
Increasing Preterm Delivery and Small for Gestational Age Trends in South Carolina during the COVID-19 Pandemic
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
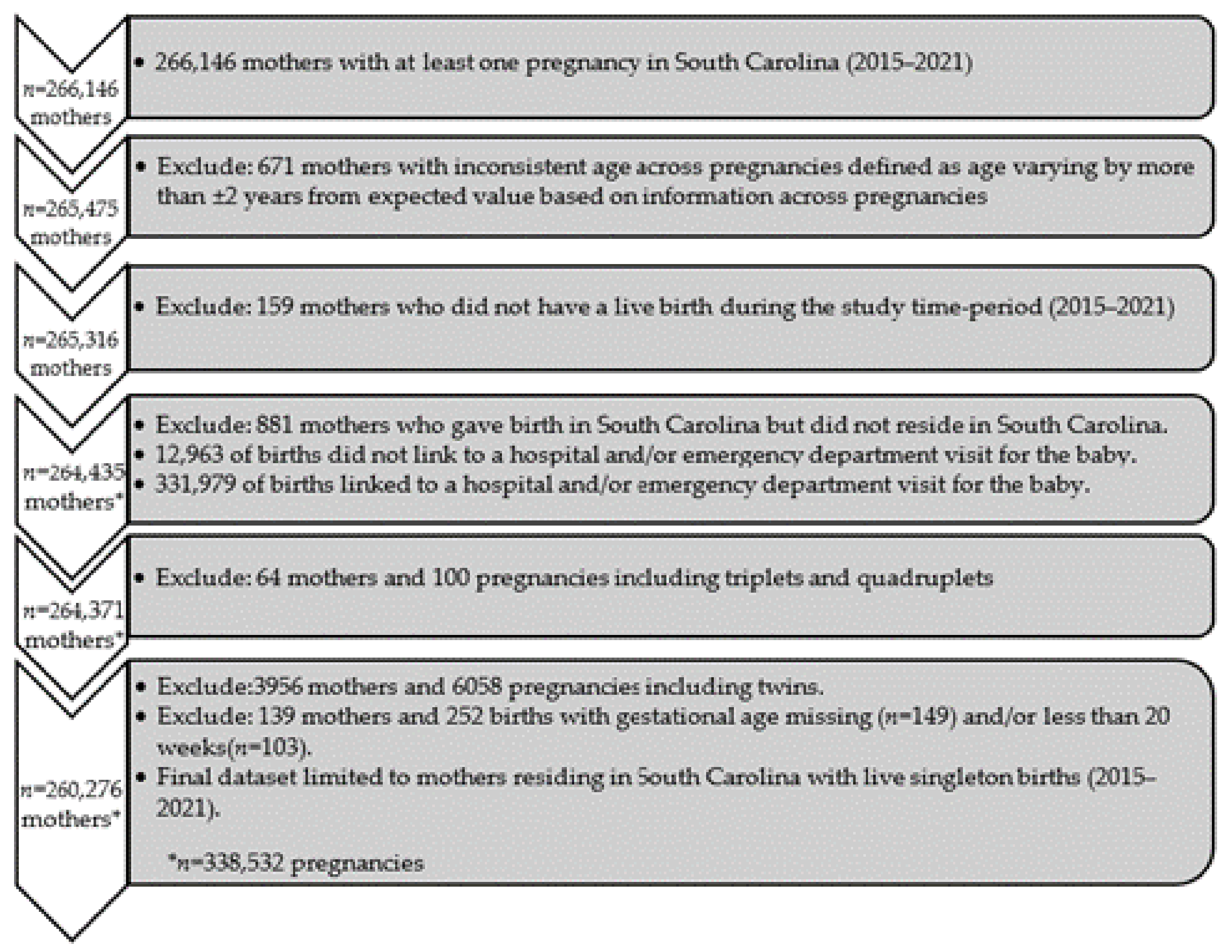
2.2. Cohort Selection
2.3. Definitions
2.4. Statistical Analysis
3. Results
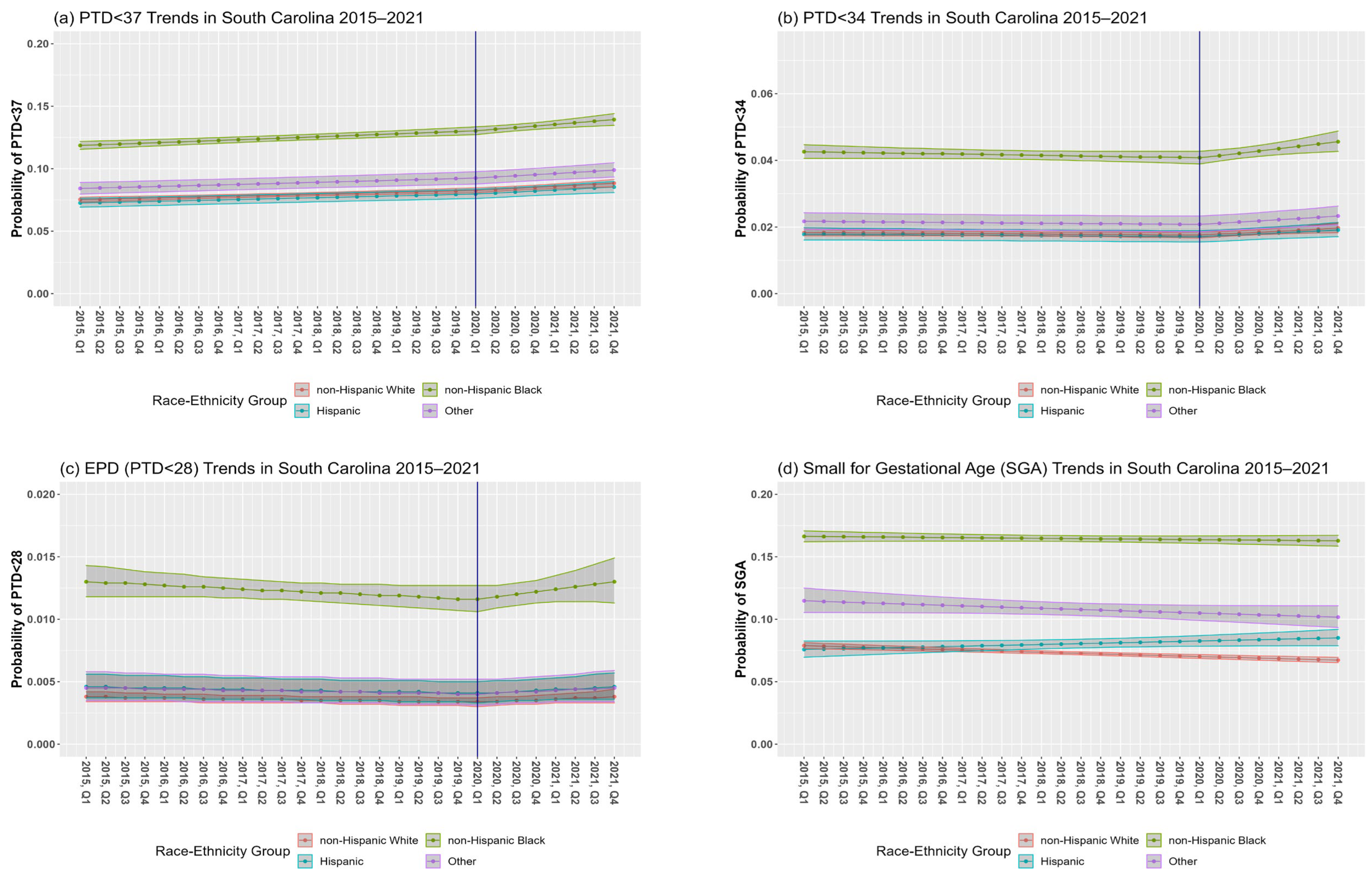
3.1. PTD from 20 to Less than 37 Weeks of Gestation (PTD < 37)
3.2. PTD from 20 to Less than 34 Weeks of Gestation (PTD < 34)
3.3. PTD from 20 to Less than 28 Weeks of Gestation (EPD < 28 wks.)
3.4. SGA
3.5. Secondary Analyses: Covariates Associated with Outcomes of Interest before and during the Pandemic
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Katz, J.; Lee, A.C.; Kozuki, N.; Lawn, J.E.; Cousens, S.; Blencowe, H.; Ezzati, M.; Bhutta, Z.A.; Marchant, T.; Willey, B.A.; et al. Mortality risk in preterm and small-for-gestational-age infants in low-income and middle-income countries: A pooled country analysis. Lancet 2013, 382, 417–425. [Google Scholar] [CrossRef]
- Perin, J.; Mulick, A.; Yeung, D.; Villavicencio, F.; Lopez, G.; Strong, K.L.; Prieto-Merino, D.; Cousens, S.; Black, R.E.; Liu, L. Global, regional, and national causes of under-5 mortality in 2000–19: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet Child Adolesc. Health 2022, 6, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Jelliffe-Pawlowski, L.L.; Hansen, R.L. Neurodevelopmental outcome at 8 months and 4 years among infants born full-term small-for-gestational-age. J. Perinatol. 2004, 24, 505–514. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Khalil, A.; von Dadelszen, P.; Kalafat, E.; Sebghati, M.; Ladhani, S.; Ugwumadu, A.; Draycott, T.; O’Brien, P.; Magee, L. Change in obstetric attendance and activities during the COVID-19 pandemic. Lancet Infect. Dis. 2021, 21, e115. [Google Scholar] [CrossRef] [PubMed]
- Kotlar, B.; Gerson, E.M.; Petrillo, S.; Langer, A.; Tiemeier, H. The impact of the COVID-19 pandemic on maternal and perinatal health: A scoping review. Reprod. Health 2021, 18, 10. [Google Scholar] [CrossRef] [PubMed]
- Lebel, C.; MacKinnon, A.; Bagshawe, M.; Tomfohr-Madsen, L.; Giesbrecht, G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J. Affect. Disord. 2020, 277, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; von Dadelszen, P.; Draycott, T.; Ugwumadu, A.; O’brien, P.; Magee, L. Change in the Incidence of Stillbirth and Preterm Delivery During the COVID-19 Pandemic. JAMA 2020, 324, 705–706. [Google Scholar] [CrossRef] [PubMed]
- Chmielewska, B.; Barratt, I.; Townsend, R.; Kalafat, E.; van der Meulen, J.; Gurol-Urganci, I.; O’Brien, P.; Morris, E.; Draycott, T.; Thangaratinam, S.; et al. Effects of the COVID-19 pandemic on maternal and perinatal outcomes: A systematic review and meta-analysis. Lancet Glob. Health 2021, 9, e759–e772. [Google Scholar] [CrossRef] [PubMed]
- Karimi, L.; Makvandi, S.; Vahedian-Azimi, A.; Sathyapalan, T.; Sahebkar, A. Effect of COVID-19 on Mortality of Pregnant and Postpartum Women: A Systematic Review and Meta-Analysis. J. Pregnancy 2021, 2021, 8870129. [Google Scholar] [CrossRef]
- Petersen, E.E. Racial/Ethnic Disparities in Pregnancy-Related Deaths—United States, 2007–2016. Morbidity and Mortality Weekly Report- US Department of Health and Human Services/Centers for Disease Control and Prevention. MMWR Morb. Mortal. Wkly. Rep. 2019, 68. [Google Scholar] [CrossRef]
- Hoyert, D. Maternal mortality rates in the United States, 2021. NCHS Health E-Stats. Natl. Cent. Health Stat. 2023, 230, 1–440. [Google Scholar]
- South Carolina Maternal Morbidity and Mortality Review Committee. South Carolina Maternal Morbidity and Mortality Review Committee Legislative Brief March. Available online: https://scdhec.gov/sites/default/files/media/document/2023-SC-MMMRC-Legislative-Brief.pdf (accessed on 25 August 2023).
- Xu, J.; Sherry, L.; Murphy, B.S.; Kenneth, D.; Kochanek, M.A.; Arias, E. Mortality in the United States, 2021; Department of Health And Human Services Centers for Disease Control and Prevention National Center for Health Statistics: Hyattsville, MD, USA, 2022.
- South Carolina Department of Health and Environmental Control. Infant Mortality and Selected Birth Characteristics- 2021 South Carolina Residence Data. Available online: https://scdhec.gov/sites/default/files/Library/CR-012142-2021.pdf (accessed on 25 August 2023).
- Bell, T.J. Closing the Gap in Health Care: A Personal Odyssey. J. Law Med. Ethic. 2021, 49, 168–173. [Google Scholar] [CrossRef]
- Ben, J.; Cormack, D.; Harris, R.; Paradies, Y. Racism and health service utilisation: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189900. [Google Scholar] [CrossRef]
- Paradies, Y.; Ben, J.; Denson, N.; Elias, A.; Priest, N.; Pieterse, A.; Gupta, A.; Kelaher, M.; Gee, G. Racism as a Determinant of Health: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0138511. [Google Scholar] [CrossRef]
- Sullivan, L.S.; Pelzer, D.; Rice, A.; Peterson, Y.K.; Sade, R.M.; Townsend, D.M.; Zisk, N. Responsibility for Structural Racism in Medicine: Reflections and Recommendations from One Institution. Narrat. Inq. Bioeth. 2021, 11, 221–229. [Google Scholar] [CrossRef]
- Thompson, T.-A.M.; Young, Y.-Y.; Bass, T.M.; Baker, S.; Njoku, O.; Norwood, J.; Simpson, M. Racism Runs Through It: Examining The Sexual And Reproductive Health Experience Of Black Women In The South. Health Aff. 2022, 41, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Brady, E.; Hamilton, P.D.; Joyce, A.; Martin, M.P.H.; Michelle, J.K.; Osterman, M.H.S. Births Provisional Data for Division of Vital Statistics. Report No. 20; Division of Vital Statistics, National Center for Health Statistics: Hyattsville, MD, USA, 2022.
- Alexander, G.R.; Himes, J.H.; Kaufman, R.B.; Mor, J.; Kogan, M. A united states national reference for fetal growth. Obstetrics & Gynecology 1996, 87, 163–168. [Google Scholar] [CrossRef]
- Talge, N.M.; Mudd, L.M.; Sikorskii, A.; Basso, O. United states birth weight reference corrected for implausible gestational age estimates. Pediatrics 2014, 133, 844–853. [Google Scholar] [CrossRef] [PubMed]
- Spiegelman, D.; Hertzmark, E. Easy SAS calculations for risk or prevalence ratios and differences. Am. J. Epidemiology 2005, 162, 199–200. [Google Scholar] [CrossRef]
- Thoma, M.E.; Drew, L.B.; Hirai, A.H.; Kim, T.Y.; Fenelon, A.; Shenassa, E.D. Black-White Disparities in Preterm Birth: Geographic, Social, and Health Determinants. Am. J. Prev. Med. 2019, 57, 675–686. [Google Scholar] [CrossRef]
- Manuck, T.A. Racial and ethnic differences in preterm birth: A complex, multifactorial problem. Semin. Perinatol. 2017, 41, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Mendez, Y.; Linda, A.; Alpuing, R.; Delgadillo Chabolla, L.E.; Castillo Cruz, A.; Johanan, L.; Salim, S. Gestational diabetes mellitus and COVID-19: The epidemic during the pandemic. World J. Diabetes 2023, 14, 1178–1193. [Google Scholar] [CrossRef] [PubMed]
- La Verde, M.; Torella, M.; Riemma, G.; Narciso, G.; Iavarone, I.; Gliubizzi, L.; Palma, M.; Morlando, M.; Colacurci, N.; De Franciscis, P. Incidence of gestational diabetes mellitus before and after the COVID-19 lockdown: A retrospective cohort study. J. Obstet. Gynaecol. Res. 2022, 48, 1126–1131. [Google Scholar] [CrossRef] [PubMed]
- Sinnott, C.; Freret, T.S.; Clapp, M.A.; Little, S.E. Increased rates of hypertensive disorders of pregnancy during the COVID-19 pandemic. Am. J. Perinatol. 2024, 1, 2295–3543. [Google Scholar] [CrossRef] [PubMed]
- Vaccaro, C.; Mahmoud, F.; Aboulatta, L.; Aloud, B.; Eltonsy, S. The impact of COVID-19 first wave national lockdowns on perinatal outcomes: A rapid review and meta-analysis. BMC Pregnancy Childbirth 2021, 21, 676. [Google Scholar] [CrossRef]
- Maslin, K.; McKeon-Carter, R.; Hosking, J.; Stockley, L.; Southby, C.; Shawe, J.; Latour, J.M. Preterm births in South-West England before and during the COVID-19 pandemic: An audit of retrospective data. Eur. J. Pediatr. 2021, 181, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Roberts, N.F.; Sprague, A.E.; Taljaard, M.; Fell, D.B.; Ray, J.G.; Tunde-Byass, M.; Biringer, A.; Barrett, J.F.; Khurshid, F.; Diaz, S.; et al. Maternal-Newborn Health System Changes and Outcomes in Ontario, Canada, During Wave 1 of the COVID-19 Pandemic—A Retrospective Study. J. Obstet. Gynaecol. Can. 2022, 44, 664–674. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.S.; Ye, X.Y.; Yang, J.; Campitelli, M.A. Preterm birth and stillbirth rates during the COVID-19 pandemic: A population-based cohort study. Can. Med. Assoc. J. 2021, 193, E1164–E1172. [Google Scholar] [CrossRef]
- Mullin, A.M.; Handley, S.C.; Lundsberg, L.; Elovitz, M.A.; Lorch, S.A.; McComb, E.J.; Montoya-Williams, D.; Yang, N.; Dysart, K.; Son, M.; et al. Changes in preterm birth during the COVID-19 pandemic by duration of exposure and race and ethnicity. J. Perinatol. 2022, 42, 1346–1352. [Google Scholar] [CrossRef]
- Main, E.K.; Chang, S.-C.; Carpenter, A.M.; Wise, P.H.; Stevenson, D.K.; Shaw, G.M.; Gould, J.B. Singleton preterm birth rates for racial and ethnic groups during the coronavirus disease 2019 pandemic in California. Am. J. Obstet. Gynecol. 2021, 224, 239–241. [Google Scholar] [CrossRef]
- Been, J.V.; Ochoa, L.B.; Bertens, L.C.M.; Schoenmakers, S.; Steegers, E.A.P.; Reiss, I.K.M. Impact of COVID-19 mitigation measures on the incidence of preterm birth: A national quasi-experimental study. Lancet Public Health 2020, 5, e604–e611. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, M.; Tsuji, S.; Tanaka-Mizuno, S.; Kasahara, K.; Kasahara, M.; Miura, K.; Murakami, T. Amelioration of prevalence of threatened preterm labor during the COVID-19 pandemic: Nationwide database analysis in Japan. Sci. Rep. 2022, 12, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Stumpfe, F.M.; Schneider, M.O.; Hein, A.; Faschingbauer, F.; Kehl, S.; Hermanek, P.; Mayr, A. Limited Effects of SARS-CoV-2 Pandemic-related Lockdowns and Reduced Population Mobility on Preterm Birth Rates: A Secondary Analysis of Bavarian Obstetric Quality Parameters from 2010 to 2020. Geburtshilfe Frauenheilkd 2022, 82, 842–851. [Google Scholar] [CrossRef]
- Yang, J.; D’souza, R.; Kharrat, A.; Fell, D.B.; Snelgrove, J.W.; Murphy, K.E.; Shah, P.S. Coronavirus disease 2019 pandemic and pregnancy and neonatal outcomes in general population: A living systematic review and meta-analysis (updated Aug 14, 2021). Acta Obstet. Gynecol. Scand. 2022, 101, 7–24. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Ferre, C.; Ouyang, L.; Mohamoud, Y.; Barfield, W.; Cox, S. Changes and geographic variation in rates of preterm birth and stillbirth during the prepandemic period and COVID-19 pandemic, according to health insurance claims in the United States, April–June 2019 and April–June. Am. J. Obstet. Gynecol. MFM 2022, 4, 100508. [Google Scholar] [CrossRef] [PubMed]
- Harvey, E.M.; McNeer, E.; McDonald, M.F.; Shapiro-Mendoza, C.K.; Dupont, W.D.; Barfield, W.; Patrick, S.W. Association of Preterm Birth Rate With COVID-19 Statewide Stay-at-Home Orders in Tennessee. JAMA Pediatr. 2021, 175, 635–637. [Google Scholar] [CrossRef] [PubMed]
- Calvert, C.; Brockway, M.; Zoega, H.; Miller, J.E.; Been, J.V.; Amegah, A.K.; Racine-Poon, A.; Oskoui, S.E.; Abok, I.I.; Aghaeepour, N.; et al. Changes in preterm birth and stillbirth during COVID-19 lockdowns in 26 countries. Nat. Hum. Behav. 2023, 7, 529–544. [Google Scholar] [CrossRef] [PubMed]
- Fresson, J.; Bruckner, T.A.; Le Ray, C.; Goffinet, F.; Rey, S.; Blondel, B.; Deneux-Tharaux, C.; Ancel, P.-Y.; Zeitlin, J. Decreases in preterm birth during the first COVID-19 lockdown in France by gestational age sub-groups and regional COVID-19 incidence. Ann. Epidemiology 2022, 72, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Kc, A.; Gurung, R.; Kinney, M.V.; Sunny, A.K.; Moinuddin, M.; Basnet, O.; Paudel, P.; Bhattarai, P.; Subedi, K.; Shrestha, M.P.; et al. Effect of the COVID-19 pandemic response on intrapartum care, stillbirth, and neonatal mortality outcomes in Nepal: A prospective observational study. Lancet Glob. Health 2020, 8, e1273–e1281. [Google Scholar] [CrossRef]
- Lee, J.Y.; Park, J.; Lee, M.; Han, M.; Jung, I.; Lim, S.M.; Baek, J.Y.; Kang, J.-M.; Park, M.S.; Ahn, J.G. The impact of non-pharmaceutical interventions on premature births during the COVID-19 pandemic: A nationwide observational study in Korea. Front. Pediatr. 2023, 11, 1140556. [Google Scholar] [CrossRef]
- Aboulatta, L.; Kowalec, K.; Leong, C.; Delaney, J.A.; Falk, J.; Alessi-Severini, S.; Chateau, D.; Tan, Q.; Kearns, K.; Raimondi, C.; et al. Preterm birth and stillbirth rates associated with socioeconomic disparities during COVID-19 pandemic: A population-based cross-sectional study. BMJ Paediatr. Open 2023, 7, e001686. [Google Scholar] [CrossRef] [PubMed]
- Mak, A.H.M.; Cicero, S.; Hui, P.W. Impact of COVID-19 pandemic on preterm delivery. J. Obstet. Gynaecol. Res. 2023, 49, 1539–1544. [Google Scholar] [CrossRef] [PubMed]
- Naqvi, S.; Naqvi, F.; Saleem, S.; Thorsten, V.R.; Figueroa, L.; Mazariegos, M.; Goldenberg, R.L. Health care in pregnancy during the COVID-19 pandemic and pregnancy outcomes in six low- and-middle-income countries: Evidence from a prospective, observational registry of the Global Network for Women’s and Children’s Health. BJOG 2022, 129, 1298–1307. [Google Scholar] [CrossRef] [PubMed]
- Maki, Y.; Tokuda, A.; Kino, E.; Yamauchi, A.; Ohtsuka, T.; Terao, K. No significant changes in preterm birth, low-birth-weight, and small-for-gestational-age infants during the first year of the COVID-19 pandemic in a rural area in Japan. J. Obstet. Gynaecol. Res. 2023, 49, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Dietz, P.M.; Bombard, J.M.; Hutchings, Y.L.; Gauthier, J.P.; Gambatese, M.A.; Ko, J.Y.; Martin, J.A.; Callaghan, W.M. Validation of obstetric estimate of gestational age on US birth certificates. Am. J. Obstet. Gynecol. 2014, 210, 335.e1–335.e5. [Google Scholar] [CrossRef] [PubMed]
- Stout, M.J.; Macones, G.A.; Tuuli, M.G. Accuracy of Birth Certificate Data for Classifying Preterm Birth. Paediatr. Périnat. Epidemiology 2017, 31, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.Q.; Bilodeau-Bertrand, M.; Liu, S.; Auger, N. The impact of COVID-19 on pregnancy outcomes: A systematic review and meta-analysis. Can. Med. Assoc. J. 2021, 193, E540–E548. [Google Scholar] [CrossRef]
- Papapanou, M.; Papaioannou, M.; Petta, A.; Routsi, E.; Farmaki, M.; Vlahos, N.; Siristatidis, C. Maternal and Neonatal Characteristics and Outcomes of COVID-19 in Pregnancy: An Overview of Systematic Reviews. Int. J. Environ. Res. Public Health 2021, 18, 596. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Maternal Race–Ethnicity, n (%) | Total n (%) | ||||
|---|---|---|---|---|---|
| NHW | NHB | Hispanic | Other | ||
| 191,318 (56.5%) | 105,839 (31.3%) | 25,209 (7.5%) | 16,166 (4.8%) | 338,532 (100%) | |
| % | % | % | % | % | |
| Outcomes | |||||
| PTD < 37 wks. a,b | 7.9 | 12.4 | 7.5 | 8.9 | 9.3 |
| PTD < 34 wks. a,b | 1.7 | 4.0 | 1.6 | 2.0 | 2.4 |
| EPD < 28 wks. a,b | 0.3 | 1.0 | 0.3 | 0.4 | 0.5 |
| SGA a,c | 7.2 | 16.3 | 7.9 | 10.7 | 10.2 |
| Sociodemographic covariates | |||||
| Age at delivery (y); mean (SD) a | 28.4 (5.6) | 26.8 (5.7) | 28.2 (6.2) | 29.2 (6.0) | 28.0 (5.7) |
| Mother’s education a | |||||
| Less than high school | 9.6 | 13.4 | 42.5 | 17.2 | 13.6 |
| High school or GED | 20.2 | 34.4 | 27.0 | 20.7 | 25.2 |
| Some college | 23.2 | 30.2 | 13.9 | 17.8 | 24.5 |
| ≥College degree | 46.7 | 21.7 | 16.4 | 44.0 | 36.6 |
| Rural residence | 30.1 | 35.9 | 28.4 | 23.3 | 31.5 |
| Medicaid eligibility | 39.7 | 72.6 | 70.2 | 49.4 | 52.7 |
| WIC a | 27.8 | 61.4 | 44.0 | 31.6 | 39.7 |
| Lifestyle and clinical covariates | |||||
| Smoking (during or pre-pregnancy) a | 15.1 | 8.6 | 2.0 | 4.7 | 11.6 |
| Primipara a | 33.1 | 28.8 | 25.9 | 34.0 | 31.3 |
| Previous PTD | 4.1 | 6.6 | 4.1 | 3.8 | 4.9 |
| STI during pregnancy c | 6.1 | 12.2 | 5.3 | 5.8 | 7.9 |
| GDM a | 8.9 | 8.1 | 11.2 | 13.2 | 9.0 |
| Pre-pregnancy diabetes | 1.4 | 3.2 | 1.6 | 1.7 | 2.0 |
| HDP a | 14.8 | 18.7 | 11.8 | 11.1 | 15.7 |
| Pre-pregnancy hypertension | 6.9 | 15.5 | 3.8 | 4.4 | 9.3 |
| Pre-pregnancy BMI category a,d | |||||
| Underweight | 3.7 | 2.8 | 2.0 | 4.5 | 3.3 |
| Normal | 43.8 | 27.5 | 36.2 | 45.9 | 38.3 |
| Overweight | 24.8 | 24.5 | 32.2 | 26.7 | 25.3 |
| Obese | 27.5 | 45.0 | 29.4 | 22.8 | 32.9 |
| PTD < 37 wks. | PTD < 34 wks. | EPD < 28 wks. | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristic | Model 1a | Model 1b | Model 1c | Model 2a | Model 2b | Model 2c | Model 3a | Model 3b | Model 3c |
| Calendar time before CP (per year) b,c | 1.02 (1.01, 1.03) | 1.01 (1.00, 1.02) | 0.99 (0.98, 1.00) | 0.99 (0.98,1.01) | 0.98 (0.96, 0.99) | 0.95 (0.94, 0.97) | 0.98 (0.95, 1.01) | 0.96 (0.93, 0.99) | 0.94 (0.92, 0.97) |
| Calendar time post-CP (per year) b,c,d | 1.04 (1.02, 1.06) | 1.03 (1.00, 1.05) | 1.01 (0.99,1.04) | 1.07 (1.02, 1.12) | 1.05 (1.00, 1.10) | 1.03 (0.99, 1.09) | 1.07 (0.97, 1.18) | 1.04 (0.94, 1.15) | 1.03 (0.93, 1.14) |
| CP c | p = 0.1762 | p = 0.0130 | p = 0.1452 | ||||||
| Calendar time before CP * race (per quarter) e | p = 0.8997 | - | - | p = 0.5742 | - | - | p = 0.8871 | - | - |
| Calendar time post-CP * race (per quarter) e | p = 0.8053 | - | - | p = 0.4107 | - | - | p = 0.8803 | - | - |
| Sociodemographic covariates | |||||||||
| Race–ethnic group | |||||||||
| Non-Hispanic White | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Non-Hispanic Black | 1.58 (1.54, 1.61) | 1.47 (1.44, 1.51) | 1.36 (1.32, 1.39) | 2.32 (2.22, 2.43) | 2.19 (2.08, 2.30) | 1.99 (1.89, 2.09) | 3.44 (3.13, 3.78) | 3.40 (3.05, 3.78) | 3.11 (2.78, 3.48) |
| Hispanic | 0.96 (0.92, 1.01) | 0.78 (0.75, 0.82) | 0.92 (0.87, 0.96) | 0.97 (0.88, 1.08) | 0.78 (0.70, 0.86) | 0.94 (0.85,1.05) | 1.21 (0.99, 1.49) | 1.05 (0.84, 1.30) | 1.20 (0.96, 1.50) |
| Other races–ethnicities | 1.12 (1.06, 1.18) | 1.04 (0.99, 1.10) | 1.15 (1.09, 1.21) | 1.18 (1.06, 1.32) | 1.11(0.99, 1.25) | 1.26 (1.12, 1.41) | 1.20 (0.93, 1.54) | 1.17 (0.91, 1.51) | 1.33 (1.03, 1.71) |
| Age at delivery (y) f | - | 1.03 (1.03, 1.03) | 1.01 (1.01, 1.02) | - | 1.03 (1.02, 1.03) | 1.02 (1.01, 1.02) | - | 1.01 (1.00, 1.02) | 1.01 (1.00, 1.02 |
| Maternal education | |||||||||
| Less than high school education | - | 1.00 (reference) | 1.00 (reference) | - | 1.00 (reference) | 1.00 (reference) | - | 1.00 (reference) | 1.00 (reference) |
| High school or GED | - | 0.87 (0.84, 0.90) | 0.90 (0.87, 0.93) | - | 0.87 (0.81, 0.93) | 0.91 (0.85, 0.97) | - | 0.92(0.80,1.05) | 0.95 (0.83, 1.08) |
| Some college experience | - | 0.79 (0.76, 0.82) | 0.85 (0.82, 0.88) | - | 0.75 (0.70, 0.81) | 0.81 (0.76, 0.87) | - | 0.80 (0.69, 0.92) | 0.83 (0.72, 0.96) |
| ≥College degree | - | 0.62 (0.60, 0.65) | 0.73 (0.70, 0.76) | - | 0.59 (0.54, 0.64) | 0.68 (0.63, 0.74) | - | 0.66 (0.56, 0.78) | 0.72 (0.60, 0.85) |
| Rural residence (rural versus urban) | - | 1.01 (0.98, 1.03) | 1.02 (1.00, 1.04) | - | 1.06 (1.02, 1.11) | 1.09 (1.04, 1.14) | - | 1.11 (1.01, 1.22) | 1.10 (1.00, 1.21) |
| Medicaid eligibility | - | 1.23 (1.12, 1.26) | 1.16 (1.13, 1.19) | - | 1.32 (1.25, 1.40) | 1.27 (1.20, 1.34) | - | 1.36 (1.21,1.52) | 1.36 (1.21, 1.53) |
| WIC | - | 0.91 (0.89, 0.93) | 0.88 (0.86, 0.91) | - | 0.76 (0.73, 0.80) | 0.74 (0.70, 0.77) | - | 0.61 (0.55, 0.67) | 0.58 (0.53, 0.64) |
| Lifestyle and clinical covariates | |||||||||
| Smoking (during or pre-pregnancy) | - | - | 1.11 (1.07, 1.15) | - | - | 1.12 (1.05, 1.19) | - | - | 1.16 (1.01, 1.33) |
| Primipara | - | - | 1.10 (1.08, 1.13) | - | - | 1.42 (1.35, 1.50) | - | - | 1.64 (1.47, 1.83) |
| Previous PTD | - | - | 2.41 (2.34, 2.48) | - | - | 2.70 (2.53, 2.87) | - | - | 2.47 (2.15, 2.83) |
| STI during pregnancy g | - | - | 1.01 (0.98, 1.05) | - | - | 0.98 (0.90, 1.05) | - | - | 0.86 (0.74, 1.01) |
| GDM | - | - | 1.24 (1.20, 1.28) | - | - | 0.93 (0.87,1.00) | - | - | 0.46 (0.37, 0.56) |
| Pre-pregnancy diabetes | - | - | 2.04 (1.96, 2.13) | - | - | 1.70 (1.55, 1.85) | - | - | 1.47 (1.12, 1.79) |
| HDP | - | - | 2.41 (2.36, 2.47) | - | - | 2.79 (2.67, 2.92) | - | - | 1.53 (1.38, 1.69) |
| Pre-pregnancy hypertension | - | - | 1.57 (1.53, 1.61) | - | - | 1.86 (1.76, 1.97) | - | - | 1.75 (1.55, 1.96) |
| Pre-pregnancy BMI category h | |||||||||
| Underweight | - | - | 1.31 (1.24, 1.39) | - | - | 1.26 (1.12, 1.42) | - | - | 1.07 (0.82, 1.38) |
| Normal | - | - | 1.00 (reference) | - | - | 1.00 (reference) | - | - | 1.00 (reference) |
| Overweight | - | - | 0.89 (0.87, 0.92) | - | - | 0.92 (0.87, 0.98) | - | - | 1.10 (0.98, 1.24) |
| Obese | - | - | 0.86 (0.83, 0.88) | - | - | 0.88 (0.84, 0.93) | - | - | 1.25 (1.11, 1.40) |
| Characteristic | Model 4a | Model 4b | Model 4c |
|---|---|---|---|
| Calendar time before CP (per year) b,c | - | - | - |
| Calendar time post-CP (per year) b,c,d | - | - | - |
| CP (per quarter) c,e | p = 0.8442 | - | - |
| Calendar time before CP * race (per quarter) | p = 0.0155 | - | - |
| Non-Hispanic White (per year) | 0.98 (0.97, 0.98) | 0.99 (0.98, 1.00) | 1.00 (0.99, 1.00) |
| Non-Hispanic Black (per year) | 1.00 (0.99, 1.00) | 1.01 (1.00, 1.01) | 1.01 (1.00, 1.01) |
| Hispanic (per year) | 1.02 (1.00, 1.04) | 1.04 (1.01, 1.06) | 1.03 (1.01, 1.05) |
| Other races–ethnicities (per year) | 0.98 (0.96, 1.00) | 0.99 (0.97, 1.01) | 0.99 (0.97, 1.01) |
| Calendar time after CP * race (per quarter) e | p = 0.7252 | - | - |
| Non-Hispanic White | - | - | - |
| Non-Hispanic Black | - | - | - |
| Hispanic | - | - | - |
| Other races–ethnicities | - | - | - |
| Sociodemographic covariates | - | - | - |
| Age at delivery (years) f | - | 0.99 (0.99, 0.99) | 1.01 (1.01, 1.01) |
| Maternal education | |||
| Less than high school | - | 1.00 (reference) | 1.00 (reference) |
| High school or GED | - | 0.89 (0.86, 0.92) | 0.92 (0.89, 0.95) |
| Some college | - | 0.79 (0.76, 0.81) | 0.82 (0.80, 0.85) |
| ≥College degree | - | 0.69 (0.67, 0.72) | 0.71 (0.69, 0.74) |
| Rural residence (rural versus urban) | - | 1.05 (1.03, 1.08) | 1.06 (1.04, 1.08) |
| Medicaid eligibility | - | 1.10 (1.08, 1.13) | 1.12 (1.09, 1.15) |
| WIC | - | 1.11 (1.09, 1.14) | 1.09 (1.06, 1.11) |
| Lifestyle and clinical covariates | |||
| Smoking (during or pre-pregnancy) | - | - | 1.57 (1.53, 1.61) |
| Primipara | - | - | 1.46 (1.43, 1.50) |
| Previous PTD | - | - | 1.16 (1.11, 1.21) |
| STI during pregnancy g | - | - | 0.99 (0.96, 1.02) |
| GDM | - | - | 0.80 (0.77, 0.84) |
| Pre-pregnancy diabetes | - | - | 0.72 (0.66, 0.78) |
| HDP g | - | - | 1.36 (1.32, 1.39) |
| Pre-pregnancy hypertension | - | - | 1.20 (1.16, 1.24) |
| Pre-pregnancy BMI category h | |||
| Underweight | - | - | 1.47 (1.41, 1.53) |
| Normal | - | - | 1.00 (reference) |
| Overweight | - | - | 0.80 (0.78, 0.82) |
| Obese | - | - | 0.68 (0.66, 0.70) |
| Outcomes b | PTD < 37 wks. | PTD < 34 wks. | EPD | SGA | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Covariates c | p-Value of Interaction | Pre-pandemic d | Pandemic e | p-Value of Interaction | Pre-pandemic d | Pandemic e | p-Value of Interaction | Pre-pandemic d | Pandemic e | p-Value of Interaction | Pre-pandemic d | Pandemic e |
| Maternal education | 0.0026 | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ||
| Less than high school | 1.41 (1.35, 1.47) | 1.58 (1.49, 1.67) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| High school or GED | 1.37 (1.33, 1.42) | 1.39 (1.32, 1.45) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| Some college | 1.26 (1.22, 1.30) | 1.35 (1.29, 1.42) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| ≥College degree | 1.00 (reference) | 1.00 (reference) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| Medicaid eligibility | <0.0001 | 1.33 (1.30, 1.36) | 1.48 (1.42, 1.54) | ---- | ---- | ---- | ---- | ---- | ---- | <0.0001 | 1.49 (1.45, 1.52) | 1.75 (1.68, 1.83) |
| Smoking (during or pre-pregnancy) | 0.0016 | 1.17 (1.13, 1.22) | 1.31 (1.24, 1.39) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- |
| Primipara | 0.0348 | 0.94 (0.92, 0.97) | 0.89 (0.86, 0.93) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- |
| Previous PTD | <0.0001 | 2.66 (2.56, 2.77) | 2.16 (2.02, 2.31) | 0.0105 | 3.15 (2.93, 3.39) | 2.66 (2.35, 3.01) | ---- | ---- | ---- | ---- | ---- | ---- |
| Pre-pregnancy diabetes | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | 0.0420 | 0.84 (0.76, 0.92) | 0.99 (0.87, 1.12) |
| HDP | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | 0.0320 | 1.42 (1.38, 1.46) | 1.34 (1.28, 1.40) |
| Pre-pregnancy hypertension | ---- | ---- | ---- | ---- | ---- | ---- | 0.0462 | 2.70 (2.38, 3.08) | 3.41 (2.84, 4.11) | ---- | ---- | ---- |
| Pre-pregnancy BMI category f | 0.0011 | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ||
| Underweight | 1.30 (1.21, 1.38) | 1.33 (1.19, 1.49) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| Normal | 1.00 (reference) | 1.00 (reference) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| Overweight | 1.03 (0.99, 1.06) | 1.06 (1.01, 1.12) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| Obese | 1.28 (1.24, 1.32) | 1.42 (1.36, 1.49) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| Outcomes b | PTD < 37 | PTD < 34 | EPD | SGA | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Covariates c | p-Value of Interaction | Pre-pandemic d | Pandemic e | p-Value of Interaction | Pre-pandemic d | Pandemic e | p-Value of Interaction | Pre-pandemic d | Pandemic e | p-Value of Interaction | Pre-pandemic d | Pandemic e |
| Maternal education | 0.0196 | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ||
| Less than high school | 1.28 (1.22, 1.33) | 1.39 (1.3, 1.48) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| High school or GED | 1.26 (1.22, 1.31) | 1.23 (1.17, 1.30) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| Some college | 1.17 (1.13, 1.21) | 1.21 (1.15, 1.28) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| ≥College degree | 1.00 (reference) | 1.00 (reference) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| Medicaid eligibility | 0.0011 | 1.19 (1.15, 1.22) | 1.28 (1.23, 1.34) | ---- | ---- | ---- | ---- | ---- | ---- | <0.0001 | 1.18 (1.15, 1.22) | 1.36 (1.3, 1.42) |
| Smoking (during or pre-pregnancy) | 0.1522 | 1.08 (1.04, 1.12) | 1.14 (1.07, 1.21) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- |
| Primipara | 0.9458 | 1.08 (1.05, 1.11) | 1.08 (1.03, 1.13) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- |
| Previous PTD | <0.0001 | 2.18 (2.10, 2.27) | 1.78 (1.68, 1.90) | 0.0060 | 2.64 (2.44, 2.85) | 2.20 (1.95, 2.49) | ---- | ---- | ---- | ---- | ---- | ---- |
| Pre-pregnancy diabetes | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | 0.0838 | 0.71 (0.65, 0.78) | 0.82 (0.72, 0.93) | |
| HDP e | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | 0.0112 | 1.42 (1.38, 1.46) | 1.33 (1.27, 1.39) | |
| Pre-pregnancy hypertension | ---- | ---- | ---- | ---- | ---- | 0.0264 | 1.99 (1.73, 2.30) | 2.60 (2.13, 3.16) | ---- | ---- | ---- | |
| Pre-pregnancy BMI category f | 0.1254 | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ||
| Underweight | 1.31 (1.23, 1.39) | 1.34 (1.2, 1.49) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| Normal | 1.00 (reference) | 1.00 (reference) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| Overweight | 0.90 (0.87, 0.93) | 0.92 (0.87, 0.97) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
| Obese | 0.88 (0.85, 0.91) | 0.93 (0.89, 0.98) | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | ---- | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chundru, K.J.; Korte, J.E.; Wen, C.-C.; Neelon, B.; Wilson, D.A.; Mateus, J.; Pearce, J.L.; Alkis, M.; Finneran, M.; Simpson, S.; et al. Increasing Preterm Delivery and Small for Gestational Age Trends in South Carolina during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2024, 21, 465. https://doi.org/10.3390/ijerph21040465
Chundru KJ, Korte JE, Wen C-C, Neelon B, Wilson DA, Mateus J, Pearce JL, Alkis M, Finneran M, Simpson S, et al. Increasing Preterm Delivery and Small for Gestational Age Trends in South Carolina during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2024; 21(4):465. https://doi.org/10.3390/ijerph21040465
Chicago/Turabian StyleChundru, Kalyan J., Jeffrey E. Korte, Chun-Che Wen, Brian Neelon, Dulaney A. Wilson, Julio Mateus, John L. Pearce, Mallory Alkis, Matthew Finneran, Sarah Simpson, and et al. 2024. "Increasing Preterm Delivery and Small for Gestational Age Trends in South Carolina during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 21, no. 4: 465. https://doi.org/10.3390/ijerph21040465
APA StyleChundru, K. J., Korte, J. E., Wen, C.-C., Neelon, B., Wilson, D. A., Mateus, J., Pearce, J. L., Alkis, M., Finneran, M., Simpson, S., Florez, H., Hunt, K. J., & Malek, A. M. (2024). Increasing Preterm Delivery and Small for Gestational Age Trends in South Carolina during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 21(4), 465. https://doi.org/10.3390/ijerph21040465