
A Comparison of Oral Function in Older In- and Outpatients: An Observational Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
- -
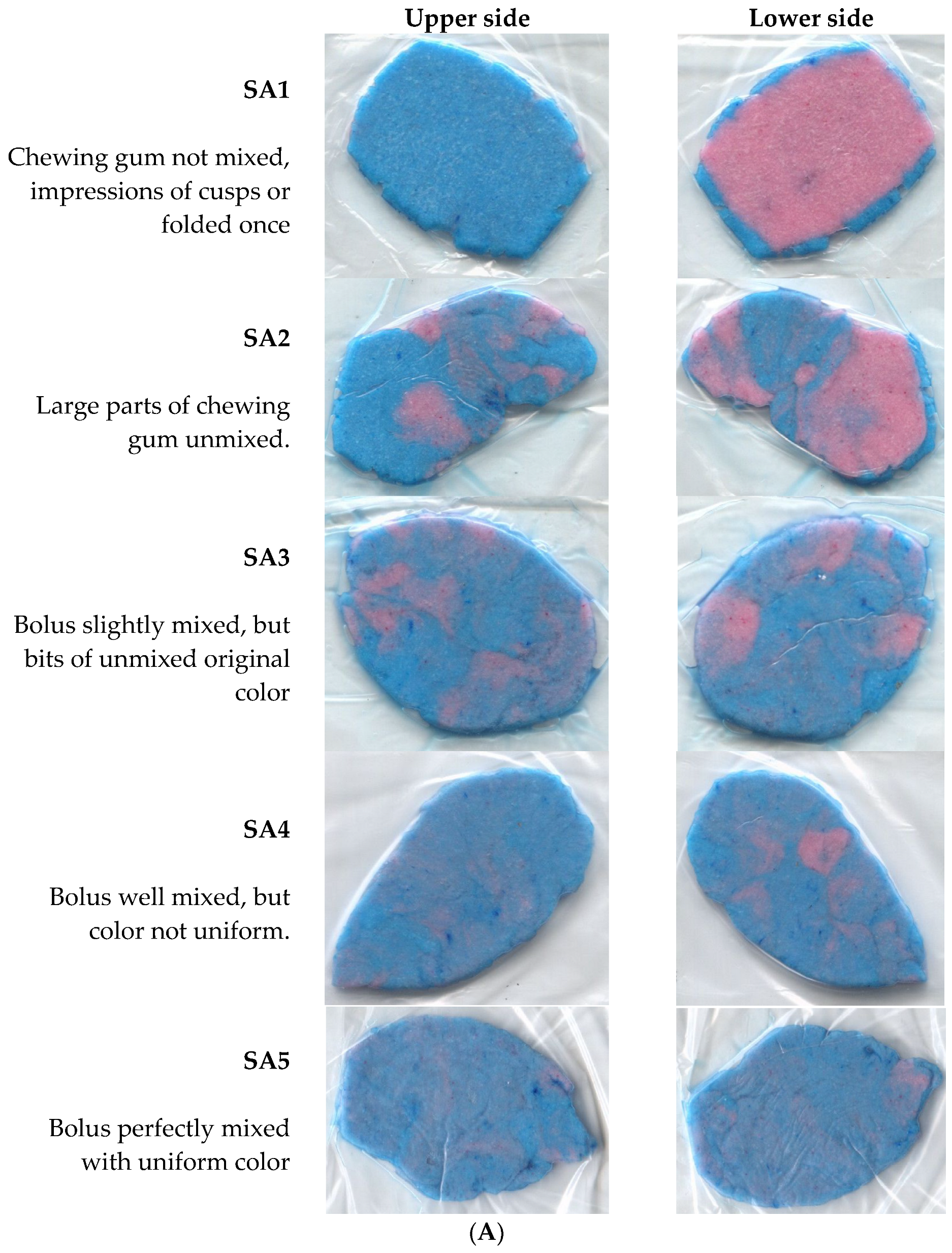
- SA1 chewing gum not mixed, impressions of cusps or folded once.
- -
- SA2 large parts of chewing gum unmixed.
- -
- SA3 bolus slightly mixed, but bits of unmixed original color.
- -
- SA4 bolus well mixed, but color not uniform.
- -
- SA5 bolus perfectly mixed with uniform color.
Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- (BFS) BfS. Lebenserwartung in der Schweiz 2022. Available online: https://www.bfs.admin.ch/bfs/de/home/statistiken/bevoelkerung/geburten-todesfaelle/lebenserwartung.html (accessed on 1 May 2024).
- Watanabe, Y.; Okada, K.; Kondo, M.; Matsushita, T.; Nakazawa, S.; Yamazaki, Y. Oral health for achieving longevity. Geriatr. Gerontol. Int. 2020, 20, 526–538. [Google Scholar] [CrossRef] [PubMed]
- Anliker, N.; Molinero-Mourelle, P.; Weijers, M.; Bukvic, H.; Bornstein, M.M.; Schimmel, M. Dental status and its correlation with polypharmacy and multimorbidity in a Swiss nursing home population: A cross-sectional study. Clin. Oral Investig. 2023, 27, 3021–3028. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.; Wallace, J.; Doshi, M.; Gadanya, M.; Ben Yahya, I.; Roseman, J.; Srisilapanan, P. Oral health for healthy ageing. Lancet Health Longev. 2021, 2, e521–e527. [Google Scholar] [CrossRef] [PubMed]
- Sakai, K.; Nakayama, E.; Yoneoka, D.; Sakata, N.; Iijima, K.; Tanaka, T.; Hayashi, K.; Sakuma, K.; Hoshino, E. Association of Oral Function and Dysphagia with Frailty and Sarcopenia in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. Cells 2022, 11, 2199. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tanaka, T.; Takahashi, K.; Hirano, H.; Kikutani, T.; Watanabe, Y.; Ohara, Y.; Furuya, H.; Tetsuo, T.; Akishita, M.; Iijima, K.; et al. Oral Frailty as a Risk Factor for Physical Frailty and Mortality in Community-Dwelling Elderly. J. Gerontol. Ser. A 2018, 73, 1661–1667. [Google Scholar] [CrossRef] [PubMed]
- Tôrres, L.H.D.N.; Tellez, M.; Hilgert, J.B.; Hugo, F.N.; Sousa, M.d.L.R.d.; Ismail, A.I. Frailty, Frailty Components, and Oral Health: A Systematic Review. J. Am. Geriatr. Soc. 2015, 63, 2555–2562. [Google Scholar] [CrossRef] [PubMed]
- Dibello, V.; Zupo, R.; Sardone, R.; Lozupone, M.; Castellana, F.; Dibello, A.; Daniele, A.; De Pergola, G.; Bortone, I.; Lampignano, L.; et al. Oral frailty and its determinants in older age: A systematic review. Lancet Health Longev. 2021, 2, e507–e520. [Google Scholar] [CrossRef] [PubMed]
- Murotani, Y.; Hatta, K.; Takahashi, T.; Gondo, Y.; Kamide, K.; Kabayama, M.; Masui, Y.; Ishizaki, T.; Matsuda, K.-I.; Mihara, Y.; et al. Oral Functions Are Associated with Muscle Strength and Physical Performance in Old-Old Japanese. Int. J. Environ. Res. Public Health 2021, 18, 13199. [Google Scholar] [CrossRef] [PubMed]
- Nagamine, Y.; Kamitani, T.; Yamazaki, H.; Ogawa, Y.; Fukuhara, S.; Yamamoto, Y. Poor oral function is associated with loss of independence or death in functionally independent older adults. PLoS ONE 2021, 16, e0253559. [Google Scholar] [CrossRef]
- Dibello, V.; Lobbezoo, F.; Lozupone, M.; Sardone, R.; Ballini, A.; Berardino, G.; Mollica, A.; Coelho-Júnior, H.J.; De Pergola, G.; Stallone, R.; et al. Oral frailty indicators to target major adverse health-related outcomes in older age: A systematic review. GeroScience 2023, 45, 663–706. [Google Scholar] [CrossRef] [PubMed]
- Schimmel, M.; Aarab, G.; Baad-Hansen, L.; Lobbezoo, F.; Svensson, P. A conceptual model of oro-facial health with an emphasis on function. J. Oral Rehabil. 2021, 48, 1283–1294. [Google Scholar] [CrossRef] [PubMed]
- Nagatani, M.; Tanaka, T.; Son, B.-K.; Kawamura, J.; Tagomori, J.; Hirano, H.; Shirobe, M.; Iijima, K. Oral frailty as a risk factor for mild cognitive impairment in community-dwelling older adults: Kashiwa study. Exp. Gerontol. 2023, 172, 112075. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Shu, X.; Leung, K.C.M.; Lo, E.C.M. Associations of general health conditions with masticatory performance and maximum bite force in older adults: A systematic review of cross-sectional studies. J. Dent. 2022, 123, 104186. [Google Scholar] [CrossRef] [PubMed]
- Lahoud, T.; Yu, A.Y.; King, S. Masticatory dysfunction in older adults: A scoping review. J. Oral Rehabil. 2023, 50, 724–737. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Hama, Y.; Futatsuya, R.; Sasaki, Y.; Noritake, K.; Yamaguchi, K.; Matsuzaki, M.; Kubota, C.; Hosoda, A.; Minakuchi, S. Association between Masticatory Performance, Nutritional Intake, and Frailty in Japanese Older Adults. Nutrients 2023, 15, 5075. [Google Scholar] [CrossRef] [PubMed]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M.; et al. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef] [PubMed]
- de Smit, M.J.; Nijholt, W.; Bakker, M.H.; Visser, A. The predictive value of masticatory function for adverse health outcomes in older adults: A systematic review. J. Nutr. Health Aging 2024, 28, 100210. [Google Scholar] [CrossRef] [PubMed]
- Ikebe, K.; Matsuda, K.-I.; Murai, S.; Maeda, Y.; Nokubi, T. Validation of the Eichner index in relation to occlusal force and masticatory performance. Int. J. Prosthodont. 2010, 23, 521–524. [Google Scholar] [PubMed]
- Schimmel, M.; Christou, P.; Miyazaki, H.; Halazonetis, D.; Herrmann, F.R.; Müller, F. A novel colourimetric technique to assess chewing function using two-coloured specimens: Validation and application. J. Dent. 2015, 43, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Buser, R.; Ziltener, V.; Samietz, S.; Fontolliet, M.; Nef, T.; Schimmel, M. Validation of a purpose-built chewing gum and smartphone application to evaluate chewing efficiency. J. Oral Rehabil. 2018, 45, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Jockusch, J.; Hopfenmüller, W.; Nitschke, I. Chewing function and related parameters as a function of the degree of dementia: Is there a link between the brain and the mouth? J. Oral Rehabil. 2021, 48, 1160–1172. [Google Scholar] [CrossRef] [PubMed]
- Andersson, P.; Ekstam, A.K. Impaired Oral Health in Older Orthopaedic In-Care Patients: The Influence of Medication and Morbidity. Clin. Interv. Aging 2021, 16, 1691–1702. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Shu, X.; Leung, K.C.M.; Lo, E.C.M. Association between masticatory performance and oral conditions in adults: A systematic review and meta-analysis. J. Dent. 2023, 129, 104395. [Google Scholar] [CrossRef] [PubMed]
- Komiyama, T.; Ohi, T.; Miyoshi, Y.; Tomata, Y.; Zhang, S.; Tsuji, I.; Watanabe, M.; Hattori, Y. Verification of the criteria for reduced occlusal force to diagnose oral hypofunction in older Japanese people: A prospective cohort study on incident functional disability. J. Oral Rehabil. 2020, 47, 989–997. [Google Scholar] [CrossRef] [PubMed]
- Hatta, K.; Murotani, Y.; Takahashi, T.; Gondo, Y.; Kamide, K.; Masui, Y.; Ishizaki, T.; Ogata, S.; Matsuda, K.; Mihara, Y.; et al. Decline of oral functions in old-old adults and their relationship with age and sex: The SONIC study. J. Am. Geriatr. Soc. 2022, 70, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Higashi, K.; Hatta, K.; Mameno, T.; Takahashi, T.; Gondo, Y.; Kamide, K.; Masui, Y.; Ishizaki, T.; Arai, Y.; Kabayama, M.; et al. The relationship between changes in occlusal support and masticatory performance using 6-year longitudinal data from the SONIC study. J. Dent. 2023, 139, 104763. [Google Scholar] [CrossRef] [PubMed]
- Schimmel, M.; Christou, P.; Herrmann, F.; Müller, F. A two-colour chewing gum test for masticatory efficiency: Development of different assessment methods. J. Oral Rehabil. 2007, 34, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Miyahara, S.; Maeda, K.; Kawamura, K.; Matsui, Y.; Satake, S.; Arai, H.; Umegaki, H. Association between intrinsic capacity and oral health in older patients in a frailty clinic. Eur. Geriatr. Med. 2024, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Robison, R.; Garand, K.L.; Affoo, R.; Yeh, C.-K.; Chin, N.; McArthur, C.; Pulia, M.; Rogus-Pulia, N. New horizons in understanding oral health and swallowing function within the context of frailty. Age Ageing 2023, 52, afac276. [Google Scholar] [CrossRef]
- Jockusch, J.; Hahnel, S.; Sobotta, B.B.A.J.; Nitschke, I. The Effect of a Masticatory Muscle Training Program on Chewing Efficiency and Bite Force in People with Dementia. Int. J. Environ. Res. Public Health 2022, 19, 3778. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall (n = 62) | Outpatients (n = 31) | Inpatients (n = 31) | p-Value |
|---|---|---|---|---|
| Age, mean (sd) | 81.9 (5.2) | 80.7 (4.3) | 83.1 (5.9) | 0.08 |
| Female sex, n (%) | 39 (62.9) | 18 (58.1) | 21 (67.7) | 0.43 |
| Eruptive teeth (n), mean (sd) | 10.56 (9.2) | 9.1 (7.9) | 12.0 (10.3) | 0.21 |
| Dentures upper jaw, n (%) | n.a. | |||
| -Natural teeth | 15 (24.2) | 4 (12.9) | 11 (35.5) | |
| -Partial dentures | 22 (35.5) | 17 (54.8) | 5 (16.1) | |
| -Total dentures | 25 (40.3) | 10 (32.3) | 15 (48.4) | |
| Dentures lower jaw, n (%) | n.a. | |||
| -Natural teeth | 23 (37.1) | 6 (19.4) | 17 (54.8) | |
| -Partial dentures | 28 (45.2) | 23 (74.2) | 5 (16.1) | |
| -Total dentures | 11 (17.7) | 2 (6.4) | 9 (29.0) | |
| Bite force (N), mean (sd) | 247 (261) | 212.2 (178.6) | 283.1 (323.5) | 0.29 |
| Bite force display area (mm2), mean (sd) | 6.5 (5.9) | 5.6 (4.1) | 6.2 (4.8) | 0.60 |
| Average pressure (N/mm2), mean (sd) | 32.8 (11.6) | 34.7 (11.0) | 31.0 (12.2) | 0.22 |
| Maximum pressure (N/mm2), mean (sd) | 77.7 (38.3) | 79.5 (35.6) | 76.2 (37.3) | 0.72 |
| Force distribution right side (%), mean (sd) | 47.9 (24.5) | 49.3 (22.5) | 46.6 (26.7) | 0.67 |
| Force distribution left side (%), mean (sd) | 45.6 (24.2) | 47.6 (22.4) | 43.7 (26.1) | 0.53 |
| Supporting zones with dentures (n), median (IQR) | 4 (3–4) | 4 (4–4) | 4 (2–4) | 0.03 |
| Eichner classification with dentures, median (IQR) | A1 (A1–B1) | A1 (A1–A1) | A3 (A1–B2) | <0.01 |
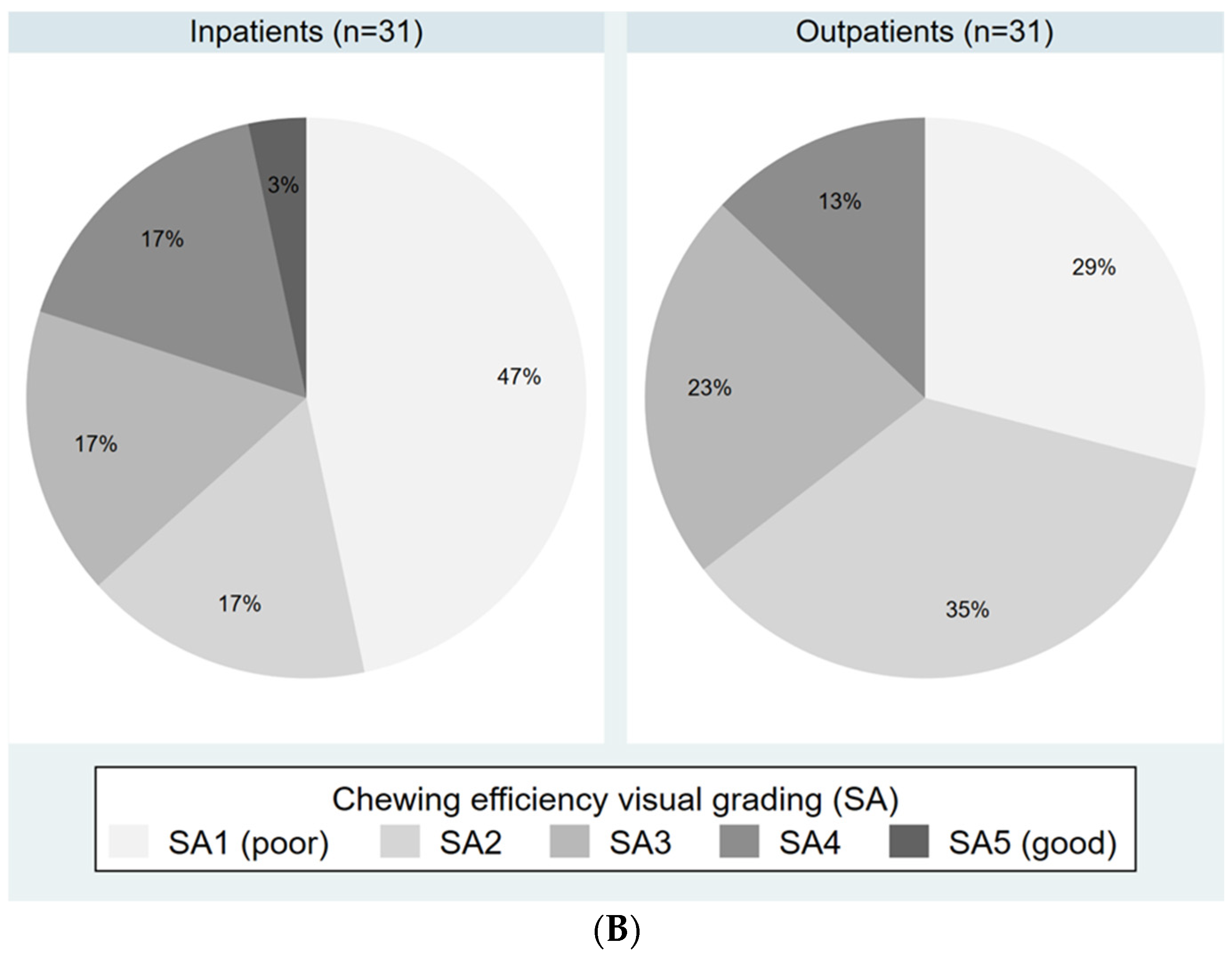
| Masticatory performance, visual scale, median (IQR) | SA2 b (SA1–SA3) | SA2 (SA1–SA3) | SA2 a (SA1–SA3) | 0.59 |
| Masticatory performance, digital scale (VoH), mean (sd) | 0.46 b (0.22) | 0.44 (0.20) | 0.48 a (0.25) | 0.49 |
| Oral Health Variable | N (%) Inpatients with Normal Masticatory Performance | N (%) Inpatients with Low Masticatory Performance | Crude OR (95% CI) | p-Value | Adjusted OR (95% CI) b | p-Value | Full Model OR (95%CI) c | p-Value |
|---|---|---|---|---|---|---|---|---|
| Maximum bite force | ||||||||
| Normal (>265 N) | 15 (68.2%) | 7 (18.0%) | Reference | Reference | ||||
| Low (≤265 N) | 7 (31.8%) | 32 (82.1%) | 9.8 (2.9–33.0) | <0.01 | 9.6 (2.8–32.7) | <0.01 | 7.4 (1.8–30.4) | <0.01 |
| Eruptive teeth | ||||||||
| ≥10 | 18 (81.8%) | 12 (30.8%) | Reference | Reference | ||||
| 0–9 | 4 (18.2%) | 27 (69.2%) | 10.1 (2.8–36.4) | <0.01 | 9.6 (2.7–35.1) | <0.01 | 7.8 (1.7–36.4) | <0.01 |
| Supporting zones with dentures | ||||||||
| 3–4 | 19 (86.4%) | 30 (61.2%) | Reference | Reference | ||||
| Low (0–2) | 3 (13.6%) | 39 (63.9%) | 1.9 (0.5–7.9) | 0.38 | 2.2 (0.5–9.7) | 0.30 | 4.9 (0.7–34.7) | 0.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eggimann, A.K.; Badura, L.; Zehnder, R.; Koemeda, M.; Buser, R.; Schimmel, M. A Comparison of Oral Function in Older In- and Outpatients: An Observational Study. Int. J. Environ. Res. Public Health 2024, 21, 995. https://doi.org/10.3390/ijerph21080995
Eggimann AK, Badura L, Zehnder R, Koemeda M, Buser R, Schimmel M. A Comparison of Oral Function in Older In- and Outpatients: An Observational Study. International Journal of Environmental Research and Public Health. 2024; 21(8):995. https://doi.org/10.3390/ijerph21080995
Chicago/Turabian StyleEggimann, Anna K., Leo Badura, Rahel Zehnder, Miriam Koemeda, Ramona Buser, and Martin Schimmel. 2024. "A Comparison of Oral Function in Older In- and Outpatients: An Observational Study" International Journal of Environmental Research and Public Health 21, no. 8: 995. https://doi.org/10.3390/ijerph21080995
APA StyleEggimann, A. K., Badura, L., Zehnder, R., Koemeda, M., Buser, R., & Schimmel, M. (2024). A Comparison of Oral Function in Older In- and Outpatients: An Observational Study. International Journal of Environmental Research and Public Health, 21(8), 995. https://doi.org/10.3390/ijerph21080995