
The Worldwide Prevalence of Internet Addiction among Medical Students: A Systematic Review and Meta-Analysis

 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Registration, Study Design, Search Strategy, and Eligibility Criteria
2.2. Study Selection
2.3. Bias Risk Assessment
2.4. Data Extraction
2.5. Statistical Analyses
3. Results
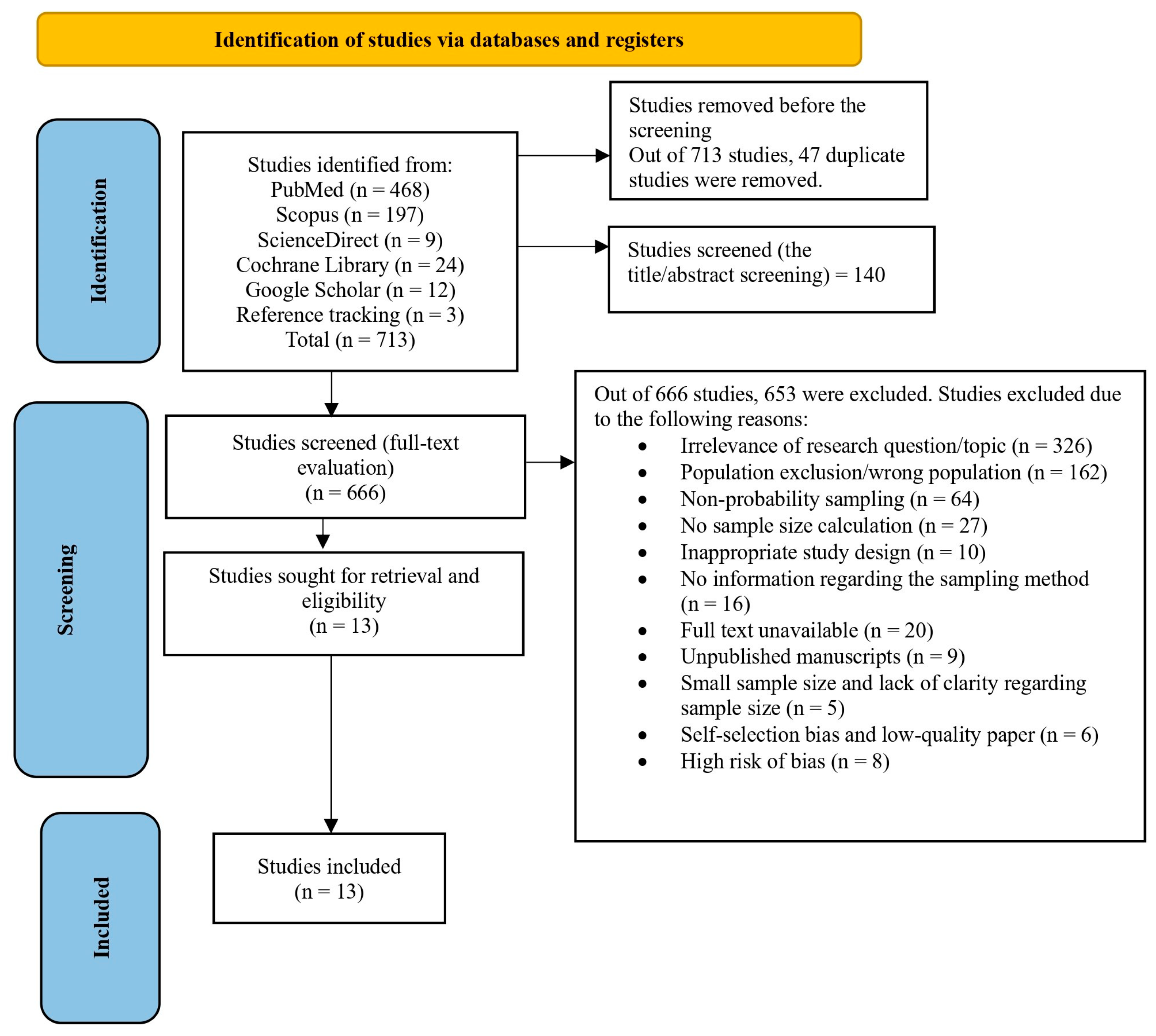
3.1. Study Selection, Sample Size, and Risk of Bias Assessment
3.2. Overview of Included Studies
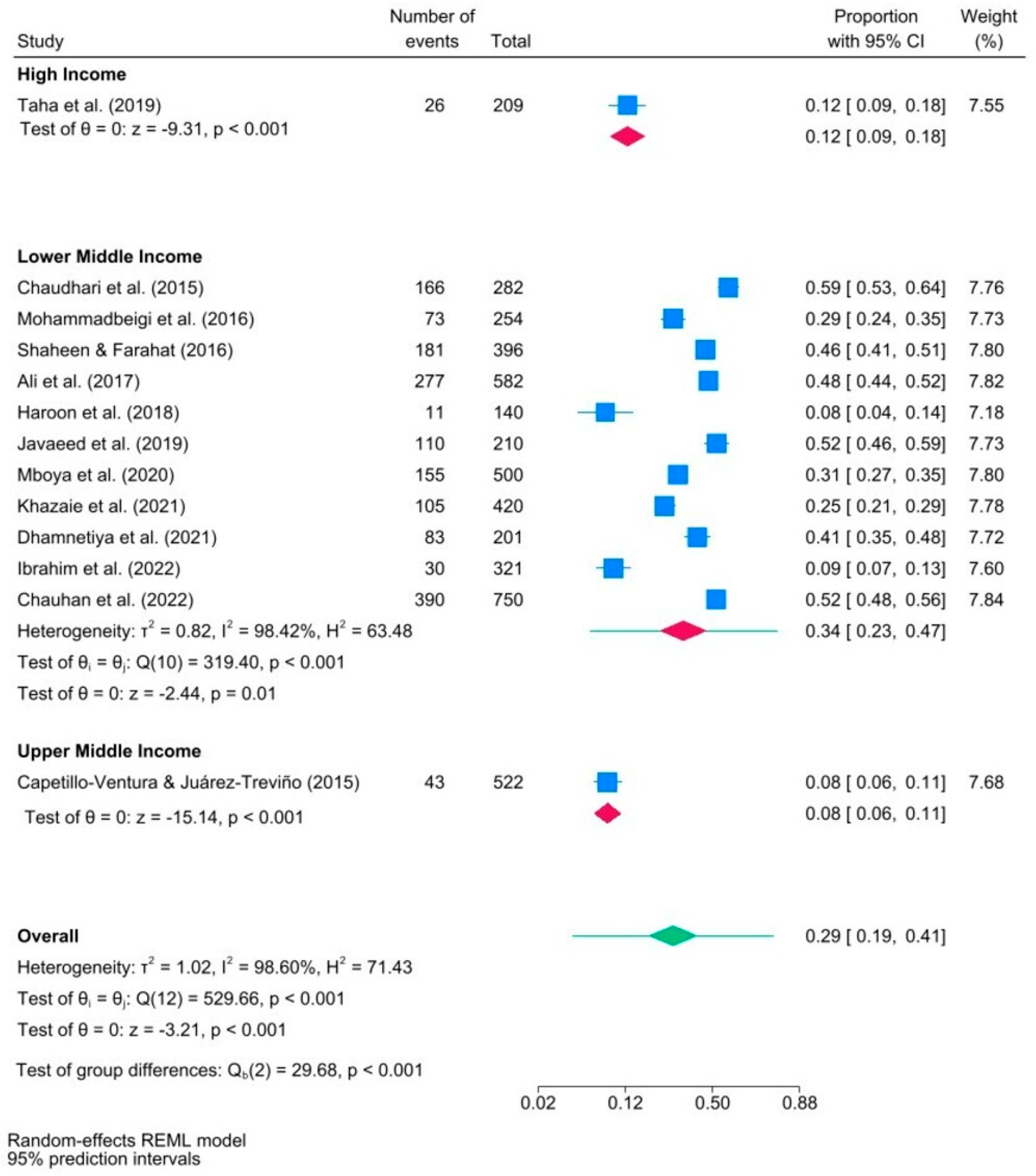
3.3. Cumulative and Subgroup Meta-Analyses
3.4. Meta-Regression Analysis, Leave-One-Out Analysis, and Publication Bias Assessment
4. Discussion
Limitations, Practical Implications, and Future Research Suggestions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, M.W.B.; Lim, R.B.C.; Lee, C.; Ho, R.C.M. Prevalence of Internet Addiction in Medical Students: A Meta-Analysis. Acad. Psychiatry 2018, 42, 88–93. [Google Scholar] [CrossRef]
- Alavi, S.S.; Ferdosi, M.; Jannatifard, F.; Eslami, M.; Alaghemandan, H.; Setare, M. Behavioral Addiction versus Substance Addiction: Correspondence of Psychiatric and Psychological Views. Int. J. Prev. Med. 2012, 3, 290–294. [Google Scholar] [PubMed]
- Cheng, C.; Li, A.Y. Internet Addiction Prevalence and Quality of (Real) Life: A Meta-Analysis of 31 Nations Across Seven World Regions. Cyberpsychology Behav. Soc. Netw. 2014, 17, 755–760. [Google Scholar] [CrossRef]
- Goldberg, I. Internet Addiction Disorder 1995.
- Kumar, S.; Kumar, A.; Badiyani, B.; Singh, S.K.; Gupta, A.; Ismail, M.B. Relationship of Internet Addiction with Depression and Academic Performance in Indian Dental Students. Med. Pharm. Rep. 2018, 91, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Xi, H.; Zhu, Q.; Wang, Z.; Han, L.; Liu, S.; Bai, W.; Zhao, Y.; Chen, L.; Ge, Z.; et al. Prevalence of Problematic Internet Use and Its Association with Quality of Life among Undergraduate Nursing Students in the Later Stage of COVID-19 Pandemic Era in China. Am. J. Addict. 2021, 30, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Capetillo-Ventura, N.; Juárez-Treviño, M. Internet Addiction in University Medical Students. Med. Univ. 2015, 17, 88–93. [Google Scholar] [CrossRef]
- Duc, T.Q.; Chi, V.T.Q.; Huyen, N.T.H.; Quang, P.N.; Thuy, B.T.; Nguyen Di, K. Growing Propensity of Internet Addiction among Asian College Students: Meta-Analysis of Pooled Prevalence from 39 Studies with over 50,000 Participants. Public Health 2024, 227, 250–258. [Google Scholar] [CrossRef]
- Chou, C.; Condron, L.; Belland, J.C. A Review of the Research on Internet Addiction. Educ. Psychol. Rev. 2005, 17, 363–388. [Google Scholar] [CrossRef]
- Grant, J.E.; Chamberlain, S.R. Expanding the Definition of Addiction: DSM-5 vs. ICD-11. CNS Spectr. 2016, 21, 300–303. [Google Scholar] [CrossRef] [PubMed]
- Bleakley, A.; Park, S.; Romer, D. Internet Addiction. In Treating and Preventing Adolescent Mental Health Disorders; Oxford University Press: Oxford, UK, 2017; pp. 585–596. ISBN 978-0-19-992816-3. [Google Scholar]
- Kaess, M.; Klar, J.; Kindler, J.; Parzer, P.; Brunner, R.; Carli, V.; Sarchiapone, M.; Hoven, C.W.; Apter, A.; Balazs, J.; et al. Excessive and Pathological Internet Use—Risk-Behavior or Psychopathology? Addict. Behav. 2021, 123, 107045. [Google Scholar] [CrossRef]
- Salehi, M.; Norozi Khalili, M.; Hojjat, S.K.; Salehi, M.; Danesh, A. Prevalence of Internet Addiction and Associated Factors among Medical Students from Mashhad, Iran in 2013. Iran. Red Crescent Med. J. 2014, 16, e17256. [Google Scholar] [CrossRef] [PubMed]
- Bai, W.; Cai, H.; Wu, S.; Zhang, L.; Feng, K.-X.; Li, Y.-C.; Liu, H.-Z.; Du, X.; Zeng, Z.-T.; Lu, C.-M.; et al. Internet Addiction and Its Association with Quality of Life in Patients with Major Depressive Disorder: A Network Perspective. Transl. Psychiatry 2022, 12, 138. [Google Scholar] [CrossRef]
- Chung, S.; Lee, J.; Lee, H.K. Personal Factors, Internet Characteristics, and Environmental Factors Contributing to Adolescent Internet Addiction: A Public Health Perspective. Int. J. Environ. Res. Public. Health 2019, 16, 4635. [Google Scholar] [CrossRef]
- Brand, M. Theoretical Models of the Development and Maintenance of Internet Addiction. In Internet Addiction; Montag, C., Reuter, M., Eds.; Studies in Neuroscience, Psychology and Behavioral Economics; Springer International Publishing: Cham, Switzerland, 2017; pp. 19–34. ISBN 978-3-319-46275-2. [Google Scholar]
- Mohamed, K.O.; Soumit, S.M.; Elseed, A.A.; Allam, W.A.; Soomit, A.M.; Humeda, H.S. Prevalence of Internet Addiction and Its Associated Risk Factors among Medical Students in Sudan: A Cross-Sectional Study. Cureus 2024, 16, e53543. [Google Scholar] [CrossRef]
- Ibrahim, A.K.; Fouad, I.; Kelly, S.J.; El Fawal, B.; Ahmed, G.K. Prevalence and Determinants of Internet Addiction among Medical Students and Its Association with Depression. J. Affect. Disord. 2022, 314, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Javaeed, A.; Zafar, M.B.; Iqbal, M.; Ghauri, S.K. Correlation between Internet Addiction, Depression, Anxiety and Stress among Undergraduate Medical Students in Azad Kashmir. Pak. J. Med. Sci. 2019, 35, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, H.M.; Farahat, T.M. Problematic Internet Use among Medical School Students in Menoufia University Egypt. J. Child Adolesc. Behav. 2016, 4, 298. [Google Scholar] [CrossRef]
- Chauhan, N.; Tiwari, P.; Ahlawat, P.; Singh, S.K.; Kamble, B.D.; Mahaur, G. Internet Addiction and Sleep Quality among Medical Students of Delhi: A New Age Epidemic. Natl. J. Community Med. 2022, 13, 864–868. [Google Scholar] [CrossRef]
- Ali, R.; Mohammed, N.; Aly, H. Internet Addiction among Medical Students of Sohag University, Egypt. J. Egypt. Public Health Assoc. 2017, 92, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Chaudhari, B.; Menon, P.; Saldanha, D.; Tewari, A.; Bhattacharya, L. Internet Addiction and Its Determinants among Medical Students. Ind. Psychiatry J. 2015, 24, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Javaeed, A.; Jeelani, R.; Gulab, S.; Ghauri, S.K. Relationship between Internet Addiction and Academic Performance of Undergraduate Medical Students of Azad Kashmir. Pak. J. Med. Sci. 2020, 36, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Traore, B.; Aguilo, Y.; Hassoune, S.; Nani, S. Determinants of Internet Addiction among Medical Students in Casablanca: A Cross-Sectional Study. Glob. Health J. 2023, 7, 101–109. [Google Scholar] [CrossRef]
- Scafuto, F.; Ciacchini, R.; Orrù, G.; Crescentini, C.; Conversano, C.; Mastorci, F.; Porricelli, M.; Gemignani, A. COVID-19 Pandemic and Internet Addiction in Young Adults: A Pilot Study on Positive and Negative Psychosocial Correlates. Clin. Neuropsychiatry 2023, 20, 240–251. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Joanna Briggs Institute Checklist for Prevalence Studies. 2020. Available online: https://jbi.global/sites/default/files/2020-08/Checklist_for_Prevalence_Studies.pdf (accessed on 1 January 2024).
- Goplen, C.M.; Verbeek, W.; Kang, S.H.; Jones, C.A.; Voaklander, D.C.; Churchill, T.A.; Beaupre, L.A. Preoperative Opioid Use Is Associated with Worse Patient Outcomes after Total Joint Arthroplasty: A Systematic Review and Meta-Analysis. BMC Musculoskelet. Disord. 2019, 20, 234. [Google Scholar] [CrossRef]
- Mohammadbeigi, A.; Valizadeh, F.; Mirshojaee, S.R.; Ahmadli, R.; Mokhtari, M.; Ghaderi, E.; Ahmadi, A.; Rezaei, H.; Ansari, H. Self-Rated Health and Internet Addiction in Iranian Medical Sciences Students; Prevalence, Risk Factors and Complications. Int. J. Biomed. Sci. IJBS 2016, 12, 65–70. [Google Scholar] [CrossRef]
- Alavi, M.; Biros, E.; Cleary, M. A Primer of Inter-rater Reliability in Clinical Measurement Studies: Pros and Pitfalls. J. Clin. Nurs. 2022, 31, e39–e42. [Google Scholar] [CrossRef] [PubMed]
- Scarpellini, G. IDOSTATISTICS. Cohen’s Kappa Free Calc. 2022. Available online: https://idostatistics.com/cohen-kappa-free-calculator/#risultati (accessed on 1 January 2024).
- Dhand, N.K.; Khatkar, M.S. Statulator: An Online Statistical Calculator. Sample Size Calculator for Estimating a Single Proportion 2014, Statulator. Available online: https://www.statulator.com/SampleSize/ss1P.html (accessed on 16 August 2024).
- StataCorp What’s New in STATA18 (18) 2023. Available online: https://www.stata.com/new-in-stata/ (accessed on 1 January 2024).
- Dettori, J.R.; Norvell, D.C.; Chapman, J.R. Fixed-Effect vs Random-Effects Models for Meta-Analysis: 3 Points to Consider. Glob. Spine J. 2022, 12, 1624–1626. [Google Scholar] [CrossRef]
- West, S.L.; Gartlehner, G.; Mansfield, A.J.; Poole, C.; Tant, E.; Lenfestey, N.; Lux, L.J.; Amoozegar, J.; Morton, S.C.; Carey, T.C.; et al. Comparative Effectiveness Review Methods: Clinical Heterogeneity; AHRQ Methods for Effective Health Care; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2010. [Google Scholar]
- StataCorp Glossary 2023. Available online: https://www.stata.com/manuals/metaglossary.pdf (accessed on 1 January 2024).
- StataCorp STATA Meta-Analysis Reference Manual Release 18 2023. Available online: https://www.stata.com/bookstore/meta-analysis-reference-manual/ (accessed on 1 January 2024).
- Borenstein, M. How to Understand and Report Heterogeneity in a Meta-Analysis: The Difference between I-Squared and Prediction Intervals. Integr. Med. Res. 2023, 12, 101014. [Google Scholar] [CrossRef]
- Izudi, J.; Semakula, D.; Sennono, R.; Tamwesigire, I.K.; Bajunirwe, F. Protocol for Systematic Review and Meta-Analysis of Treatment Success Rate among Adult Patients with Tuberculosis in Sub-Saharan Africa. BMJ Open 2018, 8, e024559. [Google Scholar] [CrossRef] [PubMed]
- Lifeng, L.; Haitao, C. Quantifying Publication Bias in Meta-Analysis. Biometrics 2018, 74, 785–794. [Google Scholar] [CrossRef]
- Our World in Data WHO Regions n.d. Available online: https://ourworldindata.org/grapher/who-regions (accessed on 10 January 2024).
- The World Bank The World by Income and Region 2023. Available online: https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html (accessed on 10 January 2024).
- Haroon, M.Z.; Zeb, Z.; Javed, Z.; Awan, Z.; Aftab, Z.; Talat, W. Internet Addiction in Medical Students. J. Ayub Med. Coll. Abbottabad JAMC 2018, 30, S659–S663. [Google Scholar]
- Taha, M.H.; Shehzad, K.; Alamro, A.S.; Wadi, M. Internet Use and Addiction Among Medical Students in Qassim University, Saudi Arabia. Sultan Qaboos Univ. Med. J. SQUMJ 2019, 19, e142–e147. [Google Scholar] [CrossRef] [PubMed]
- Mboya, I.B.; Leyaro, B.J.; Kongo, A.; Mkombe, C.; Kyando, E.; George, J. Internet Addiction and Associated Factors among Medical and Allied Health Sciences Students in Northern Tanzania: A Cross-Sectional Study. BMC Psychol. 2020, 8, 73. [Google Scholar] [CrossRef] [PubMed]
- Khazaie, H.; Lebni, J.Y.; Abbas, J.; Mahaki, B.; Chaboksavar, F.; Kianipour, N.; Toghroli, R.; Ziapour, A. Internet Addiction Status and Related Factors among Medical Students: A Cross-Sectional Study in Western Iran. Community Health Equity Res. Policy 2023, 43, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Dhamnetiya, D.; Singh, S.; Jha, R.P. Correlates of Problematic Internet Use among Undergraduate Medical Students of Delhi. BMC Psychiatry 2021, 21, 1–8. [Google Scholar] [CrossRef]
- Young, K.S. Clinical Assessment of Internet-Addicted Clients. In Internet Addiction; Young, K.S., De Abreu, C.N., Eds.; Wiley: Hoboken, NJ, USA, 2007; pp. 19–34. ISBN 978-0-470-55116-5. [Google Scholar]
- Tao, R.; Huang, X.; Wang, J.; Zhang, H.; Zhang, Y.; Li, M. Proposed Diagnostic Criteria for Internet Addiction. Addiction 2010, 105, 556–564. [Google Scholar] [CrossRef]
- Von Hippel, P.T. The Heterogeneity Statistic I2 Can Be Biased in Small Meta-Analyses. BMC Med. Res. Methodol. 2015, 15, 35. [Google Scholar] [CrossRef]
- Nearly One in Two Indians Have Poor Quality of Life: Danone India-CII Survey 2021. Available online: https://www.thehindubusinessline.com/news/national/nearly-one-in-two-indians-have-poor-quality-of-life-danone-india-cii-survey/article35485858.ece (accessed on 10 January 2024).
- Rani, S.; Sinha, N.; Kumar, R. Prevalence of Internet Addiction and Its Relationship with Insomnia, Depression, Anxiety, and Stress among Medical Students of a Tertiary Care Medical Institute of Eastern India. Ind. Psychiatry J. 2024, 33, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Gjoneska, B.; Potenza, M.N.; Jones, J.; Sales, C.M.; Hranov, G.; Demetrovics, Z. Problematic Use of the Internet in Low- and Middle-Income Countries before and during the COVID-19 Pandemic: A Scoping Review. Curr. Opin. Behav. Sci. 2022, 48, 101208. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, K.; Treder, M.S.; Chamberlain, S.R.; Kiraly, F.; Redden, S.A.; Stein, D.J.; Lochner, C.; Grant, J.E. Problematic Internet Use as an Age-Related Multifaceted Problem: Evidence from a Two-Site Survey. Addict. Behav. 2018, 81, 157–166. [Google Scholar] [CrossRef]
- Devine, D.; Ogletree, A.M.; Shah, P.; Katz, B. Internet Addiction, Cognitive, and Dispositional Factors among US Adults. Comput. Hum. Behav. Rep. 2022, 6, 100180. [Google Scholar] [CrossRef]
- Kolaib, A.A.; Alhazmi, A.H.; Kulaib, M.A. Prevalence of Internet Addiction and Its Associated Factors among Medical Students at Taiba University, Saudi Arabia. J. Fam. Med. Prim. Care 2020, 9, 4797–4800. [Google Scholar] [CrossRef] [PubMed]
- Shan, X.; Ou, Y.; Ding, Y.; Yan, H.; Chen, J.; Zhao, J.; Guo, W. Associations Between Internet Addiction and Gender, Anxiety, Coping Styles and Acceptance in University Freshmen in South China. Front. Psychiatry 2021, 12, 558080. [Google Scholar] [CrossRef]
- Meng, S.-Q.; Cheng, J.-L.; Li, Y.-Y.; Yang, X.-Q.; Zheng, J.-W.; Chang, X.-W.; Shi, Y.; Chen, Y.; Lu, L.; Sun, Y.; et al. Global Prevalence of Digital Addiction in General Population: A Systematic Review and Meta-Analysis. Clin. Psychol. Rev. 2022, 92, 102128. [Google Scholar] [CrossRef]
- Mirza, A.A.; Baig, M.; Beyari, G.M.; Halawani, M.A.; Mirza, A.A. Depression and Anxiety among Medical Students: A Brief Overview. Adv. Med. Educ. Pract. 2021, 12, 393–398. [Google Scholar] [CrossRef]
- McNicol, M.L.; Thorsteinsson, E.B. Internet Addiction, Psychological Distress, and Coping Responses Among Adolescents and Adults. Cyberpsychology Behav. Soc. Netw. 2017, 20, 296–304. [Google Scholar] [CrossRef]
- Brand, M.; Laier, C.; Young, K.S. Internet Addiction: Coping Styles, Expectancies, and Treatment Implications. Front. Psychol. 2014, 5, 1256. [Google Scholar] [CrossRef]
- Zewde, E.A.; Tolossa, T.; Tiruneh, S.A.; Azanaw, M.M.; Yitbarek, G.Y.; Admasu, F.T.; Ayehu, G.W.; Amare, T.J.; Abebe, E.C.; Muche, Z.T.; et al. Internet Addiction and Its Associated Factors Among African High School and University Students: Systematic Review and Meta-Analysis. Front. Psychol. 2022, 13, 847274. [Google Scholar] [CrossRef] [PubMed]
- Endomba, F.T.; Demina, A.; Meille, V.; Ndoadoumgue, A.L.; Danwang, C.; Petit, B.; Trojak, B. Prevalence of Internet Addiction in Africa: A Systematic Review and Meta-Analysis. J. Behav. Addict. 2022, 11, 739–753. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rucker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for Examining and Interpreting Funnel Plot Asymmetry in Meta-Analyses of Randomised Controlled Trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis. John Wiley & Sons: Chichester, UK, 2009; ISBN 978-0-470-05724-7. [Google Scholar]
- Dobrescu, A.; Nussbaumer-Streit, B.; Klerings, I.; Wagner, G.; Persad, E.; Sommer, I.; Herkner, H.; Gartlehner, G. Restricting Evidence Syntheses of Interventions to English-Language Publications Is a Viable Methodological Shortcut for Most Medical Topics: A Systematic Review. J. Clin. Epidemiol. 2021, 137, 209–217. [Google Scholar] [CrossRef]
- Harvey, L.A.; Dijkers, M.P. Should Trials That Are Highly Vulnerable to Bias Be Excluded from Systematic Reviews? Spinal Cord 2019, 57, 715–716. [Google Scholar] [CrossRef] [PubMed]
- Adams, R.J.; Smart, P.; Huff, A.S. Shades of Grey: Guidelines for Working with the Grey Literature in Systematic Reviews for Management and Organizational Studies. Int. J. Manag. Rev. 2017, 19, 432–454. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Year of Publication | Country | Region | Country Classification by Income Level | Prevalence of IA | Sample Size | Mean Age | Data Collection Tool | Proportion of Males |
|---|---|---|---|---|---|---|---|---|---|
| Chaudhari et al. (2015) [23] | 2015 | India | Southeast Asian | Lower Middle Income | 0.589 | 282 | 19.9 | Young’s IA Test | 0.432 |
| Capetillo-Ventura and Juárez-Treviño (2015) [7] | 2015 | Mexico | Americas | Upper Middle Income | 0.082 | 522 | 21.2 | Young’s IA Test | 0.538 |
| Mohammadbeigi et al. (2016) [32] | 2016 | Iran | Eastern Mediterranean | Lower Middle Income | 0.287 | 254 | 21.7 | Young’s IA Test | 0.160 |
| Shaheen and Farahat (2016) [20] | 2016 | Egypt | Eastern Mediterranean | Lower Middle Income | 0.457 | 396 | 19.7 | Young’s IA Test | 0.581 |
| Ali et al. (2017) [22] | 2017 | Egypt | Eastern Mediterranean | Lower Middle Income | 0.476 | 582 | N/A | Young’s IA Test | 0.349 |
| Haroon et al. (2018) [46] | 2018 | Pakistan | Eastern Mediterranean | Lower Middle Income | 0.079 | 140 | N/A | Tao IA Diagnostic Criteria | 0.485 |
| Taha et al. (2019) [47] | 2019 | Saudi Arabia | Eastern Mediterranean | High Income | 0.124 | 209 | N/A | Young’s IA Test | 0.578 |
| Javaeed et al. (2019) [19] | 2019 | Pakistan | Eastern Mediterranean | Lower Middle Income | 0.524 | 210 | 21.8 | Young’s IA Test | 0.357 |
| Mboya et al. (2020) [48] | 2020 | Tanzania | African | Lower Middle Income | 0.310 | 500 | 23.8 | Young’s IA Test | 0.584 |
| Khazaie et al. (2021) [49] | 2021 | Iran | Eastern Mediterranean | Lower Middle Income | 0.250 | 420 | 22.8 | Young’s IA Test | 0.466 |
| Dhamnetiya et al. (2021) [50] | 2021 | India | Southeast Asian | Lower Middle Income | 0.413 | 201 | N/A | Young’s IA Test | 0.656 |
| Ibrahim et al. (2022) [18] | 2022 | Egypt | Eastern Mediterranean | Lower Middle Income | 0.093 | 321 | 21.9 | Young’s IA Test | 0.455 |
| Chauhan et al. (2022) [21] | 2022 | India | Southeast Asian | Lower Middle Income | 0.520 | 750 | 20.3 | Young’s IA Test | 0.624 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salpynov, Z.; Kosherova, Z.; Sarría-Santamera, A.; Nurkatov, Y.; Gusmanov, A.; Semenova, Y. The Worldwide Prevalence of Internet Addiction among Medical Students: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2024, 21, 1146. https://doi.org/10.3390/ijerph21091146
Salpynov Z, Kosherova Z, Sarría-Santamera A, Nurkatov Y, Gusmanov A, Semenova Y. The Worldwide Prevalence of Internet Addiction among Medical Students: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2024; 21(9):1146. https://doi.org/10.3390/ijerph21091146
Chicago/Turabian StyleSalpynov, Zhandos, Zhanar Kosherova, Antonio Sarría-Santamera, Yerbol Nurkatov, Arnur Gusmanov, and Yuliya Semenova. 2024. "The Worldwide Prevalence of Internet Addiction among Medical Students: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 21, no. 9: 1146. https://doi.org/10.3390/ijerph21091146
APA StyleSalpynov, Z., Kosherova, Z., Sarría-Santamera, A., Nurkatov, Y., Gusmanov, A., & Semenova, Y. (2024). The Worldwide Prevalence of Internet Addiction among Medical Students: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 21(9), 1146. https://doi.org/10.3390/ijerph21091146