports, and Television Viewing During Childhood to Young Adulthood: Iowa Bone Development Study. JAMA Pediatr. 2015, 169, 666–672. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, S.J.; Petrova, M. Prevention Science in Emerging Adulthood: A Field Coming of Age. Prev. Sci. 2019, 20, 305–309. [Google Scholar] [CrossRef] [Green Version]
- Braveman, P. Health Disparities and Health Equity: Concepts and Measurement. Annu. Rev. Public Health 2006, 27, 167–194. [Google Scholar] [CrossRef] [Green Version]
- Bell, S.; Lee, C. Emerging Adulthood and Patterns of Physical Activity among Young Australian Women. Int. J. Behav. Med. 2005, 12, 227–235. [Google Scholar] [CrossRef]
- Shareck, M.; Kestens, Y.; Vallée, J.; Datta, G.; Frohlich, K.L. The Added Value of Accounting for Activity Space When Examining the Association between Tobacco Retailer Availability and Smoking among Young Adults. Tob. Control 2016, 25, 406–412. [Google Scholar] [CrossRef] [Green Version]
- Shareck, M.; Datta, G.D.; Vallee, J.; Kestens, Y.; Frohlich, K.L. Is Smoking Cessation in Young Adults Associated with Tobacco Retailer Availability in Their Activity Space? Nicotine Tob. Res. 2020, 22, 512–521. [Google Scholar] [CrossRef] [PubMed]
- Sweeting, H.; Green, M.; Benzeval, M.; West, P. The Emergence of Health Inequalities in Early Adulthood: Evidence on Timing and Mechanisms from a West of Scotland Cohort. BMC Public Health 2016, 16, 41. [Google Scholar] [CrossRef] [Green Version]
- Harris, K.M.; Gordon-Larsen, P.; Chantala, K.; Udry, J.R. Longitudinal Trends in Race/Ethnic Disparities in Leading Health Indicators From Adolescence to Young Adulthood. Arch. Pediatr. Adolesc. Med. 2006, 160, 74–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Bank. World Development Report 2007: Development and the Next Generation; World Bank: Washington, DC, USA, 2006. [Google Scholar]
- Swisher, R.R.; Kuhl, D.C.; Chavez, J.M. Racial and Ethnic Differences in Neighborhood Attainments in the Transition to Adulthood. Soc. Forces Sci. Medium Soc. Study Interpret. 2013, 91, 1399–1428. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada. The Chief Public Health Officer’s Report on the State of Public Health in Canada. Designing Healthy Living; Public Health Agency of Canada: Ottawa, ON, Canada, 2017; p. 74.
- Marmot, M. Achieving Health Equity: From Root Causes to Fair Outcomes. Lancet 2007, 370, 1153–1163. [Google Scholar] [CrossRef] [PubMed]
- Diderichsen, F.; Hallqvist, J.; Whitehead, M. Differential Vulnerability and Susceptibility: How to Make Use of Recent Development in Our Understanding of Mediation and Interaction to Tackle Health Inequalities. Int. J. Epidemiol. 2019, 48, 268–274. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Mitchell, R.; Hartig, T. The Association between Green Space and Mental Health Varies across the Lifecourse. A Longitudinal Study. J. Epidemiol. Community Health 2014, 68, 578–583. [Google Scholar] [CrossRef]
- Bishop, A.S.; Walker, S.C.; Herting, J.R.; Hill, K.G. Neighborhoods and Health during the Transition to Adulthood: A Scoping Review. Health Place 2020, 63, 102336. [Google Scholar] [CrossRef]
- Vanaken, G.-J.; Danckaerts, M. Impact of Green Space Exposure on Children’s and Adolescents’ Mental Health: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 2668. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Mavoa, S.; Zhao, J.; Raphael, D.; Smith, M. The Association between Green Space and Adolescents’ Mental Well-Being: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 6640. [Google Scholar] [CrossRef]
- Curtis, S.; Pain, R.; Fuller, S.; Khatib, Y.; Rothon, C.; Stansfeld, S.A.; Daya, S. Neighbourhood Risk Factors for Common Mental Disorders among Young People Aged 10–20 Years: A Structured Review of Quantitative Research. Health Place 2013, 20, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Fleckney, P.; Bentley, R. The Urban Public Realm and Adolescent Mental Health and Wellbeing: A Systematic Review. Soc. Sci. Med. 2021, 284, 114242. [Google Scholar] [CrossRef] [PubMed]
- Arnett, J.J.; Žukauskienė, R.; Sugimura, K. The New Life Stage of Emerging Adulthood at Ages 18–29 Years: Implications for Mental Health. Lancet Psychiatry 2014, 1, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews(PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Shareck, M.; Aube, E.; Bouthot, J.; Paquette-Guay, A. Neighborhood Physical and Social Environments and Health Inequalities in Older Adolescents and Young Adults: A Scoping Review Protocol. Available online: https://osf.io/rkxtb/ (accessed on 23 February 2023).
- Kawachi, I.; Berkman, L.F. (Eds.) Neighborhoods and Health; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Soobader, M.-J.; Leclere, F.B. Going Upstream: Social Inequality and Children’s Health. Crit. Public Health 2000, 10, 217–232. [Google Scholar] [CrossRef]
- Wickrama, K.A.S.; Bryant, C.M. Community Context of Social Resources and Adolescent Mental Health. J. Marriage Fam. 2003, 65, 850–866. [Google Scholar] [CrossRef]
- Gutman, L.M.; Sameroff, A.J. Continuities in Depression from Adolescence to Young Adulthood: Contrasting Ecological Influences. Dev. Psychopathol. 2004, 16, 967–984. [Google Scholar] [CrossRef]
- Chen, E.; Paterson, L.Q. Neighborhood, Family, and Subjective Socioeconomic Status: How Do They Relate to Adolescent Health? Health Psychol. Off. J. Div. Health Psychol. Am. Psychol. Assoc. 2006, 25, 704–714. [Google Scholar] [CrossRef] [Green Version]
- Day, J.; Wen, M. Social Capital and Adolescent Mental Well-Being: The Role of Family, School and Neighborhood. Conf. Pap.—Am. Sociol. Assoc. 2007, 27, 362–378. [Google Scholar]
- Glendinning, A.; West, P. Young People’s Mental Health in Context: Comparing Life in the City and Small Communities in Siberia. Soc. Sci. Med. 2007, 65, 1180–1191. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, H.; Vostanis, P.; Goodman, R.; Ford, T. Children’s Perceptions of Neighbourhood Trustworthiness and Safety and Their Mental Health. J. Child Psychol. Psychiatry 2007, 48, 1208–1213. [Google Scholar] [CrossRef]
- Boyce, W.F.; Davies, D.; Gallupe, O.; Shelley, D. Adolescent Risk Taking, Neighborhood Social Capital, and Health. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2008, 43, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Cicognani, E.; Albanesi, C.; Zani, B. The Impact of Residential Context on Adolescents’ Subjective Well Being. J. Community Appl. Soc. Psychol. 2008, 18, 558–575. [Google Scholar] [CrossRef]
- Larson, K.; Russ, S.A.; Crall, J.J.; Halfon, N. Influence of Multiple Social Risks on Children’s Health. Pediatrics 2008, 121, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Larson, L.R.; Mullenbach, L.E.; Browning, M.H.E.M.; Rigolon, A.; Thomsen, J.; Metcalf, E.C.; Reigner, N.P.; Sharaievska, I.; McAnirlin, O.; D’Antonio, A.; et al. Greenspace and Park Use Associated with Less Emotional Distress among College Students in the United States during the COVID-19 Pandemic. Environ. Res. 2022, 204, 112367. [Google Scholar] [CrossRef]
- Maas, J.; Verheij, R.A.; de Vries, S.; Spreeuwenberg, P.; Schellevis, F.G.; Groenewegen, P.P. Morbidity Is Related to a Green Living Environment. J. Epidemiol. Community Health 2009, 63, 967–973. [Google Scholar] [CrossRef] [Green Version]
- Borges, C.M.; Campos, A.C.V.; Vargas, A.D.; Ferreira, E.F.; Kawachi, I. Social Capital and Self-Rated Health among Adolescents in Brazil: An Exploratory Study. BMC Res. Notes 2010, 3, 338. [Google Scholar] [CrossRef] [Green Version]
- Åslund, C.; Starrin, B.; Nilsson, K.W. Social Capital in Relation to Depression, Musculoskeletal Pain, and Psychosomatic Symptoms: A Cross-Sectional Study of a Large Population-Based Cohort of Swedish Adolescents. BMC Public Health 2010, 10, 715. [Google Scholar] [CrossRef] [Green Version]
- Wu, Q.; Xie, B.; Chou, C.-P.; Palmer, P.H.; Gallaher, P.E.; Johnson, C.A. Understanding the Effect of Social Capital on the Depression of Urban Chinese Adolescents: An Integrative Framework. Am. J. Community Psychol. 2010, 45, 1–16. [Google Scholar] [CrossRef]
- De Clercq, B.; Vyncke, V.; Hublet, A.; Elgar, F.J.; Ravens-Sieberer, U.; Currie, C.; Hooghe, M.; Ieven, A.; Maes, L. Social Capital and Social Inequality in Adolescents’ Health in 601 Flemish Communities: A Multilevel Analysis. Soc. Sci. Med. 2012, 74, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Aminzadeh, K.; Denny, S.; Utter, J.; Milfont, T.L.; Ameratunga, S.; Teevale, T.; Clark, T. Neighbourhood Social Capital and Adolescent Self-Reported Wellbeing in New Zealand: A Multilevel Analysis. Soc. Sci. Med. 2013, 84, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Huynh, Q.; Craig, W.; Janssen, I.; Pickett, W. Exposure to Public Natural Space as a Protective Factor for Emotional Well-Being among Young People in Canada. BMC Public Health 2013, 13, 407. [Google Scholar] [CrossRef] [Green Version]
- Delany-Brumsey, A.; Mays, V.M.; Cochran, S.D. Does Neighborhood Social Capital Buffer the Effects of Maternal Depression on Adolescent Behavior Problems? Am. J. Community Psychol. 2014, 53, 275–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ivert, A.-K.; Levander, M.T. Adolescents’ Perceptions of Neighbourhood Social Characteristics—Is There a Correlation with Mental Health? Child Indic. Res. 2014, 7, 177–192. [Google Scholar] [CrossRef]
- Marshall, B.D.; Astone, N.; Blum, R.W.; Jejeebhoy, S.; Delany-Moretlwe, S.; Brahmbhatt, H.; Olumide, A.; Wang, Z. Social Capital and Vulnerable Urban Youth in Five Global Cities. J. Adolesc. Health 2014, 55, S21–S30. [Google Scholar] [CrossRef] [Green Version]
- Mmari, K.; Blum, R.; Sonenstein, F.; Marshall, B.; Brahmbhatt, H.; Venables, E.; Delany-Moretlwe, S.; Lou, C.; Gao, E.; Acharya, R.; et al. Adolescents’ Perceptions of Health from Disadvantaged Urban Communities: Findings from the WAVE Study. Soc. Sci. Med. 2014, 104, 124–132. [Google Scholar] [CrossRef]
- Assari, S.; Smith, J.R.; Caldwell, C.H.; Zimmerman, M.A. Gender Differences in Longitudinal Links between Neighborhood Fear, Parental Support, and Depression among African American Emerging Adults. Societies 2015, 5, 151–170. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.-J.; Liechty, J.M. Longitudinal Associations Between Immigrant Ethnic Density, Neighborhood Processes, and Latino Immigrant Youth Depression. J. Immigr. Minor. Health 2015, 17, 983–991. [Google Scholar] [CrossRef]
- Novak, D.; Kawachi, I. Influence of Different Domains of Social Capital on Psychological Distress among Croatian High School Students. Int. J. Ment. Health Syst. 2015, 9, 18. [Google Scholar] [CrossRef] [Green Version]
- Novak, D.; Suzuki, E.; Kawachi, I. Are Family, Neighbourhood and School Social Capital Associated with Higher Self-Rated Health among Croatian High School Students? A Population-Based Study. BMJ Open 2015, 5, e007184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novak, D.; Milanovic, I.; Janic, S.R.; Štefan, L.; Kristicevic, T. The Influence of Social Capital Domains on Self-Rated Health among Serbian High-School Students? A School-Based Cross-Sectional Study. Montenegrin J. Sports Sci. Med. 2016, 5, 33–38. [Google Scholar]
- Saw, L.E.; Lim, F.K.S.; Carrasco, L.R. The Relationship between Natural Park Usage and Happiness Does Not Hold in a Tropical City-State. PLoS ONE 2015, 10, e0133781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hogan, M.J.; Leyden, K.M.; Conway, R.; Goldberg, A.; Walsh, D.; McKenna-Plumley, P.E. Happiness and Health across the Lifespan in Five Major Cities: The Impact of Place and Government Performance. Soc. Sci. Med. 2016, 162, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Pabayo, R.; Dunn, E.C.; Gilman, S.E.; Kawachi, I.; Molnar, B.E. Income Inequality within Urban Settings and Depressive Symptoms among Adolescents. J. Epidemiol. Community Health 2016, 70, 997–1003. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, S. Beyond Broken Windows: Youth Perspectives on Housing Abandonment and Its Impact on Individual and Community Well-Being. Child Indic. Res. 2016, 9, 581–607. [Google Scholar] [CrossRef]
- Vilhjalmsdottir, A.; Gardarsdottir, R.B.; Bernburg, J.G.; Sigfusdottir, I.D. Neighborhood Income Inequality, Social Capital and Emotional Distress among Adolescents: A Population-Based Study. J. Adolesc. 2016, 51, 92–102. [Google Scholar] [CrossRef]
- Dzhambov, A.; Tilov, B.; Markevych, I.; Dimitrova, D. Residential Road Traffic Noise and General Mental Health in Youth: The Role of Noise Annoyance, Neighborhood Restorative Quality, Physical Activity, and Social Cohesion as Potential Mediators. Environ. Int. 2017, 109, 1–9. [Google Scholar] [CrossRef]
- Dzhambov, A.; Hartig, T.; Markevych, I.; Tilov, B.; Dimitrova, D. Urban Residential Greenspace and Mental Health in Youth: Different Approaches to Testing Multiple Pathways Yield Different Conclusions. Environ. Res. 2018, 160, 47–59. [Google Scholar] [CrossRef]
- Dzhambov, A.M.; Markevych, I.; Hartig, T.; Tilov, B.; Arabadzhiev, Z.; Stoyanov, D.; Gatseva, P.; Dimitrova, D.D. Multiple Pathways Link Urban Green- and Bluespace to Mental Health in Young Adults. Environ. Res. 2018, 166, 223–233. [Google Scholar] [CrossRef]
- Dzhambov, A.M.; Markevych, I.; Tilov, B.; Arabadzhiev, Z.; Stoyanov, D.; Gatseva, P.; Dimitrova, D.D. Pathways Linking Residential Noise and Air Pollution to Mental Ill-Health in Young Adults. Environ. Res. 2018, 166, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Roe, J.J.; Aspinall, P.A.; Thompson, C.W. Coping with Stress in Deprived Urban Neighborhoods: What Is the Role of Green Space According to Life Stage? Front. Psychol. 2017, 8, 1760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnhart, S.; Gearhart, M.C.; Maguire-Jack, K. Perceptions of Collective Efficacy Among Single Mothers: Insights for Conceptualization and Measurement. J. Fam. Issues 2018, 39, 4019–4040. [Google Scholar] [CrossRef]
- Bezold, C.P.; Banay, R.F.; Coull, B.A.; Hart, J.E.; James, P.; Kubzansky, L.D.; Missmer, S.A.; Laden, F. The Association Between Natural Environments and Depressive Symptoms in Adolescents Living in the United States. J. Adolesc. Health 2018, 62, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Cole, A.; Ramirez, L.A.; Villodas, M.R.; Ben-David, S.; Munson, M.L. “I Want to Rise above It All”: Perceptions of the Neighborhood among Young Adults Living in Public Housing. Child. Youth Serv. Rev. 2019, 103, 63–69. [Google Scholar] [CrossRef]
- Colley, R.C.; Christidis, T.; Michaud, I.; Tjepkema, M.; Ross, N.A. An Examination of the Associations between Walkable Neighbourhoods and Obesity and Self-Rated Health in Canadians. Health Rep. 2019, 30, 14–24. [Google Scholar]
- Engemann, K.; Pedersen, C.B.; Arge, L.; Tsirogiannis, C.; Mortensen, P.B.; Svenning, J.-C. Residential Green Space in Childhood Is Associated with Lower Risk of Psychiatric Disorders from Adolescence into Adulthood. Proc. Natl. Acad. Sci. USA 2019, 116, 5188–5193. [Google Scholar] [CrossRef] [Green Version]
- Estrada-Martínez, L.M.; Lee, H.; Shapiro, E. Trajectories of Depressive Symptoms from Adolescence to Adulthood among Multiple Latino Subgroups. J. Latinx Psychol. 2019, 7, 322–338. [Google Scholar] [CrossRef]
- Kleszczewska, D.; Szkutnik, A.M.; Siedlecka, J.; Mazur, J. Physical Activity, Sedentary Behaviours and Duration of Sleep as Factors Affecting the Well-Being of Young People against the Background of Environmental Moderators. Int. J. Environ. Res. Public Health 2019, 16, 915. [Google Scholar] [CrossRef] [Green Version]
- Laurence, J. Community Disadvantage, Inequalities in Adolescent Subjective Well-Being, and Local Social Relations: The Role of Positive and Negative Social Interactions. Soc. Sci. Med. 2019, 237, 112442. [Google Scholar] [CrossRef]
- Lorenzo-Blanco, E.I.; Meca, A.; Unger, J.B.; Szapocznik, J.; Cano, M.Á.; Des Rosiers, S.E.; Schwartz, S.J. Cultural Stress, Emotional Well-Being, and Health Risk Behaviors among Recent Immigrant Latinx Families: The Moderating Role of Perceived Neighborhood Characteristics. J. Youth Adolesc. 2019, 48, 114–131. [Google Scholar] [CrossRef] [PubMed]
- Malinowska-Cieślik, M.; Mazur, J.; Nałęcz, H.; Małkowska-Szkutnik, A. Social and Behavioral Predictors of Adolescents’ Positive Attitude towards Life and Self. Int. J. Environ. Res. Public Health 2019, 16, 4404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavoa, S.; Lucassen, M.; Denny, S.; Utter, J.; Clark, T.; Smith, M. Natural Neighbourhood Environments and the Emotional Health of Urban New Zealand Adolescents. Landsc. Urban Plan. 2019, 191, 103638. [Google Scholar] [CrossRef]
- Rigg, K.K.; McNeish, R.; Schadrac, D.; Gonzalez, A.; Tran, Q. Community Needs of Minority Male Youth Living in Inner-City Chicago. Child. Youth Serv. Rev. 2019, 98, 284–289. [Google Scholar] [CrossRef]
- Srugo, S.A.; de Groh, M.; Jiang, Y.; Morrison, H.I.; Hamilton, H.A.; Villeneuve, P.J. Assessing the Impact of School-Based Greenness on Mental Health among Adolescent Students in Ontario, Canada. Int. J. Environ. Res. Public Health 2019, 16, 4364. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Meng, Y.-Y.; Lam, V.; Ponce, N. Green Space and Serious Psychological Distress among Adults and Teens: A Population-Based Study in California. Health Place 2019, 56, 184–190. [Google Scholar] [CrossRef]
- Franklin, M.; Yin, X.; McConnell, R.; Fruin, S. Association of the Built Environment With Childhood Psychosocial Stress. JAMA Netw. Open 2020, 3, e2017634. [Google Scholar] [CrossRef] [PubMed]
- Oluwaseyi, S.D.; Simo Fotso, A. The Effect of Family and Neighbourhood Social Capital on Youth Mental Health in South Africa. J. Adolesc. 2020, 83, 22–26. [Google Scholar]
- Poulain, T.; Sobek, C.; Ludwig, J.; Igel, U.; Grande, G.; Ott, V.; Kiess, W.; Körner, A.; Vogel, M. Associations of Green Spaces and Streets in the Living Environment with Outdoor Activity, Media Use, Overweight/Obesity and Emotional Wellbeing in Children and Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 6321. [Google Scholar] [CrossRef]
- Benninger, E.; Schmidt-Sane, M.; Spilsbury, J.C. Conceptualizing Social Determinants of Neighborhood Health through a Youth Lens. Child Indic. Res. 2021, 14, 2393–2416. [Google Scholar] [CrossRef]
- Currier, D.; Patton, G.; Sanci, L.; Sahabandu, S.; Spittal, M.; English, D.; Milner, A.; Pirkis, J. Socioeconomic Disadvantage, Mental Health and Substance Use in Young Men in Emerging Adulthood. Behav. Med. 2021, 47, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Oswald, T.K.; Rumbold, A.R.; Kedzior, S.G.E.; Kohler, M.; Moore, V.M. Mental Health of Young Australians during the COVID-19 Pandemic: Exploring the Roles of Employment Precarity, Screen Time, and Contact with Nature. Int. J. Environ. Res. Public Health 2021, 18, 5630. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Yang, Z.; Chen, Z.; Guo, M.; Guo, P. Optimizing Urban Forest Landscape for Better Perceptions of Positive Emotions. Forests 2021, 12, 1691. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhao, J.; Mavoa, S.; Erika, I.; Clark, T.C.; Crengle, S.; Smith, M. Urban Green Space and Mental Well-Being of Aotearoa New Zealand Adolescents: A Path Analysis. Wellbeing Space Soc. 2022, 3, 100085. [Google Scholar] [CrossRef]
- Hirota, T.; Paksarian, D.; He, J.-P.; Inoue, S.; Stapp, E.K.; Van Meter, A.; Merikangas, K.R. Associations of Social Capital with Mental Disorder Prevalence, Severity, and Comorbidity among U.S. Adolescents. J. Clin. Child Adolesc. Psychol. 2022, 51, 970–981. [Google Scholar] [CrossRef] [PubMed]
- Bloemsma, L.D.; Wijga, A.H.; Klompmaker, J.O.; Hoek, G.; Janssen, N.A.H.; Lebret, E.; Brunekreef, B.; Gehring, U. Green Space, Air Pollution, Traffic Noise and Mental Wellbeing throughout Adolescence: Findings from the PIAMA Study. Environ. Int. 2022, 163, 107197. [Google Scholar] [CrossRef] [PubMed]
- Carrillo-Alvarez, E.; Andrés, A.; Riera-Romaní, J.; Novak, D.; Rodriguez-Monforte, M.; Costa-Tutusaus, L.; Guerra-Balic, M. The Association between Social Capital Indicators and Psychological Distress in Catalan Adolescents. Front. Psychol. 2022, 13, 4886. [Google Scholar] [CrossRef]
- Hunduma, G.; Deyessa, N.; Dessie, Y.; Geda, B.; Yadeta, T.A. High Social Capital Is Associated with Decreased Mental Health Problem Among In-School Adolescents in Eastern Ethiopia: A Cross-Sectional Study. Psychol. Res. Behav. Manag. 2022, 15, 503–516. [Google Scholar] [CrossRef]
- Sadler, R.C.; Felton, J.W.; Rabinowitz, J.A.; Powell, T.W.; Latimore, A.; Tandon, D. Inequitable Housing Practices and Youth Internalizing Symptoms: Mediation Via Perceptions of Neighborhood Cohesion. Urban Plan. 2022, 7, 153–166. [Google Scholar] [CrossRef]
- Shen, Y. Race/Ethnicity, Built Environment in Neighborhood, and Children’s Mental Health in the US. Int. J. Environ. Health Res. 2022, 32, 277–291. [Google Scholar] [CrossRef]
- Stahlmann, K.; Mena, E.; Kuhnert, R.; Conrad, A.; Bolte, G. Social Inequalities in the Association between Social Infrastructure and Mental Health: An Observational Cross-Sectional Analysis of Children and Adolescents in Germany. Int. J. Environ. Res. Public Health 2022, 19, 6760. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.; Fisher, H.L.; Dewa, L.H.; Hussain, T.; Kabba, Z.; Toledano, M.B. Adolescents’ Thoughts and Feelings about the Local and Global Environment: A Qualitative Interview Study. Child Adolesc. Ment. Health 2022, 27, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Zewdie, H.Y.; Whetten, K.; Dubie, M.E.; Kenea, B.; Bekele, T.; Temesgen, C.; Molla, W.; Puffer, E.S.; Ostermann, J.; Hobbie, A.M.; et al. The Association between Urban Greenspace and Psychological Health among Young Adults in Addis Ababa, Ethiopia. Environ. Res. 2022, 215, 114258. [Google Scholar] [CrossRef] [PubMed]
- Shareck, M.; Dassa, C.; Frohlich, K.L. Improving the Measurement of Neighbourhood Characteristics through Systematic Observation: Inequalities in Smoking as a Case Study. Health Place 2012, 18, 671–682. [Google Scholar] [CrossRef] [Green Version]
- Yakubovich, A.R.; Heron, J.; Humphreys, D.K. How Do Perceived and Objective Measures of Neighbourhood Disadvantage Vary over Time? Results from a Prospective-Longitudinal Study in the UK with Implications for Longitudinal Research on Neighbourhood Effects on Health. PLoS ONE 2020, 15, e0231779. [Google Scholar] [CrossRef] [Green Version]
- Diderichsen, F.; Evans, T.; Whitehead, M. The Social Basis of Disparities in Health. Challenging Inequities Health Ethics Action 2001, 1, 12–23. [Google Scholar]
- Committee on Improving the Health, Safety, and Well-Being of Young Adults; Board on Children, Youth, and Families; Institute of Medicine; National Research Council. Investing in the Health and Well-Being of Young Adults; Bonnie, R.J., Stroud, C., Breiner, H., Eds.; National Academies Press: Washington, DC, USA, 2015. [Google Scholar]
- Mehdipanah, R.; Manzano, A.; Borrell, C.; Malmusi, D.; Rodriguez-Sanz, M.; Greenhalgh, J.; Muntaner, C.; Pawson, R. Exploring Complex Causal Pathways between Urban Renewal, Health and Health Inequality Using a Theory-Driven Realist Approach. Soc. Sci. Med. 2015, 124, 266–274. [Google Scholar] [CrossRef]
- Anguelovski, I.; Brand, A.L.; Connolly, J.J.T.; Corbera, E.; Kotsila, P.; Steil, J.; Garcia-Lamarca, M.; Triguero-Mas, M.; Cole, H.; Baró, F.; et al. Expanding the Boundaries of Justice in Urban Greening Scholarship: Toward an Emancipatory, Antisubordination, Intersectional, and Relational Approach. Ann. Am. Assoc. Geogr. 2020, 110, 1743–1769. [Google Scholar] [CrossRef]
- Burke, J.; O’Campo, P.; Salmon, C.; Walker, R. Pathways Connecting Neighborhood Influences and Mental Well-Being: Socioeconomic Position and Gender Differences. Soc. Sci. Med. 2009, 68, 1294–1304. [Google Scholar] [CrossRef]
- Rodriguez-Loureiro, L.; Casas, L.; Bauwelinck, M.; Lefebvre, W.; Vanpoucke, C.; Vanroelen, C.; Gadeyne, S. Social Inequalities in the Associations between Urban Green Spaces, Self-Perceived Health and Mortality in Brussels: Results from a Census-Based Cohort Study. Health Place 2021, 70, 102603. [Google Scholar] [CrossRef]
- Skelton, T. Young People’s Urban Im/Mobilities: Relationality and Identity Formation. Urban Stud. 2013, 50, 467–483. [Google Scholar] [CrossRef]
- Morency, C.; Paez, A.; Roorda, M.J.; Mercado, R.; Farber, S. Distance Traveled in Three Canadian Cities: Spatial Analysis from the Perspective of Vulnerable Population Segments. J. Transp. Geogr. 2011, 19, 39–50. [Google Scholar] [CrossRef]
- Shareck, M.; Kestens, Y.; Frohlich, K.L. Considering daily mobility for a more comprehensive understanding of contextual effects on social inequalities in health: A conceptual proposal. Health Place 2014, 29, 154–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shareck, M.; Kestens, Y.; Frohlich, K.L. Moving beyond the Residential Neighborhood to Explore Social Inequalities in Exposure to Area-Level Disadvantage: Results from the Interdisciplinary Study on Inequalities in Smoking. Soc. Sci. Med. 2014, 108, 106–114. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n (%) | ||||
|---|---|---|---|---|
| Approach | Quantitative | 62 (89.9) | ||
| Qualitative | 5 (7.2) | |||
| Mixed | 2 (2.9) | |||
| Study location a | North America | 31 (44.9) | ||
| Europe | 26 (37.7) | |||
| Other | 15 (21.7) | |||
| Design | Cross-sectional | 59 (85.5) | ||
| Longitudinal | 10 (14.5) | |||
| Recruitment | Population-based | 35 (50.7) | ||
| School-based | 30 (43.5) | |||
| Other | 4 (5.8) | |||
| Health outcomes | Subjective | Mental health (e.g., stress, psychological/emotional distress, self-esteem) | 32 (46.4) | |
| Depression and depressive symptoms (e.g., suicidal ideations and/or attempts) | 17 (24.6) | |||
| Well-being (e.g., general satisfaction with life, self-efficacy, happiness, emotional response (happy vs. sad), flourishing) | 18 (26.1) | |||
| Emotional problems | 3 (4.3) | |||
| Behavioral problems (e.g., alcohol and drugs hazardous use) | 4 (5.8) | |||
| General health | 15 (21.7) | |||
| Objective | Mental health (e.g., psychiatric disorders) | 2 (2.9) | ||
| Well-being (e.g., emotional response) | 1 (1.4) | |||
| General health (e.g., morbidity, physiological measures: BMI, cortisol, etc.) | 3 (4.3) | |||
| Environmental exposures | Subjective | Neighborhood social capital (e.g., neighborhood cohesiveness, sense of community, social trust, collective socialization, collective efficacy, social cohesion, social support, social interaction, social control) | 33 (47.8) | |
| Natural and built environment (e.g., use, distance, quality, access, motivation to use, housing abandonment perception and built environment quality) | 13 (18.8) | |||
| Neighborhood safety (e.g., violence, crime, safety, disorder, problems, danger, fear) | 15 (21.7) | |||
| Neighborhood socioeconomic status (e.g., perceived neighborhood socioeconomic status). | 2 (2.9) | |||
| Neighborhood satisfaction | 2 (2.9) | |||
| Residential stability | 1 (1.4) | |||
| Objective | Natural and built environment (e.g., greenspace, greenness, blue space, natural space, urbanicity, public natural space, intersection density, housing abandonment) | 21 (30.4) | ||
| Neighborhood socioeconomic status (e.g., income inequality, economic deprivation, disadvantage, average income, poverty) | 14 (20.3) | |||
| Residential stability | 1 (1.4) | |||
| Immigrant density/ethnic heterogeneity | 1 (1.4) | |||
| Inequitable housing practices | 1 (1.4) | |||
| Pollution (e.g., air and noise pollution) | 5 (7.2) | |||
| Setting within which exposures were measured | Residential | 66 (95.7) | ||
| School | 2 (2.9) | |||
| Other | 1 (1.4) | |||
| Area definition | Self-defined | 32 (46.4) | ||
| Administrative unit (e.g., census block or tract, zip code area) | 25 (36.2) | |||
| Buffer (e.g., circular, road-network) | 12 (17.4) | |||
| Social inequality assessment | Yes b | Sex/gender | 23/31 | 31 (44.9) |
| Socioeconomic status (income, education, affluence) | 8/31 | |||
| Ethnicity | 6/31 | |||
| Other (immigrant status, urbanicity) | 4/31 | |||
| No | 38 (55.1) | |||
| Exposure | “Neighborhood Social Capital” b | “Natural and Built Environment” c | “Neighborhood Safety” d | “Neighborhood Socioeconomic Status” e | “Neighborhood Satisfaction” | “Residential Stability” | “Immigrant Density/Ethnic Heterogeneity” | “Pollution” f | |
|---|---|---|---|---|---|---|---|---|---|
| Outcome | |||||||||
| “Mental health” g | Gutman 2004 [33], Glendinning 2007 [36], Novak 2015 [55], Cole 2019 [70], Kleszczewska 2019 [74], Lorenzo-Blanco 2019 [76], Hirota 2021 [90], Carrillo-Alvarez 2022 [92], Hunduma 2022 [93] | Astell-Burt 2014 [20], Glendinning 2007 [36], Larson 2022 [41], Dzhambov 2018 [64], Dzhambov 2018 [65], Roe 2017 [67], Cole 2019 [70], Colley 2019 [71], Engemann 2019 [72], Srugo 2019 [80], Wang 2019 [81], Franklin 2020 [82], Oswald 2021 [87], Shen 2020 [95], Stahlmann 2022 [96], Zewdie 2022 [98] | Gutman 2004 [33], Glendinning 2007 [36], Ivert 2013 [50] | Soobader 2000 [31], Chen 2006 [34], Ivert 2013 [50], Kleszczewska 2019 [74] | Cicognani 2008 [39] | Cole 2019 [70] | Dzhambov 2017 [63], Dzhambov 2018 [66], Franklin 2020 [82] | ||
| “Depression and depressive symptoms” h | Wickrama 2003 [32], Day 2007 [35], Aslund 2010 [44], Wu 2010 [45], Delany-Brumsey 2014 [49], Lee 2015 [54], Pabayo 2016 [60], Estrada-Martinez 2019 [73], Kleszczewska 2019 [74], Lorenzo-Blanco 2019 [76], Oluwaseyi 2020 [83], Sadler 2022 [94] | Bezold 2018 [69], Mavoa 2019 [78], Zewdie 2022 [98] | Assari 2015 [53], Pabayo 2016 [60], Oluwaseyi 2020 [83], Kleszczewska 2019 [74], Mavoa 2019 [78] | Wickrama 2003 [32], Delany-Brumsey 2014 [49], Lee 2015 [54], Pabayo 2016 [60], Vilhjalmsdottir 2016 [62], Estrada-Martinez 2019 [73], Currier 2019 [86] | Estrada-Martinez 2019 [73] | Wickrama 2003 [32], Lee 2015 [54], Estrada-Martinez 2019 [73] | |||
| “Well-being” i | Day 2007 [35], Cicognani 2008 [39], DeClercq 2012 [46], Aminzadeh 2013 [47], Barnhart 2022 [68], Kleszczewska 2019 [74], Laurence 2019 [75], Malinowska-Cieslik 2019 [77], Benninger 2021 [85] | Huynh 2013 [48], Saw 2015 [58], Hogan 2016 [59], Teixeira 2016 [61], Roe 2017 [67], Mavoa 2019 [78], Zhang 2021 [88], Zhang 2022 [89], Bloemsma 2022 [91], Thompson 2022 [97] | Meltzer 2007 [37], Kleszczewska 2019 [74], Mavoa 2019 [78], Rigg 2019 [79], Benninger 2021 [85] | Day 2007 [35], Meltzer 2007 [37], Cicognani 2008 [39], DeClercq 2012 [46], Saw 2015 [58], Laurence 2019 [75] | Aminzadeh 2013 [47] | Bloemsma 2022 [91] | |||
| “Emotional problems” | Poulain 2020 [84] | Larson 2008 [40] | Soobader 2000 [31] | ||||||
| “Behavioral problems” j | Delany-Brumsey 2014 [49], Lorenzo-Blanco 2019 [76] | Soobader 2000 [31], Delany-Brumsey 2014 [49] | Delany-Brumsey 2014 [49] | ||||||
| “General health” k | Glendinning 2007 [36], Boyce 2008 [38], Borges 2010 [43], DeClercq 2012 [46], Marshall 2014 [51], Mmari 2014 [52], Novak 2015 [56], Novak 2016 [57], Benninger 2021 [85] | Glendinning 2007 [36], Maas 2009 [42], Mmari 2014 [52], Roe 2017 [67], Colley 2019 [71], Benninger 2021 [85], Thompson 2022 [97] | Larson 2008 [40], Benninger 2021 [85] | Soobader 2000 [31], Chen 2006 [34], Glendinning 2007 [36], DeClercq 2012 [46] | |||||
| Author (Year) | Outcome(s)/Exposure(s) | Inequality Assessment Method | Description of Finding |
|---|---|---|---|
| Inequalities by sex/gender | |||
| Gutman (2004) [33] | Mental health/Neighborhood cohesiveness and problems | Subgroup analysis | Significant association between neighborhood cohesiveness and less depressive symptoms among girls but not boys. |
| Day (2007) [35] | Well-being and depression/Neighborhood social capital, social control, safety and SES | Effect measure modification | No significant interaction between neighborhood exposures and sex/gender. |
| Cicognani (2008) [39] | Well-being and stress/Sense of community, social support, area-level disadvantage | Subgroup analysis | Girls living in more disadvantaged town had higher well-being scores than boys. |
| Huynh (2013) [48] | Well-being/Natural space | Effect measure modification | No significant interaction between natural space and sex/gender. |
| Astell-Burt (2014) [20] | General health/Greenspace | Subgroup analysis | Greenspace associated with lower psychiatric morbidity among older adolescent and young adult women. Among men, greenspace not associated with psychiatric morbidity among 15–20 year-olds, but an inverse association strengthens by age 30. |
| Ivert (2014) [50] | Mental health/Neighborhood SES, collective efficacy and social disorder | Subgroup analysis | Poor collective efficacy associated with poorer mental health among boys but not girls. |
| Marshall (2014) [51] | General health/Neighborhood social capital | Subgroup analysis | Stronger associations between social capital and general health among girls compared to boys. |
| Mmari (2014) [52] (qualitative) | Health/Physical and social environments | Subgroup analysis | Feeling unsafe in the neighborhood mentioned as influencing health in Baltimore and Johannesburg (boys), and New Delhi, Shanghai and Ibadan (girls). Physical environment factors such as garbage, dirt, vacant housing and lack of recreation spaces mentioned by both boys and girls. |
| Assari (2015) [53] | Depression/Neighborhood fear of violence | Subgroup analysis | Increase in fear of neighborhood violence over a one-year period associated with an increase in depressive symptoms among men but not women. |
| Lee (2015) [54] | Depression and self-esteem/Neighborhood collective efficacy, Latino immigrant density and neighborhood poverty | Subgroup analysis | Neighborhood density of Latino immigrants associated with lower odds of depression among both male and female Latino immigrant youth, but not among non-immigrant Latino youth. |
| Novak (2015) [55] | Psychological distress/Neighborhood social capital | Effect measure modification | No significant interaction between social capital and sex/gender. |
| Novak (2015) [56] | General health/Neighborhood social capital | Subgroup analysis | No significant interaction between social capital and sex/gender. |
| Pabayo (2016) [60] | Depressive symptoms/Neighborhood disorder, danger, social cohesion, deprivation and income inequality | Effect measure modification | Girls living in more unequal neighborhoods had higher depressive symptoms than those living in more equal areas. |
| Dzhambov (2018) [64] | Mental health/Greenspace | Stratified analysis | Objective and perceived blue space measures associated with lower depressive symptoms among boys only. |
| Dzhambov (2018) [65] | Mental health/Greenspace | Effect measure modification and stratified analysis | No significant effect measure modification between greenspace and sex/gender. |
| Cole (2019) [70] (qualitative) | Resilience and mental health/Community member influences, building/land environment, diversity | Subgroup analysis | Boys reported more concerns about relations with police than girls, which might influence their health unequally. |
| Kleszczewska (2019) [74] | Depression, stress, satisfaction with life and self-efficacy/Neighborhood deprivation and social capital | Subgroup analysis | Social capital had the strongest protective effect for boys vs. girls in least privileged communities. Girls living in unsupportive neighborhood environments had very low satisfaction with life. |
| Malinowska-Cieslik (2019) [77] | Positive attitude/Neighborhood social capital | Subgroup analysis | No significant difference in associations between neighborhood social capital and positive attitude across sex/gender. |
| Poulain (2020) [84] | Emotional problems/Greenspace | Effect measure modification | No significant interaction between greenspace and sex/gender. |
| Zhang (2021) [88] | Emotional response/Greenspace | Effect measure modification | Male adolescents had higher happy scores than female adolescents. |
| Bloemsma (2022) [91] | Well-being/Greenspace and air and noise pollution | Effect measure modification | No significant interaction between greenspace and air or noise pollution and sex/gender. |
| Sadler (2022) [94] | Anxiety and depressive symptoms/Neighborhood social cohesion and inequitable housing practices (gentrifying, blockbusting, redlining) | Effect measure modification | Gentrification has a negative effect on social cohesion and well-being among girls but not boys. Blockbusted neighborhoods have lower social cohesion, leading to higher anxiety and depressive symptoms among boys but not girls. |
| Zewdie (2022) [98] | Psychological health (difficulties and depressive symptoms)/Greenspace | Effect measure modification | Greenspace inversely associated with total difficulties and depressive symptoms among boys but not girls. |
| Inequalities by socioeconomic status (SES) | |||
| Aminzadeh (2013) [47] | Well-being and general mood/Neighborhood social capital | Effect measure modification | Membership in community organizations had stronger protective effect for students who were more, vs. less, socioeconomically disadvantaged. |
| Dzhambov (2018c) [65] | Mental health/Greenspace | Effect measure modification and stratified analysis | No significant interaction between greenspace and SES. |
| Srugo (2019) [80] | Psychological distress, mental health/Greenspace | Effect measure modification | No significant interaction between greenspace and individual SES or neighborhood deprivation. |
| Franklin (2020) [82] | Perceived stress/Pollution, greenness, and night light radiance | Effect measure modification | Association between artificial light at night and stress strongest among participants with lower vs. higher household income. |
| Poulain (2020) [84] | Emotional problems/Greenspace | Effect measure modification | No significant interaction between greenspace and SES. |
| Bloemsma (2022) [91] | Well-being/Greenspace and air and noise pollution | Effect measure modification | No significant interaction between greenspace and air or noise pollution and parental education. |
| Stahlmann (2022) [96] | Mental health/Built environment (social infrastructure places) | Stratified analyses | Stronger associations between social infrastructure and mental health among adolescents with high SES. |
| Zewdie (2022) [98] | Psychological health (difficulties and depressive symptoms)/Greenspace | Effect measure modification | Greenspace exposure associated with lower difficulties among those with an income vs. those without an income. |
| Inequalities by ethnicity | |||
| Huynh (2013) [48] | Well-being/Natural space | Effect measure modification | No significant interaction between natural space and ethnicity. |
| Dzhambov (2018a) [64] | Mental health/Greenspace | Stratified analysis | Greenspace and blue space more strongly associated with mental health in non-Bulgarians than in Bulgarians. |
| Dzhambov (2018b) [66] | Mental health/Noise and air pollution | Subgroup analysis | Stronger inverse associations between noise and air pollution and mental health among non-Bulgarians than among Bulgarians. |
| Cole (2019) [70] (qualitative) | Resilience and mental health/Community member influences, building/land environment, diversity | Subgroup analysis | Asians more concerned about feeling unsafe in the community, while more Latinx youth emphasized feeling their community was like home and family. These differences in perceptions and concerns might unequally influence health. |
| Estrada-Martinez (2019) [73] | Depressive symptoms/Neighborhood satisfaction, SES and immigrant racial/ethnic composition | Effect measure modification and stratified analysis | Significant interaction between ethnicity and neighborhood satisfaction, racial/ethnic composition, and SES (e.g., low neighborhood satisfaction in adolescence associated with increases in depressive symptoms into adulthood for Mexicans and Puerto Ricans, and with lower levels of depressive symptoms in Cubans and other Latinos. |
| Shen (2022) [95] | Mental health/Built environment | Subgroup analysis | Built environment associations with mental health vary across ethnic groups (e.g., presence of libraries positively influences white youth’s mental health, presence of parks has a greater positive impact on Asian American youth’s mental health). |
| Inequalities by immigrant status | |||
| Day (2007) [35] | Well-being and depression/Neighborhood social capital, social control, safety and SES | Effect measure modification | No significant interaction between neighborhood exposures and immigrant status. |
| Ivert (2014) [50] | Mental health/Neighborhood SES, collective efficacy and social disorder | Subgroup analysis | High perceived social disorder associated with mental health problems among Swedish background adolescents but not among those from immigrant backgrounds. |
| Lee (2015) [54] | Depression and self-esteem/Neighborhood collective efficacy, Latino immigrant density and neighborhood poverty | Subgroup analysis | Neighborhood density of Latino immigrants associated with lower odds of depression among Latino immigrant youth, both male and female, but not among non-immigrant Latino youth. |
| Inequalities by level of urbanicity | |||
| Glendinning (2007) [36] | Mental health and general health/Social relations and trust and built environment | Subgroup analysis | Poorer perceptions of social and built environment characteristics associated with mental health in the city but not the smaller (rural) community. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shareck, M.; Aubé, E.; Sersli, S. Neighborhood Physical and Social Environments and Social Inequalities in Health in Older Adolescents and Young Adults: A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 5474. https://doi.org/10.3390/ijerph20085474
Shareck M, Aubé E, Sersli S. Neighborhood Physical and Social Environments and Social Inequalities in Health in Older Adolescents and Young Adults: A Scoping Review. International Journal of Environmental Research and Public Health. 2023; 20(8):5474. https://doi.org/10.3390/ijerph20085474
Chicago/Turabian StyleShareck, Martine, Eliana Aubé, and Stephanie Sersli. 2023. "Neighborhood Physical and Social Environments and Social Inequalities in Health in Older Adolescents and Young Adults: A Scoping Review" International Journal of Environmental Research and Public Health 20, no. 8: 5474. https://doi.org/10.3390/ijerph20085474
APA StyleShareck, M., Aubé, E., & Sersli, S. (2023). Neighborhood Physical and Social Environments and Social Inequalities in Health in Older Adolescents and Young Adults: A Scoping Review. International Journal of Environmental Research and Public Health, 20(8), 5474. https://doi.org/10.3390/ijerph20085474