
The Effect of Social Isolation, Loneliness, and Physical Activity on Depressive Symptoms of Older Adults during COVID-19: A Moderated Mediation Analysis


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Descriptive Data and Correlations
3.2. Mediation Analysis
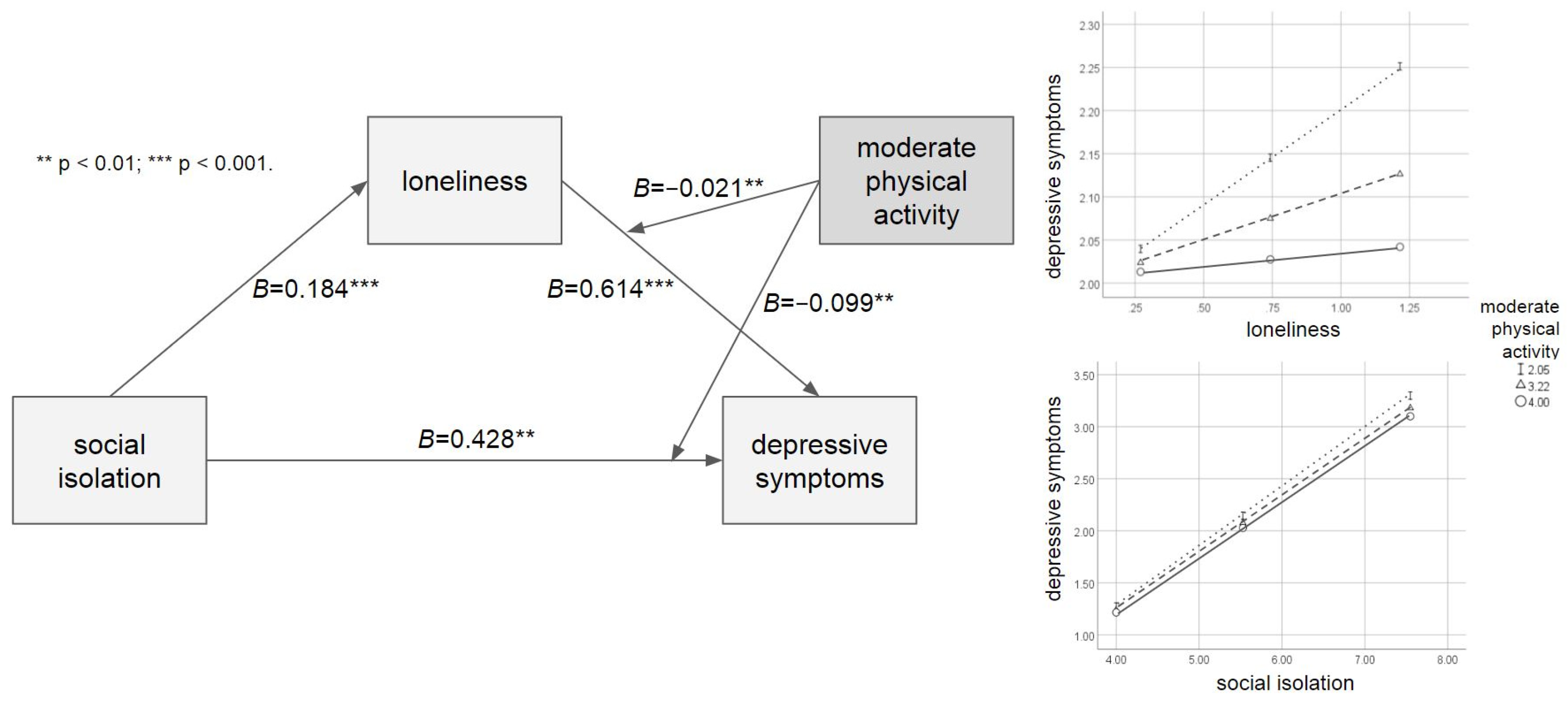
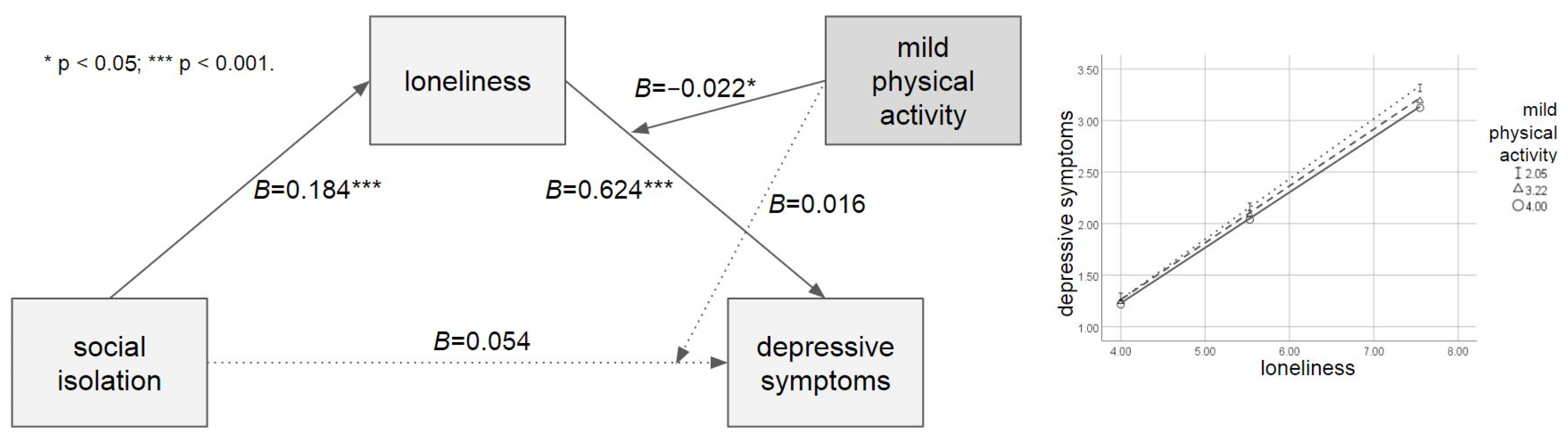
3.3. Moderated Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bailey, L.; Ward, M.; DiCosimo, A.; Baunta, S.; Cunningham, C.; Romero-Ortuno, R.; Kenny, R.A.; Purcell, R.; Lannon, R.; McCarroll, K.; et al. Physical and mental health of older people while cocooning during the COVID-19 pandemic. QJM Int. J. Med. 2021, 114, 648–653. [Google Scholar] [CrossRef] [PubMed]
- Levkovich, I.; Shinan-Altman, S.; Schvartz, N.E.; Alperin, M. Depression and health-related quality of life among elderly patients during the COVID-19 pandemic in Israel: A cross-sectional study. J. Prim. Care Community Health 2021, 12, 2150132721995448. [Google Scholar] [CrossRef]
- Mistry, S.K.; Ali, A.R.M.M.; Hossain, B.; Yadav, U.N.; Ghimire, S.; Rahman, A.; Irfan, N.M.; Huque, R. Exploring depressive symptoms and its associates among Bangladeshi older adults amid COVID-19 pandemic: Findings from a cross-sectional study. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 1487–1497. [Google Scholar] [CrossRef] [PubMed]
- Robb, C.E.; de Jager, C.A.; Ahmadi-Abhari, S.; Giannakopoulou, P.; Udeh-Momoh, C.; McKeand, J.; Price, G.; Car, J.; Majeed, A.; Ward, H.; et al. Associations of social isolation with anxiety and depression during the early COVID-19 pandemic: A survey of older adults in London, UK. Front. Psychiatry 2020, 11, 591120. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Du, X.; Lai, L.; Ren, Z.; Li, H. Prevalence of depressive and anxiety symptoms among Chinese older adults during the COVID-19 pandemic: A systematic review and meta-analysis. J. Geriatr. Psychiatry Neurol. 2022, 35, 182–195. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Jeong, G.-C.; Yim, J. Consideration of the psychological and mental health of the elderly during COVID-19: A theoretical review. Int. J. Environ. Res. Public Health 2020, 17, 8098. [Google Scholar] [CrossRef] [PubMed]
- Louie, L.L.; Chan, W.-C.; Cheng, C.P. Suicidal risk in older patients with depression during COVID-19 pandemic: A case-control study. East Asian Arch. Psychiatry 2021, 31, 3–8. [Google Scholar] [CrossRef]
- Sher, L. The impact of the COVID-19 pandemic on suicide rates. QJM Int. J. Med. 2020, 113, 707–712. [Google Scholar] [CrossRef]
- Santini, Z.I.; Jose, P.E.; Cornwell, E.Y.; Koyanagi, A.; Nielsen, L.; Hinrichsen, C.; Meilstrup, C.; Madsen, K.R.; Koushede, V. Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): A longitudinal mediation analysis. Lancet Public Health 2020, 5, e62–e70. [Google Scholar] [CrossRef]
- Webb, L. COVID-19 lockdown: A perfect storm for older people’s mental health. J. Psychiatr. Ment. Health Nurs. 2021, 28, 300. [Google Scholar] [CrossRef]
- Victor, C.; Scambler, S.; Bond, J.; Bowling, A. Being alone in later life: Loneliness, social isolation and living alone. Rev. Clin. Gerontol. 2000, 10, 407–417. [Google Scholar] [CrossRef]
- de Jong-Gierveld, J.; van Tilburg, T.G.; Dykstra, P.A. Loneliness and social isolation. In The Cambridge Handbook of Personal Relationships; Cambridge University Press: Cambridge, UK, 2006; pp. 485–500. [Google Scholar]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, D. The impact of COVID-19 pandemic on elderly mental health. Int. J. Geriatr. Psychiatry 2020, 35, 1466–1467. [Google Scholar] [CrossRef] [PubMed]
- Shrira, A.; Hoffman, Y.; Bodner, E.; Palgi, Y. COVID-19-related loneliness and psychiatric symptoms among older adults: The buffering role of subjective age. Am. J. Geriatr. Psychiatry 2020, 28, 1200–1204. [Google Scholar] [CrossRef] [PubMed]
- Callow, D.D.; Arnold-Nedimala, N.A.; Jordan, L.S.; Pena, G.S.; Won, J.; Woodard, J.L.; Smith, J.C. The mental health benefits of physical activity in older adults survive the COVID-19 pandemic. Am. J. Geriatr. Psychiatry 2020, 28, 1046–1057. [Google Scholar] [CrossRef] [PubMed]
- Siegmund, L.A.; Distelhorst, K.S.; Bena, J.F.; Morrison, S.L. Relationships between physical activity, social isolation, and depression among older adults during COVID-19: A path analysis. Geriatr. Nurs. 2021, 42, 1240–1244. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.; Seiffer, B.; Zeibig, J.-M.; Welkerling, J.; Brokmeier, L.; Atrott, B.; Ehring, T.; Schuch, F.B. Is physical activity associated with less depression and anxiety during the COVID-19 pandemic? A rapid systematic review. Sports Med. 2021, 51, 1771–1783. [Google Scholar] [CrossRef]
- Lage, A.; Carrapatoso, S.; Neto, E.S.d.Q.; Gomes, S.; Soares-Miranda, L.; Bohn, L. Associations between depressive symptoms and physical activity intensity in an older adult population during COVID-19 lockdown. Front. Psychol. 2021, 12, 644106. [Google Scholar] [CrossRef]
- Herbolsheimer, F.; Ungar, N.; Peter, R. Why is social isolation among older adults associated with depressive symptoms? The mediating role of out-of-home physical activity. Int. J. Behav. Med. 2018, 25, 649–657. [Google Scholar] [CrossRef]
- Hawkley, L.C.; Thisted, R.A.; Cacioppo, J.T. Loneliness predicts reduced physical activity: Cross-sectional & longitudinal analyses. Health Psychol. 2009, 28, 354–363. [Google Scholar] [CrossRef]
- Addario, G.; Dangerfield, P.; Hussey, D.; Pacchioti, B.; Wood, M. Adapting fieldwork during the COVID-19 outbreak: A methodological overview of the ELSA COVID-19 Substudy (wave 1). NatCen 2020, 44, 3–5. [Google Scholar]
- Ge, L.; Yap, C.W.; Ong, R.; Heng, B.H. Social isolation, loneliness and their relationships with depressive symptoms: A population-based study. PLoS ONE 2017, 12, e0182145. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, J.-A.; Brar, J.S.; Rush, E.B.; Jolley, C.J. Physical activity and depressive symptoms in older adults. Geriatr. Nurs. 2014, 35, 37–41. [Google Scholar] [CrossRef] [PubMed]
- O’Halloran, A.; Kenny, R.; King-Kallimanis, B. The latent factors of depression from the short forms of the CES-D are consistent, reliable and valid in community-living older adults. Eur. Geriatr. Med. 2014, 5, 97–102. [Google Scholar] [CrossRef]
- Russell, D.; Peplau, L.A.; Cutrona, C.E. The revised UCLA Loneliness Scale: Concurrent and discriminant validity evidence. J. Personal. Soc. Psychol. 1980, 39, 472–480. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA; London, UK, 2017. [Google Scholar]
- Curran, P.J.; West, S.G.; Finch, J.F. The robustness of test statistics to nonnormality and specification error in confirmatory factor analysis. Psychol. Methods 1996, 1, 16–29. [Google Scholar] [CrossRef]
- Hayes, A.F.; Rockwood, N.J. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav. Res. Ther. 2017, 98, 39–57. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Irwin, M.R.; Cho, H.J. Impact of social isolation on behavioral health in elderly: Systematic review. World J. Psychiatry 2015, 5, 432–438. [Google Scholar] [CrossRef]
- Gorenko, J.A.; Moran, C.; Flynn, M.; Dobson, K.; Konnert, C. Social isolation and psychological distress among older adults related to COVID-19: A narrative review of remotely-delivered interventions and recommendations. J. Appl. Gerontol. 2021, 40, 3–13. [Google Scholar] [CrossRef]
- de Sousa, I.L.M.; Silveira, R.; Takito, M.Y.; Pereira, A.L.; Lucianelli-Júnior, D.; Carmona, G.S.; Viegas, A.P.D.V.; Teixeira, F.B.; Santos, O.S.; Valentin, F.N. The impact of the social isolation in elderly Brazilian mental health (anxiety and depression) during the COVID-19 pandemic. Front. Psychiatry 2022, 13, 888234. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Hughes, M.E.; Waite, L.J.; Hawkley, L.C.; Thisted, R.A. Loneliness as a specific risk factor for depressive symptoms: Cross-sectional and longitudinal analyses. Psychol. Aging 2006, 21, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Domènech-Abella, J.; Mundó, J.; Haro, J.M.; Rubio-Valera, M. Anxiety, depression, loneliness and social network in the elderly: Longitudinal associations from The Irish Longitudinal Study on Ageing (TILDA). J. Affect. Disord. 2019, 246, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Gerst-Emerson, K.; Jayawardhana, J. Loneliness as a public health issue: The impact of loneliness on health care utilization among older adults. Am. J. Public Health 2015, 105, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Newall, N.E.G.; Menec, V.H. Loneliness and social isolation of older adults: Why it is important to examine these social aspects together. J. Soc. Pers. Relatsh. 2019, 36, 925–939. [Google Scholar] [CrossRef]
- Donovan, N.J.; Blazer, D. Social isolation and loneliness in older adults: Review and commentary of a national academies report. Am. J. Geriatr. Psychiatry 2020, 28, 1233–1244. [Google Scholar] [CrossRef] [PubMed]
- Tragantzopoulou, P.; Giannouli, V. Social isolation and loneliness in old age: Exploring their role in mental and physical health. Psychiatriki 2021, 32, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Kuang, J.; Xin, Z.; Fang, J.; Song, R.; Yang, Y.; Song, P.; Wang, Y.; Wang, J. Loneliness, social isolation, depression and anxiety among the elderly in Shanghai: Findings from a longitudinal study. Arch. Gerontol. Geriatr. 2023, 110, 104980. [Google Scholar] [CrossRef]
- Creese, B.; Khan, Z.; Henley, W.; O’Dwyer, S.; Corbett, A.; Da Silva, M.V.; Mills, K.; Wright, N.; Testad, I.; Aarsland, D.; et al. Loneliness, physical activity, and mental health during COVID-19: A longitudinal analysis of depression and anxiety in adults over the age of 50 between 2015 and 2020. Int. Psychogeriatr. 2021, 33, 505–514. [Google Scholar] [CrossRef]
- Vargas, I.; Howie, E.K.; Muench, A.; Perlis, M.L. Measuring the effects of social isolation and dissatisfaction on depressive symptoms during the COVID-19 pandemic: The moderating role of sleep and physical activity. Brain Sci. 2021, 11, 1449. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef]
- Li, L.; Wang, L.; Duan, Y.; Xiao, P.; Zhou, Y.; Luo, X.; Liu, X.; Xie, J.; Cheng, A.S.K. Intelligent physical activity versus modified behavioral activation in adolescent and young adult cancer patients with psychological distress: A randomized, controlled pilot trial. Cancer Med. 2023, 12, 1935–1948. [Google Scholar] [CrossRef] [PubMed]
- Pentecost, C.; Farrand, P.; Greaves, C.J.; Taylor, R.S.; Warren, F.C.; Hillsdon, M.; Green, C.; Welsman, J.R.; Rayson, K.; Evans, P.H.; et al. Combining behavioural activation with physical activity promotion for adults with depression: Findings of a parallel-group pilot randomised controlled trial (BAcPAc). Trials 2015, 16, 367. [Google Scholar] [CrossRef] [PubMed]
- Soucy, I.; Provencher, M.D.; Fortier, M.; McFadden, T. Secondary outcomes of the guided self-help behavioral activation and physical activity for depression trial. J. Ment. Health 2018, 28, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Buman, M.P.; Tuccitto, D.E.; Giacobbi, P.R. Predicting daily reports of leisure-time exercise from stress appraisals and coping using a multilevel modeling approach. J. Sport Exerc. Psychol. 2007, 29, S150. [Google Scholar]
- Sudeck, G.; Pfeifer, K. Bewegungsbezogene Gesundheitskompetenz als integrative Zielgröße in Bewegungstherapie und Gesundheitssport–Konzeption und Validierung eines Erhebungsverfahrens. Sportwissenschaft 2016, 46, 74–87. [Google Scholar] [CrossRef]
- Baumbach, L.; König, H.-H.; Hajek, A. Associations between changes in physical activity and perceived social exclusion and loneliness within middle-aged adults—Longitudinal evidence from the German ageing survey. BMC Public Health 2023, 23, 274. [Google Scholar] [CrossRef] [PubMed]
- Schrempft, S.; Jackowska, M.; Hamer, M.; Steptoe, A. Associations between social isolation, loneliness, and objective physical activity in older men and women. BMC Public Health 2019, 19, 74. [Google Scholar] [CrossRef]
- Shvedko, A.; Whittaker, A.C.; Thompson, J.L.; Greig, C.A. Physical activity interventions for treatment of social isolation, loneliness or low social support in older adults: A systematic review and meta-analysis of randomised controlled trials. Psychol. Sport Exerc. 2018, 34, 128–137. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- McMullan, I.I.; Bunting, B.P.; Burns, A.; Smith, L.; Cunningham, C.; O’Sullivan, R.; Blackburn, N.E.; Wilson, J.J.; Tully, M.A. Is physical activity associated with loneliness or social isolation in older adults? Results of a longitudinal analysis using the Irish longitudinal study on ageing. J. Aging Phys. Act. 2021, 29, 562–572. [Google Scholar] [CrossRef]
- Pels, F.; Kleinert, J. Loneliness and physical activity: A systematic review. Int. Rev. Sport Exerc. Psychol. 2016, 9, 231–260. [Google Scholar] [CrossRef]
- Bae, S.M. The Association between adverse childhood and adulthood experiences, social isolation, loneliness, and depression among young adults in South Korea. Int. J. Environ. Res. Public Health 2023, 20, 6900. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Zhang, M.; Yang, Q.; Yu, B. Gender differences in the influence of social isolation and loneliness on depressive symptoms in college students: A longitudinal study. Soc. Psychiatry Psychiatr. Epidemiol. 2020, 55, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Xie, W.; Wang, Y.; Xiong, Y.; Chen, S.; Han, J.; Wu, Q. A comparative overview of COVID-19, MERS and SARS: Review article. Int. J. Surg. 2020, 81, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Boden, M.; Cohen, N.; Froelich, J.M.; Hoggatt, K.J.; Magid, H.S.A.; Mushiana, S.S. Mental disorder prevalence among populations impacted by coronavirus pandemics: A multilevel meta-analytic study of COVID-19, MERS & SARS. Gen. Hosp. Psychiatry 2021, 70, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Delanerolle, G.; Zeng, Y.; Shi, J.-Q.; Yeng, X.; Goodison, W.; Shetty, A.; Shetty, S.; Haque, N.; Elliot, K.; Ranaweera, S.; et al. Mental health impact of the Middle East respiratory syndrome, SARS, and COVID-19: A comparative systematic review and meta-analysis. World J. Psychiatry 2022, 12, 739–765. [Google Scholar] [CrossRef]
- Hawton, A.; Green, C.; Dickens, A.P.; Richards, S.H.; Taylor, R.S.; Edwards, R.; Greaves, C.J.; Campbell, J.L. The impact of social isolation on the health status and health-related quality of life of older people. Qual. Life Res. 2011, 20, 57–67. [Google Scholar] [CrossRef]
- Nicholson, N.R., Jr. Social isolation in older adults: An evolutionary concept analysis. J. Adv. Nurs. 2009, 65, 1342–1352. [Google Scholar] [CrossRef]
- Bar-Hillel, M. The role of sample size in sample evaluation. Organ. Behav. Hum. Perform. 1979, 23, 245–257. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. depressive symptoms | - | |||||
| 2. social isolation | 0.051 *** | - | ||||
| 3. loneliness | 0.526 *** | 0.047 *** | - | |||
| 4. vigorous physical activity | −0.007 | −0.037 ** | 0.015 | - | ||
| 5. moderate physical activity | −0.042 ** | −0.016 | −0.004 | 0.247 *** | - | |
| 6. mild physical activity | −0.044 *** | 0.014 | 0.003 | 0.146 *** | 0.434 *** | - |
| M | 2.086 | 0.743 | 5.530 | 2.010 | 3.216 | 3.458 |
| SD | 2.339 | 0.472 | 2.018 | 1.249 | 1.163 | 0.986 |
| B | SE | t | 95% CI | |||
|---|---|---|---|---|---|---|
| LLCI | ULCI | |||||
| DV: loneliness (R = 0.475, R2 = 0.225, MSE = 3.161, F = 171.560 ***) | ||||||
| social isolation | 0.184 | 0.048 | 3.808 *** | 0.089 | 0.279 | |
| DV depressive symptoms (R = 0.735, R2 = 0.540, MSE = 2.535, F = 506.441 ***) | ||||||
| social isolation | 0.428 | 0.130 | 3.306 ** | 0.174 | 0.682 | |
| loneliness | 0.614 | 0.026 | 23.551 *** | 0.563 | 0.665 | |
| moderate physical activity | 0.128 | 0.056 | 2.289 * | 0.018 | 0.237 | |
| social isolation × moderate physical activity | −0.099 | 0.037 | −2.662 ** | −0.173 | −0.026 | |
| loneliness × moderate physical activity | −0.021 | 0.008 | −2.615 ** | −0.036 | −0.005 | |
| Index of moderated mediation | SE | 95% CI | ||||
| LLCI | ULCI | |||||
| −0.004 | 0.002 | −0.008 | −0.001 | |||
| B | SE | t | 95% CI | |||
|---|---|---|---|---|---|---|
| LLCI | ULCI | |||||
| DV: loneliness (R = 0.475, R2 = 0.225, MSE = 3.161, F = 171.560 ***) | ||||||
| social isolation | 0.184 | 0.048 | 3.808 *** | 0.089 | 0.279 | |
| DV depressive symptoms (R = 0.734, R2 = 0.539, MSE = 2.527, F = 505.533 ***) | ||||||
| social isolation | 0.054 | 0.152 | 0.353 | 0.174 | 0. 682 | |
| loneliness | 0.624 | 0.032 | 19.244 *** | 0.563 | 0.665 | |
| mild physical activity | 0.025 | 0.064 | 0.385 | 0.018 | 0.237 | |
| social isolation × mild physical activity | 0.016 | 0.042 | 0.384 | −0.173 | −0.026 | |
| loneliness × mild physical activity | −0.022 | 0.009 | −2.357 * | −0.036 | −0.005 | |
| Index of moderated mediation | SE | 95% CI | ||||
| LLCI | ULCI | |||||
| −0.004 | 0.002 | −0.009 | −0.001 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, M.J.; Bae, S.M. The Effect of Social Isolation, Loneliness, and Physical Activity on Depressive Symptoms of Older Adults during COVID-19: A Moderated Mediation Analysis. Int. J. Environ. Res. Public Health 2024, 21, 26. https://doi.org/10.3390/ijerph21010026
Jin MJ, Bae SM. The Effect of Social Isolation, Loneliness, and Physical Activity on Depressive Symptoms of Older Adults during COVID-19: A Moderated Mediation Analysis. International Journal of Environmental Research and Public Health. 2024; 21(1):26. https://doi.org/10.3390/ijerph21010026
Chicago/Turabian StyleJin, Min Jin, and Sung Man Bae. 2024. "The Effect of Social Isolation, Loneliness, and Physical Activity on Depressive Symptoms of Older Adults during COVID-19: A Moderated Mediation Analysis" International Journal of Environmental Research and Public Health 21, no. 1: 26. https://doi.org/10.3390/ijerph21010026
APA StyleJin, M. J., & Bae, S. M. (2024). The Effect of Social Isolation, Loneliness, and Physical Activity on Depressive Symptoms of Older Adults during COVID-19: A Moderated Mediation Analysis. International Journal of Environmental Research and Public Health, 21(1), 26. https://doi.org/10.3390/ijerph21010026