
A Dynamic Model of Opioid Overdose Deaths in Canada during the Co-Occurring Opioid Overdose Crisis and COVID-19 Pandemic

Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Belzak, L.; Halverson, J. Evidence synthesis–The opioid crisis in Canada: A national perspective. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2018, 38, 224. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada. Opioid- and Stimulant-Related Harms [Internet]. 2022. Available online: https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/ (accessed on 27 January 2023).
- Enns, A.; Pinto, A.; Venugopal, J.; Grywacheski, V.; Gheorghe, M.; Kakkar, T. Evidence-informed policy brief substance use and related harms in the context of COVID-19: A conceptual model. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2020, 40, 342–349. [Google Scholar]
- Jalali, M.S.; Botticelli, M.; Hwang, R.C.; Koh, H.K.; McHugh, R.K. The opioid crisis: A contextual, social-ecological framework. Health Res Policy Syst. 2020, 18, 87. [Google Scholar] [CrossRef] [PubMed]
- Luke, D.A.; Stamatakis, K.A. Systems science methods in public health: Dynamics, networks, and agents. Annu. Rev. Public Health 2012, 33, 357–376. [Google Scholar] [CrossRef] [PubMed]
- Jalali, M.S.; Botticelli, M.; Hwang, R.C.; Koh, H.K.; McHugh, R.K. The opioid crisis: Need for systems science research. Health Res. Policy Syst. 2020, 18, 88. [Google Scholar] [CrossRef]
- Cerdá, M.; Jalali, M.S.; Hamilton, A.D.; Digennaro, C.; Hyder, A.; Santaella-Tenorio, J.; Kaur, N.; Wang, C.; Keyes, K.M. A systematic review of simulation models to track and address the opioid crisis. Epidemiol. Rev. 2021, 43, 147–165. [Google Scholar] [CrossRef] [PubMed]
- Sharareh, N.; Sabounchi, S.S.; McFarland, M.; Hess, R. Evidence of modeling impact in development of policies for controlling the opioid epidemic and improving public health: A scoping review. Subst. Abus. 2019, 13. [Google Scholar] [CrossRef] [PubMed]
- Baia Medeiros, D.T.; Hahn-Goldberg, S.; Aleman, D.M.; O’Connor, E. Planning capacity for mental health and addiction services in the emergency department: A discrete-event simulation approach. J. Healthc. Eng. 2019, 2019, 8973515. [Google Scholar] [PubMed]
- McGregor, M.; Nielsen, A.; Chung, C.; Fillery, M.D.; Wakeland, W.; Mior, S. System dynamics to investigate opioid use and chiropractic care for chronic musculoskeletal pain. J. Manip. Physiol. Ther. 2019, 42, 237–246. [Google Scholar]
- Marks, C.I.; Borquez, A.I.; Jain, S.; Sun, X.; Strathdee, S.A.; Garfein, R.S.; Milloy, M.J.; DeBeck, K.; Cepeda, J.A.; Werb, D.; et al. Opioid agonist treatment scale-up and the initiation of injection drug use: A dynamic modeling analysis. PLoS Med. 2019, 16, e1002973. [Google Scholar] [CrossRef]
- Irvine, M.A.; Kuo, M.; Buxton, J.A.; Balshaw, R.; Otterstatter, M.; Macdougall, L.; Milloy, M.J.; Bharmal, A.; Henry, B.; Tyndall, M.; et al. Modelling the combined impact of interventions in averting deaths during a synthetic-opioid overdose epidemic. Addiction 2019, 114, 1602–1613. [Google Scholar] [CrossRef] [PubMed]
- Becker, W.C.; Fiellin, D.A. When epidemics collide: Coronavirus Disease 2019 (COVID-19) and the Opioid Crisis. Ann. Intern. Med. 2020, 173, 59–60. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, A.; Lokuge, B.; Masters, D.; Sequeira, M.; Saul, P.; Dunlop, G.; Ryan, J.; Hall, M.; Ezard, N.; Haber, P.; et al. Challenges in maintaining treatment services for people who use drugs during the COVID-19 pandemic. Harm Reduct. J. 2020, 17, 26. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Population estimates on July 1st, by age and sex. 2023. [Internet]. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1710000501 (accessed on 27 January 2023).
- Canadian Institute for Health Information. Opioid Prescribing in Canada: How Are Practices Changing? [Internet]. 2019. Available online: https://www.cihi.ca/sites/default/files/document/opioid-prescribing-canada-trends-en-web.pdf (accessed on 27 January 2023).
- Statistics Canada. Statistics Canada. Pain Relief Medication Containing Opioids, 2018 [Internet]. Health Fact Sheets. Available online: https://www150.statcan.gc.ca/n1/pub/82-625-x/2019001/article/00008-eng.htm (accessed on 27 January 2023).
- Popova, S.; Patra, J.; Mohapatra, S.; Fischer, B.; Rehm, J. How many people in Canada use prescription opioids nonmedically in general and street drug using populations? Can. J. Public Health 2009, 100, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Popova, S.; Rehm, J.; Fischer, B. An overview of illegal opioid use and health services utilization in Canada. Public Health 2006, 120, 320–328. [Google Scholar] [CrossRef]
- Champagne-Langabeer, T.; Madu, R.; Giri, S.; Stotts, A.L.; Langabeer, J.R. Opioid prescribing patterns and overdose deaths in Texas. Subst. Abus. 2019, 42, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Battista, N.A.; Pearcy, L.B.; Strickland, W.C. Modeling the prescription opioid epidemic. Bull Math Biol 2019, 81, 2258–2289. [Google Scholar] [CrossRef] [PubMed]
- Gaither, J.R.; Goulet, J.L.; Becker, W.C.; Crystal, S.; Edelman, E.J.; Gordon, K.; Kerns, R.D.; Rimland, D.; Skanderson, M.; Justice, A.C.; et al. The association between receipt of guideline-concordant long-term opioid therapy and all-cause mortality. J. Gen. Intern. Med. 2016, 31, 492–501. [Google Scholar] [CrossRef]
- Fishbain, D.A.; Cole, B.; Lewis, J.; Rosomoff, H.L.; Rosomoff, R.S. What percentage of chronic nonmalignant pain patients exposed to chronic opioid analgesic therapy develop abuse/addiction and/or aberrant drug-related behaviors? A structured evidence-based review. Pain Med. 2008, 9, 444–459. [Google Scholar] [CrossRef]
- Wakeland, W.; Nielsen, A.; Schmidt, T. System dynamics modeling of medical use, nonmedical use and diversion of prescription opioid analgesics. In Proceedings of the 30th International Conference of the System Dynamics Society, St Gallen, Switzerland, 22–26 July 2012; pp. 1–23. Available online: http://archives.pdx.edu/ds/psu/17635 (accessed on 27 January 2023).
- Calabria, B.; Degenhardt, L.; Briegleb, C.; Vos, T.; Hall, W.; Lynskey, M.; Callaghan, B.; Rana, U.; McLaren, J. Systematic review of prospective studies investigating “remission” from amphetamine, cannabis, cocaine or opioid dependence. Addict. Behav. 2010, 35, 741–749. [Google Scholar] [CrossRef]
- Caldwell, W.K.; Freedman, B.; Settles, L.; Thomas, M.M.; Camacho, E.T.; Wirkus, S. The Vicodin abuse problem: A mathematical approach. J. Theor. Biol. 2019, 483, 110003. [Google Scholar] [CrossRef] [PubMed]
- Kaplovitch, E.; Gomes, T.; Camacho, X.; Dhalla, I.A.; Mamdani, M.M.; Juurlink, D.N. Sex differences in dose escalation and overdose death during chronic opioid therapy: A population-based cohort study. PLoS ONE 2015, 10, e0134550. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Bucello, C.; Mathers, B.; Briegleb, C.; Ali, H.; Hickman, M.; McLaren, J. Mortality among regular or dependent users of heroin and other opioids: A systematic review and meta-analysis of cohort studies. Addiction 2011, 106, 32–51. [Google Scholar] [CrossRef] [PubMed]
- Larney, S.; Peacock, A.; Tran, L.T.; Stockings, E.; Santomauro, D.; Santo, T.; Degenhardt, L. All-cause and overdose mortality risk among people prescribed opioids: A systematic review and meta-analysis. Pain Med. 2020, 21, 3700–3711. [Google Scholar] [CrossRef] [PubMed]
- Analyzed Drug Report—Drug Analysis Service. Public Health Infobase—Public Health Agency of Canada [Internet]. Available online: https://health-infobase.canada.ca/drug-analysis-service/analyzed-drug-report.html (accessed on 30 January 2023).
- Facts about Fentanyl [Internet]. Available online: https://www.dea.gov/resources/facts-about-fentanyl (accessed on 27 January 2023).
- Good Samaritan Drug Overdose Act [Internet]. Available online: https://laws.justice.gc.ca/eng/AnnualStatutes/2017_4/index.html (accessed on 27 January 2023).
- Health Canada. Federal Actions on Opioids to Date—Canada.ca [Internet]. 2022. Available online: https://www.canada.ca/en/health-canada/services/opioids/federal-actions/overview.html (accessed on 27 January 2023).
- Modelling Opioid-Related Deaths during the COVID-19 Outbreak—Canada.ca [Internet]. Available online: https://www.canada.ca/en/health-canada/services/opioids/data-surveillance-research/modelling.html (accessed on 23 March 2024).
- Friesen, E.L.; Kurdyak, P.A.; Gomes, T.; Kolla, G.; Leece, P.; Zhu, L.; Tomb, E.; O’Neill, B.; Stall, N.M.; Juni, P.; et al. The impact of the COVID-19 pandemic on opioid-related harm in Ontario. Sci. Briefs Ont. COVID-19 Sci. Advis. Table 2021, 2. [Google Scholar] [CrossRef]
- Panagiotoglou, D. Evaluating the population-level effects of overdose prevention sites and supervised consumption sites in British Columbia, Canada: Controlled interrupted time series. PLoS ONE 2022, 17, e0265665. [Google Scholar] [CrossRef] [PubMed]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef]
- COVID Policy Tracker: Methodology for calculating indices. [Internet]. Available online: https://github.com/OxCGRT/covid-policy-tracker/blob/master/documentation/index_methodology.md#indices (accessed on 26 February 2023).
- Caulkins, J.P.; Pardo, B.; Kilmer, B. Supervised consumption sites: A nuanced assessment of the causal evidence. Addiction 2019, 114, 2109–2115. [Google Scholar] [CrossRef]
- Hayes, C.J.; Cucciare, M.A.; Martin, B.C.; Hudson, T.J.; Bush, K.; Lo-Ciganic, W.; Yu, H.; Charron, E.; Gordon, A.J. Using data science to improve outcomes for persons with opioid use disorder. Subst. Abus. 2022, 43, 956–963. [Google Scholar] [CrossRef]
- Li, X.; Keeler, B.; Zahan, R.; Duan, L.; Safarishahrbijari, A.; Goertzen, J.; Tian, Y.; Liu, J.; Osgood, N.D. Illuminating the hidden elements and future evolution of opioid abuse using dynamic modeling, Big Data and Particle Markov Chain Monte Carlo. [Internet]. In Proceedings of 2018 International Conference on Social Computing, Behavioral-Cultural Modeling, & Prediction and Behavior Representation in Modeling and Simulation, Washington, DC, USA, 10–13 July 2018; pp. 1–10. Available online: https://sbp-brims.org/2018/proceedings/papers/challenge_papers/Illuminating%20the%20HiddenElements.pdf (accessed on 27 January 2023).




{kind=link}
{kind=link}
{kind=link}
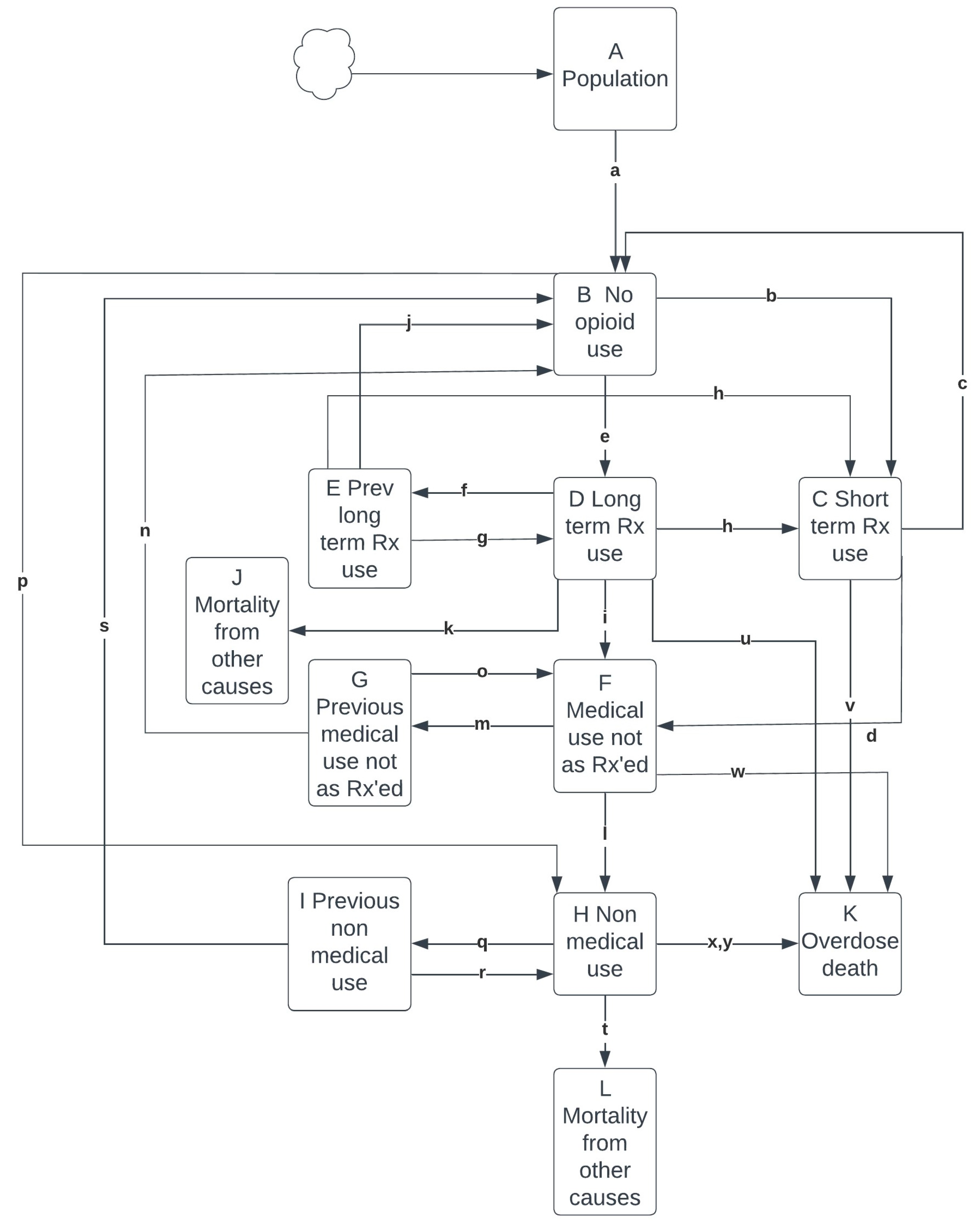
| No opioid use |
| (a) Monthly population increase = A * α |
| Prescription opioid use |
| Short-term prescription opioid use |
| (b) Starting short-term use = B * β * γ |
| (c) Stopping short-term use = C * δ |
| (d) Short-term use to use not as prescribed = C * ε/10 |
| Long-term prescription opioid use |
| (e) Starting long-term use = B * β * (1.0 − γ) |
| (f) Stopping long term use = D * ζ |
| (g) Previous long-term use to long term use = E * η * (1.0 − γ) |
| (h) Previous long-term use to short-term use = E * η * γ |
| (i) Long-term use to use not as prescribed = D * ε |
| (j) Previous long-term use to no use = E * θ |
| (k) Long term-use all-cause mortality = D * ι |
| Prescription use not as prescribed |
| (l) Use not as prescribed to non-medical use = F * κ |
| (m) Stopping use not as prescribed = F * μ * 2 |
| (n) Previous use not as prescribed to no use = G * ν |
| (o) Restarting use not as prescribed = G * (ξ/2) |
| Non-medical use |
| (p) Starting non-medical use = B * λ |
| (q) Stopping non-medical use = H * μ |
| (r) Restarting non-medical use = I * ξ |
| (s) Previous non-medical use to no use = I * ν |
| (t) Non-medical use all-cause mortality = H * σ |
| Overdose mortality |
| (u) Long-term use overdose mortality = D * ο |
| (v) Short-term use overdose mortality = C * π |
| (w) Use not as prescribed overdose mortality = F * ρ * χ * φ * τ |
| (x) Non-medical–non-fentanyl-related overdose mortality = H * ρ * φ * τ |
| (y) Non-medical-fentanyl-related overdose mortality = H * ρ * ψ * υ * φ * τ |
| Concepts | Parameter | Value | Evidence Source |
|---|---|---|---|
| Population | A | 30,874,000 | [15] |
| No opioid use | B | A – (C + D + E + F + G + H + I) | |
| Short-term prescription use | C | 262,170 | [16] |
| Long-term prescription use | D | 690,594 | [16] |
| Previous long-term prescription use | E | 700,000 | |
| Prescription use not as prescribed | F | 320,256 | [17] |
| Previous prescription use not as prescribed | G | 100,000 | |
| Non-medical use (illicit and illegal opioids) | H | 200,000 | [18,19] |
| Previous non-medical use | I | No initial value provided | |
| Mortality from other causes among those using long-term prescription opioids | J | No initial value provided | |
| Mortality from opioid overdose | K | No initial value provided | |
| Mortality from other causes among those using non-medical opioids | L | No initial value provided | |
| Population increase | α | 0.014 per year 0.00117 per month | [15] |
| Rate starting opioid prescription varies during first four years | β | [20] | |
| Opioid Rx 2016 | 2016 | 0.0866/12 per month | |
| Opioid Rx 2017 | 2017 | 0.0838/12 per month | |
| Opioid Rx 2018 | 2018 | 0.081/12 per month | |
| Opioid Rx 2019 | 2019 | 0.0782/12 per month | |
| Proportion new short-term prescription use | γ | 0.9 | [20] |
| Rate stopping short-term prescription use | δ | 0.9 per month | [20] |
| Rate prescription use to use not as prescribed | ε | 0.093 per year 0.00775 per month | [21] |
| Rate stopping long-term prescription use | ζ | 0.017 per month | [20] |
| Rate previous long-term to new prescription use | η | 0.65 per year 0.55 per month | [20] |
| Rate to no long-term prescription use | θ | 0.08796 per year 0.00733 per month | [20] |
| Rate of all-cause mortality among those using long-term prescription use | ι | 0.06 per year 0.005 per month | [22] |
| Rate of moving from prescription use not as prescribed to non-medical use | κ | 0.065 per year 0.0054 per month | [23] |
| Rate start non-medical use | λ | 0.00006 per year 0.000005 per month | [24] |
| Rate stop using prescription not as prescribed and non-medical use | μ | 0.09 per year 0.0075 per month | [25] |
| Delay to no use | ν | 0.028 | |
| Rate restart non-medical use | ξ | 0.20 per year 0.017 per month | [26] |
| Rate of opioid-related mortality from long-term prescription use | ο | 0.0000582769 per month | [27] |
| Rate of opioid-related mortality from short-term prescription use | π | 0.0000043333 per month | [21] |
| Rate of opioid-related mortality from prescription opioid use not as prescribed and non-medical use | |||
| Initial value | ρ | 0.000542 per month | [28] |
| Optimized value | ρ’ | 0.000318 per month | |
| Rate of mortality from all other causes among people with non-medical use | σ | 0.000783 per month | [29] |
| Seasonality value | τ | 1.02, 1.01, 0.95, and 0.99 for Quarters 1 through 4 | [2] |
| Proxy for level of fentanyl in the drug supply | υ | 2016—0.25 2017—0.48 2018—0.61 2019—0.08 2020—1.00 2021—1.22 | [30] |
| Level of deaths prevented through health interventions | φ | See Table S3 | See Section 2 |
| Mortality multiplication factor for prescription use not as prescribed | |||
| Initial value | χ | 1 | |
| Optimized value | χ’ | 0.1 | |
| Mortality multiplication factor for fentanyl | |||
| Initial value | ψ | 5 | |
| Optimized value | ψ’ | 10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zahan, R.; Osgood, N.D.; Plouffe, R.; Orpana, H. A Dynamic Model of Opioid Overdose Deaths in Canada during the Co-Occurring Opioid Overdose Crisis and COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2024, 21, 442. https://doi.org/10.3390/ijerph21040442
Zahan R, Osgood ND, Plouffe R, Orpana H. A Dynamic Model of Opioid Overdose Deaths in Canada during the Co-Occurring Opioid Overdose Crisis and COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2024; 21(4):442. https://doi.org/10.3390/ijerph21040442
Chicago/Turabian StyleZahan, Rifat, Nathaniel D. Osgood, Rebecca Plouffe, and Heather Orpana. 2024. "A Dynamic Model of Opioid Overdose Deaths in Canada during the Co-Occurring Opioid Overdose Crisis and COVID-19 Pandemic" International Journal of Environmental Research and Public Health 21, no. 4: 442. https://doi.org/10.3390/ijerph21040442