
Radiation-Induced Childhood Thyroid Cancer after the Fukushima Daiichi Nuclear Power Plant Accident
Abstract
:1. Introduction
2. Materials and Methods
3. Results and Discussion
3.1. Estimation of the Incidence Rate at the Time of Fukushima NPP Accident
3.2. Estimation of the Annual Incidence Rate after the Accident in BS and 4 Rounds of FSS
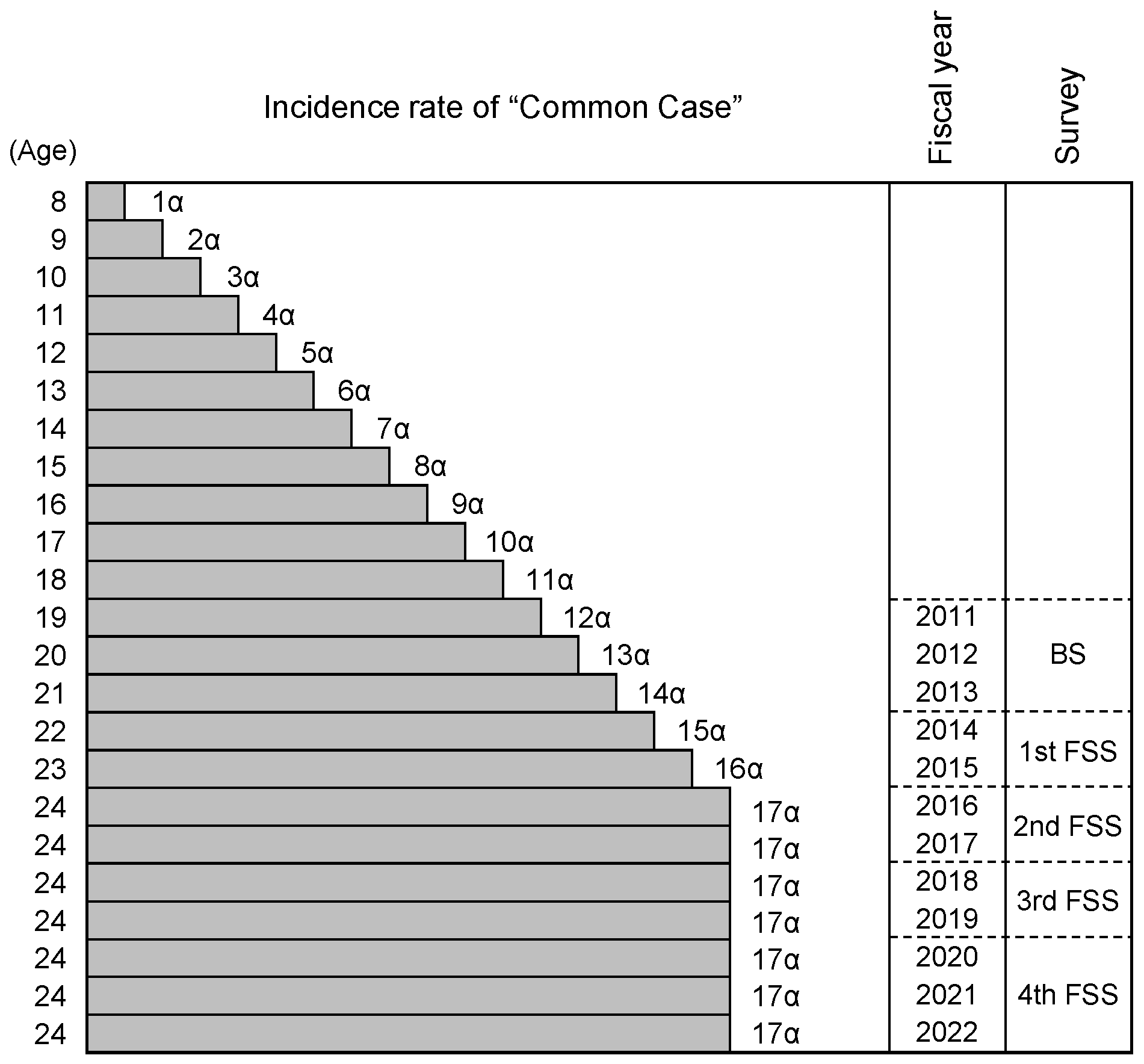
3.3. Annual Incidence Rate of “Common Case” before and after the Accident
3.4. Transition of the Annual Incidence Rate of Thyroid Cancer during Surveys after the Fukushima Daiichi NPP Accident
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| NPP | Nuclear Power Plant |
| BS | Basic Survey |
| FSS | Full-Scale Survey |
| 95% CI | 95% Confidence interval |
References
- Kazakov, V.S.; Demidchik, E.P.; Astakhova, L.N. Thyroid cancer after Chernobyl. Nature 1992, 359, 21. [Google Scholar] [CrossRef] [PubMed]
- Shibata, Y.; Yamashita, S.; Masyakin, V.B.; Panasyuk, G.D.; Nagataki, S. 15 years after Chernobyl: New evidence of thyroid cancer. Lancet 2001, 358, 1965–1966. [Google Scholar] [CrossRef]
- Cardis, E.; Hatch, M. The Chernobyl accident—An epidemiological perspective. Clin. Oncol. 2011, 23, 251–260. [Google Scholar] [CrossRef]
- Yasumura, S.; Hosoya, M.; Yamashita, S.; Kamiya, K.; Abe, M.; Akashi, M.; Kodama, K.; Ozasa, K.; Fukushima Health Management Survey Group. Study protocol for the Fukushima health management survey. J. Epidemiol. 2012, 22, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S. Childhood and adolescent thyroid cancer in Fukushima after the Fukushima Daiichi Nuclear Power Plant accident: 5 years on. Clin. Oncol. 2016, 28, 263–271. [Google Scholar] [CrossRef]
- The 23rd Prefectural Oversight Committee Meeting for Fukushima Health Management Survey. Report of First-Round Examination (Basic Survey). 2015. Available online: https://www.pref.fukushima.lg.jp/uploaded/attachment/461398.pdf (accessed on 6 June 2016). (In Japanese).
- Matsuda, A.; Matsuda, T.; Shibata, A.; Katanoda, K.; Sobue, T.; Nishimoto, H.; The Japan Cancer Surveillance Research Group. Cancer incidence and incidence rates in Japan in 2007: A study of 21 population-based cancer registries for the Monitoring of Cancer Incidence in Japan (MCIJ) project. Jpn. J. Clin. Oncol. 2013, 43, 328–336. [Google Scholar] [CrossRef]
- Tsuda, T.; Tokinobu, A.; Yamamoto, E.; Suzuki, E. Thyroid cancer detection by ultrasound among residents ages 18 years and younger in Fukushima, Japan: 2011 to 2014. Epidemiology 2016, 27, 316–322. [Google Scholar] [CrossRef]
- Tronko, M.D.; Saenko, V.A.; Shpak, V.M.; Bogdanova, T.I.; Suzuki, S.; Yamashita, S. Age distribution of childhood thyroid cancer patients in Ukraine after Chernobyl and in Fukushima after the TEPCO-Fukushima Daiichi NPP accident. Thyroid 2014, 24, 1547–1548. [Google Scholar] [CrossRef] [PubMed]
- The 28th Prefectural Oversight Committee Meeting for Fukushima Health Management Survey. Report of Second-Round Thyroid Ultrasound Examinations (First Full-Scale Thyroid Screening Program). 2017. Available online: https://www.pref.fukushima.lg.jp/uploaded/attachment/238768.pdf (accessed on 23 October 2017). (In Japanese).
- The 39th Prefectural Oversight Committee Meeting for Fukushima Health Management Survey. Report of Third-Round Examination (2nd Full Scale Survey). 2020. Available online: https://www.pref.fukushima.lg.jp/uploaded/attachment/401325.pdf (accessed on 31 August 2020). (In Japanese).
- The 45th Prefectural Oversight Committee Meeting for Fukushima Health Management Survey. Report of 3rd Full Scale Survey. 2021. Available online: https://www.pref.fukushima.lg.jp/uploaded/attachment/529187.pdf (accessed on 1 October 2022). (In Japanese).
- The 52nd Prefectural Oversight Committee Meeting for Fukushima Health Management Survey. Report of 4th Full Scale Survey. 2024. Available online: https://www.pref.fukushima.lg.jp/uploaded/attachment/644647.pdf (accessed on 2 August 2024). (In Japanese).
- Vesely, M.D.; Kershaw, M.H.; Schreiber, R.D.; Smyth, M.J. Natural innate and adaptive immunity to cancer. Annu. Rev. Immunol. 2011, 29, 235–271. [Google Scholar] [CrossRef]
- Schreiber, R.D.; Old, L.J.; Smyth, M.J. Cancer immunoediting: Integrating immunity’s roles in cancer suppression and promotion. Science 2011, 331, 1565–1570. [Google Scholar] [CrossRef]
- Chen, D.S.; Mellman, I. Oncology meets immunology: The cancer-immunity cycle. Immunity 2013, 39, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ochiai, K.; Hayama, S.; Nakiri, S.; Nakanishi, S.; Ishii, N.; Uno, T.; Kato, T.; Konno, F.; Kawamoto, Y.; Tsuchida, S.; et al. Low blood cell counts in wild Japanese monkeys after the Fukushima Daiichi nuclear disaster. Sci. Rep. 2014, 4, 5793. [Google Scholar] [CrossRef]
- Urushihara, Y.; Suzuki, T.; Shimizu, Y.; Ohtaki, M.; Kuwahara, Y.; Suzuki, M.; Uno, T.; Fujita, S.; Saito, A.; Yamashiro, H.; et al. Haematological analysis of Japanese macaques (Macaca fuscata) in the area affected by the Fukushima Daiichi Nuclear Power Plant accident. Sci. Rep. 2018, 8, 16748. [Google Scholar] [CrossRef] [PubMed]
- Stepanova, E.; Karmaus, W.; Naboka, M.; Vdovenko, V.; Mousseau, T.; Shestopalov, V.M.; Vena, J.; Svendsen, E.; Underhill, D.; Pastides, H. Exposure from the Chernobyl accident had adverse effects on erythrocytes, leukocytes, and, platelets in children in the Narodichesky region, Ukraine: A 6-year follow-up study. Environ. Health 2008, 7, 21. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, H.; Hayashi, K.; Scherb, H. Association between the detection rate of thyroid cancer and the external radiation dose-rate after the nuclear power plant accidents in Fukushima, Japan. Medicine 2019, 98, e17165. [Google Scholar] [CrossRef]
- Kato, T.; Yamada, K.; Hongyo, T. Area Dose-Response and Radiation Origin of Childhood Thyroid Cancer in Fukushima Based on Thyroid Dose in UNSCEAR 2020/2021: High (131)I Exposure Comparable to Chernobyl. Cancers 2023, 15, 4583. [Google Scholar] [CrossRef]
- Toki, H.; Wada, T.; Manabe, Y.; Hirota, S.; Higuchi, T.; Tanihata, I.; Satoh, K.; Bando, M. Relationship between environmental radiation and radioactivity and childhood thyroid cancer found in Fukushima health management survey. Sci. Rep. 2020, 10, 4074. [Google Scholar] [CrossRef] [PubMed]
- Ohira, T.; Ohtsuru, A.; Midorikawa, S.; Takahashi, H.; Yasumura, S.; Suzuki, S.; Matsuzuka, T.; Shimura, H.; Ishikawa, T.; Sakai, A.; et al. External radiation dose, obesity, and risk of childhood thyroid cancer after the Fukushima Daiichi Nuclear Power Plant accident: The Fukushima health management survey. Epidemiology 2019, 30, 853–860. [Google Scholar] [CrossRef]
- Ohira, T.; Shimura, H.; Hayashi, F.; Nagao, M.; Yasumura, S.; Takahashi, H.; Suzuki, S.; Matsuzuka, T.; Suzuki, S.; Iwadate, M.; et al. Absorbed radiation doses in the thyroid as estimated by UNSCEAR and subsequent risk of childhood thyroid cancer following the Great East Japan Earthquake. J. Radiat. Res. 2020, 61, 243–248. [Google Scholar] [CrossRef]
- Lubin, J.H.; Adams, M.J.; Shore, R.; Holmberg, E.; Schneider, A.B.; Hawkins, M.M.; Robison, L.L.; Inskip, P.D.; Lundell, M.; Johansson, R.; et al. Thyroid cancer following childhood low-dose radiation exposure: A pooled analysis of nine cohorts. J. Clin. Endocrinol. Metab. 2017, 102, 2575–2583. [Google Scholar] [CrossRef]
- Yamamoto, H.; Hayashi, K.; Scherb, H. A comment on: ‘Absorbed radiation doses in the thyroid as estimated by UNSCEAR and subsequent risk of childhood thyroid cancer following the Great East Japan’. J. Radiat. Res. 2021, 62, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Ohira, T.; Shimura, H.; Yasumura, S.; Yokoya, S.; Ohto, H.; Kamiya, K. Response to the Letter to the Editor: ‘Absorbed radiation doses in the thyroid as estimated by UNSCEAR and subsequent risk of childhood thyroid cancer following the Great East Japan Earthquake’, by Ohira et al. J. Radiat. Res. 2021, 62, 425–426. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, S.; Shibata, Y. Chernobyl: A Decade: Proceedings of the fifth Chernobyl Sasakawa Medical Cooperation Symposium, Kiev, Ukraine, 14–15 October 1996; Elsevier: Amsterdam, The Netherlands, 1997. [Google Scholar]
- Iwadate, M.; Mitsutake, N.; Matsuse, M.; Fukushima, T.; Suzuki, S.; Matsumoto, Y.; Ookouchi, C.; Mizunuma, H.; Nakamura, I.; Nakano, K.; et al. The Clinicopathological Results of Thyroid Cancer with BRAFV600E Mutation in the Young Population of Fukushima. J. Clin. Endocrinol. Metab. 2020, 105, e4328–e4336. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Survey | Area | Inspection Period (Year) | No. of Objects | No. of Examinees * | No. of Patients |
|---|---|---|---|---|---|
| BS | A | 1 | 35,014 | 30,605 (87.4%) | 14 |
| B | 2 | 114,825 | 98,808 (86.1%) | 56 | |
| C | 3 | 78,616 | 59,714 (76.0%) | 33 | |
| D | 3 | 36,772 | 23,552 (64.0%) | 12 | |
| Total | 265,227 | 212,679 (80.2%) | 115 | ||
| 1st FSS | A | 3 | 37,025 | 25,873 (69.9%) | 17 |
| B | 2 | 125,731 | 93,583 (74.4%) | 35 | |
| C | 2 | 89,585 | 62,953 (70.3%) | 14 | |
| D | 2 | 42,224 | 26,271 (62.2%) | 5 | |
| Total | 294,565 | 208,680 (70.8%) | 71 | ||
| 2nd FSS | A | 2 | 35,154 | 214,25 (60.9%) | 6 |
| B | 2 | 120,103 | 78,546 (65.4%) | 7 | |
| C | 2 | 86,162 | 53,468 (62.1%) | 13 | |
| D | 2 | 39,315 | 23,100 (58.8%) | 5 | |
| Total | 280,734 | 176,539 (62.9%) | 31 | ||
| 3rd FSS | A | 2 | 33,382 | 19,108 (57.2%) | 2 |
| B | 2 | 115,663 | 72,346 (62.5%) | 20 | |
| C | 2 | 82,233 | 48,271 (58.7%) | 12 | |
| D | 2 | 37,131 | 21,099 (56.8%) | 5 | |
| Total | 268,409 | 160,824 (59.9%) | 39 | ||
| 4th FSS | A | 3 | 32,140 | 14,787 (46.0%) | 6 |
| B | 3 | 112,762 | 54,391 (48.2%) | 23 | |
| C | 3 | 74,592 | 31,990 (42.9%) | 14 | |
| D | 3 | 33,444 | 12,791 (38.2%) | 3 | |
| Total | 252,938 | 113,959 (45.1%) | 46 |
| Area | BS | 1st FSS | BS and 1st FSS | ||
|---|---|---|---|---|---|
| Elapsed Time (year) * | Incidence Rate ** | Elapsed Time (Year) * | Incidence Rate ** | Cumulative Sum | |
| A | 1 | 45.7 | 4 | 65.7 | 111.4 |
| B | 2 | 56.7 | 4 | 37.4 | 94.1 |
| C | 3 | 55.3 | 5 | 22.2 | 77.5 |
| D | 3 | 51.0 | 5 | 19.0 | 70.0 |
| Survey | Area | Incidence Rate * | Inspection Period (Year) | Annual Incidence Rate ** (95% CI ***) |
|---|---|---|---|---|
| BS | A | 45.7 − 21.9 = 23.8 | 1 | 23.8 (17.7, 29.9) |
| B | 56.7 − 21.9 = 34.8 | 2 | 17.4 (14.4, 20.5) | |
| C | 55.3 − 21.9 = 33.4 | 3 | 11.1 (7.0, 15.2) | |
| D | 51.0 − 21.9 = 29.1 | 3 | 9.7 (2.2, 17.3) | |
| 1st FSS | A | 65.7 | 3 | 21.9 (11.9, 31.7) |
| B | 37.4 | 2 | 18.7 (14.3, 23.1) | |
| C | 22.2 | 2 | 11.1 (6.6, 15.6) | |
| D | 19.0 | 2 | 9.5 (2.3, 16.7) | |
| 2nd FSS | A | 28.0 | 2 | 14.0 (5.7, 22.3) |
| B | 8.9 | 2 | 4.5 (2.2, 6.8) | |
| C | 24.3 | 2 | 12.2 (7.4, 17.0) | |
| D | 21.6 | 2 | 10.8 (3.6, 18.0) | |
| 3rd FSS | A | 10.5 | 2 | 5.2 (−1.5, 11.9) |
| B | 27.6 | 2 | 13.8 (8.6, 19.1) | |
| C | 24.9 | 2 | 12.4 (6.1, 18.8) | |
| D | 23.7 | 2 | 11.8 (2.2, 21.5) | |
| 4th FSS | A | 40.6 | 3 | 13.5 (2.0, 27.3) |
| B | 42.3 | 3 | 14.1 (6.9, 21.3) | |
| C | 43.8 | 3 | 14.6 (4.6, 24.6) | |
| D | 23.5 | 3 | 7.8 (−4.2, 19.8) |
| Survey | Area | Incidence Rate * | Inspection Period (Year) | Annual Incidence Rate ** (95% CI ***) |
|---|---|---|---|---|
| BS at the time of accident | all areas | 11α **** = 3.65 | - | 3.65 (2.47, 4.83) |
| BS after the accident | A | 12α = 3.98 | 1 | 3.96 (1.47, 6,45) |
| B | (12 + 13)α = 8.30 | 2 | 4.15 (2.66, 5.64) | |
| C | (12 + 13 + 14)α = 12.95 | 3 | 4.32 (1.75, 6.89) | |
| D | (12 + 13 + 14)α = 12.95 | 3 | 4.32 (−0.71, 9,35) | |
| 1st FSS | A | (13 + 14 + 15)α = 13.94 | 3 | 4.65 (0.10, 9.20) |
| B | (14 + 15)α = 9.63 | 2 | 4.82 (2,59, 7.05) | |
| C | (15 + 16)α = 10.29 | 2 | 5.15 (2.11, 8.19) | |
| D | (15 + 16)α = 10.29 | 2 | 5.15 (−0.18, 10.48) | |
| 2nd FSS | A | (16 + 17)α = 10.96 | 2 | 5.48 (−0.70, 11.66) |
| B | (16 + 17)α = 10.96 | 2 | 5.48 (2.44, 8.52) | |
| C | (17 + 17)α = 11.29 | 2 | 5.64 (1,72, 9.56) | |
| D | (17 + 17)α = 11.29 | 2 | 5.64 (−0.57, 11.85) | |
| 3rd FSS | A | (17 + 17)α = 11.29 | 2 | 5.64 (−1.32, 12.60) |
| B | (17 + 17)α = 11.29 | 2 | 5.64 (2.29, 8.99) | |
| C | (17 + 17)α = 11.29 | 2 | 5.64 (1.33, 9.95) | |
| D | (17 + 17)α = 11.29 | 2 | 5.64 (−1.00, 12.28) | |
| 4th FSS | A | (17 + 17 + 17)α = 16.93 | 3 | 5.64 (−3.25, 14.53) |
| B | (17 + 17 + 17)α = 16.93 | 3 | 5.64 (1.11, 10.17) | |
| C | (17 + 17 + 17)α = 16.93 | 3 | 5.64 (−0.57, 11.85) | |
| D | (17 + 17 + 17)α = 16.93 | 3 | 5.64 (−4.57, 15.85) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sokawa, Y. Radiation-Induced Childhood Thyroid Cancer after the Fukushima Daiichi Nuclear Power Plant Accident. Int. J. Environ. Res. Public Health 2024, 21, 1162. https://doi.org/10.3390/ijerph21091162
Sokawa Y. Radiation-Induced Childhood Thyroid Cancer after the Fukushima Daiichi Nuclear Power Plant Accident. International Journal of Environmental Research and Public Health. 2024; 21(9):1162. https://doi.org/10.3390/ijerph21091162
Chicago/Turabian StyleSokawa, Yoshihiro. 2024. "Radiation-Induced Childhood Thyroid Cancer after the Fukushima Daiichi Nuclear Power Plant Accident" International Journal of Environmental Research and Public Health 21, no. 9: 1162. https://doi.org/10.3390/ijerph21091162