National Survey of the Smoking Cessation Services in Italy


Abstract
:1. Introduction
2. Experimental Section Methods
2.1. Study Participants
2.2. Data Collection
2.2.1. SCS Locations and Additional Information on Service’s Organization
2.2.2. Service’s Access Modalities
2.2.3. Smoking Cessation Programs Offered
2.2.4. SCS Staff and Professional’s Qualification of Specialists
2.2.5. Number of Smokers Treated in 2007
2.3. Data Analysis
3. Results
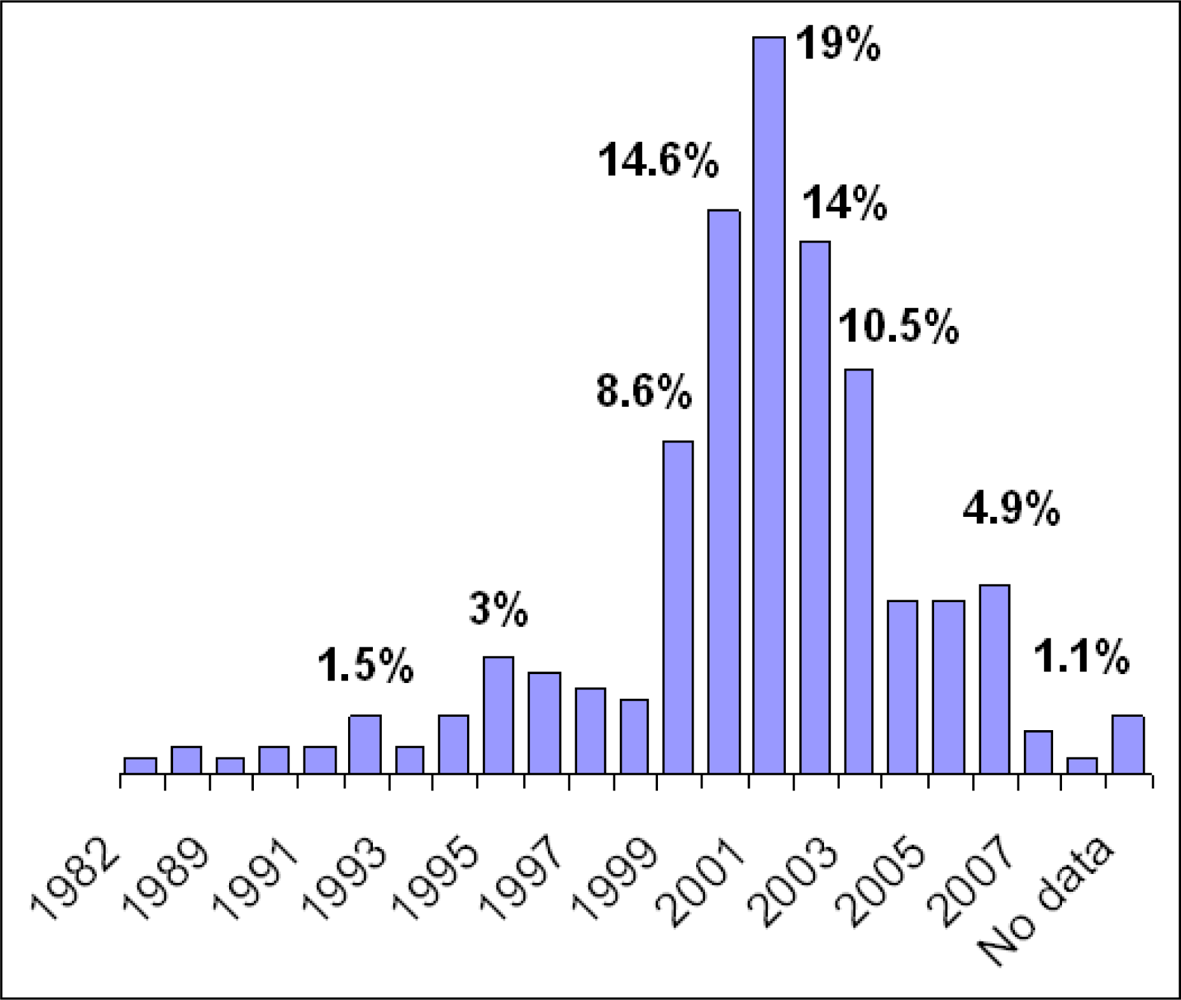
3.1. SCS Locations and Organization
3.2. Service Access Modalities
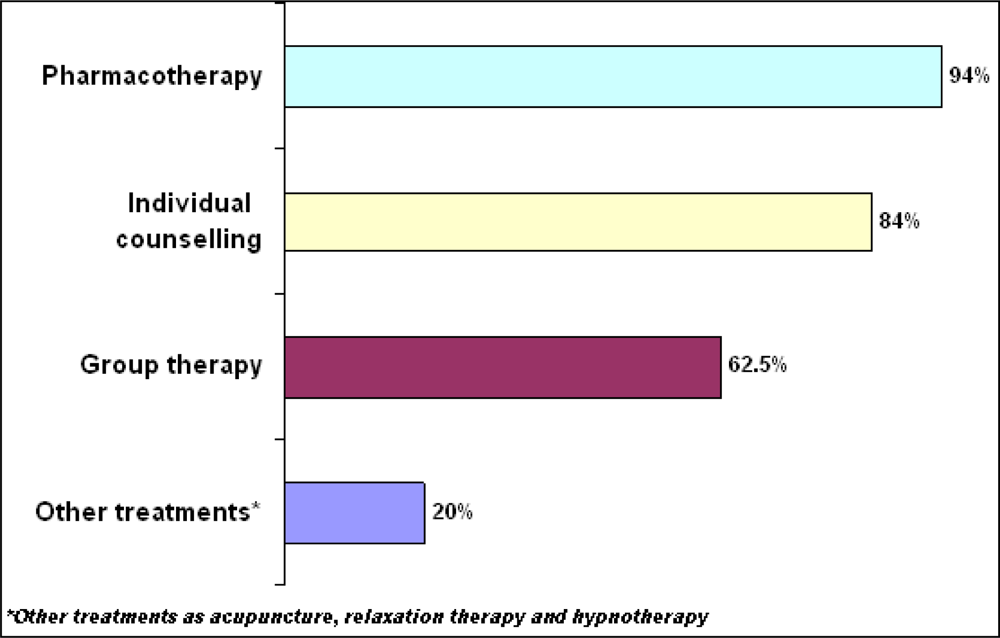
3.3. Smoking Cessation Programs
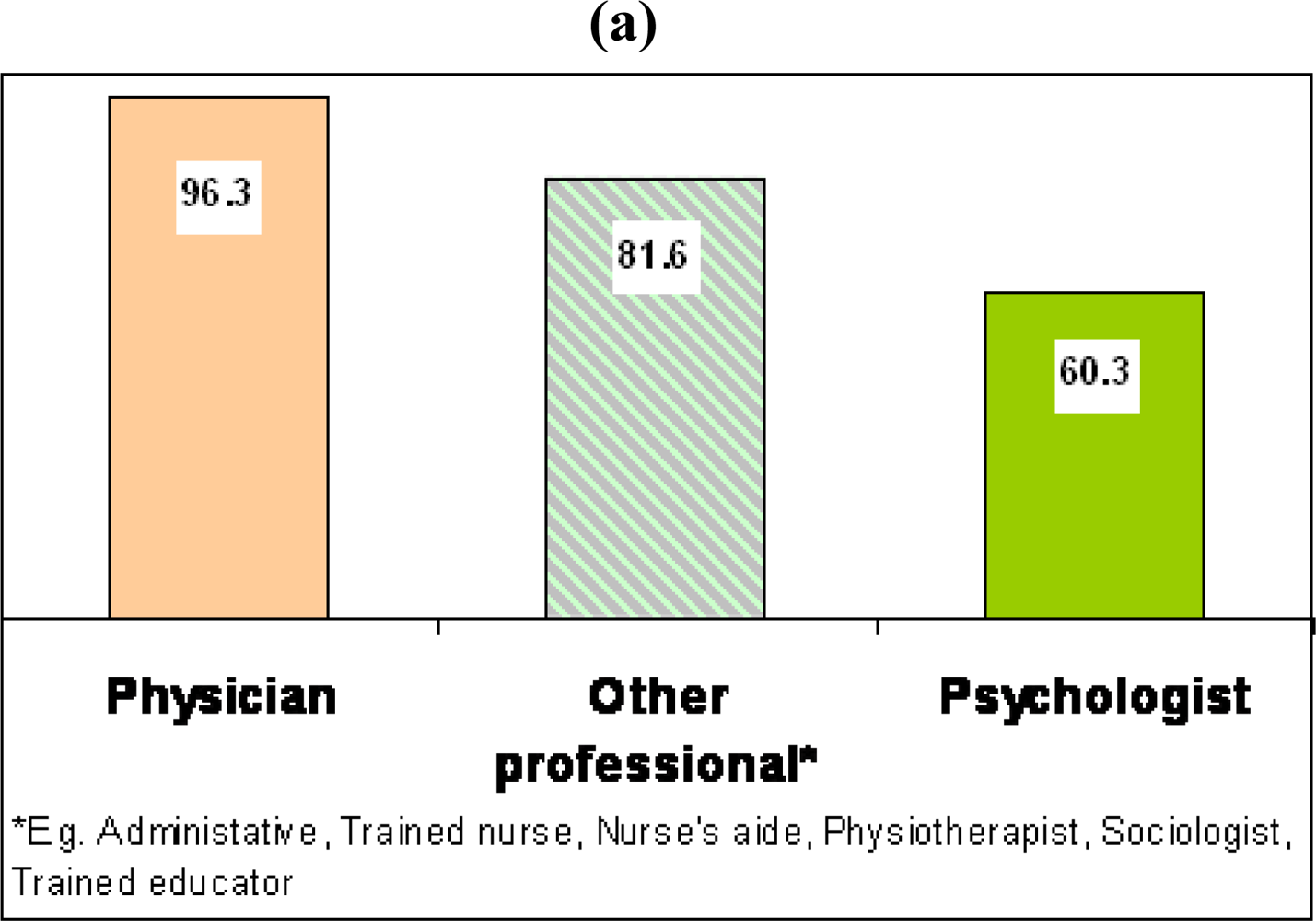
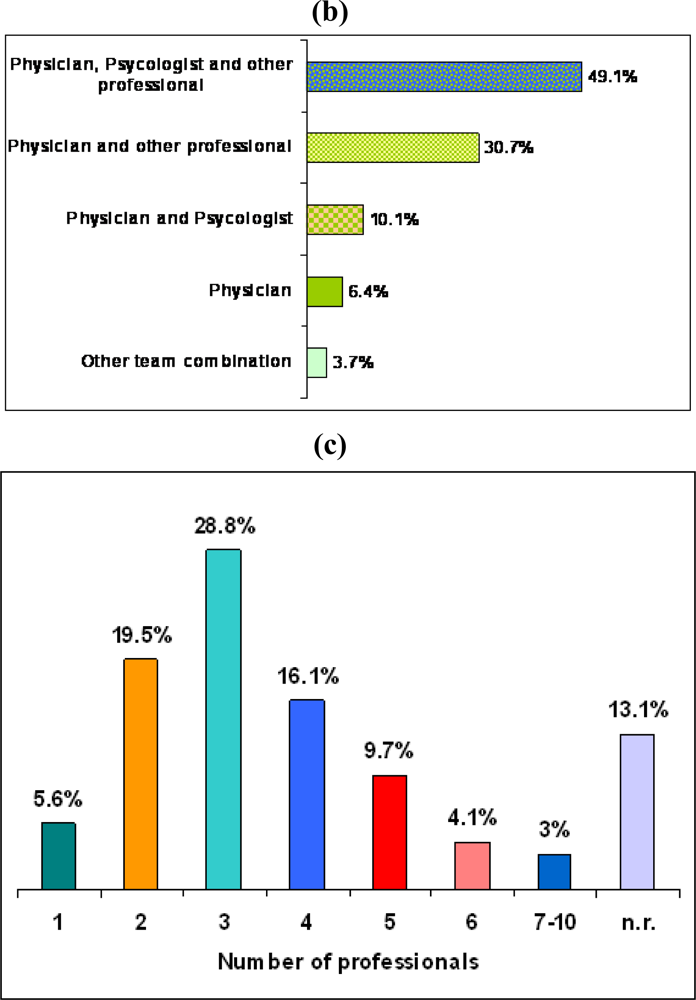
3.4. SCS Staff and Professional’s Qualification
3.5. Number of Individuals Treated for Smoking Habit during 2007
4. Discussion and Conclusions
Acknowledgments
Appendix 1. Structured interview form

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SCS location/setting and information on service organization |
| Institution connected to SCS (Local health units/hospital/other): |
| Department: |
| SCS denomination and Address: |
| Principal Coordinator (Surname/ First name/ Address): |
| Service activation year: ________ |
| Legal authorization that regulates SCS activities: |
| Service access modalities |
| Registration procedures:
□ By telephone □ Direct to SCS □ Other |
| Registration modalities:
□ Written family doctor request □ Free admission □ Other__________ |
| Consulting days per week:
□ 1–3 days □ 4–5 days □ 6–7 days □ other____________/___________________ |
| Costs to access the tobacco-use cessation program:
□ Patient’s contribution required □ Cost-free □ Other________ |
| Smoking cessation programs |
| □ Pharmacotherapy__________________________ |
| □ Individual counseling__________________________ |
| □ Group therapy__________________________ |
| □ Other treatments (specify) __________________________ |
| For all programs specify frequency and duration of therapeutic treatment |
| SCS Staff and Professional’s Qualification |
| Number and Professional’s qualifications: |
| □ N. __ Physician |
| □ N. __ Clinical Psychologist |
| □ N. __ Other professional (specify) __________________________ |
| □ N. __ Other professional (specify) __________________________ |
| Number of Smokers treated in 2007 |
| Numbers of individuals who received at least one treatment to quit smoking in 2007: ______ |
References
- Zuccaro, P; Di Pucchio, A; Pizzi, E; Martucci, L; Carosi, G; Solimini, R; Rossi, S. Il fumo in Italia. Respiro 2008, 2, 23–24. [Google Scholar]
- Osservatorio Fumo, Alcol e Droga. Il fumo in Italia: Indagine DOXA 2008; Istituto Superiore di Sanita’: Roma, Italy, 2008. [Google Scholar]
- Pacifici, R. Tabagismo e Servizio Sanitario Nazionale: prospettive ed impegni. Presented at the X Convegno Nazionale; Tabagismo e Servizio Sanitario Nazionale: Rome, Italy, May 2008. [Google Scholar]
- Gallus, S; Zuccaro, P; Colombo, P; Apolone, G; Pacifici, R; Garattini, S; Bosetti, C; La Vecchia, C. Smoking in Italy 2005–2006: effects of a comprehensive national tobacco regulation. Prev. Med 2007, 45, 198–201. [Google Scholar]
- Rossi, S; Carosi, G; Spoletini, R; Pizzi, E; Di Pucchio, A; Mattioli, D; Mazzola, M; Mastrobattista, L; Solimini, R; Pacifici, R. IX Convegno Nazionale “Tabagismo e Servizio Sanitario Nazionale“. Not Ist Super Sanità. 2007, 20, pp. 17–19. Available at http://www.iss.it/binary/publ/cont/lu-ago.1188907080.pdf (accessed February 2009).
- U.S. Department of Health and Human Services. Treating Tobacco Use and Dependence: 2008 Update; Public Health Service: Rockville, MD, U.S.A., May 2008. [Google Scholar]
- Lancaster, T; Stead, L; Silagy, C; Sowden, A. Effectiveness of interventions to help people stop smoking: findings from the Cochrane Library. BMJ 2000, 321, 355–358. [Google Scholar]
- Belleudi, V; Bargagli, AM; Davoli, M; Di Pucchio, A; Pacifici, R; Pizzi, E; Zuccaro, P; Perucci, CA. Gruppo di Studio dei Servizi Territoriali per la Cessazione dal Fumo. Interventi per la cessazione dell’abitudine al fumo in Italia: offerta ed efficacia nella pratica. Risultati di uno studio longitudinale multicentrico. Epidemiologia Prevenzione 2007, 31, 148–157. [Google Scholar]
- Ferguson, J; Bauld, L; Chesterman, J; Judge, K. The English smoking treatment services: one-year outcomes. Addiction 2005, 100, 59–69. [Google Scholar]
- Bauld, L; Chesterman, J; Judge, K; Pound, E; Coleman, T. On behalf of the English Evaluation of Smoking Cessation Services (EESCS). Impact of UK National Health Service smoking cessation services: variations in outcomes in England. Tob. Control 2003, 12, 296–301. [Google Scholar]
- Pizzi, E; Di Pucchio, A; Rossi, S; Carosi, G; Martucci, L; Mattioli, D; Mazzola, M; Mortali, C; Pacifici, R; Zuccaro, P. Guida ai Servizi Sanitari Territoriali per la Cessazione dal Fumo di Tabacco (aggiornamento 2007). Strumenti di Riferimento; Istituto Superiore di Sanità, 2008. 08/S1; Available at http://www.iss.it/binary/publ/cont/08_S1%20web.1209980472.pdf (accessed February 2009).
- Ferketich, AK; Gallus, S; Colombo, P; Fossati, R; Apolone, G; Zuccaro, P; La Vecchia, C. Physician-Delivered Advice to Quit Smoking Among Italian Smokers. Am. J. Prev. Med 2008, 35, 60–63. [Google Scholar]
- McEwen, A; West, R; Owen, L; Raw, M. General practitioners’ views on and referral to NHS smoking cessation services. Public Health 2005, 119, 262–268. [Google Scholar]
- Zuccaro, P; Di Pucchio, A; Martucci, L; Modigliani, G; Pizzi, E; Pacifici, R. Guida ai Servizi Territoriali per la Cessazione dal Fumo di Tabacco. Strumenti di Riferimento; Istituto Superiore di Sanita’, 2001. 18; Available at http://www.iss.it/binary/publ/publi/0118.1110208615.pdf (accessed February 2009).
- Pacifici, R; Di Pucchio, A; Pizzi, E; Pichini, S; Zuccaro, P. Italian Smoking Cessation Services: A National Network. In Abstract book 2003, Proceedings of 12th World Conference on Tobacco or Health, Helsinki, Finland, August 2003.
- Pacifici, R; Pizzi, E; Di Pucchio, A; Zuccaro, P; Galeone, D; Greco, D; Maglione, T. Gruppo Tecnico sul Tabagismo delle Regioni e Provincie Autonome. Servizi territoriali per la cessazione dal fumo di tabacco: risultati di una ricerca nazionale. Rapporti Istisan; Istituto Superiore di Sanità, 2006. 06/8; Available at http://www.cedostar.it/documenti/elenco_servizi_tabagismo_iss_2006.PDF (accessed February 2009).
- Di Pucchio, A; Pizzi, E; Solimini, R; Mastrobattista, L; Rossi, S. Structural and operational characteristics of Italian Smoking cessation Services: a national investigation. In Final Program Book 2008, Proceedings of 10th Annual Conference of SRNT Europe, Rome, Italy; September 2008; p. 173. [Google Scholar]
- Zuccaro, P; Caraffa, G; Corti, FM; Davoli, M; Enea, D; Fogliani, V; Galeone, D; Malvezzi, E; Minozzi, S; Nardini, S; Pacifici, R; Vannuzzo, D. Gruppo di Lavoro OssFAD. Linee Guida per promuovere la cessazione dell’abitudine al fumo. Guida breve per la realizzazione degli interventi (Aggiornamento 2008); Istituto Superiore di Sanità: Roma, Italy, 2008. Available at http://www.iss.it/binary/ofad/cont/linee%20guida%20brevi%202008%20per%20web.1211805168.pdf (accessed February 2009).
- Raw, M; Regan, S; Rigotti, NA; McNeill, A. A survey of tobacco dependence treatment services in 36 countries. Addiction 2008, 104, 279–287. [Google Scholar]




| Geographic availability of SCS | % |
|---|---|
| North | 59 |
| Central | 22 |
| South and Island | 19 |
Institution connected to SCS | |
| Local health units | 55.8 |
| Hospital | 40.8 |
| Other* | 3.4 |
SCS location | |
| Department of Drug Addiction | 29.9 |
| Department of Lung and Breath Care | 29.6 |
| Other locations** | 40.5 |
| SCS Characteristics | % |
|---|---|
| Registration procedures | |
| By telephone | 33.9 |
| Direct to SCS | 1.3 |
| A combination of both | 64.8 |
Registration modalities | |
| Written family doctor request | 49.8 |
| Free admission | 44.6 |
| A combination of both | 4.8 |
| Data not available | 0.8 |
Consulting days per week | |
| 1–3 days | 36.3 |
| 4–5 days | 43.1 |
| 6–7 days | 3.4 |
| Data not available | 17.2 |
Costs of access to smoking cessation programs | |
| Patient’s contribution required | 59 |
| Cost-free | 22 |
| A combination of both | 19 |
| Combinations of therapeutic treatment | % |
|---|---|
| Pharmacotherapy + Individual counseling +group therapy | 32.2 |
| Pharmacotherapy + Individual counseling | 22.1 |
| Pharmacotherapy + Individual counseling +group therapy + other treatment* | 17.6 |
| Other combinations | 28.1 |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Di Pucchio, A.; Pizzi, E.; Carosi, G.; Mazzola, M.; Mattioli, D.; Pacifici, R.; Pichini, S. National Survey of the Smoking Cessation Services in Italy. Int. J. Environ. Res. Public Health 2009, 6, 915-926. https://doi.org/10.3390/ijerph6030915
Di Pucchio A, Pizzi E, Carosi G, Mazzola M, Mattioli D, Pacifici R, Pichini S. National Survey of the Smoking Cessation Services in Italy. International Journal of Environmental Research and Public Health. 2009; 6(3):915-926. https://doi.org/10.3390/ijerph6030915
Chicago/Turabian StyleDi Pucchio, Alessandra, Enrica Pizzi, Giordano Carosi, Monica Mazzola, Donatella Mattioli, Roberta Pacifici, and Simona Pichini. 2009. "National Survey of the Smoking Cessation Services in Italy" International Journal of Environmental Research and Public Health 6, no. 3: 915-926. https://doi.org/10.3390/ijerph6030915
APA StyleDi Pucchio, A., Pizzi, E., Carosi, G., Mazzola, M., Mattioli, D., Pacifici, R., & Pichini, S. (2009). National Survey of the Smoking Cessation Services in Italy. International Journal of Environmental Research and Public Health, 6(3), 915-926. https://doi.org/10.3390/ijerph6030915