1. Introduction
The marked increases in prevalence of overweight and obesity over the last several decades in the United States poses a major public health concern [
1]. Toxic metals may be conjectured to play a role in contributing to obesity by displacing vital metals such as zinc, chromium, copper, iron, and magnesium, which may in turn affect energy production, carbohydrate tolerance, and other metabolic process[
2]. In mice, zinc deficiency induced by a mutation in the Znt7 zinc transporter caused a reduced body weight gain that was largely due to the decrease in body fat accumulation [
3]. In contrast, deficiency of other essential metals, chromium [
4,
5], copper [
6], iron [
7,
8], and magnesium [
9], causes an increase in adiposity. The toxic metals, lead and cadmium are ubiquitous environmental toxins that are related to a broad range of physiologic, biochemical, and behavioral dysfunctions[
10,
11] and recent epidemiologic studies have reported that environmental exposure to lead or cadmium concentration has a graded association with several disease outcomes such as hypertension, peripheral artery diseases, kidney diseases, and cognitive impairment [
12–
17]. To our knowledge, this is the first study to demonstrate an association between lead and other toxic metals and obesity.
Heavy metals are a heterogeneous group of highly reactive substances, which may act as essential cofactors for physiologic processes and/or as toxic elements. Some metals induce oxidative stress directly, such as iron redox-cycling between Fe
3+ and Fe
2+ and creating superoxide (O
2−) in the process [
18]. Whereas iron (Fe), copper (Cu), chromium (Cr), vanadium (V) and cobalt (Co) undergo redox-cycling reactions under physiological conditions, other metals such as mercury (Hg), cadmium (Cd) and nickel (Ni), and arsenic (As) increase oxidative stress indirectly by depleting glutathione and bonding to sulfhydryl groups of proteins [
18]. The unifying factor in determining metal toxicity is the generation of reactive oxygen and nitrogen species [
18].
The toxic metals we investigated in this study range from ubiquitous to rare in the environment. Lead, cadmium, cobalt, antimony, and cesium are all on the 2007 CERCLA (Comprehensive Environmental Response, Compensation, and Liability Act) priority list of hazardous substances (
http://www.atsdr.cdc.gov/cercla/index.html). The CERCLA requires the EPA to prepare a list, in order of priority, of substances that are most commonly found at Superfund sites (also known as the National Priority List (NPL) sites). These contaminants are determined to pose the most significant potential threat to human health due to their known or suspected toxicity and potential for human exposure at these NPL sites.
As an initial exploratory inquiry, the present study investigated the association of body mass index (BMI) and waist circumference (WC) with toxic metals adjusting for age, ethnicity, and gender via multiple linear regressions using participants aged 6–60 across National Health and Nutrition Examination Survey (NHANES) 99-02. BMI is calculated as weight in kilograms/height in meters squared and WC is measured in centimeters. The toxic metals examined included barium, cadmium, cobalt, cesium, molybdenum, lead, antimony, thallium, and tungsten.
4. Conclusions
Our results indicate several significant associations. The toxic metals barium and thallium are positively associated with BMI and WC, whereas cadmium, cobalt, cesium, and lead are negatively associated with BMI and WC. Most toxic metals such as cadmium have more than one oxidation state; accordingly the same metal may have different effects on humans [
18]. Weight gain or weight loss, depending on the toxic metal, tends to occur at much lower levels of exposure of metals than those that make animals or humans obviously ill. For example, the CDC health concern blood lead level (BLL) is 10 μg/dL, and higher levels warrant intervention such as chelation therapy, especially in children [
26]. The mean BLL in the NHANES, 1999–2000, population is 2.7 μg/dL and only 4.4% had BLL concentrations above the CDC health concern level [
27]. A broad range of lead levels had negative associations with BMI and WC, suggesting that levels much lower than 10 μg/dL affect these traits. This result is consistent with studies of neurodevelopmenttal defects in children associated with low blood lead levels that have led to call for the Centers for Disease Control and Prevention to reduce the current screening guideline of 10 μg/dL [
28–
31]. Exposure to lead can happen from breathing workplace air or dust, eating contaminated foods, or drinking contaminated water. Lead has been found in at least 1,272 of the 1,684 National Priority List (NPL) sites identified by the Environmental Protection Agency (EPA) (
http://www.atsdr.cdc.gov/cercla/index.html).
The other toxic metals in this study have various sources. Exposure to barium occurs mostly in the workplace or from drinking contaminated water. Barium and barium compounds have been found in at least 798 of the 1,684 NPL sites identified by the EPA. Exposure to thallium occurs mainly from eating food, but high levels of exposure may occur in the workplace. Thallium has been found in at least 210 of 1,416 NPL sites identified by the EPA. Exposure to cadmium happens mostly in the workplace, but lower doses are obtained from breathing cigarette smoke or eating cadmium contaminated foods. Cadmium has been found in at least 1,014 of the 1,669 NPL sites identified by the EPA. The general population is exposed to low levels of cobalt in air, water, and food. Cobalt has both beneficial effects, as part of vitamin B12, and harmful effects on health at high doses. Cobalt has been found in at least 426 of the 1,636 NPL sites identified by the EPA. Exposure to stable or radioactive cesium occurs from ingesting contaminated food or drinking water or breathing contaminated air. High levels of radioactive cesium may occur after nuclear accidents or detonation of atomic bombs. Stable (non-radioactive) cesium has been found in at least 8 of the 1,636 NPL sites and radioactive cesium has been found in at least 23 of the 1,636 NPL sites identified by the EPA.
One possible explanation for why some toxic metals (barium and thallium) positively associate with obesity is that they induce oxidative stress, which increases lipogenesis at the expense of energy production [
32]. Oxidative stress can be either by directly generating free radicals, in the case of redox-cycling metals such as barium or thallium, or indirectly by non-redox cycling metals such as lead and mercury [
18]. Indirect induction of oxidative stress can be mediated by reducing glutathione levels or by interfering with iron metabolism. Reactive oxygen species directly or indirectly generated by metals can inhibit the normal mitochondrial metabolic function, and prevent the mitochondria from producing energy, in the form of ATP, by oxidative phosphorylation. The lower levels of ATP, coupled by the diminished efficacy of the tricarboxylic acid (TCA) cycle due to inhibition of enzymes such as aconitase, which are sensitve to oxidative stress, would cause the liver to divert metabolites to lipogenesis [
32]. However, if metal-induced oxidative stress is a major cause of obesity, it is not clear why some metals, such as barium and thallium, positively associate with obesity, whereas other metals, such as lead, cadmium, and cesium negatively associate with obesity.
The finding that lead, cadmium, cobalt, and cesium negatively associate with obesity is surprising. A recent study has shown that lead is a predictor of diabetic neuropathy, and that chelation therapy that reduces the lead burden slows the rate of diabetic neuropathy [
19]. Also, even in patients without diabetes, lead chelation therapy has been shown to slow the progression of chronic renal diseases [
33,
34]. Furthermore, using data from the Normative Aging Study, Tsaih and colleagues [
35] showed significant interactions of blood lead and tibia lead with diabetes and renal function. For example, increasing the tibia lead level from the lowest to the highest quartiles was associated with an increase in the rate of rise of serum creatinine that was 17.6 fold greater in diabetics than in non-diabetics. The implication of this result is that lead damages the kidneys much more readily in diabetics than in non-diabetics [
35]. Our study suggests that cadmium, cobalt, and cesium might function in a manner similar to lead in that, for whatever reason, they all negatively associate with obesity. It will be interesting to determine whether, like lead, any of the other toxic metals in our study positively associate with diabetic neuropathy.
However, urine lead levels, which were all that is available in the NHANES 99-02 studies analyzed here, only reflect recent lead exposures and the abovementioned studies were careful to also analyze total lead burden by measuring lead levels after EDTA chelation [
19,
33,
34], which mobilizes lead from the bone to the circulation, or X-ray analyses of bone lead [
35]. Blood lead levels are only proportional to body lead levels if there is a constant exposure to lead. However, blood lead levels have fallen over the past three decades in the U.S. because of the elimination of leaded paint and gasoline in the late 1970s, whereas the body burden of lead can last for several decades [
36].
It is possible that the negative association between obesity and blood lead levels is misleading. There is a positive association between creatinine levels and obesity, and several studies have shown that body lead levels are proportional to creatinine levels because, as mentioned above, lead positively associates with kidney dysfunction and this prevents proper filtration of creatinine, which is produced from creatine kinase breakdown in muscles from the blood [
19,
33,
34]. Also, a recent study has shown that recent severe weight loss can cause the release of stored lead from bones [
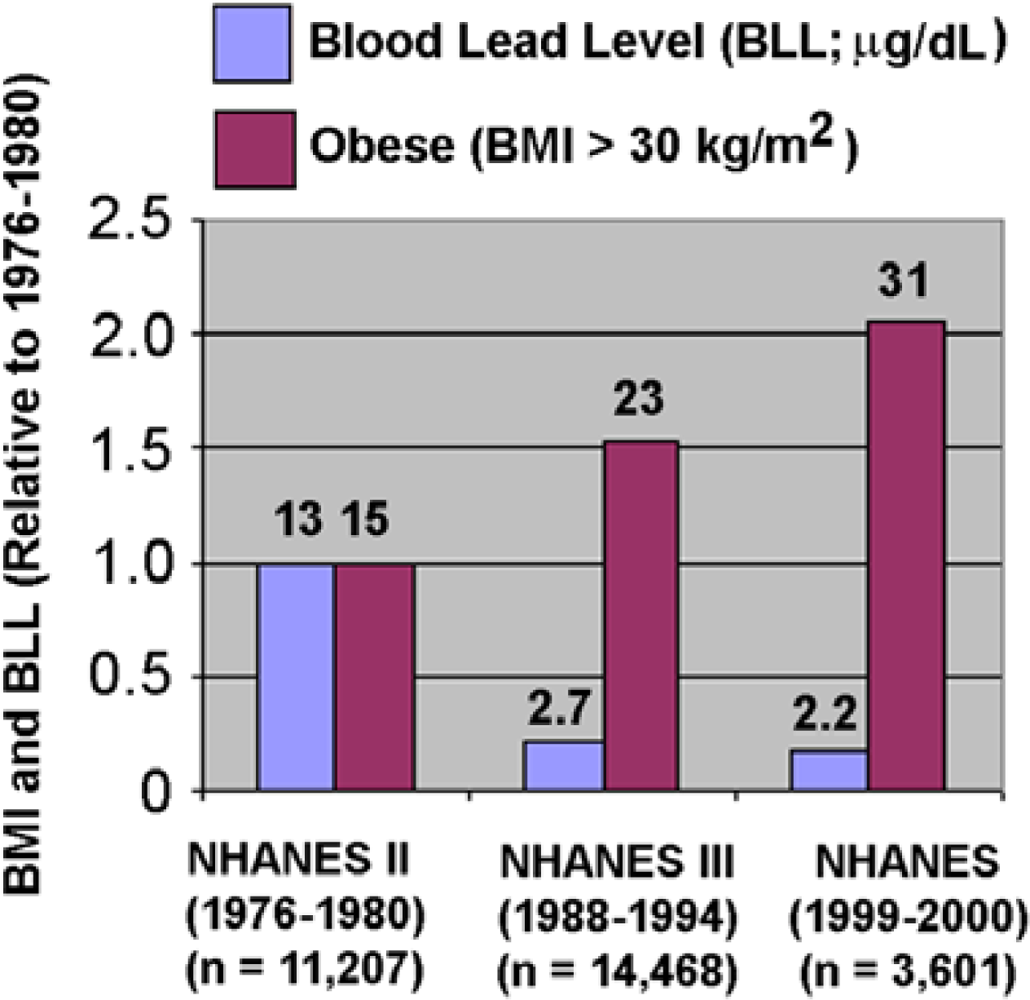
37], and the weight history of the NHANES sample is not completely known. However, as shown in
Figure 1, there has been a steady decrease in blood lead levels from 1977 to 2000 at the same time that there has been a steady increase in obesity in the NHANES populations. This result is consistent with lead being negatively associated with obesity. We note that
Figure 1 is based on NHANES population studies, which are cross-sectional in that both metals and outcomes are assessed at the same time. Further prospective studies are needed to address the temporality of these findings.
In conclusion, there is, by and large, a negative association of heavy toxic metal urine concentrations with BMI and WC. This suggests that the association of heavy metals with BMI and WC is still unclear because the findings here are in the opposite direction of past research and hypotheses. Future research should be further conducted in order to establish a clear understanding of the association of heavy metals with BMI and WC.





{kind=link}