Abstract
Cancer is an important health issue in Turkey because it ranks as the second cause of death in the country. Examination of the relationships between the distribution of cancer cases and geo-environmental factors is significant in determining the causes of cancer. In this study, GIS were used to provide data about the distribution of cancer types in Trabzon province, Turkey. To determine the cancer occurrence density, the cancer incidence rates were calculated according to local census data, then a cancer density map was produced, and correlations between cancer types and geographical factors were examined.
1. Introduction
Cancer is a major health issue and one of the most common diseases in the World, with more than 11 million cases being diagnosed every year [1]. The World Health Organization (WHO) estimated that of 58 million lives lost globally in 2005, 7.6 million died from cancer and 84 million people will die over the next 10 years if no action is taken. More than 70% of all cancer related deaths occur in countries where the population has a medium to low level standard of living and limited resources for the prevention, diagnosis, and treatment of cancer [2].
In Turkey, cancer has become the second major cause of death [3]. In 2005, approximately 52,000 people died from cancer in Turkey and 37,000 were under the age of 70 [4]. According to Cancer Research UK (2002) the average cancer incidence rates are 330.5 in North America, 266.7 in Western Europe and 195.9 in Eastern Europe. In the region where Turkey is located the average incidence rate is 130.2 per 100,000 population [5]. Cancer not only has a high level of mortality but also can result in serious disability and impacts on the productivity of the labour force. Treatment costs are high and have major implications for government expenditures on health services.
The Cancer Control Program (CCP) initiated by the WHO aims to reduce the incidence of cancer and cancer related deaths, and to improve the quality of life of cancer patients [6]. Within the context of this program, descriptive statistics presenting the distribution of cancer cases, existing density of cancer cases, and the most common cancer types in the country should be determined [7]. In order to enforce cancer control strategies effectively in Turkey, firstly, statistical data about cancer cases should be collected. Then, cancer maps need to be created to obtain a realistic analysis of the spatial distribution of the cases. These maps facilitate the determination of the regions with greatest density of cancer cases and the spatial examination of the environmental factors possibly causing cancer in these regions [8]. In this context, Geographic Information Systems (GIS) can be used to map and analyze the geographical distribution of populations at risk, to determine environmental risk factors, to explore associations between risk factors and health outcomes, and to address health issues [9,10].
This research aimed to examine the relationship between the distribution of cancer cases and environmental factors in Trabzon province, Turkey. Firstly, various data collected with GIS & Remote Sensing (RS) techniques are combined in a spatial database. Then, the geo-statistical maps displaying the cancer density within administrative units were produced with regard to the cancer cases of Trabzon province for the year 2004. Thus, the distribution of the cancer cases was investigated in conjunction with population and environmental factors. The distribution map of cancer cases based on land cover was produced to examine whether there is any statistical relationship between land cover and cancer types.
2. Method
2.1. Background: Cancer Registry Process in Turkey
Disease Centers collect information about notable diseases In Turkey and maintain disease registries on databases [11]. Cancer case data is collected by local health centers using a recording system protected by laws governing privacy and confidentiality. This data includes the residential address of the cancer patients. In this way, with analytical studies the trends of cancer incidence and mortality in different populations can spatially be determined in order to examine the relationships between incidence, mortality, and environmental risk factors [12].
By supporting an epidemiological study cancer registries play an important role in investigating the relationship between the causes and frequency trends of cancer. The main characteristics of cancer registries are to monitor trends in cancer incidence, prevalence, and mortality over time and between different areas and social groups. These depend on the implementation of the Cancer Control Program and the available cancer registries [13]. In order to put a cancer control program into practice, reliable population-based information on cancer incidence, prevalence, and mortality rates is required.
2.2. Geographical Information Systems and Cancer Maps
The earliest disease maps were produced in Germany over two hundred years ago. Then in 1855, John Snow’s dot maps of a cholera epidemic in UK were the first published and became the most famous example of spatial epidemiology [14]. The first cancer maps in colour were produced in 1875 [15]. In the 1970s, the use of GIS increased among epidemiologists and public health researchers in conjunction with the development of new technologies [16]. The recent advances and increased awareness of GIS and mapping techniques have created new opportunities for public health administrators to enhance their planning, analysis, and monitoring capabilities. Thus, they are able to assess the relationship between public health and the geographic characteristics of residential area [17–19]. Specifically, in terms of epidemiologic studies for cancer, GIS supports the exploration of the relationship between environmental risk factors and disease. GIS is widely utilized in order to produce cancer maps and to implement statistical and spatial analysis for cancer globally [20–28]. There are a large number of statistical or geo-statistical methods for cancer investigation in epidemiology [29–31].
2.3. The Registration Process of Cancer Cases in Turkey
In Turkey, cancer registries have been collected since 1982, the registration process being conducted by the Cancer Control Department of the Turkish Ministry of Health. In the past, cancer cases were registered in a disorganized manner without complying with any national or international standard. Therefore, to determine the overall profile of the incidence of cancer in Turkey the “Turkish Cancer Registry and Incidence” project was initiated in 1992 to monitor cancer cases countrywide. Cancer Registry Centers (CRCs) were founded in 11 provinces and the cancer cases began to be recorded according to the International Classification of Diseases (ICD-9) coding system. This standard is used to develop a reliable database for cancer cases in these centers [32].
Since 2004, the Trabzon CRC, a subdivision of Provincial Health Directorate of Trabzon, has been collecting active cancer data from all health institutions and hospitals in Trabzon province in accordance with ICD-9 standard. This center collaborates with the Cancer Division of Ministry of Health and coordinates the activities of all the allied units. The personnel of this center enter the data into computers, control the quality of all the data, prevent duplications, evaluate the data, and prepare reports explaining the cancer incidence rates.
2.4. The Study Area
Trabzon, the chosen study area, is situated between 38°30′–40°30′ east longitude and 40°30′–41°30′ north latitude, with the Black Sea to the north, Gumushane and Bayburt on the southern side, Rize on the eastern side, and Giresun on the western side. Trabzon province has a socio-economic development ranking of 38th out of the 81 provinces of Turkey [33]. As can be seen on the map (Figure 1), Trabzon province comprises 17 county towns and 537 villages and covers an area of 4,664 km2. According to 2008 census conducted by the Turkey Statistics Institute the population of Trabzon was 748,982, with a density of 161 people per square kilometre [34].

Figure 1.
Study Area.
2.5. Data Collection and Organization
Health data limitation is a problem that has faced GIS users in Turkey. To collect new data related to disease facts and to convert paper maps and data into digital format continues to be a problem. In many cases there are issues of confidentiality, national security, etc. which have prevented its use by health-related departments. One data problem that is particularly difficult to deal with cases address. While there may be some data available from the census, it is usually too old or not done frequently enough to be useful for epidemiologic research. The primary option is for health officers to conduct special surveys to determine the cases living locations. While this can result in accurate data, it cannot be used historically and takes time to collect. One way of approaching data problems is to set up a pilot program. A pilot program would have several benefits including: showing decision makers what is possible; working out problems on a small scale before launching an entire program nationwide; collecting data or converting if from analog format.
The data about cancer cases must include the patient’s age, sex, address, cancer type with topology, and diagnosis date. To investigate the locations of cancer cases in this study, Administrative Units and Roads spatial data sets are required for address geocoding. The Administrative Unit data sets include administrative boundaries as areas and allocation centers as points for districts and villages at the lowest administration level. To examine the relationship between geography and cancer cases, different types of spatial data sets should be produced and classified accordingly. Table 1 shows the database design and required data for this study.

Table 1.
Required spatial data themes.
The data related to cancer cases was obtained from the Trabzon Cancer Registry Center, which has been recording cancer cases diagnosed in Health Institutions of Trabzon since 2004. From that time the centre has recorded 1,216 cancer cases for the province. Cancer case data that did not have sufficient address information, and therefore, could not be identified, was eliminated. In this way, 1,150 cancer cases were examined with the data including the patient’s sex, age, address, and disease name/type, as shown in Table 1.
ArcGIS 9.x was used to combine the data and achieve spatial analysis. For all the spatial data sets, the datum is ITRF-96 (International Terrestrial Reference System) and the ellipsoid is GRS-80 (Geodetic Reference System-1980). The reference System is determined as ETRS89 Lambert Azimuthal Equal Area (ETRS-LAEA) because it has advantages for statistical analysis and presentation [35]. The Administration Unit Spatial Data Sets were collected from 1:25,000 and 1:100,000 scaled maps of the General Directorate of Rural Services, Trabzon Province Administration, and the sub institutions of Trabzon and was managed on a GIS environment. Population data for each Administrative Unit was collected from the Turkish Statistics Institute (TURKSTAT).
After matching the address related to each cancer case with the administrative unit data set, the location of cancer cases can be shown on the map that is produced. For each cancer case, an Administration Unit Code (IDBK) was determined and entered into the Cancer Registry dataset for geocoding at district/village level. This dataset was collected in dbase format as a spreadsheet. By using IDBK as a hierarchical unique value of each Administrative Unit, the number of cancer cases for each Administrative Unit was decided.
Elevation data sets were extracted from 1:25,000 scaled Digital Topography Maps and a Digital Elevation Model (DEM) was produced from the elevation data sets. Land Cover Spatial Data Sets were produced from LANDSAT 7 ETM+ (Enhance Tematic Mapper+) satellite images using RS supervised classification techniques. The spatial analysis function “Intersect” in ESRI ArcGIS was used to determine the relationship between cancer cases and topography and elevation.
2.6. Statistical Analysis
Incidence means the frequency with which a disease appears in a particular population or area. A cancer incidence rate is the number of new cancers of a specific site/type occurring in a specified population over a year, usually expressed as the number of cancers per 100,000 people at risk. The incidence rate for each administrative unit was calculated with Equation 1 below:
According to the WHO, the number of cancer cases is estimated to be between a minimum 150 and maximum 300 for a population of 100,000 in developing countries [36] therefore, administrative units with a cancer incidence rate of more than 300 are considered to have a high cancer density level.
The Pearson chi-square (χ2) statistics test the independency between the sub categories of two variables of R*C (Row*Column). The importance of χ2p is determined, to compare critical values of χ2α, df and the freedom degree is calculated using df = (R – 1)(C – 1) [31]. SPSS ® version 10.0 was used for this statistical analysis.
3. Results and Discussion
3.1. Mapping of the Distribution of Cancer Cases
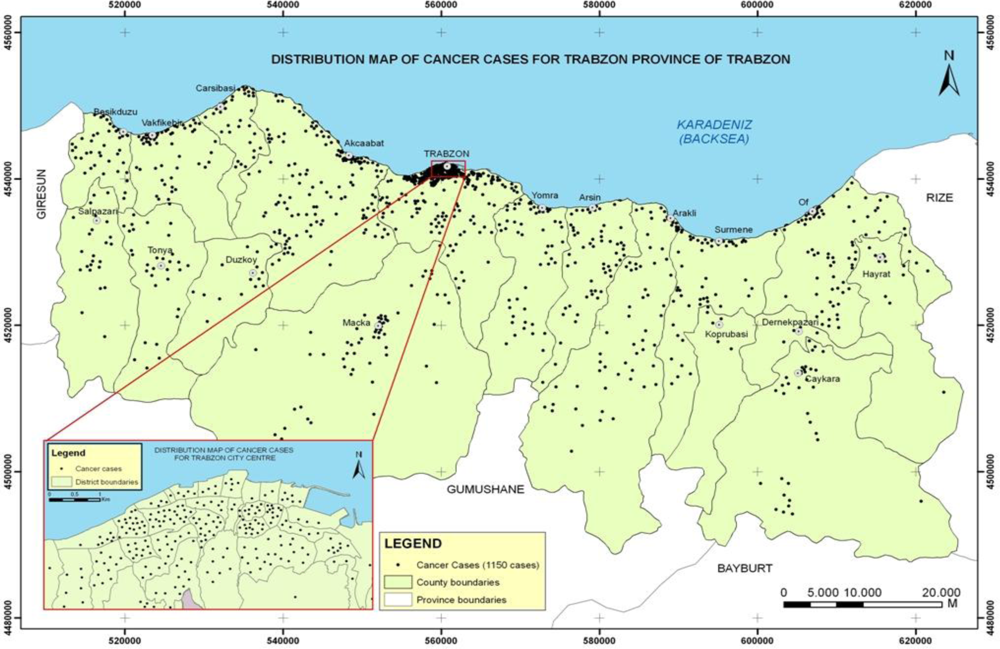
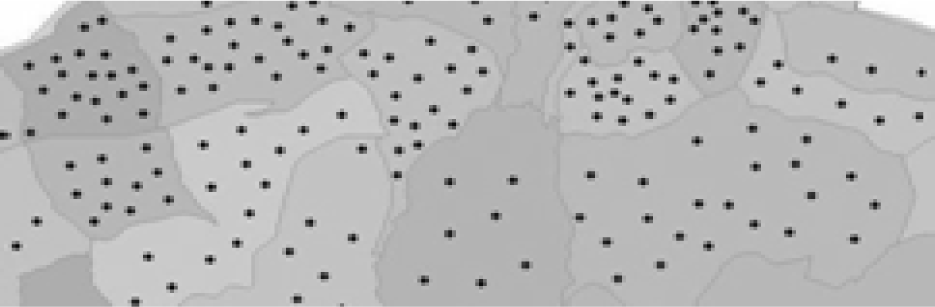
After determining the location of cancer cases spatially, the distribution of cancer cases was examined using the Administrative Unit Spatial Data Set. The cases were classified in five common cancer types for Trabzon City. At the district and village level, the Distribution Map of Cancer Cases shown in Figure 2 was produced to visually present the frequency of cancer cases and types.
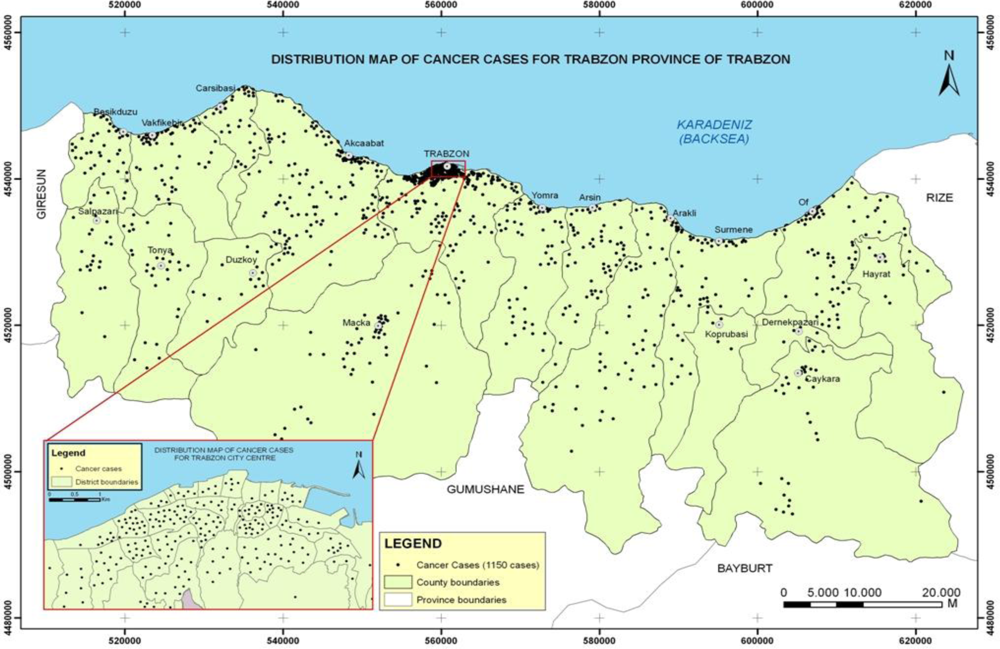
Figure 2.
Distribution map of cancer cases.
As seen on the map in Figure 2, more heavily populated administration units have more cancer cases, distributed in city and county centers, coastal residential areas, and across valleys. Investigating the 1,150 cancer cases, it was determined that the five common cancer types were lung (19.1%), skin (12.3%), breast (9.9%), stomach (9.5%), and bladder (6.8%), which is in keeping with the common cancers globally. Table 2 shows the percentage of different cancer types for men and women most notably showing that lung cancer is more prevalent in men and breast cancer more common in women.
Table 2.
The most common cancer types with respect to sex in Trabzon (out of population 2004).
3.2. The Cancer Incidence Map
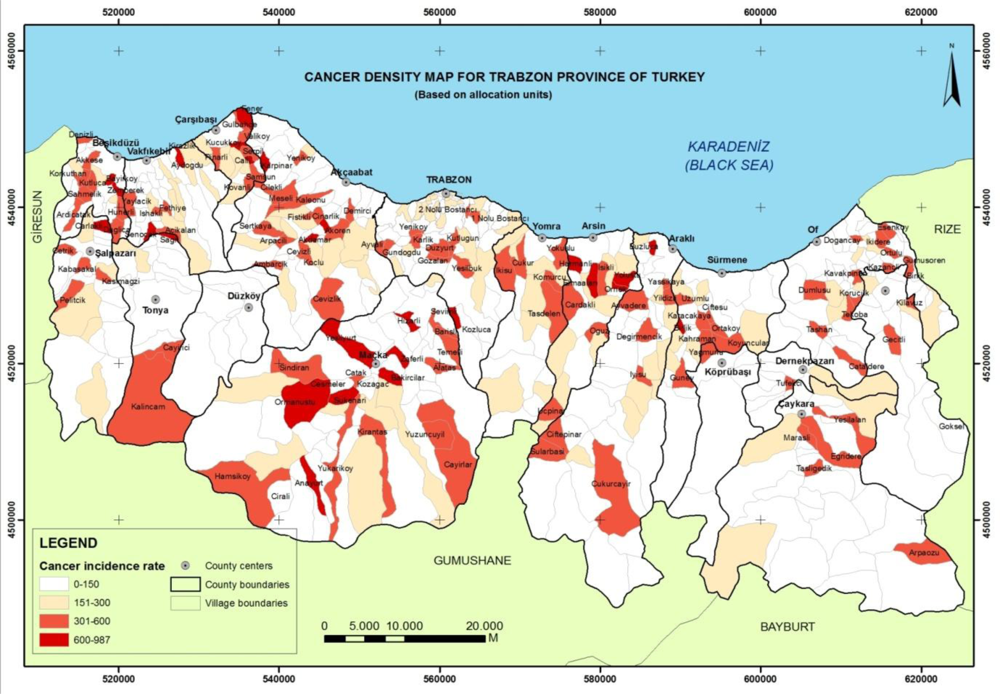
To analyze the distribution of cancer cases and cancer density on the map, the incidence rates of the administrative units were used as a comparison factor for the statistical research. After the number of cancer cases for each administrative unit was calculated, the incidence rate for each administration unit was determined using the population in the year 2004. The Cancer Density Map in Figure 3 was produced showing the incidence rates of the administrative units with classified groups at district and village level (see Table 3).
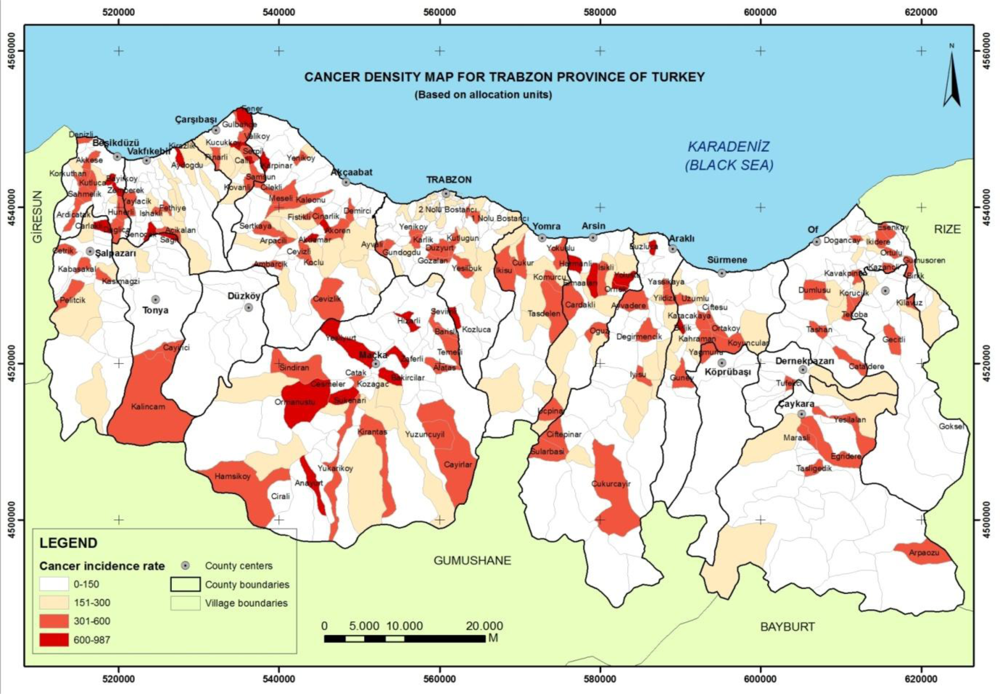
Figure 3.
Cancer incidence map of Trabzon province in Turkey.
Table 3.
The number of administrative units on groups of incidence rates.
Administrative units with incidence rates of more than 300 are regions at risk in terms of cancer density are shaded in dark red on the map shown in Figure 3. It was determined that 138 administrative units, comprising 22% of all the administrative units, have a high incidence rate of cancer. The calculated incidence rate of Trabzon province was determined to be 118, thus confirm that overall the province has a lower incidence of cancer than that estimated by WHO for developing countries.
3.3. Relationship between the Cancer Cases and Land Cover
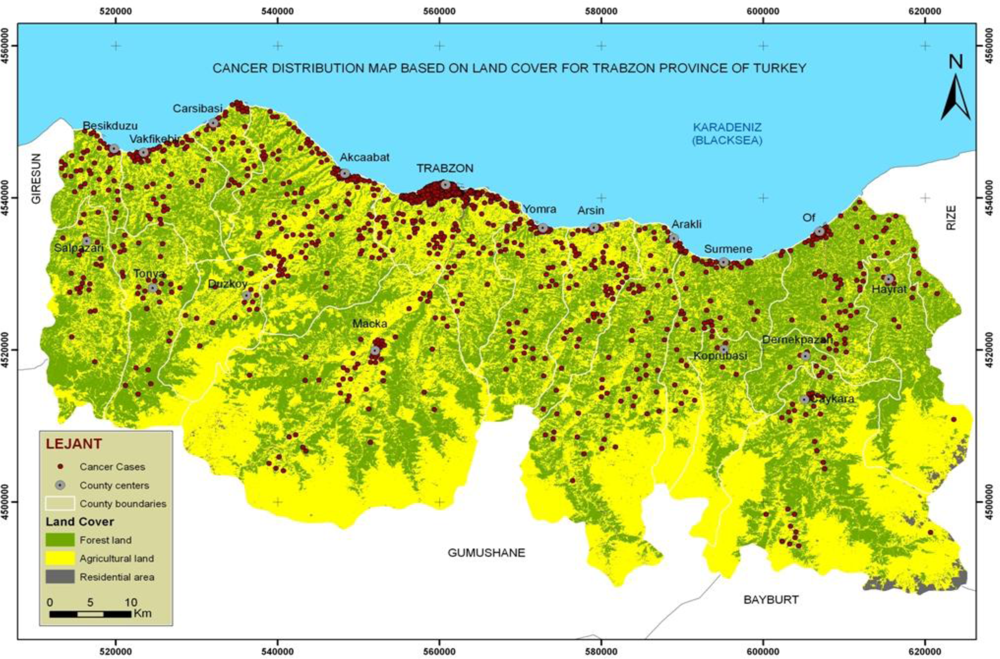
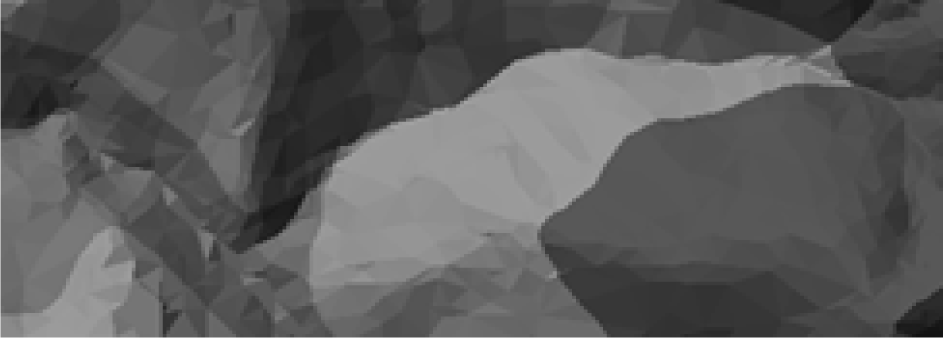
The distribution map of cancer cases based on land cover was produced to examine whether there is a relationship between land cover and cancer types. After producing the Trabzon Province Land Cover data sets like forest land, agriculture land and residential areas with supervised classification method as shown in Figure 4, the number of cancer cases in each land cover class was determined with the spatial analysis function “Intersect” as shown in Table 4.
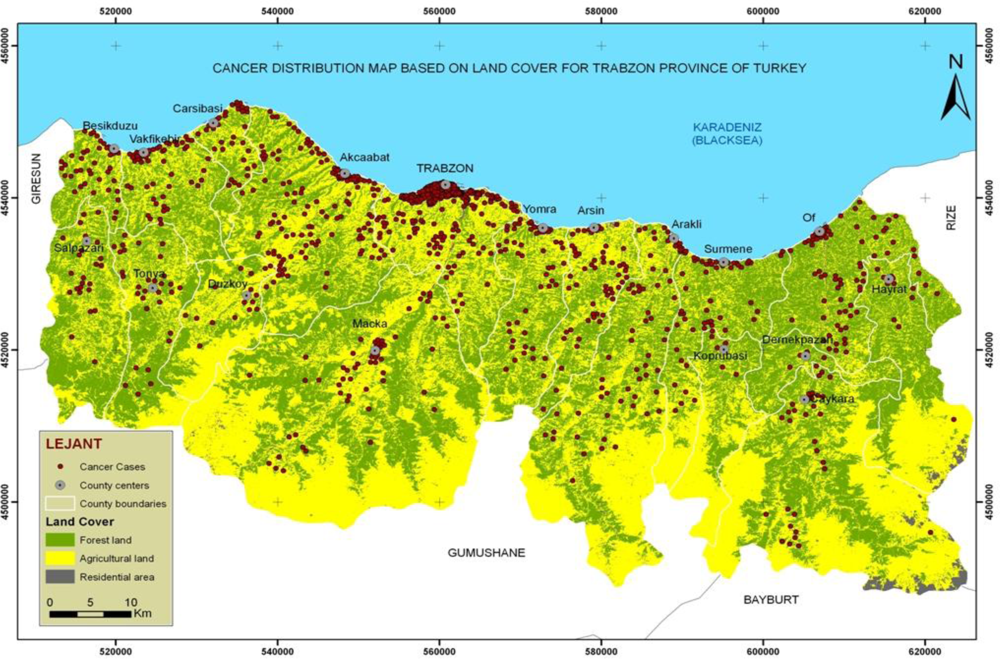
Figure 4.
The distribution map of cancer cases based on land cover.
Table 4.
The number of cancer cases within each land cover class.
Forty five cancer types and five land cover classes were determined in this study. To enable the statistical analysis, tea and hazelnut were combined with the Agriculture Land Cover Class. The Cancer Types were reduced to eight common cancer types taking related cancer types into consideration, as shown in Table 5. The number of cancer cases of each cancer type within each land cover class was calculated with a database query. To test whether there is a statistical relationship between land cover and cancer type, The Pearson chi square test was used and showed that there was a relationship between cancer types and land cover, χ2 = 24.391, df = 14, p = 0.041. Supposing the Ho (null) hypothesis to be true, count, the expected count, percentage, and adjusted residual were presented on the crosstabs of Table 5 for 1,150 cancer cases.
Table 5.
Crosstab presenting the relationship between land cover and cancer types.
On examining the percentage of cancer cases by land cover classes as shown on Table 5, 47.8% corresponded to agriculture, 33.8% to forestry, and 18.3% to residential areas. On examining the percentage of the types of cancer cases, 22.3% of lung/bronchus/larynx/throat, 12.3% of skin, 9.9% of breast, 13.8% stomach, 6.8% of bladder, 4.9% of prostate, 4.8% of thyroid, and 25.1% of other cancer cases overlapped with classified land cover types, thus, making the supposition that the Ho hypothesis is false, showing that there is relationship between cancer types and land cover. Breast cancer occurred more in residential areas than other cancer types. Skin and thyroid cancer occurred more in forestry areas than the other cancer types. In addition, skin cancer cases in forestry areas have frequency values of, count = 61 and expected count = 48. 43% of skin cancer cases were diagnosed in forestry areas and these account for 5.3% of all cancer cases.
3.4. Relationship between the Distribution of Cancer Cases and Elevation
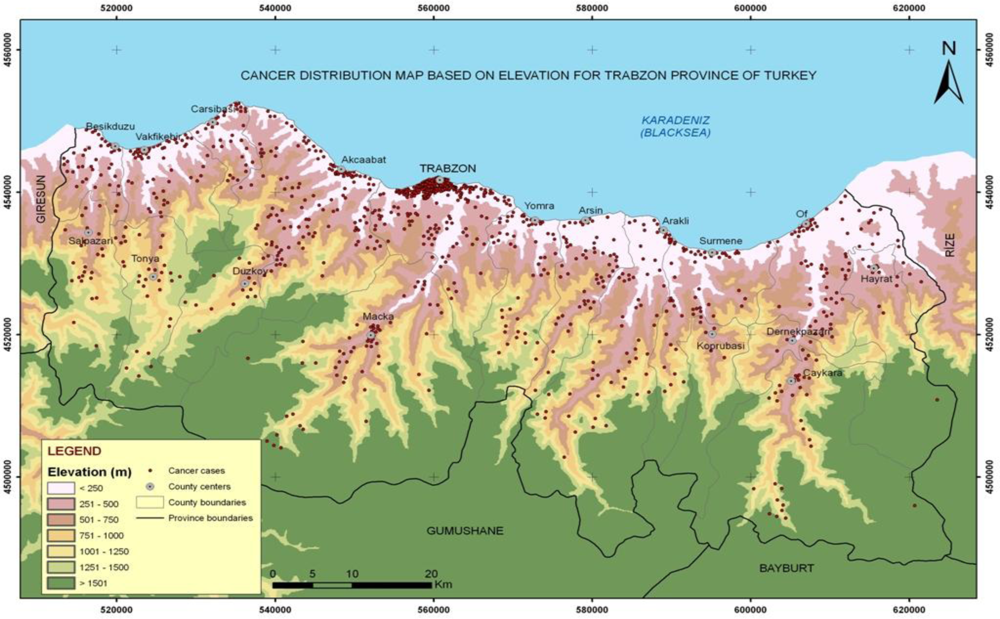
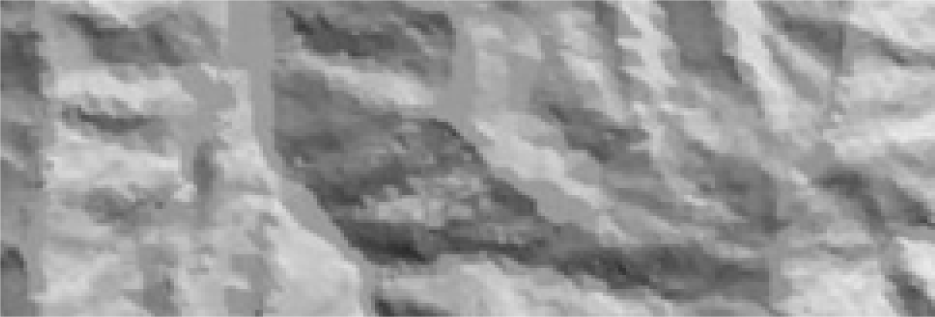
The distribution map of cancer cases based on elevation was produced to examine whether there is a relationship between elevation and cancer types. After producing a Digital Elevation Model (DEM) with elevation classes at 250 m intervals, as shown in Figure 5, the number of cancer cases of each cancer type in each elevation class was determined with the spatial analysis “Intersect” and database query as shown in Table 6.
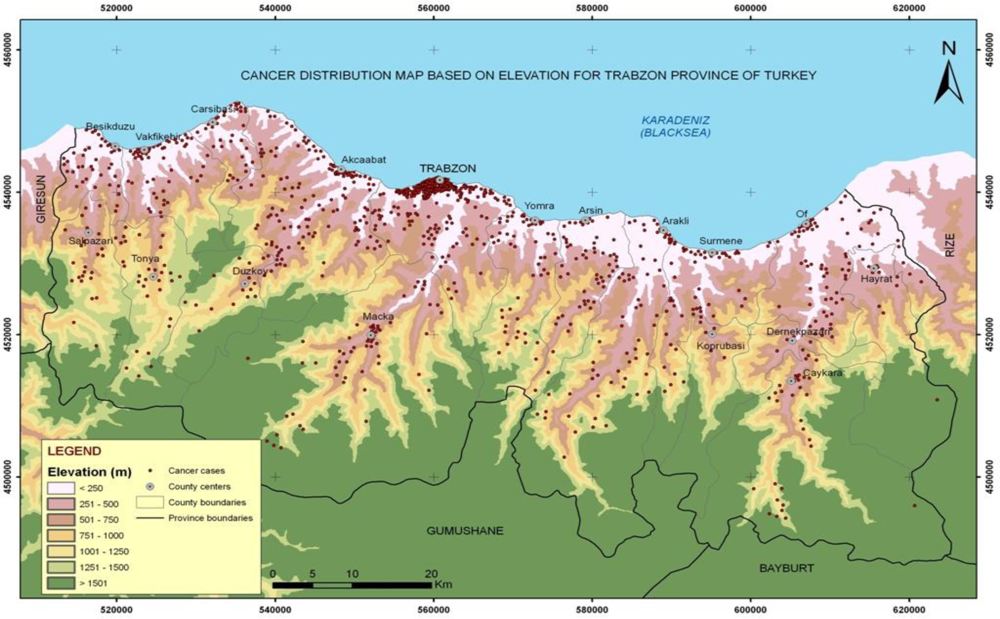
Figure 5.
The distribution map of cancer cases based on elevation.
Table 6.
Crosstab presenting the relationship between elevation and cancer types.
The Table 6 has five elevation classes and eight cancer types. To test whether there is a statistical relationship between elevation and cancer type, The Pearson chi square test was used and indicated that there was a relationship between cancer types and elevation, χ2 = 46.466, df = 28, p = 0.016. If it is supposed that the Ho (null) hypothesis is true, count, expected count, percentage, and adjusted residual are presented in the crosstabs of Table 6 for 1,150 cancer cases.
Examining the percentage of cancer cases in the elevation classes as shown on Table 6, it was found that 54.2 % of all cancer types occurred at 0–250 m, 20.7% at 251–500 m, 11.1% at 501–750 m, 6.6% at 751–1,000 m, and 7.4% at an elevation of more than 1,000 m. If the Ho hypothesis is false, then there is relationship between cancer types and elevation.
In this case, there is a relationship between the 0–250 m elevation class and skin, breast and thyroid cancer types. In addition, breast cancer cases in the 0–250 m elevation have frequency values, count = 77 and expected count = 62. 67.5% of the Breast Cancer Cases occurred within the 0–250 m elevation and these are 6.7% of all cancer cases.
4. Conclusions
Today, GIS is not only a system employed for making disease maps but also leads to better understanding of the causative relationships between the environment and human health. Specifically, consideration of the relationship(s) between cancer cases and environmental factors is important in order to better manage cancer combating strategies and determining the causes of cancer. Therefore, creating geo-referenced maps is necessary to obtain valuable information about cancer cases with respect to frequency in spatial features. The great potential of GIS for health care management is just now beginning to be realized. Data integration and spatial visualization is now highly achievable with GIS. GIS can quickly make maps, and that maps are much easier to understand than tables. Because many do not understand what GIS does and what it could do, getting financial support continues to be a problem. This was a problem identified in the early days of GIS and it remains a problem today.
In this research, GIS applications were carried out in order to analyze the distribution of cancer types geographically. To determine cancer density statistics, the cancer incidence rates of the administrative units were calculated according to local census data then a cancer density map was produced. The ecological data such as land cover and elevation were combined and compared with the locations of cancer cases produced by address geocoding. The administrative units having a high incidence rate were generated combining both GIS and the Pearson chi-square (χ2) statistics analysis to locate areas where greater number of cancer cases occurred.
It is determined that the Trabzon province of Turkey has the number of cancer cases as anticipated by the WHO data, but only 23% of the villages and districts have more than the expected number of cancer cases. A relationship between breast cancer cases, land cover class and elevation class, was determined from statistical examinations. This showed that breast cancer cases commonly occurred in residential areas that are generally situated on the coast and along valleys and within the low elevation class. On the other hand, the numbers of skin and thyroid cancer cases within low elevation class were less than expected. In terms of land cover, the forestry areas, situated in high elevation classes were where more skin and thyroid cancer cases occurred.
In conclusion, the GIS and related spatial analysis methods provide a set of tools to describe and understanding the changing spatial organization of health care, to examine its relationship to health outcomes and access, and to explore how the delivery of health care can be improved. Epidemiologists, for example, have traditionally used maps when analyzing associations between location, environment, and disease. GIS is particularly well suited for studying these associations because of its spatial analysis and display capabilities.
Acknowledgments
The authors gratefully acknowledge the financial support of The Scientific and Technical Research Council of Turkey (TUBITAK) under Project ID: 105Y308.
References
- The International Union Against Cancer. World Cancer Campaign.
- Cancer Control: Knowledge into Action. In WHO Guide for Effective Programmes: Module 1-Planning; World Health Organization: Geneva, Switzerland, 2006.
- San, TA; Sari, D; Turkistanli, EC. Knowledge, Attitudes, Risk Factors, and Early Detection of Cancer Relevant to the School Teachers in Izmir, Turkey. Prev. Med 2005, 40, 636–641. [Google Scholar]
- World Health Organization. WHO Global Infobase Online.
- .
- World Health Organization. 58th World Health Assembly Approved Resolution on Cancer Prevention and Control Report 2005.
- Sengelen, M. Cancer Statistics in Turkey. Science Expertise Thesis, Hacettepe University, Health Science Institute, Ankara, Turkey, 2002 (In Turkish).
- Colak, E; Yomralioglu, T. Creating GIS-Based Cancer Density Maps for Trabzon Province of Turkey. Proceedings of the ESRI Health GIS Conference, Chicago, IL, USA, October 23–26; 2005. [Google Scholar]
- Kistemann, T; Dangendorf, F; Schweikart, J. New Perspectives on the Use of Geographical Information Systems (GIS) in Environmental Health Sciences. Int. J. Hyg. Environ. Health 2002, 205, 169–181. [Google Scholar]
- Vieira, V; Webster, T; Aschengrau, A; Ozonoff, D. A Method for Spatial Analysis of Risk in a Polulation-Based Case-Control Study. Int. J. Hyg. Environ. Health 2002, 205, 115–120. [Google Scholar]
- Friis, R; Sellers, T. Epidemiology for Public Health Practice; Apsen Publications: Gaithersburg, MD, USA, 1996. [Google Scholar]
- Cromley, EK; McLafferty, SL. GIS and Public Health; The Guilford Press: New York, NY, USA, 2002; pp. 158–232. [Google Scholar]
- National Cancer Control Programmes. In Policies and Managerial Guideliness, 2nd ed; World Health Organization: Geneva, Switzerland, 2002.
- Snow, J. On the Mode of Communication of Cholera, 2nd ed; John Churchill: London, UK, 1855. [Google Scholar]
- Haviland, A. The Geographical Distribution of Heart Disease and Dropsy. In Cancer in Phthisis in Females in England and Wales; Swan Schonnenschein: London, UK, 1875. [Google Scholar]
- Walter, SD. Disease Mapping: a Historical Perspective. In Spatial Epidemiology: Methods and Applications, 1st ed; Elliott, P, Wakefield, J, Best, N, Briggs, D, Eds.; Oxford University Press: New York, NY, USA, 2000; pp. 223–239. [Google Scholar]
- Morra, P; Bagli, S; Spadoni, G. The Analysis of Human Health Risk with a Detailed Procedure Operating in a GIS Environment. Environ. Int 2006, 32, 444–454. [Google Scholar]
- Pearce, J; Boyle, P. Examining the Relationship between Lung Cancer and Radon in Small Areas across Scotland. Health Place 2005, 11, 275–282. [Google Scholar]
- Poulstrup, A; Hansen, HL. Use of GIS and Exposure Modeling as Tools in a Study of Cancer Incidence in a Population Exposed to Airborne Dioxin. Environ. Health Perspect 2004, 112, 1032–1036. [Google Scholar]
- Elliott, P; Wakefield, J; Best, N; Briggs, D. Spatial Epidemiology: Methods and Applications. In Spatial Epidemiology: Methods and Applications, 1st ed; Elliott, P, Wakefield, J, Best, N, Briggs, D, Eds.; Oxford University Press: New York, NY, USA, 2000; pp. 3–15. [Google Scholar]
- Flinton, DM; Walters, NJ. Occupational Activity and Risk of Prostate Cancer in Ireland. J. Radiother. Pract 2004, 4, 102–106. [Google Scholar]
- Grauman, DJ; Robert, E; Tarone, RE; Devesa, SS; Fraumeni, JF. Alternate Ranging Methods for Cancer Mortality Maps. J. Natl. Cancer Inst 2000, 92, 534–543. [Google Scholar]
- Gregorio, DI; Cromley, E; Mrozinski, R; Walsh, SJ. Subject Loss in Spatial Analysis of breast cancer. Health Place 1999, 5, 173–177. [Google Scholar]
- Mosavi-Jarrahi, A; Moini, M; Mohagheghi, M; Alebouyeh, M; Yazdizadeh, B; Shahabian, A; Nahvijo, A; Alizadeh, R. Clustering of Childhood Cancer in the Inner City of Tehran Metropolitan Area: A GIS-Based Analysis. Int. J. Hyg. Environ. Health 2007, 210, 113–119. [Google Scholar]
- Oliver, MN; Matthews, KA; Siadaty, M; Hauck, FR; Pickle, LW. Geographic Bias Related to Geocoding in Epidemiologic Studies. Int. J. Health Geogr 2005, 4, 29. [Google Scholar]
- Pickle, LW; Waller, LA; Lawson, AB. Current Practices in Cancer Spatial Data Analysis: A Call for Guidance. Int. J. Health Geogr 2005, 4, 3. [Google Scholar]
- Roche, LM; Skinner, R; Weinstein, RB. Use of a Geographic System to Identify and Characterize Areas with High Proportions of Distant Stage Breast Cancer. J. Publ. Health Manag. Pract 2002, 8, 26–32. [Google Scholar]
- Scott, D; Curtis, B; Twumasi, FO. Towards the Creation of a Health Information System for Cancer in KwaZulu-Natal, South Africa. Health Place 2002, 8, 237–249. [Google Scholar]
- Lawson, AB. Statistical Methods in Spatial Epidemiology, 2nd ed; John Wiley & Sons: England, UK, 2006. [Google Scholar]
- Pickle, LW. Spatial Analysis of Disease. In Biostatistical Applications in Cancer Research; Beam, C, Ed.; Klewer Academic Publishers: Boston, USA, 2002; pp. 113–150. [Google Scholar]
- Waller, LA; Gotway, CA. Applied Spatial Statistics for Public Health Data; John Wiley & Sons, Inc: Hoboken, NJ, USA, 2004. [Google Scholar]
- Cancer Control Department. Cancer Control Policy and Cancer Data 1995–99, Republic of Turkey, Ministry of Health, Report No: 618; Ankara, Turkey, 2000 (In Turkish).
- Turkey State Planning Organization. Socio-economic Development Ranking of Provinces of Turkey, May 2003; ; Issue No: 2671; Turkey, 2003; pp. 250.
- .
- Annoni, A; Luzet, C; Gubler, E; Ihde, J. Map Projections for Europe; European Commission Joint Research Centre, Institute for Environment and Sustainability: Italy, 2003. [Google Scholar]
- Bilge, N. Standardization of Education and Radiotherapy Centers related to Cancer in Turkey. In Cancer Rate in Turkey; Tuncer, I, Ed.; TUBITAK and Cukurova University: Adana, Turkey, 1994. (In Turkish) [Google Scholar]







© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).