
The Pendulum Swings Both Ways: Evidence for U-Shaped Association between Sleep Duration and Mental Health Outcomes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Study Variables
2.3. Confounders
2.4. Statistical Analysis
3. Results
3.1. Description of the Sample
3.2. Sleep Duration and Mental Health by Subjective Health
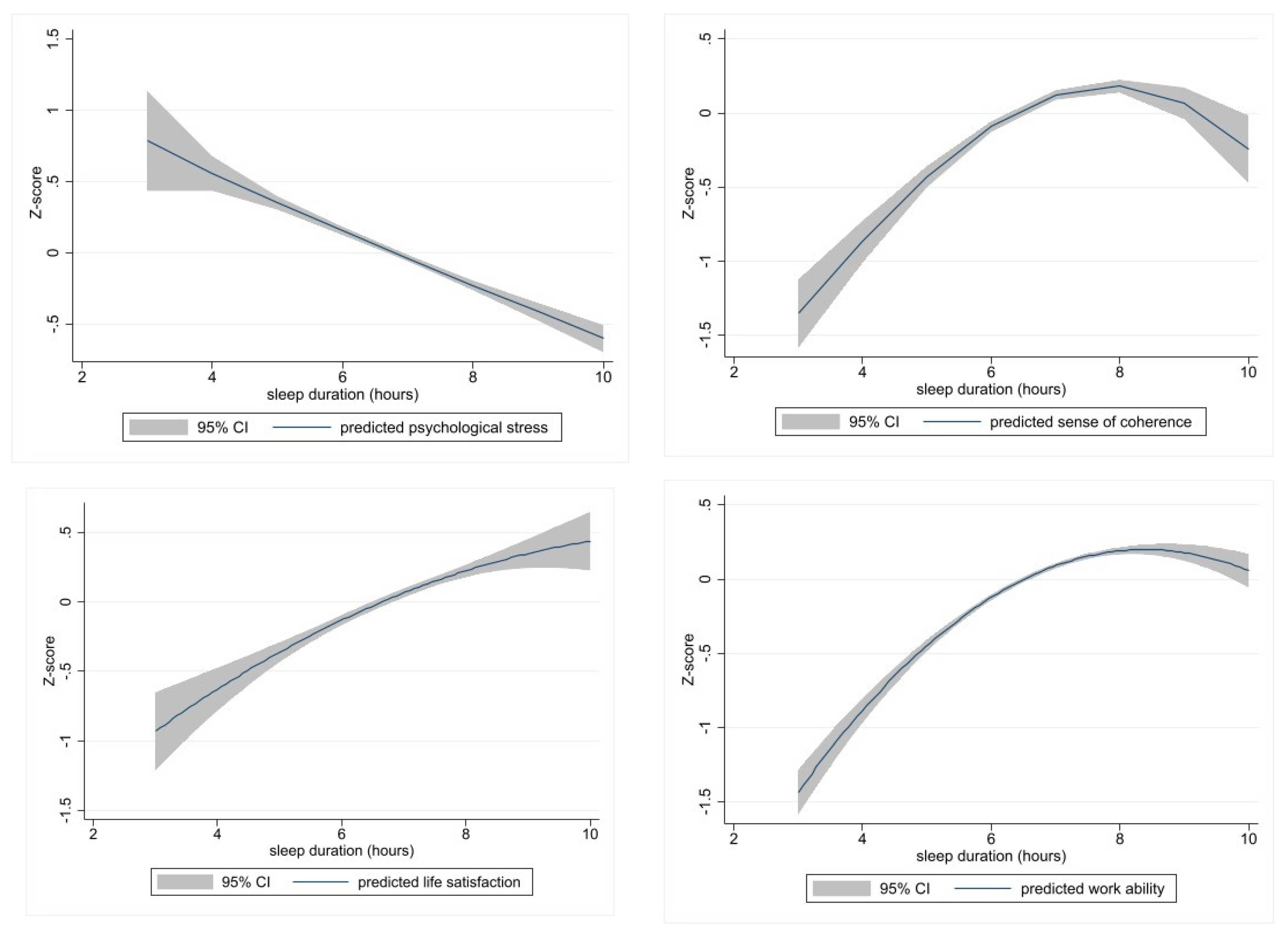
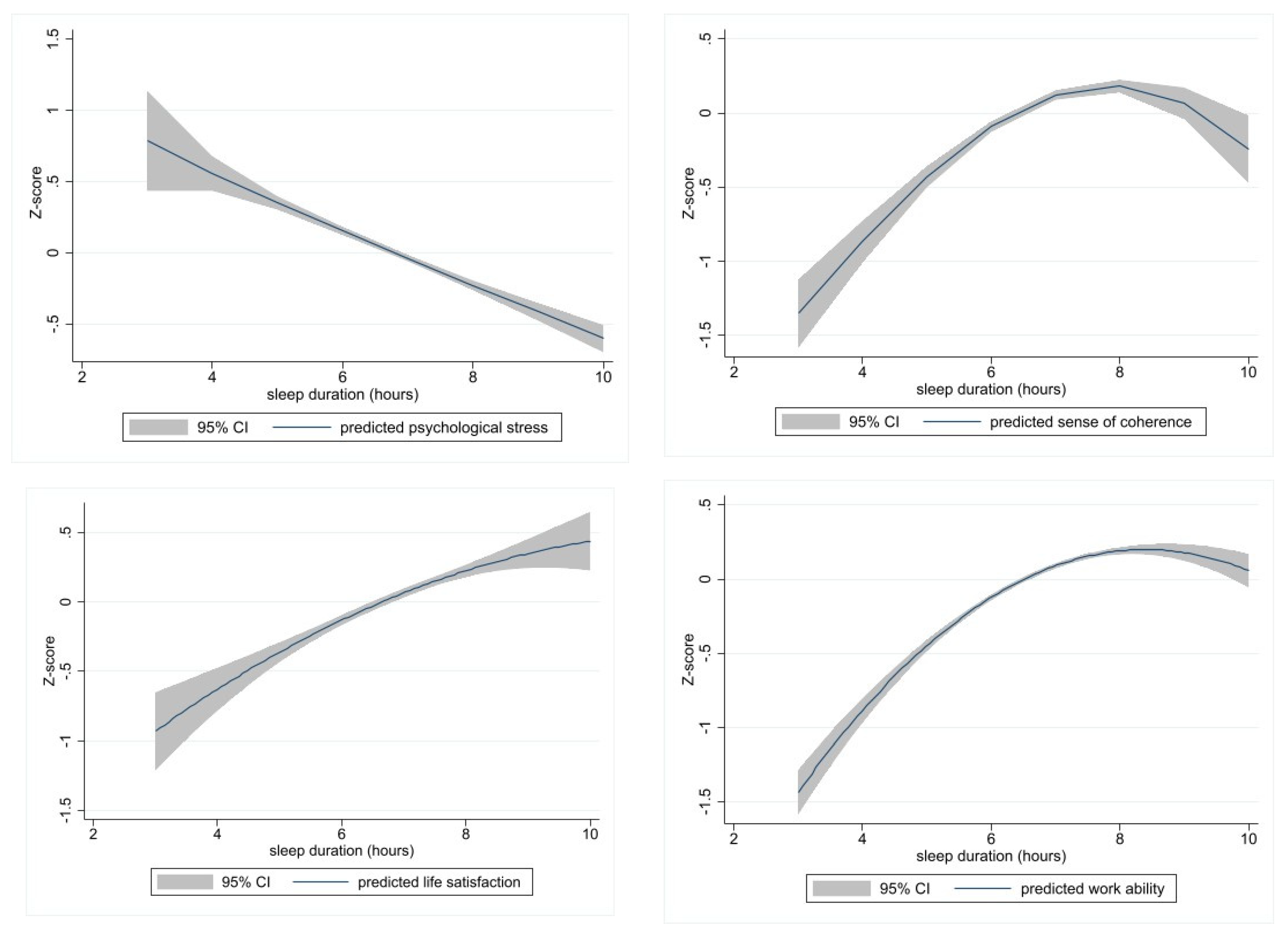
3.3. Effect of Sleep Duration on Measures of Mental Health
3.4. Estimating Parameters in the Best Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dement, W.C. The study of human sleep: A historical perspective. Thorax 1998, 53, S2–S7. [Google Scholar] [PubMed]
- Grandner, M.A. Sleep, Health, and Society. Sleep Med. Clin. 2017, 12, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.R.; Olmstead, R.; Carroll, J.E. Sleep Disturbance, Sleep Duration, and Inflammation: A Systematic Review and Meta-Analysis of Cohort Studies and Experimental Sleep Deprivation. Biol. Psychiatry 2016, 80, 40–52. [Google Scholar] [CrossRef]
- Itani, O.; Jike, M.; Watanabe, N.; Kaneita, Y. Short sleep duration and health outcomes: A systematic review, meta-analysis, and meta-regression. Sleep Med. 2017, 32, 246–256. [Google Scholar] [CrossRef] [PubMed]
- 5American Academy of Sleep Medicine. In International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014.
- Pavlova, M.K.; Latreille, V. Sleep Disorders. Am. J. Med. 2019, 132, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Shepard, J.W.; Buysse, D.J.; Chesson, A.L.; Dement, W.C.; Goldberg, R.; Guilleminault, C.; Harris, C.D.; Iber, C.; Mignot, E.; Mitler, M.M.; et al. History of the Development of Sleep Medicine in the United States. J. Clin. Sleep Med. 2005, 1, 61–82. [Google Scholar] [CrossRef] [PubMed]
- Watson, N.F.; Badr, M.S.; Belenky, G.; Bliwise, D.L.; Buxton, O.M.; Buysse, D.; Dinges, D.F.; Gangwisch, J.; Grandner, M.A.; Kushida, C.; et al. Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society on the Recommended Amount of Sleep for a Healthy Adult: Methodology and Discussion. Sleep 2015, 38, 1161–1183. [Google Scholar] [CrossRef]
- Liu, Y.; Wheaton, A.G.; Chapman, D.P.; Cunningham, T.J.; Lu, H.; Croft, J.B. Prevalence of Healthy Sleep Duration among Adults—United States, 2014. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 137–141. [Google Scholar] [CrossRef]
- Ferrie, J.E.; Kumari, M.; Salo, P.; Singh-Manoux, A.; Kivimaki, M. Sleep epidemiology—A rapidly growing field. Int. J. Epidemiol. 2011, 40, 1431–1437. [Google Scholar] [CrossRef]
- Chattu, V.K.; Manzar, M.D.; Kumary, S.; Burman, D.; Spence, D.W.; Pandi-Perumal, S.R. The Global Problem of Insufficient Sleep and Its Serious Public Health Implications. Healthcare 2018, 7, 1. [Google Scholar] [CrossRef]
- Kripke, D.F.; Garfinkel, L.; Wingard, D.L.; Klauber, M.R.; Marler, M.R. Mortality associated with sleep duration and insomnia. Arch. Gen. Psychiatry 2002, 59, 131–136. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Sleep Duration and All-Cause Mortality: A Systematic Review and Meta-Analysis of Prospective Studies. Sleep 2010, 33, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Gallicchio, L.; Kalesan, B. Sleep duration and mortality: A systematic review and meta-analysis. J. Sleep Res. 2009, 18, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Jike, M.; Itani, O.; Watanabe, N.; Buysse, D.J.; Kaneita, Y. Long sleep duration and health outcomes: A systematic review, meta-analysis and meta-regression. Sleep Med. Rev. 2018, 39, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Tempaku, P.; Hirotsu, C.; Mazzotti, D.; Xavier, G.; Maurya, P.; Brielzke, E.; Belangero, S.; Poyares, D.; Bittencourt, L.; Tufik, S. Long Sleep Duration, Insomnia, and Insomnia With Short Objective Sleep Duration Are Independently Associated with Short Telomere Length. J. Clin. Sleep Med. 2018, 14, 2037–2045. [Google Scholar] [CrossRef]
- de Bruin, A.; Picavet, H.S.J.; Nossikov, A. Health Interview Surveys: Towards International Harmonization of Methods and Instruments; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 1996. [Google Scholar]
- Örkényi, Á. Lelki Egészség. Országos Lakossági Egészségfelmérés 2003 [Mental Health. Hungarian National Health Interview Survey 2003]; Országos Epidemiológiai Központ (National Center of Epidemiology): Budapest, Hungary, 2005. [Google Scholar]
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O.; Rutter, C. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Mittelmark, M.; Sagy, S.; Eriksson, M. The Handbook of Salutogenesis; (e-book) Springer: Cham, Switzerland, 2017. [Google Scholar] [CrossRef]
- Balajti, I.; Vokó, Z.; Ádány, R.; Kósa, K. A rövidített koherencia-érzés és az általános egészség (GHQ) kérdőívek magyar nyelvű változatának validálása [Validation of the Hungarian versions of the abbreviated sense of coherence (SoC) and the general health questionnaire (GHQ-12)]. Mentálhigiéné És Pszichoszomatika 2007, 8, 147–161. [Google Scholar] [CrossRef]
- Antonovsky, A. Unravelling the Mystery of Health—How People Manage Stress and Stay Well; Jossey Bass Publishers: San Francisco, CA, USA, 1987. [Google Scholar]
- Quality of Life Indicators—Overall Experience of Life. Eurostat Statistics Explained. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Quality_of_life_indicators_-_overall_experience_of_life (accessed on 26 January 2021).
- Munkaképességi Index Kérdőív [Work Ability Index Questionnaire]; Nemzeti Munkaügyi Hivatal [National Office of Occupational Health]: Budapest, Hungary, 2012.
- Albert, F.; Dávid, B.; Németh, R. Társas Támogatás, Társadalmi Kohézió [Social Support, Social Cohesion]. Országos Lakossági Egészségfelmérés (OLEF) 2003. [Hungarian National Health Interview Survey 2003]; Országos Epidemiológiai Központ: Budapest, Hungary, 2005. [Google Scholar]
- ELEF Kérdőív 2014 [EHIS Questionnaire 2014]. Available online: http://www.ksh.hu/elef/archiv/2014/pdfs/elef2014_kerdoiv.pdf (accessed on 26 January 2021).
- Darren, G.; Mallery, P. SPSS for Windows Step by Step: A Simple Guide and Reference, 17.0; Allyn&Bacon: Boston, MA, USA, 2010. [Google Scholar]
- Lallukka, T.; Pietilainen, O.; Jappinen, S.; Laaksonen, M.; Lahti, J.; Rahkonen, O. Factors associated with health survey response among young employees: A register-based study using online, mailed and telephone interview data collection methods. BMC Public Health 2020, 20, 184. [Google Scholar] [CrossRef]
- Yang, Y.; Zhu, J.F.; Yang, S.Y.; Lin, H.J.; Chen, Y.; Zhao, Q.; Fu, C.W. Prevalence and associated factors of poor sleep quality among Chinese returning workers during the COVID-19 pandemic. Sleep Med. 2020, 73, 47–52. [Google Scholar] [CrossRef]
- Cheung, K.L.; ten Klooster, P.M.; Smit, C.; de Vries, H.; Pieterse, M.E. The impact of non-response bias due to sampling in public health studies: A comparison of voluntary versus mandatory recruitment in a Dutch national survey on adolescent health. BMC Public Health 2017, 17, 276. [Google Scholar] [CrossRef]
- Glozier, N.; Martiniuk, A.; Patton, G.; Ivers, R.; Li, Q.A.; Hickie, I.; Senserrick, T.; Woodward, M.; Norton, R.; Stevenson, M. Short Sleep Duration in Prevalent and Persistent Psychological Distress in Young Adults: The DRIVE Study. Sleep 2010, 33, 1139–1145. [Google Scholar] [CrossRef] [PubMed]
- John, U.; Meyer, C.; Rumpf, H.J.; Hapke, U. Relationships of psychiatric disorders with sleep duration in an adult general population sample. J. Psychiatry Res. 2005, 39, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Kaneita, Y.; Ohida, T.; Uchiyama, M.; Takemura, S.; Kawahara, K.; Yokoyama, E.; Miyake, T.; Harano, S.; Suzuki, K.; Fujita, T. The relationship between depression and sleep disturbances: A Japanese nationwide general population survey. J. Clin. Psychiatry 2006, 67, 196–203. [Google Scholar] [CrossRef]
- Ryu, S.Y.; Kim, K.S.; Han, M.A. Factors Associated with Sleep Duration in Korean Adults: Results of a 2008 Community Health Survey in Gwangju Metropolitan City, Korea. J. Korean Med. Sci. 2011, 26, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M.; Han, S.M.; Min, I.K.; Heo, K.; Kim, W.J.; Chu, M.K. Weekend catch-up sleep and depression: Results from a nationally representative sample in Korea. Sleep Med. 2021, 87, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.W.; Jin, X.L.; Shan, Z.L.; Li, S.Z.; Huang, H.; Li, P.Y.; Peng, X.B.; Peng, Z.; Yu, K.F.; Bao, W.; et al. Relationship of Sleep Duration With All-Cause Mortality and Cardiovascular Events: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. J. Am. Heart Assoc. 2017, 6, e005947. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Reynolds, C.F.; Dauvilliers, Y. Excessive sleep duration and quality of life. Ann. Neurol. 2013, 73, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C.; Son, D.H.; Kwon, Y.J. U-Shaped Association between Sleep Duration, C-Reactive Protein, and Uric Acid in Korean Women. Int. J. Environ. Res. Public Health 2020, 17, 2657. [Google Scholar] [CrossRef]
- Tsai, T.C.; Wu, J.S.; Yang, Y.C.; Huang, Y.H.; Lu, F.H.; Chang, C.J. Long Sleep Duration Associated With a Higher Risk of Increased Arterial Stiffness in Males. Sleep 2014, 37, 1315–1320. [Google Scholar] [CrossRef]
- Anujuo, K.; Stronks, K.; Snijder, M.B.; Jean-Louis, G.; van den Born, B.J.; Peters, R.J.; Agyemang, C. Relationship between sleep duration and arterial stiffness in a multi-ethnic population: The HELIUS study. Chronobiol. Int. 2016, 33, 543–552. [Google Scholar] [CrossRef]
- Youngstedt, S.D.; Goff, E.E.; Reynolds, A.M.; Kripke, D.F.; Irwin, M.R.; Bootzin, R.R.; Khan, N.; Jean-Louis, G. Has adult sleep duration declined over the last 50+years? Sleep Med. Rev. 2016, 28, 69–85. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | Sleep Duration | p Value | |||||
|---|---|---|---|---|---|---|---|
| <7 h | 7 h | >7 h | |||||
| N | % | N | % | N | % | ||
| Gender | 0.103 | ||||||
| Male | 141 | 36.34 | 154 | 39.69 | 93 | 23.97 | |
| Female | 275 | 33.37 | 303 | 36.77 | 246 | 29.85 | |
| Age group | 0.169 | ||||||
| 18–29 years | 49 | 28.32 | 62 | 35.84 | 62 | 35.84 | |
| 30–45 years | 212 | 35.16 | 229 | 37.98 | 162 | 26.87 | |
| 46–59 years | 131 | 38.3 | 126 | 36.84 | 85 | 24.85 | |
| 60 ≥ years | 25 | 32.05 | 31 | 39.74 | 22 | 28.21 | |
| Lives with partner | 0.829 | ||||||
| No | 151 | 33.48 | 171 | 37.92 | 129 | 28.6 | |
| Yes | 263 | 35.21 | 277 | 37.08 | 207 | 27.71 | |
| Education | 0.544 | ||||||
| Secondary | 55 | 33.74 | 57 | 34.97 | 51 | 31.29 | |
| Tertiary | 362 | 34.54 | 400 | 38.17 | 286 | 27.29 | |
| Employment position | 0.013 | ||||||
| Manager | 65 | 43.62 | 58 | 38.93 | 26 | 17.45 | |
| Non-manager | 348 | 33.82 | 397 | 38.58 | 284 | 27.6 | |
| Smoking | 0.593 | ||||||
| Current smoker | 67 | 38.07 | 66 | 37.5 | 43 | 24.43 | |
| Former smoker | 80 | 37.74 | 78 | 36.79 | 54 | 25.47 | |
| Never smoked | 264 | 33.55 | 305 | 38.75 | 218 | 27.7 | |
| Social support | 0.001 | ||||||
| Severe lack | 61 | 47.66 | 49 | 38.28 | 18 | 14.06 | |
| Moderate lack | 87 | 40.47 | 76 | 35.35 | 52 | 24.19 | |
| Optimal support | 246 | 31.82 | 305 | 39.46 | 222 | 28.72 | |
| Variables | Subjective Health | p | |
|---|---|---|---|
| Less Than Good | At Least Good | ||
| Gender (%) | 0.178 | ||
| Male | 27.65 | 72.35 | |
| Female | 31.46 | 68.54 | |
| Age (years) | 43.72 | 40.97 | <0.001 |
| Lives with partner (%) | 0.825 | ||
| No | 29.69 | 70.31 | |
| Yes | 30.29 | 69.71 | |
| Education (%) | <0.001 | ||
| Secondary | 44.17 | 55.83 | |
| Tertiary | 28.16 | 71.84 | |
| Employment position (%) | 0.638 | ||
| Manager | 28.38 | 71.62 | |
| Nonmanager | 30.27 | 69.73 | |
| Social support (%) | <0.001 | ||
| Severe lack | 51.56 | 48.44 | |
| Moderate lack | 33.64 | 66.36 | |
| Optimal support | 25.03 | 74.97 | |
| Sleep duration (hours) | 6.62 | 6.91 | <0.001 |
| Psychological distress (GHQ-12, %) | <0.001 | ||
| Stressed | 52.90 | 47.10 | |
| Not stressed | 27.01 | 72.99 | |
| Sense of coherence (mean) | 63.10 | 68.37 | <0.001 |
| Satisfaction with life (mean) | 7.55 | 8.38 | <0.001 |
| Work ability (mean) | 8.1 | 8.7 | <0.001 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 gender | 1.000 | ||||||||||||
| 2 age | 1.000 | ||||||||||||
| 3 lives with partner | 0.284 * | 1.000 | |||||||||||
| 4 education | −0.107 | 1.000 | |||||||||||
| 5 employment position | 0.144 * | −0.317 * | 0.155 * | 0.128 * | 1.000 | ||||||||
| 6 smoking | 1.000 | ||||||||||||
| 7 social support | 1.000 | ||||||||||||
| 8 sleep duration | 0.129 | 1.000 | |||||||||||
| 9 subjective health | −0.120 | 0.137 * | 0.181 * | 0.140 * | 1.000 | ||||||||
| 10 psychol.stress | −0.103 | −0.112 | −0.304 * | −0.186 * | −0.306 * | 1.000 | |||||||
| 11 sense of coherence | 0.190 * | 0.200 * | −0.189 * | 0.352 * | 0.155 * | 0.232 * | −0.489 * | 1.000 | |||||
| 12 satisfaction w/ llife | 0.209 * | −0.130 * | 0.421 * | 0.183 * | 0.282 * | −0.458 * | 0.555 * | 1.000 | |||||
| 13 work ability | 0.101 | 0.203 * | 0.182 * | 0.263 * | −0.319 * | 0.358 * | 0.406 * | 1.000 | |||||
| Mean (±SD) | n/a | 41.83 (11) | n/a | n/a | n/a | n/a | n/a | 6.83 (0.98) | n/a | 23.86 (4.04) | 66.77 (11.26) | 8.13 (1.65) | 8.52 (1.23) |
| Min-max values | 223–85 | 1−12 | 15–43 | 23–91 | 1–10 | 2–10 |
| Outcomes | Linear Model | Quadratic Model | Fractional Polynomial Model |
|---|---|---|---|
| Psychological distress | |||
| sleep duration (p) | <0.001 | 0.002 | |
| sleep duration squared (p) | n/a | 0.033 | n/a |
| sleep duration (power → p) | n/a | n/a | 1 → <0.001 |
| age (power → p) | 3 → <0.001 | ||
| adjusted R2 | 0.130 | 0.133 | 0.134 |
| RMSE | 0.933 | 0.931 | 0.931 |
| AIC | 2745.9 | 2743.3 | 2740.9 |
| Sense of coherence | |||
| sleep duration (p) | <0.001 | 0.002 | |
| sleep duration squared (p) | n/a | 0.018 | n/a |
| sleep duration1 (power → p) | n/a | n/a | 2 → <0.001 |
| sleep duration2 (power → p) | n/a | n/a | 3 → <0.001 |
| adjusted R2 | 0.190 | 0.194 | 0.199 |
| RMSE | 0.890 | 0.888 | 0.886 |
| AIC | 2523.7 | 2520.1 | 2514.2 |
| Life satisfaction | |||
| sleep duration (p) | <0.001 | 0.021 | |
| sleep duration squared (p) | n/a | 0.132 | n/a |
| sleep duration (power → p) | n/a | n/a | 1 → <0.001 |
| adjusted R2 | 0.224 | 0.225 | 0.224 |
| RMSE | 0.871 | 0.871 | 0.871 |
| AIC | 2673.9 | 2673.6 | 2673.9 |
| Work ability | |||
| sleep duration (p) | <0.001 | <0.001 | |
| sleep duration squared (p) | n/a | <0.001 | n/a |
| sleep duration (power → p) | n/a | n/a | −1 → <0.001 |
| adjusted R2 | 0.075 | 0.086 | 0.079 |
| RMSE | 0.958 | 0.952 | 0.955 |
| AIC | 2903.4 | 2891.5 | 2898.0 |
| Sleep as Main Effect Variable and Covariates | Outcome Indicators of Mental Health | |||
|---|---|---|---|---|
| Psychological Stress Estimate (SE) | Sense of Coherence Estimate (SE) | Life Satisfaction Estimate (SE) | Work Ability Estimate (SE) | |
| Model | Frac. polynomial | Frac. polynomial | Quadratic | Quadratic |
| sleep duration (hours) | n/a | n/a | 0.406 (0.18) * | 0.866 (0.15) *** |
| sleep duration squared | n/a | n/a | −0.019 (0.01) | −0.051 (0.01) *** |
| sleep duration power1 | −0.173 (0.03) *** | 0.096 (0.02) *** | n/a | n/a |
| sleep duration power2 | n/a | −0.008 (0.002) ** | n/a | n/a |
| gender (female vs male) | 0.096 (0.06) | 0.016 (0.06) | 0.196 (0.06) ** | 0.186 (0.06) ** |
| age (years) | n/a | 0.013 (0.002) *** | 0.001 (0.002) | −0.003 (0.002) |
| age (years) power | −0.017 (0.0004) *** | n/a | n/a | n/a |
| living w/partner (yes vs no) | −0.051 (0.06) | 0.353 (0.06) ** | 0.352 (0.05) *** | 0.130 (0.06) |
| education (tertiary vs secondary) | −0.073 (0.09) | 0.303 (0.10) ** | 0.300 (0.08) *** | 0.059 (0.10) |
| employment position (manager vs non-manager) | −0.200 (0.07) ** | 0.341 (0.08) *** | 0.268 (0.06) *** | 0.401 (0.07) *** |
| social support (optimal vs suboptimal) | −0.589 (0.07) *** | 0.639 (0.06) *** | 0.750 (0.06) *** | 0.401 (0.06) *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kósa, K.; Vincze, S.; Veres-Balajti, I.; Bába, É.B. The Pendulum Swings Both Ways: Evidence for U-Shaped Association between Sleep Duration and Mental Health Outcomes. Int. J. Environ. Res. Public Health 2023, 20, 5650. https://doi.org/10.3390/ijerph20095650
Kósa K, Vincze S, Veres-Balajti I, Bába ÉB. The Pendulum Swings Both Ways: Evidence for U-Shaped Association between Sleep Duration and Mental Health Outcomes. International Journal of Environmental Research and Public Health. 2023; 20(9):5650. https://doi.org/10.3390/ijerph20095650
Chicago/Turabian StyleKósa, Karolina, Szilvia Vincze, Ilona Veres-Balajti, and Éva Bácsné Bába. 2023. "The Pendulum Swings Both Ways: Evidence for U-Shaped Association between Sleep Duration and Mental Health Outcomes" International Journal of Environmental Research and Public Health 20, no. 9: 5650. https://doi.org/10.3390/ijerph20095650
APA StyleKósa, K., Vincze, S., Veres-Balajti, I., & Bába, É. B. (2023). The Pendulum Swings Both Ways: Evidence for U-Shaped Association between Sleep Duration and Mental Health Outcomes. International Journal of Environmental Research and Public Health, 20(9), 5650. https://doi.org/10.3390/ijerph20095650