
Effect of Training for an Athletic Challenge on Illness Cognition in Individuals with Chronic Disability: A Prospective Cohort Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
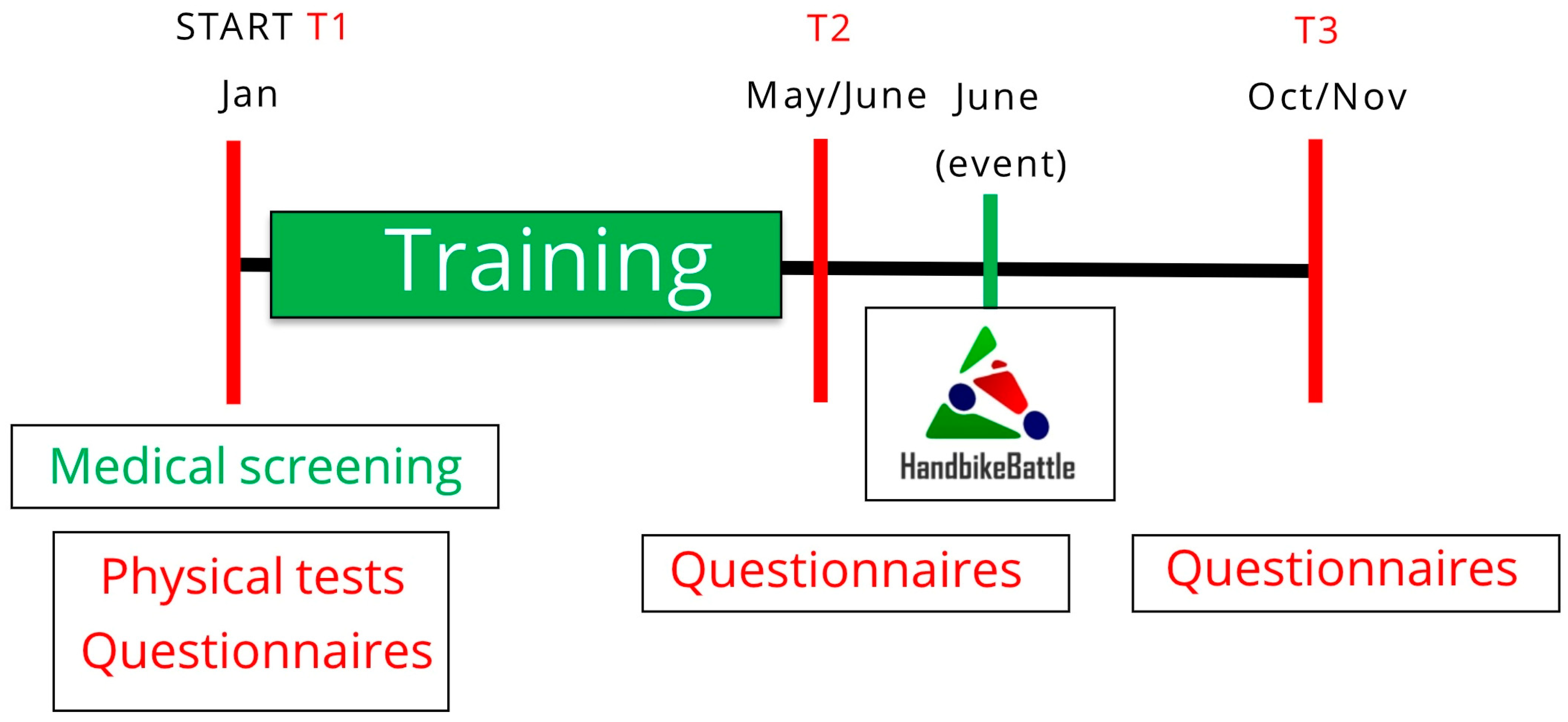
2.1. The HandbikeBattle
2.2. Participants
2.3. Data Collection
2.4. Questionnaires
2.4.1. Illness Cognition Questionnaire
2.4.2. Mental Health Inventory
2.4.3. Self-Efficacy
2.4.4. Pain Assessment
2.4.5. Sports Participation
2.5. Physical Determinants
2.5.1. Disability Etiology
2.5.2. SCI Lesion Characteristics
2.5.3. Time Since Injury
2.5.4. Physical Fitness
2.5.5. Body Mass Index
2.6. Statistical Analysis
3. Results
3.1. Longitudinal Changes in Illness Cognition
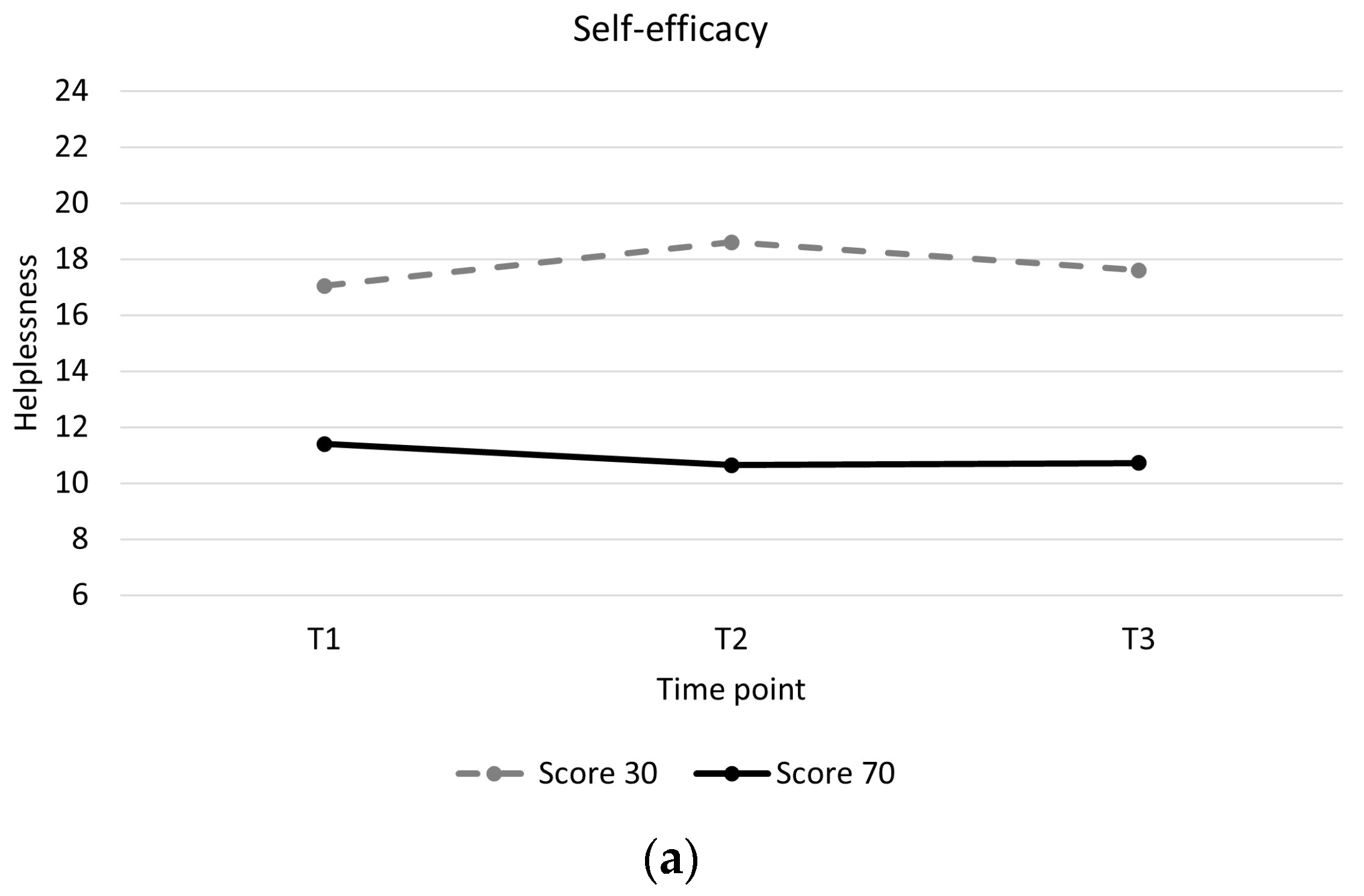
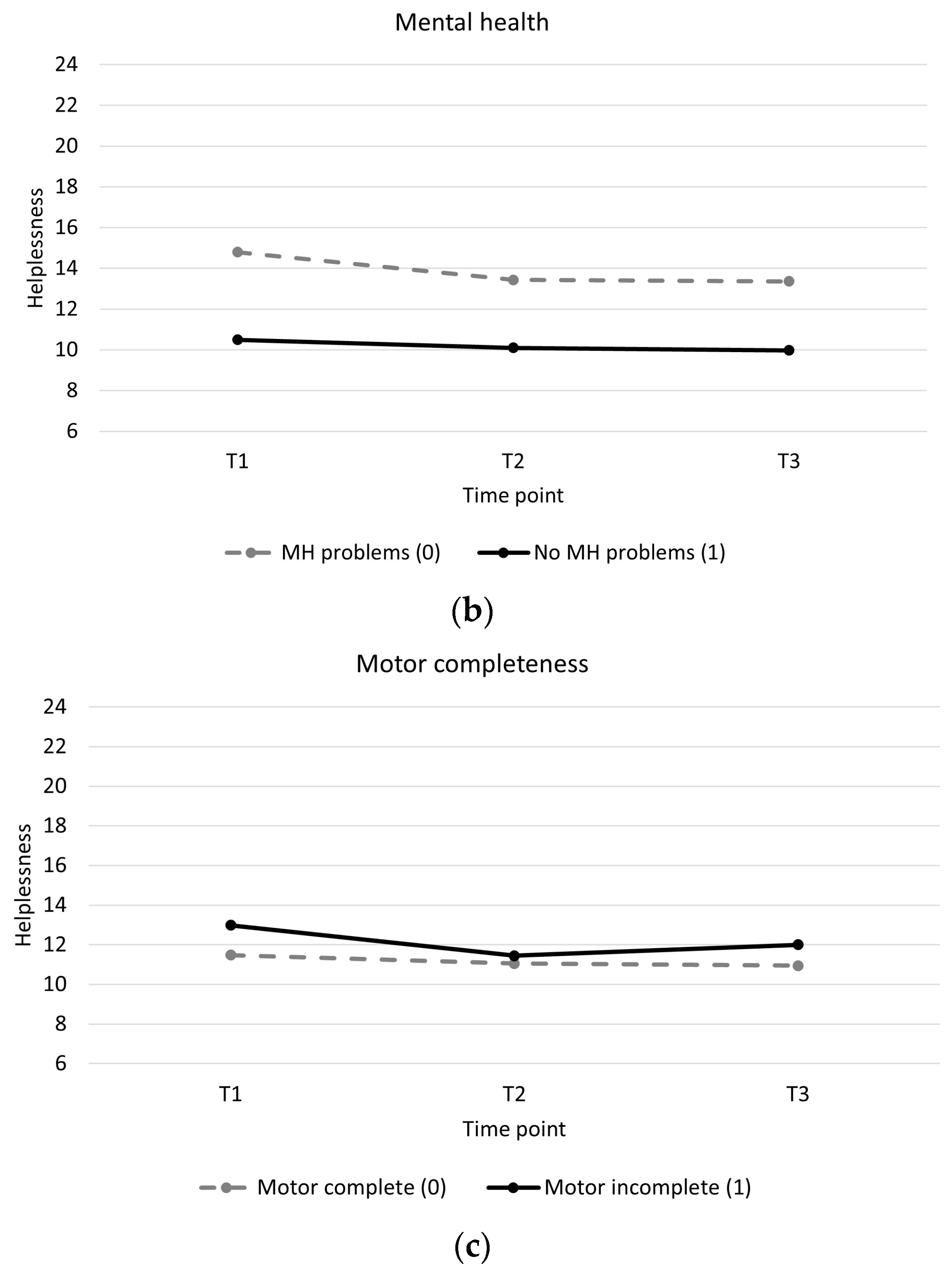
3.2. Factors Associated with Change in Illness Cognition
4. Discussion
4.1. Practical Implications
4.2. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Koppenhagen, C.F.; Post, M.W.M.; van der Woude, L.H.V.; de Witte, L.P. Changes and Determinants of Life Satisfaction After Spinal Cord Injury: A Cohort Study in The Netherlands. Arch. Phys. Med. Rehabil. 2008, 89, 1733–1740. [Google Scholar] [CrossRef] [PubMed]
- Dijkers, M.P.J.M. Quality of life of individuals with spinal cord injury: A review of conceptualization, measurement, and research findings. JRRD 2005, 42, 87–110. [Google Scholar] [CrossRef] [PubMed]
- Craig, A.; Tran, Y.; Middleton, J. Psychological morbidity and spinal cord injury: A systematic review. Spinal Cord 2009, 47, 108–114. [Google Scholar] [CrossRef] [PubMed]
- North, N.T. The psychological effects of spinal cord injury: A review. J. Spinal Cord Med. 1999, 37, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Petrie, K.J.; Broadbent, E.; Kydd, R. Illness perceptions in mental health: Issues and potential applications. J. Ment. Health 2008, 17, 559–564. [Google Scholar] [CrossRef]
- Evers, A.W.M.; Kraaimaat, F.W.; van Lankveld, W.; Jongen, P.J.H.; Jacobs, J.W.G.; Bijlsma, J.W.J. Beyond unfavorable thinking: The Illness Cognition Questionnaire for chronic diseases. J. Consult. Clin. Psychol. 2001, 69, 1026–1036. [Google Scholar] [CrossRef]
- Broadbent, E.; Petrie, K.J.; Main, J.; Weinman, J. The Brief Illness Perception Questionnaire. J. Psychosom. Res. 2006, 60, 631–637. [Google Scholar] [CrossRef]
- Shabany, M.; Ghodsi, S.M.; Arejan, R.H.; Baigi, V.; Ghodsi, Z.; Rakhshani, F.; Gholami, M.; Sharif, P.M.; Shool, S.; Vaccaro, A.R.; et al. Cognitive appraisals of disability in persons with traumatic spinal cord injury: A scoping review. Spinal Cord 2022, 60, 954–962. [Google Scholar] [CrossRef]
- Russell, M.; Ames, H.; Dunn, C.; Beckwith, S.; Holmes, S.A. Appraisals of disability and psychological adjustment in veterans with spinal cord injuries. J. Spinal Cord Med. 2021, 44, 958–965. [Google Scholar] [CrossRef]
- Kennedy, P.; Evans, M.; Sandhu, N. Psychological adjustment to spinal cord injury: The contribution of coping, hope and cognitive appraisals. Psychol. Health Med. 2009, 14, 17–33. [Google Scholar] [CrossRef]
- Van Leeuwen, C.M.C.; Post, M.W.M.; Westers, P.; van der Woude, L.H.V. Relationships Between Activities, Participation, Personal Factors, Mental Health, and Life Satisfaction in Persons with Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2012, 93, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Wollaars, M.M.; Post, M.W.M.; van Asbeck, F.W.A.; Brand, N. Spinal Cord Injury Pain: The Influence of Psychologic Factors and Impact on Quality of Life. Clin. J. Pain 2007, 23, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, C.M.C.; Edelaar-Peeters, Y.; Peter, C.; Stiggelbout, A.M.; Post, M.W.M. Psychological factors and mental health in persons with spinal cord injury: An exploration of change or stability. J. Rehabil. Med. 2015, 47, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Kuiper, H.; van Leeuwen, C.M.C.; Stolwijk-Swüste, J.M.; Post, M.W.M. Illness perception of individuals with spinal cord injury (SCI) during inpatient rehabilitation: A longitudinal study. Spinal Cord 2022, 60, 831–836. [Google Scholar] [CrossRef]
- Jones, C.J.; Smith, H.E.; Llewellyn, C.D. A systematic review of the effectiveness of interventions using the Common Sense Self-Regulatory Model to improve adherence behaviours. J. Health Psychol. 2016, 21, 2709–2724. [Google Scholar] [CrossRef]
- Mülhauser, S.; Bonhote Börner, M.; Saner, H.; Zumstein-Shaha, M. The impact of motivational interviewing on illness perception in patients with stable coronary artery disease-a randomised controlled study. Pflege 2018, 31, 75–85. [Google Scholar] [CrossRef]
- Dalili, Z.; Bayazi, M.H. The effectiveness of Mindfulness-Based Cognitive Therapy on the illness perception and Psychological Symptoms in patients with Rheumatoid Arthritis. Complement. Ther. Clin. Pract. 2019, 34, 139–144. [Google Scholar] [CrossRef]
- Sararoudi, R.B.; Motmaen, M.; Maracy, M.R.; Pishghadam, E.; Kheirabadi, G.R. Efficacy of illness perception focused intervention on quality of life, anxiety, and depression in patients with myocardial infarction. J. Res. Med. Sci. 2016, 21, 125. [Google Scholar] [CrossRef]
- Weldam, S.W.M.; Schuurmans, M.J.; Zanen, P.; Heijmans, M.J.W.M.; Sachs, A.P.E.; Lammers, J.W.J. The effectiveness of a nurse-led illness perception intervention in COPD patients: A cluster randomised trial in primary care. ERJ Open Res. 2017, 3, 115–2016. [Google Scholar] [CrossRef]
- Côté-Leclerc, F.; Boileau Duchesne, G.; Bolduc, P.; Gëlinas-Lafreniere, A.; Santerre, C.; Desrosiers, J.; Levasseur, M. How does playing adapted sports affect quality of life of people with mobility limitations? Results from a mixed-method sequential explanatory study. Health Qual. Life Outcomes 2017, 15, 1–8. [Google Scholar] [CrossRef]
- Sporner, M.L.; Fitzgerald, S.G.; DiCianno, B.E.; Collins, D.; Teodorski, E.; Pasquina, P.F.; Cooper, R.A. Psychosocial impact of participation in the National Veterans Wheelchair Games and Winter Sports Clinic. Disabil. Rehabil. 2009, 31, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Ashton-Shaeffer, C.; Gibson, H.; Holt, M.; Willming, C. Women’s resistance and empowerment through wheelchair sport. World Leisure 2001, 4, 11–21. [Google Scholar] [CrossRef]
- Kouwijzer, I.; de Groot, S.; van Leeuwen, C.M.C.; Valent, L.J.M.; Stolwijk-Swüste, J.M.; HandbikeBattle group; van der Woude, L.H.V.; Post, M.W.M. Changes in body satisfaction during and after a 5-month handcycle training period and associations with physical capacity and body composition in individuals with a physical impairment. Disabil. Rehabil. 2023. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Kouwijzer, I.; de Groot, S.; van Leeuwen, C.M.C.; Valent, L.J.M.; van Koppenhagen, C.F.; HandbikeBattle group; van der Woude, L.H.V.; Post, M.W.M. Changes in Quality of Life During Training for the HandbikeBattle and Associations With Cardiorespiratory Fitness. Arch. Phys. Med. Rehabil. 2020, 101, 1017–1024. [Google Scholar] [CrossRef]
- Treharne, G.J.; Kitas, G.D.; Lyons, A.C.; Booth, D.A. Well-being in rheumatoid arthritis: The effects of disease duration and psychosocial factors. J. Health Psychol. 2005, 10, 457–474. [Google Scholar] [CrossRef] [PubMed]
- Maas, M.; Taal, E.; van der Linden, S.; Boonen, A. A review of instruments to assess illness representations in patients with rheumatic diseases. Ann. Rheum. Dis. 2009, 68, 305–309. [Google Scholar] [CrossRef]
- Sawyer, A.T.; Harris, S.L.; Koenig, H.G. Illness perception and high readmission health outcomes. Health Psychol. Open 2019, 6, 2055102919844504. [Google Scholar] [CrossRef]
- De Raaij, E.J.; Ostelo, R.W.; Maissan, F.; Mollema, J.; Wittink, H. The association of illness perception and prognosis for pain and physical function in patients with noncancer musculoskeletal pain: A systematic literature review. J. Orthop. Sports Phys. Ther. 2018, 48, 789–800. [Google Scholar] [CrossRef]
- Arat, S.; de Cock, D.; Moons, P.; Vandenberghe, J.; Westhovens, R. Modifiable correlates of illness perceptions in adults with chronic somatic conditions: A systematic review. Res. Nurs. Health 2018, 41, 173–184. [Google Scholar] [CrossRef]
- Han, J.; Liu, J.E.; Qiu, H.; Nie, Z.H.; Su, Y.L. Illness cognitions and the associated socio-demographic and clinical factors in Chinese women with breast cancer. Eur. J. Oncol. Nurs. 2018, 32, 33–39. [Google Scholar] [CrossRef]
- Chao, H.L.; Tsai, T.Y.; Livneh, H.; Lee, H.C.; Hsieh, P.C. Patients with colorectal cancer: Relationship between demographic and disease characteristics and acceptance of disability. J. Adv. Nurs. 2010, 66, 2278–2286. [Google Scholar] [CrossRef] [PubMed]
- Lauwerier, E.; Crombez, G.; van Damme, S.; Goubert, L.; Vogelaers, D.; Evers, A.W.M. The construct validity of the Illness Cognition Questionnaire: The robustness of the three-factor structure across patients with chronic pain and chronic fatigue. Int. J. Behav. Med. 2010, 17, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Chaiamnuay, S.; Bertoli, A.M.; Fernandez, M.; Apte, M.; Vila, L.M.; Reveille, J.D.; Alarcon, G.S.; LUMINA study group. The impact of increased body mass index on systemic lupus erythematosus: Data from LUMINA, a multiethnic cohort. J. Clin. Rheumatol. 2007, 13, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Tığlı, A.; Soy, E.H.A.; Aytar, A.; Moray, G.; Haberal, M. Relationship between exercise perception with physical activity level, body awareness, and illness cognition in renal transplant patients: A pilot study. Exp. Clin. Transplant. 2019, 17, 270–276. [Google Scholar] [CrossRef]
- Lupash, E.; Ehrman, J.J. (Eds.) ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Voerman, G.E.; Erren-Wolters, C.V.; Fleuren, J.F.; Hermens, H.J.; Geurts, A.C. Perceived spasticity in chronic spinal cord injured patients: Associations with psychological factors. Disabil. Rehabil. 2010, 32, 775–780. [Google Scholar] [CrossRef] [PubMed]
- Hoeymans, N.; Garssen, A.A.; Westert, G.P.; Verhaak, P.F.M. Measuring mental health of the Dutch population: A comparison of the GHQ-12 and the MHI-5. Health Qual. Life Outcomes 2004, 36, 1–6. [Google Scholar]
- Van Leeuwen, C.M.C.; van der Woude, L.H.V.; Post, M.W.M. Validity of the mental health subscale of the SF-36 in persons with spinal cord injury. Spinal Cord 2012, 50, 707–710. [Google Scholar] [CrossRef]
- Bosscher, R.J.; Smit, J.H. Confirmatory factor analysis of the general self-efficacy scale. Behav. Res. Ther. 1998, 36, 339–343. [Google Scholar] [CrossRef]
- Sherer, M.; Maddux, J.E.; Mercandante, B.; Prentice-Dunn, S.; Jacobs, B.; Rogers, R.W. The self-efficacy scale: Construction and validation. Psychol. Rep. 1982, 51, 663–671. [Google Scholar] [CrossRef]
- Van Drongelen, S.; De Groot, S.; Veeger, H.E.J.; Angenot, E.L.D.; Dallmeijer, A.J.; Post, M.W.M.; Van Der Woude, L.H.V. Upper extremity musculoskeletal pain during and after rehabilitation in wheelchair-using persons with a spinal cord injury. Spinal Cord 2006, 44, 152–159. [Google Scholar] [CrossRef]
- Kirshblum, S.C.; Burns, S.P.; Biering-Sorensen, F.; Donovan, W.; Graves, D.E.; Jha, A.; Johansen, M.; Jones, L.; Krassioukov, A.; Mulcahey, M.J.; et al. International standards for neurological classification of spinal cord injury (Revised 2011). J. Spinal Cord Med. 2011, 34, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Rasbash, J.; Charlton, C.; Browne, W.J.; Healy, M.; Cameron, B. MLwiN Version 2.36. Centre for Multilevel Modelling, University of Bristol. 2005. Available online: https://www.bristol.ac.uk/cmm/software/mlwin/refs.html (accessed on 6 October 2023).
- Maas, C.J.M.; Snijders, T.A.B. The Multilevel Approach to Repeated Measures for Complete and Incomplete Data. Qual. Quant. 2003, 37, 71–89. [Google Scholar] [CrossRef]
- Van Mierlo, M.L.; van Heugten, C.M.; Post, M.W.M.; de Kort, P.L.M.; Visser-Meily, J.M.A. Life satisfaction post stroke: The role of illness cognitions. J. Psychosom. Res. 2015, 79, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Callahan, L.F.; Shreffler, J.H.; Altpeter, M.; Schoster, B.; Hootman, J.; Houenou, L.O.; Martin, K.R.; Schwartz, T.A. Evaluation of group and self-directed formats of the arthritis foundation’s Walk with Ease program. Arthritis Care Res. 2011, 63, 1098–1107. [Google Scholar] [CrossRef] [PubMed]
- Silverman, M.N.; Deuster, P.A. Biological mechanisms underlying the role of physical fitness in health and resilience. Interface Focus 2014, 4, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, B.N.; Fleshner, M. Exercise, learned helplessness, and the stress-resistant brain. Neuro Mol. Med. 2008, 10, 81–98. [Google Scholar] [CrossRef] [PubMed]
- Hicks, A.L.; Martin, K.A.; Ditor, D.S.; Latimer, A.E.; Craven, C.; Bugaresti, J.; McCartney, N. Long-term exercise training in persons with spinal cord injury: Effects on strength, arm ergometry performance and psychological well-being. Spinal Cord 2003, 41, 34–43. [Google Scholar] [CrossRef]
- Motl, R.W.; McAuley, E. Pathways Between Physical Activity and Quality of Life in Adults with Multiple Sclerosis. Health Psychol. 2009, 28, 682–689. [Google Scholar] [CrossRef]
- Sweet, S.N.; Martin Ginis, K.A.; Tomasone, J.R. Investigating Intermediary Variables in the Physical Activity and Quality of Life Relationship in Persons With Spinal Cord Injury. Health Psychol. 2013, 32, 877–885. [Google Scholar] [CrossRef]
- Haisma, J.A.; Post, M.W.M.; van der Woude, L.H.V.; Stam, H.J.; Bergen, M.P.; Sluis, T.A.; van den Berg-Emons, H.J.; Bussmann, J.B. Functional independence and health-related functional status following spinal cord injury: A prospective study of the association with pfysical capacity. J. Rehabil. Med. 2008, 40, 812–818. [Google Scholar] [CrossRef]
- Martin Ginis, K.A.; Jetha, A.; Mack, D.E.; Hetz, S. Physical activity and subjective well-being among people with spinal cord injury: A meta-analysis. Spinal Cord 2010, 48, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Aaby, A.; Lykkegaard Ravn, S.; Kasch, H.; Andersen, T.E. The associations of acceptance with quality of life and mental health following spinal cord injury: A systematic review. Spinal Cord 2020, 58, 130–148. [Google Scholar] [CrossRef] [PubMed]
- Moyano, S.; Scolnik, M.; Vergara, F.; Garcia, M.V.; Sabelli, M.R.; Rosa, J.E.; Catoggio, L.J.; Soriano, E.R. Evaluation of Learned Helplessness, Perceived Self-efficacy, and Functional Capacity in Patients with Fibromyalgia and Rheumatoid Arthritis. J. Clin. Rheumatol. 2019, 25, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Calderon, J.; Meeus, M.; Struyf, F.; Luque-Suarez, A. The role of self-efficacy in pain intensity, function, psychological factors, health behaviors, and quality of life in people with rheumatoid arthritis: A systematic review. Physiother. Theory Pract. 2020, 36, 21–37. [Google Scholar] [CrossRef]
- La Touche, R.; Grande-Alonso, M.; Arnés-Prieto, P.; Paris-Alemany, A. How does self-efficacy influence pain perception, postural stability and range of motion in individuals with chronic low back pain? Pain Physician 2019, 22, E1–E13. [Google Scholar] [CrossRef]
- Schulz, U.; Mohamed, N.E. Turning the tide: Benefit finding after cancer surgery. Soc. Sci. Med. 2004, 59, 653–662. [Google Scholar] [CrossRef]
- Ames, H.; Wilson, C.; Barnett, S.D.; Njoh, E.; Ottomanelli, L. Does functional motor incomplete (AIS D) spinal cord injury confer unanticipated challenges? Rehabil. Psychol. 2017, 62, 401–406. [Google Scholar] [CrossRef]
- Prince, S.A.; Adamo, K.B.; Hamel, M.; Hardt, J.; Connor Gorber, S.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | N | Participants | N | Non-Participants | ||
|---|---|---|---|---|---|---|
| Sex (male/female) (%male) | 220 | 164/56 | (75%) | 99 | 75/24 | (76%) |
| Age (years) | 220 | 41 ± 13 * | 97 | 36 ± 12 * | ||
| Disability etiology | 220 | 91 | ||||
| Spinal cord injury/Spina bifida | 151 | (69%) | 64 | (70%) | ||
| Other | 69 | (31%) | 27 | (30%) | ||
| Time since injury (years) | 199 | 12 ± 13 | 79 | 13 ± 13 | ||
| <2 years | 39 | (19%) | 11 | (14%) | ||
| 2–9 years | 71 | (36%) | 28 | (35%) | ||
| >9 years | 89 | (45%) | 40 | (51%) | ||
| Body Mass Index (kg/m2) | 210 | 24.6 ± 4.5 | 77 | 24.9 ± 5.6 | ||
| POpeak (W) | 189 | 117 ± 37 * | 70 | 104 ± 34 * | ||
| Self-efficacy | 121 | 68.8 ± 9.0 | 20 | 63.3 ± 12.8 | ||
| Illness Cognition | ||||||
| Helplessness | 200 | 12.0 ± 3.9 | 38 | 11.1 ± 4.2 | ||
| Acceptance | 199 | 18.7 ± 4.1 | 38 | 18.3 ± 4.7 | ||
| Perceived benefits | 199 | 17.1 ± 4.8 | 38 | 17.9 ± 4.4 | ||
| Mental Health Inventory | 200 | 76.5 ± 15.4 | 39 | 72.1 ± 18.2 | ||
| ≤72 (mental health problems) | 68 | (34%) | 19 | (49%) | ||
| >72 (no mental health problems) | 132 | (66%) | 20 | (51%) | ||
| Musculoskeletal pain (no-mild/moderate-severe) (%no-mild) | 120/79 | (60%) | 23/18 | (56%) | ||
| Completeness of injury (SCI only) | 131 | 53 | ||||
| Motor complete | 86 | (66%) | 33 | (62%) | ||
| Motor incomplete | 45 | (34%) | 20 | (38%) | ||
| Level of injury (SCI only) | 135 | 57 | ||||
| Tetraplegia | 21 | (16%) | 11 | (19%) | ||
| Paraplegia | 114 | (84%) | 46 | (81%) | ||
| T1 | T2 | T3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| N | Mean ± SD | Median [IQR] | N | Mean ± SD | Median [IQR] | N | Mean ± SD | Median [IQR] | |
| Helplessness (6–24) | 200 | 12.0 ± 3.9 | 11.0 [9.0–14.8] | 207 | 11.3 ± 3.8 | 11.0 [9.0–13.0] | 179 | 11.1 ± 3.8 | 10.0 [8.0–13.0] |
| Acceptance (6–24) | 199 | 18.7 ± 4.1 | 19.0 [16.0–22.0] | 206 | 18.8 ± 3.9 | 19.0 [16.0–22.0] | 179 | 18.8 ± 3.9 | 19.0 [16.0–22.0] |
| Perceived benefits (6–24) | 199 | 17.1 ± 4.8 | 17.0 [14.0–21.0] | 206 | 17.6 ± 4.8 | 18.0 [14.0–22.0] | 178 | 17.2 ± 4.7 | 17.0 [14.0–21.3] |
| Helplessness | Acceptance | Perceived Benefits | ||||
|---|---|---|---|---|---|---|
| Beta (SE) | p-Value | Beta (SE) | p-Value | Beta (SE) | p-Value | |
| Constant (reference T2) | 11.277 (0.262) | 18.806 (0.270) | 17.577 (0.324) | |||
| ∆ T2–T1 | 0.678 (0.187) | <0.01 * | −0.245 (0.201) | 0.22 | −0.669 (0.219) | <0.01 * |
| ∆ T2–T3 | −0.121 (0.195) | 0.53 | −0.086 (0.209) | 0.68 | −0.338 (0.229) | 0.14 |
| Constant (reference T1) | 11.956 (0.263) | 18.560 (0.271) | 16.908 (0.326) | |||
| ∆ T1–T2 | −0.678 (0.187) | <0.01 * | 0.245 (0.201) | 0.22 | 0.669 (0.219) | <0.01 * |
| ∆ T1–T3 | −0.800 (0.198) | <0.01 * | 0.160 (0.212) | 0.45 | 0.331 (0.232) | 0.15 |
| Determinants | Constant (Reference:T2) | ∆ T2–T1 | ∆ T2–T3 | Determinant | (∆ T2–T1) × Determinant | (∆ T2–T3) × Determinant |
|---|---|---|---|---|---|---|
| Sex (reference: male) | 11.411 (0.302) | 0.565 (0.215) * | −0.145 (0.227) | −0.536 (0.602) | 0.455 (0.432) | 0.120 (0.440) |
| Age, years | 9.720 (0.864) | 0.923 (0.628) | −0.386 (0.653) | 0.038 (0.020) | −0.006 (0.014) | 0.006 (0.015) |
| Disability etiology (reference: SCI/SB) | 11.189 (0.315) | 0.629 (0.222) * | 0.054 (0.239) | 0.283 (0.563) | 0.180 (0.408) | −0.503 (0.412) |
| Time since injury (years) | 11.503 (0.365) | 1.030 (0.270) * | −0.131 (0.275) | −0.026 (0.021) | −0.025 (0.015) | 0.003 (0.015) |
| Body Mass Index, kg/m2 | 8.165 (1.449) | −0.215 (1.044) | 0.301 (1.154) | 0.126 (0.058) * | 0.036 (0.042) | −0.016 (0.046) |
| POpeak (W) | 11.630 (0.943) | 0.796 (0.692) | 0.764 (0.707) | −0.002 (0.008) | −0.001 (0.006) | −0.008 (0.006) |
| Self-efficacy | 24.569 (2.573) | −3.299 (1.769) | −1.811 (1.929) | −0.199 (0.037) * | 0.058 (0.025) * | 0.027 (0.028) |
| Mental Health (reference: ≤72 (mental health problems)) | 13.439 (0.417) | 1.355 (0.322) * | 0.192 (0.361) | −3.337 (0.514) * | −0.960 (0.398) * | −0.315 (0.440) |
| Musculoskeletal pain (reference: no-mild pain) | 10.836 (0.352) | 0.669 (0.247) * | 0.117 (0.272) | 1.074 (0.558) | 0.143 (0.392) | −0.341 (0.425) |
| Lesion completeness (reference: motor complete) | 11.047 (0.385) | 0.435 (0.263) | −0.097 (0.289) | 0.401 (0.659) | 1.101 (0.460) * | 0.652 (0.478) |
| Level of injury (reference: tetraplegia) | 10.283 (0.786) | 1.320 (0.556) * | 0.461 (0.568) | 1.138 (0.855) | −0.629 (0.601) | −0.395 (0.619) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
DeShazo, J.M.; Kouwijzer, I.; de Groot, S.; Post, M.W.M.; Valent, L.J.M.; van Leeuwen, C.M.C.; Wen, H.; Cowan, R.E.; on behalf of the HandbikeBattle Group. Effect of Training for an Athletic Challenge on Illness Cognition in Individuals with Chronic Disability: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2024, 21, 58. https://doi.org/10.3390/ijerph21010058
DeShazo JM, Kouwijzer I, de Groot S, Post MWM, Valent LJM, van Leeuwen CMC, Wen H, Cowan RE, on behalf of the HandbikeBattle Group. Effect of Training for an Athletic Challenge on Illness Cognition in Individuals with Chronic Disability: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2024; 21(1):58. https://doi.org/10.3390/ijerph21010058
Chicago/Turabian StyleDeShazo, Joy M., Ingrid Kouwijzer, Sonja de Groot, Marcel W. M. Post, Linda J. M. Valent, Christel M. C. van Leeuwen, Huacong Wen, Rachel E. Cowan, and on behalf of the HandbikeBattle Group. 2024. "Effect of Training for an Athletic Challenge on Illness Cognition in Individuals with Chronic Disability: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 21, no. 1: 58. https://doi.org/10.3390/ijerph21010058
APA StyleDeShazo, J. M., Kouwijzer, I., de Groot, S., Post, M. W. M., Valent, L. J. M., van Leeuwen, C. M. C., Wen, H., Cowan, R. E., & on behalf of the HandbikeBattle Group. (2024). Effect of Training for an Athletic Challenge on Illness Cognition in Individuals with Chronic Disability: A Prospective Cohort Study. International Journal of Environmental Research and Public Health, 21(1), 58. https://doi.org/10.3390/ijerph21010058