1. Introduction
In Canada, prescription opioid use has increased steadily over the past two decades with marked increases in the number of opioid overdoses and opioid-related deaths [
1]. National strategies and guidelines have been developed to address the opioid crisis but they primarily focus on opioid use in chronic noncancer pain populations [
2].
In oncology and palliative care, there remains a pervasive belief that the risk of opioid use disorder (OUD) is low, despite a paucity of supporting research [
3,
4]. Increasingly, evidence suggests that patients with cancer might be at higher risk of nonmedical opioid use (NMOU) than was previously thought [
5,
6,
7]. An integrative literature review by Carmichael et al. found that at least one in five patients with cancer may be at risk of OUD [
5]. Despite this, there is scant literature on opioid risk evaluation and mitigation in the cancer population, and few guidelines on how to manage NMOU and substance use disorders in patients with cancer [
6,
7,
8,
9]. The limited literature outlines similar risk mitigation strategies as those recommended for the chronic noncancer pain population including screening, a multidisciplinary approach, utilization of adjuvant agents, structured dispensing, pill counts, urine drug tests, and treatment contracts [
10,
11,
12,
13]. Unfortunately, the evidence base for utilizing these approaches for patients with cancer is lacking [
13].
Given the increasing incidence and survival rates for cancer [
14], and the growing emphasis on early palliative care [
15], more patients are exposed to opioids for longer periods of time. It is thus essential that both clinicians and patients are educated around the safe and effective use of opioids, in order to maximize quality of life while minimizing risk. This study aimed to describe oncology clinicians’ attitudes, confidence, and practices around managing opioids prescribed to patients with cancer in the outpatient setting.
2. Materials and Methods
For this cross-sectional study, we developed three profession-specific surveys to assess opioid management and safety practices of those who provide outpatient clinical care, including: (1) physicians/nurse practitioners (MD/NP), (2) nurses (including registered nurses (RN) and clinical nurse specialists (CNS)), and (3) pharmacists. These surveys were developed by an interdisciplinary research team of nurses, pharmacists and physicians working in palliative care, based on clinical experience and nonsystematic literature review. The surveys were also reviewed by addictions medicine and oncology clinicians. There were no major differences in survey content between the three profession-specific surveys, however some questions were reworded or reframed in order to be relevant to the scope of each profession’s practice. A copy of the survey adapted for pharmacists is available in
Supplementary Materials.
Each survey was piloted with at least two individuals from each profession. No major revisions to the survey content were necessary based on the feedback from this initial pilot. The surveys addressed the following topics: demographics, attitudes towards opioid use in cancer care, confidence and practices in managing opioids in cancer care, personal experiences with adverse events in patients with cancer using opioids, and education and resources. The surveys employed 4 and 5-point Likert scales to rate the frequency of practice, or level of agreement, respectively. Surveys were administered in English. Ethics approval was obtained through University Health Network—Research Ethics Board (Coordinated Approval Process for Clinical Research, ID 18-6052) on December 14, 2018.
Final surveys were built using Qualtrics Survey Software™ (Qualtrics XM, Qualtrics LLC, Provo, UT, USA), a secure web-based survey tool. Invitations were distributed in January 2019 by department leads in the areas of palliative care, oncology, nursing, and pharmacy at the Princess Margaret Cancer Centre (PM) in Toronto, Canada, a tertiary cancer center. Reminder emails were sent 4 weeks after the initial invitation emails were sent. The survey remained open for approximately 2 months. Eligible participants were RN, CNS, pharmacists, MD and NP fluent in English, and employed at PM to provide outpatient care to patients with cancer. Employees who did not provide outpatient care and trainees were not eligible. This study employed an implied consent process. Completion of the surveys was taken as the participants’ consent to participate in the study. The invitation and reminder emails included information on the study’s purpose, risks and benefits of participation, estimated amount of time required to complete the survey, a link to voluntarily complete the survey online through the use of the software program, Qualtrics, and outlined their ability to withdraw from the study at any time. Surveys were completed anonymously.
Descriptive analyses of the survey results were conducted. Counts and proportions were provided for demographic or practice-related variables. Mean (SD) and median (range) were calculated for continuous variables. The differences in survey responses among the three profession groups were compared using Chi-squared tests or Fisher’s exact tests. Correlations between average practice and average confidence were calculated. In addition, univariate linear regression models were performed to examine the associations between the outcome variable ‘average practice score’ and factors of interest, such as ‘average confidence score’, profession, gender, and years in practice. Average practice score was the numeric average of all opioid safety practice question responses (never: 1, rarely: 2, often: 3, always: 4). Average confidence score was the numeric average of all confidence question responses (assigned as strongly disagree: -2; somewhat disagree: -1; neutral: 0; somewhat agree: 1; strongly agree: 2). Variables showing statistical importance in the univariate analyses (p < 0.10), or with clinical importance, were entered into the multiple linear regression model. Statistical significance defined as p-value 0.05. SAS 9.4 (SAS Institute, Cary, NC, USA) was used to perform the statistical analyses.
3. Results
Given the survey length, we will present findings focused on demographics, attitudes towards opioid use in cancer care, confidence and practices in managing opioids in cancer care. The surveys were distributed to approximately 400 clinicians in January 2019, based on best estimates of staffing numbers within the cancer center. Sixty-five responses were received, including incomplete surveys; a response rate of 16%. Of these, 27 were MD/NP (41%), 31 were RN/CNS (48%), and 7 were pharmacists (11%). Thirty-five (54%) participants had been working in oncology for 10 years or less (
Table 1).
Over a third of respondents (37%) agreed that patients with cancer are at very low risk for opioid-related harms because they have pain. Fifty-three percent agreed that patients with cancer frequently do not take their opioids as prescribed. Fifteen percent agreed that patients with cancer frequently become addicted to opioids. Twenty-seven percent agreed that many patients with cancer have comorbidities that put them at high risk for developing OUD. Twenty-five percent agreed that many patients with cancer are at high risk of opioid overdose.
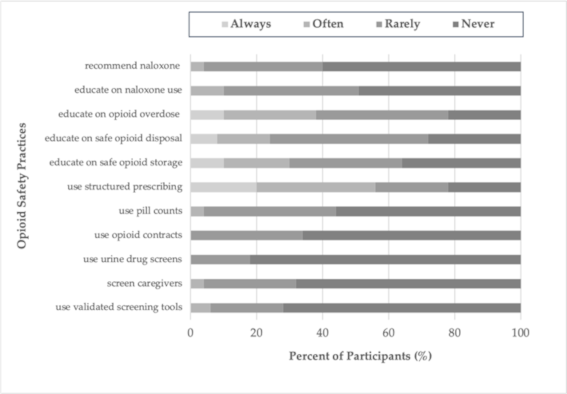
While a majority of respondents felt confident assessing patients’ pain while on opioids (75%), or providing pain management for a patient on opioid agonist therapy (OAT) (74%), only 55% felt confident managing aberrant medication taking behaviors, 39% in recognizing signs of OUD and only 47% in screening for OUD (
Table 2). In terms of opioid safety practices, over half of participants never recommended or educated patients around naloxone use, utilized screening tools, pill counting, or urine drug screens. Over 60% rarely or never provided education on the safe storage or disposal of opioids (
Figure 1).
Univariate linear regression analyses results demonstrated that practice score was significantly associated with confidence score and profession, whereas gender and years in palliative and oncology practice did not show significant effects. In the multiple linear regression model, higher confidence remained significantly associated with higher practice score (β = 0.38, p < 0.0001). Pharmacists reported higher overall practice scores compared to RN/CNS (β = 0.52, 95% CI = (0.16–0.88), p = 0.0052) and a trend toward higher scores compared to MD/NP (β = 0.35, 95% CI = (−0.01–0.71), p = 0.06).
4. Discussion
Increasingly, evidence suggests that patients with cancer might be at higher risk of NMOU and opioid-related harm than was previously thought [
5,
6,
7,
13]. However, there is limited understanding of how well-equipped oncology professionals are in recognizing, mitigating and managing these behaviors and associated risks.
Our results show that over one third of participants agreed that patients with cancer are at very low risk for opioid-related harms. This is raises concern that the belief that opioid-related harms are low in cancer population remains persistent, despite a paucity of supporting research [
3,
4]. Almost half of participants endorsed a lack of confidence in recognizing OUD in their patients with cancer. These results suggest that this under-recognition of OUD may be due to knowledge and practice gaps among oncology clinicians [
5].
Participants in this study endorsed overall limited confidence in opioid management and risk mitigation practices, as well as limited and varied opioid safety practices. Participants infrequently engaged in safety practices such as screening, structured prescribing, pill counts, urine drug screens, overdose education, and naloxone education. This is not surprising given there are limited evidence-based recommendations for safer opioid prescribing in patients with cancer related pain [
13].
Over 25% of participants reported never educating patients on safe opioid storage and disposal (
Figure 1). A study by Reddy et al. found that 74% of adult cancer outpatients receiving opioids were unaware of proper opioid disposal methods, and that 46% have unused opioids at home [
16]. Based on our results, we suspect that a lack of clinician education regarding safe storage and disposal is likely contributing to these unsafe conditions, which may lead to diversion, accidental overdose and death. Pharmacists demonstrated overall higher average practice scores, which may be due to the standardization of their medication safety education and practices and an integration with patient care at the time of opioid dispensing.
There are multiple limitations of this study. The sample size was small and from a single, tertiary cancer center. Dissemination of the survey via email, and the lack of an incentive to complete the survey, may have contributed to the poor response rate. Participants were mostly MDs and RNs with a smaller number of pharmacists. As such, our results may not be generalizable to a nonspecialist setting.
5. Conclusions
This study suggests that attitudes, confidence and practices around opioid safety in patients with cancer seem to widely vary between oncology care professionals. Overall, confidence in managing and mitigating risk of opioids appears to be low and safety practices, infrequent. This raises concern that there may be gaps in knowledge, education and training of oncology clinicians in the area of opioid safety for this unique patient population. This study provides us insight into these gaps that may be contributing to unsafe opioid prescribing, uncontrolled cancer pain, under-recognition of NMOU and OUD, and unnecessary risk. There is an urgent need for research, guidelines, and educational tools aimed at effectively and sustainably closing these gaps in order to minimize opioid-related harm while optimally managing symptoms and quality of life in patients with cancer. Larger, multicenter studies are needed to confirm our findings and inform future work in this area.
Author Contributions
Conceptualization, methodology and validation, A.T., J.B., B.H., L.H., J.L.; formal analysis, A.T., J.L.; investigation, A.T., J.L.; data curation, A.T.; writing—original draft preparation, A.T.; writing—review and editing, A.T., J.B., B.H., L.H., J.L.; supervision, J.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
The authors would like to thank Shiyi Chen and Nadia Swami for their contributions to this study. The abstract of this study has been presented and published at the XVIII Symposium of the International Society of Oncology Pharmacy Practitioners, 10–13 October 2019 in London, UK.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Government of Canada. Opioid Related Harms in Canada. Available online: https://health-infobase.canada.ca/substance-related-harms/opioids/maps (accessed on 1 September 2020).
- National Pain Center Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Available online: http://nationalpaincentre.mcmaster.ca/documents/Opioid%20GL%20for%20CMAJ_01may2017.pdf (accessed on 10 May 2020).
- Leung, P.T.M.; Macdonald, E.M.; Stanbrook, M.B.; Dhalla, I.A.; Juurlink, D. A 1980 Letter on the Risk of Opioid Addiction. N. Engl. J. Med. 2017, 376, 2194–2195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knaul, F.M.; Farmer, P.E.; Krakauer, E.L.; De Lima, L.; Bhadelia, A.; Kwete, X.J.; Arreola-Ornelas, H.; Gómez-Dantés, O.; Rodriquez, N.M.; Alleyne, G.O.A.; et al. The Lancet Commissions Alleviating the access abyss in palliative care and pain relief—An imperative of universal health coverage: the Lancet Commission report. Lancet 2017, 39, 1391–1454. [Google Scholar] [CrossRef]
- Carmichael, A.N.; Morgan, L.; Del Fabbro, E. Identifying and assessing the risk of opioid abuse in patients with cancer: an integrative review. Subst. Abuse Rehabil. 2016, 7, 71–79. [Google Scholar] [PubMed] [Green Version]
- Arthur, J.A.; Edwards, T.; Lu, Z.; Reddy, S.; Hui, D.; Wu, J.; Liu, D.; Williams, J.L.; Brurera, E. Frequency, predictors, and outcomes of urine drug testing among patients with advanced cancer on chronic opioid therapy at an outpatient supportive care clinic. Cancer 2016, 122, 3732–3739. [Google Scholar] [CrossRef] [PubMed]
- Rauenzahn, S.; Sima, A.; Cassel, B.; Noreika, D.; Gomez, T.H.; Ryan, L.; Wolf, C.E.; Legakis, L.; Del Fabbro, E. Urine drug screen findings among ambulatory oncology patients in a supportive care clinic. Support. Care Cancer 2017, 25, 1859–1864. [Google Scholar] [CrossRef] [PubMed]
- American Society of Clinical Oncology (ASCO) Policy Statement on Opioid Therapy: Protecting Access to Treatment for Cancer-Related Pain. Available online: https://www.asco.org/sites/new-www.asco.org/files/2016-ASCO-Policy-Statement-Opioid-Therapy.pdf (accessed on 26 September 2020).
- Paice, J.A.; Portenoy, R.; Lachetti, C.; Campbell, T.; Cheville, A.; Citron, M.; Costine, L.S.; Cooper, A.; Glare, P.; Keefe, F.; et al. Management of Chronic Pain in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2016, 34, 3325–3345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passik, S.D.; Portenoy, R.K.; Ricketts, P.L. Substance abuse issues in cancer patients. Part 2: Evaluation and treatment. Oncology 1998, 12, 517–521. [Google Scholar] [PubMed]
- Blackhall, L.J.; Alfson, E.D.; Barclay, J.S. Screening for substance abuse and diversion in Virginia hospices. J. Palliat. Med. 2013, 16, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Kirsh, K.L.; Passik, S. Palliative Care of the Terminally Ill Drug Addict. Cancer Investig. 2006, 24, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Arthur, J.; Brurera, E. Balancing opioid analgesia with the risk of nonmedical opioid use in patients with cancer. Nat. Rev. Clin. Oncol. 2019, 16, 213–226. [Google Scholar] [CrossRef]
- World Health Organization: International Agency for Research on Cancer Global Cancer Observatory. Available online: https://gco.iarc.fr (accessed on 1 October 2020).
- Ferrell, B.R.; Temel, J.S.; Temin, S.; Alesi, E.R.; Balboni, T.A.; Basch, E.M.; Firn, J.I.; Paice, J.A.; Peppercorn, J.M.; Phillips, T.; et al. Integration of Palliative Care Into Standard Oncology Care: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2017, 35, 96–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddy, A.; de la Cruz, M.; Rodriguez, E.M.; Thames, J.; Wu, J.; Chrisholm, G.; Liu, D.; Frisbee-Hume, S.; Yennurajalingam, S.; Hui, D.; et al. Patterns of Storage, Use, and Disposal of Opioids Among Cancer Outpatients. Oncologist 2014, 19, 780–785. [Google Scholar] [CrossRef] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



{kind=link}