
Water, Sanitation, and Hygiene Infrastructure and Resources in Schools in Belize during the COVID-19 Pandemic, 2021–2023

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Methods
2.1. National Survey
2.2. Pilot School Selection
2.3. Facility Assessment at 12 Pilot Schools
2.4. Intervention at 12 Pilot Schools
2.5. Statistical Analyses
3. Results
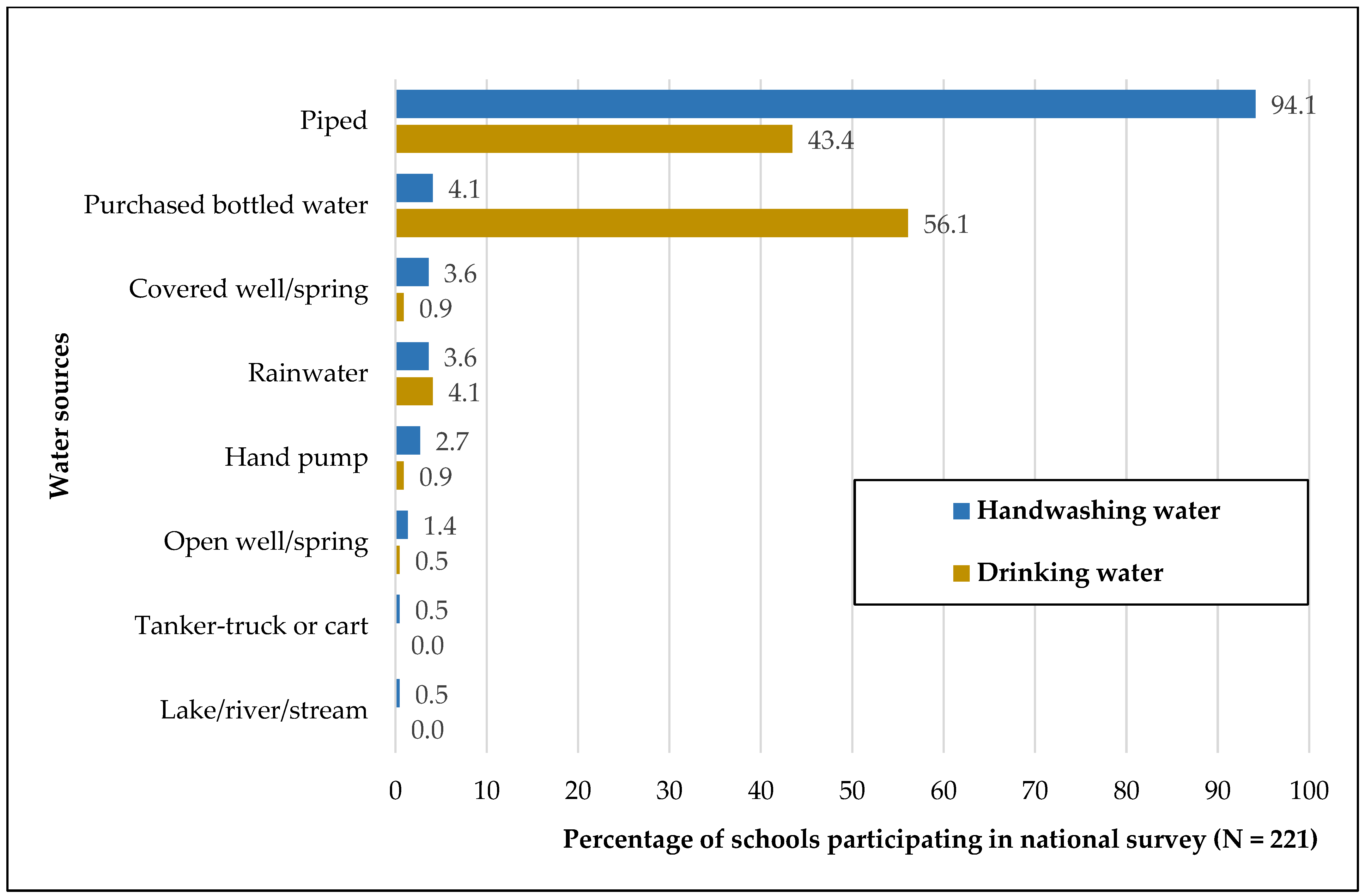
3.1. National Survey
3.2. Pilot School Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 6 September 2023).
- Troeger, C.; Blacker, B.F.; Khalil, I.A.; Rao, P.C.; Cao, S.; Zimsen, S.R.; Albertson, S.B.; Stanaway, J.D.; Deshpande, A.; Abebe, Z.; et al. Estimates of the Global, Regional, and National Morbidity, Mortality, and Aetiologies of Diarrhoea in 195 Countries: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar] [CrossRef] [PubMed]
- Wolf, J.; Johnston, R.B.; Ambelu, A.; Arnold, B.F.; Bain, R.; Brauer, M.; Brown, J.; Caruso, B.A.; Clasen, T.; Colford, J.M.; et al. Burden of Disease Attributable to Unsafe Drinking Water, Sanitation, and Hygiene in Domestic Settings: A Global Analysis for Selected Adverse Health Outcomes. Lancet 2023, 401, 2060–2071. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Goal 6: Ensure Access to Water and Sanitation for All. Available online: https://www.un.org/sustainabledevelopment/water-and-sanitation/ (accessed on 6 September 2023).
- United Nations. Goal 4: Quality Education. Available online: https://www.un.org/sustainabledevelopment/education/ (accessed on 6 September 2023).
- World Health Organization; UNICEF. Joint Monitoring Programme: WASH in Schools. Available online: https://washdata.org/data/school#!/ (accessed on 6 September 2023).
- World Health Organization. Advice for the Public: Coronavirus Disease (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 6 September 2023).
- U.S. Centers for Disease Control and Prevention. Keeping Hands Clean. Available online: https://www.cdc.gov/hygiene/personal-hygiene/hands.html (accessed on 6 September 2023).
- Statistical Institute of Belize. Multidimensional Poverty in Belize. Available online: https://sib.org.bz/wp-content/uploads/MPI_Infographic_v03.pdf (accessed on 6 September 2023).
- Tomassini, M. 5 Ways COVID-19 Is Affecting Children in Belize and How UNICEF Is Helping. Available online: https://www.unicef.org/belize/stories/5-ways-covid-19-affecting-children-belize (accessed on 6 September 2023).
- Chatterley, C. National Assessment of WASH in Schools—Belize. Available online: https://issuu.com/unicefbelize/docs/final_wash_assessment (accessed on 6 September 2023).
- World Health Organization; UNICEF. Core Questions and Indicators for Monitoring WASH in Schools in the Sustainable Development Goals. World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)—A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata Statistical Software: Release 17. 2021. [Google Scholar]
- Channel 5. Belize Hybrid Classes Will Resume January 10th. Available online: https://edition.channel5belize.com/archives/228348 (accessed on 6 September 2023).
- Government of Belize Press Office. COVID-19 Vaccines Now Available for Children Five to 11 Years. Available online: https://www.pressoffice.gov.bz/covid-19-vaccines-now-available-for-children-five-to-11-years/ (accessed on 18 February 2024).
- World Health Organization. Belize: WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int (accessed on 10 September 2022).
- World Health Organization. Statement on the Fifteenth Meeting of the IHR (2005) Emergency Committee on the COVID-19 Pandemic. Available online: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(COVID-19)-pandemic (accessed on 6 September 2023).
- Poague, K.I.H.M.; Blanford, J.I.; Anthonj, C. Water, Sanitation and Hygiene in Schools in Low- and Middle-Income Countries: A Systematic Review and Implications for the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 3124. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; UNICEF. Disability-Inclusive WASH in Schools. Available online: https://washdata.org/monitoring/wash-schools/disability-inclusive-wash-schools (accessed on 7 September 2023).
- UNICEF. Water, Sanitation and Hygiene (W.A.S.H). Available online: https://www.unicef.org/belize/water-sanitation-and-hygiene-wash (accessed on 6 September 2023).
- Karon, A.J.; Cronin, A.A.; Cronk, R.; Hendrawan, R. Improving Water, Sanitation, and Hygiene in Schools in Indonesia: A Cross-Sectional Assessment on Sustaining Infrastructural and Behavioral Interventions. Int. J. Hyg. Environ. Health 2017, 220, 539–550. [Google Scholar] [CrossRef] [PubMed]
- Vally, H.; McMichael, C.; Doherty, C.; Li, X.; Guevarra, G.; Tobias, P. The Impact of a School-Based Water, Sanitation and Hygiene Intervention on Knowledge, Practices, and Diarrhoea Rates in the Philippines. Int. J. Environ. Res. Public Health 2019, 16, 4056. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Criterion | Score |
|---|---|
| Handwashing station | |
| No functional handwashing station | 5 |
| Functional handwashing station present | 0 |
| Soap | |
| No soap available | 4 |
| There is sometimes soap available | 3 |
| There is always soap available | 0 |
| Alcohol-based hand rub (ABHR) | |
| No ABHR available | 3 |
| There is sometimes ABHR available | 2 |
| There is always ABHR available | 0 |
| Water | |
| There are times when water is not available | 2 |
| Water is always available | 0 |
| There is a concern about water quality | 1 |
| There is no concern about water quality | 0 |
| Schools that Did not Complete the National Survey (N = 87) n (%) | Schools That Completed the National Survey (N = 221) n (%) | Pilot Schools Selected for Intervention (N = 12) n (%) | |
|---|---|---|---|
| District ** | |||
| Corozal | 3 (3) | 44 (20) | 2 (17) |
| Orange Walk | 4 (5) | 35 (16) | 2 (17) |
| Belize | 15 (17) | 49 (22) | 2 (17) |
| Cayo | 35 (40) | 34 (15) | 2 (17) |
| Stann Creek | 7 (8) | 24 (11) | 2 (17) |
| Toledo | 23 (26) | 35 (16) | 2 (17) |
| Locality | |||
| Rural | 60 (69) | 146 (66) | 10 (83) |
| Urban | 27 (31) | 75 (34) | 2 (17) |
| Grade level ** | |||
| Primary | 67 (77) | 191 (86) | 12 (100) |
| Secondary | 20 (23) | 30 (14) | 0 (0) |
| School operation | |||
| Open/Hybrid | - | 84 (38) | 12 (100) * |
| Closed | - | 137 (62) | 0 (0) |
| Number of classrooms, median (IQR) | - | 9 (10) | 8.5 (9) |
| Student enrollment, median (IQR) | - | 195 (246) | 177 (185) |
| Questions from the National Survey | N = 221 n (%) |
|---|---|
| There are times when water is not available | 121 (55) |
| Concerns about water quality | 65 (29) |
| Type of concern * | |
| Color of water | 28 (13) |
| Smell of water | 14 (6) |
| Taste of water | 32 (14) |
| Contamination of water source | 24 (11) |
| There is a handwashing station | 219 (99) |
| There is a functional handwashing station | 197 (89) |
| There is soap available for handwashing | |
| Always | 103 (47) |
| Sometimes | 110 (50) |
| Never | 6 (3) |
| There is alcohol-based hand rub available for students | |
| Always | 45 (20) |
| Sometimes | 89 (40) |
| Never | 87 (39) |
| There are restrooms separated by sex | 210 (95) |
| Most common type of toilet on school ground | |
| Flush/pour-flush toilet | 200 (91) |
| Pit latrines with slab | 16 (7) |
| Pit latrines without a slab | 2 (1) |
| Baseline | Follow-Up | Percent Change | p-Value | |
|---|---|---|---|---|
| Handwashing Station | ||||
| Total handwashing access points | 165 | 142 | - | - |
| Functional handwashing access points ** | 150 (91%) | 114 (80%) | −11% | 0.007 |
| Functional handwashing access points with soap, n (%) † | 111 (74%) | 83 (73%) | −1% | 0.828 |
| Functional handwashing access points with paper towels, n (%) † | 63 (42%) | 50 (44%) | +2% | 0.762 |
| Functional handwashing access points accessible for individuals with disabilities, n (%) † | 91 (61%) | 50 (44%) | −17% | 0.007 |
| Functional handwashing access points accessible for small children, n (%) † | 126 (84%) | 63 (55%) | −29% | <0.001 |
| ABHR | ||||
| Total ABHR dispensers | 119 | 94 | ||
| Functional ABHR dispensers | 115 (97%) | 79 (84%) | −13% | 0.001 |
| Restrooms | ||||
| Total restrooms | 61 | 53 | ||
| Restrooms with a handwashing station with water within 5 m, n (%) | 53 (87%) | 39 (74%) | −13% | 0.073 |
| Restrooms with a handwashing station with water and soap within 5 m, n (%) | 42 (69%) | 35 (66%) | −3% | 0.749 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ly, A.N.; McDavid, K.; Craig, C.; Maheia, D.; Gongora, Y.; Medley, A.; Morey, F.; Manzanero, R.; Morazan, G.; Lino, A.; et al. Water, Sanitation, and Hygiene Infrastructure and Resources in Schools in Belize during the COVID-19 Pandemic, 2021–2023. Int. J. Environ. Res. Public Health 2024, 21, 470. https://doi.org/10.3390/ijerph21040470
Ly AN, McDavid K, Craig C, Maheia D, Gongora Y, Medley A, Morey F, Manzanero R, Morazan G, Lino A, et al. Water, Sanitation, and Hygiene Infrastructure and Resources in Schools in Belize during the COVID-19 Pandemic, 2021–2023. International Journal of Environmental Research and Public Health. 2024; 21(4):470. https://doi.org/10.3390/ijerph21040470
Chicago/Turabian StyleLy, Anh N., Kelsey McDavid, Christina Craig, Dian Maheia, Yolanda Gongora, Alexandra Medley, Francis Morey, Russell Manzanero, Gerhaldine Morazan, Allison Lino, and et al. 2024. "Water, Sanitation, and Hygiene Infrastructure and Resources in Schools in Belize during the COVID-19 Pandemic, 2021–2023" International Journal of Environmental Research and Public Health 21, no. 4: 470. https://doi.org/10.3390/ijerph21040470
APA StyleLy, A. N., McDavid, K., Craig, C., Maheia, D., Gongora, Y., Medley, A., Morey, F., Manzanero, R., Morazan, G., Lino, A., Romero, V., Blanco, R., Ishida, K., Lozier, M., & Murray, K. O. (2024). Water, Sanitation, and Hygiene Infrastructure and Resources in Schools in Belize during the COVID-19 Pandemic, 2021–2023. International Journal of Environmental Research and Public Health, 21(4), 470. https://doi.org/10.3390/ijerph21040470