Omental Macrophagic “Crown-like Structures” Are Associated with Poor Prognosis in Advanced-Stage Serous Ovarian Cancer

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Enrollment
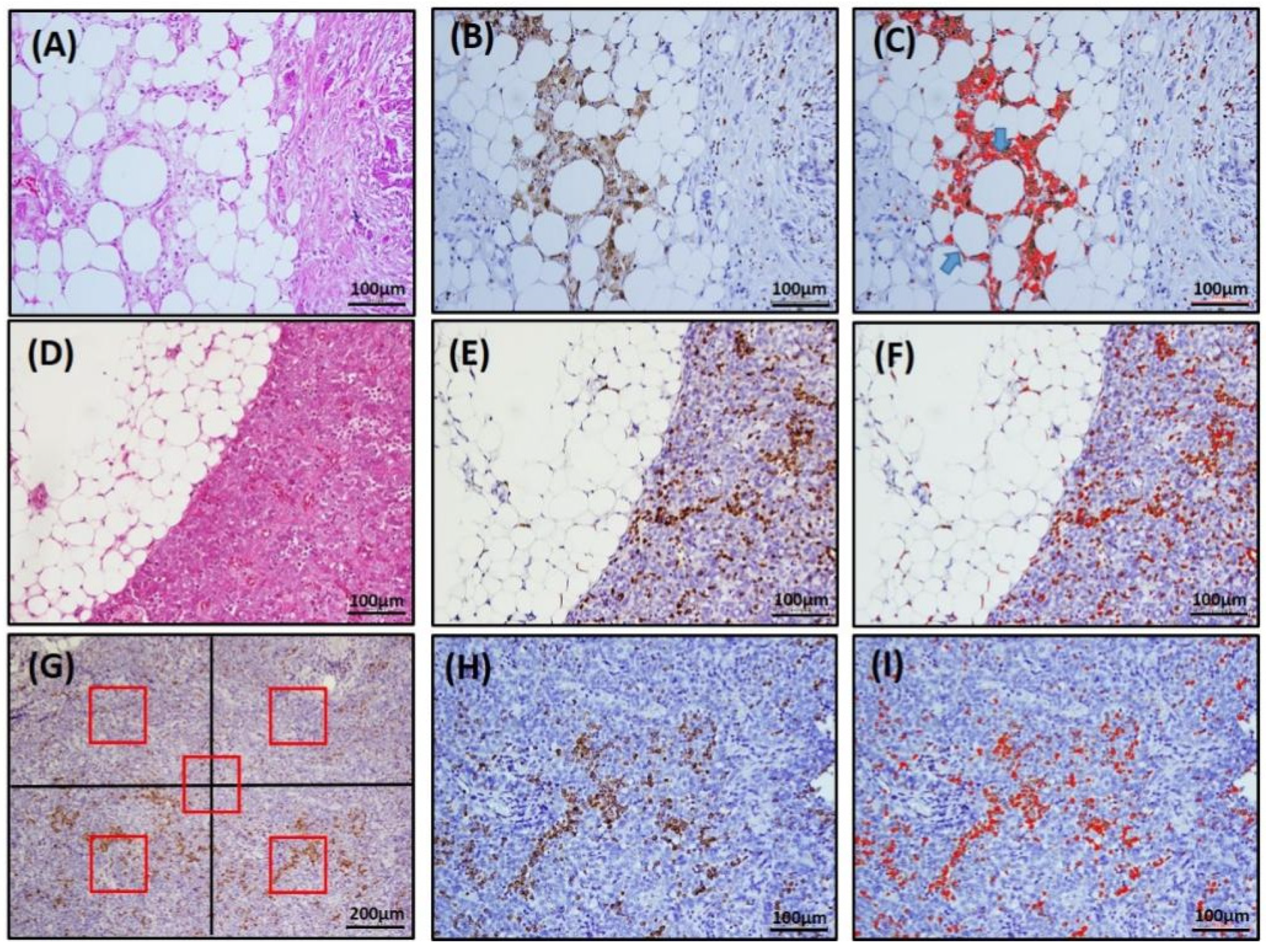
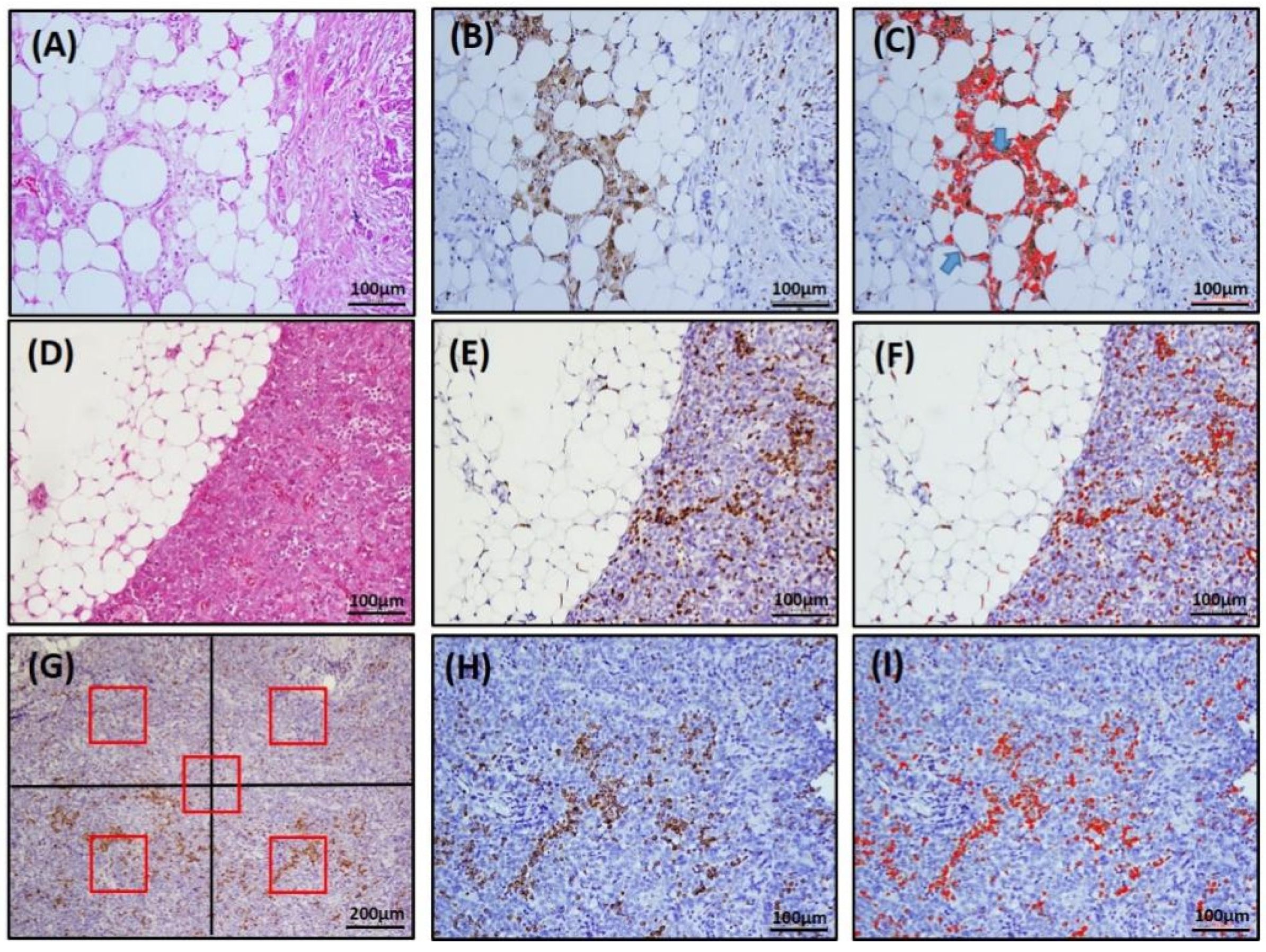
2.2. Immunohistochemistry and TAM, CLS Assessment
3. Statistical Analyses
4. Results
4.1. Patient Characteristics
4.2. The Number of Omental CD68+ Clss Had a Strongly Positive Correlation with Omental CD163+ CLS; Density of CD68+ om-TAMs Had a Strong Positive Correlation with the Density of CD163+ om-TAMs
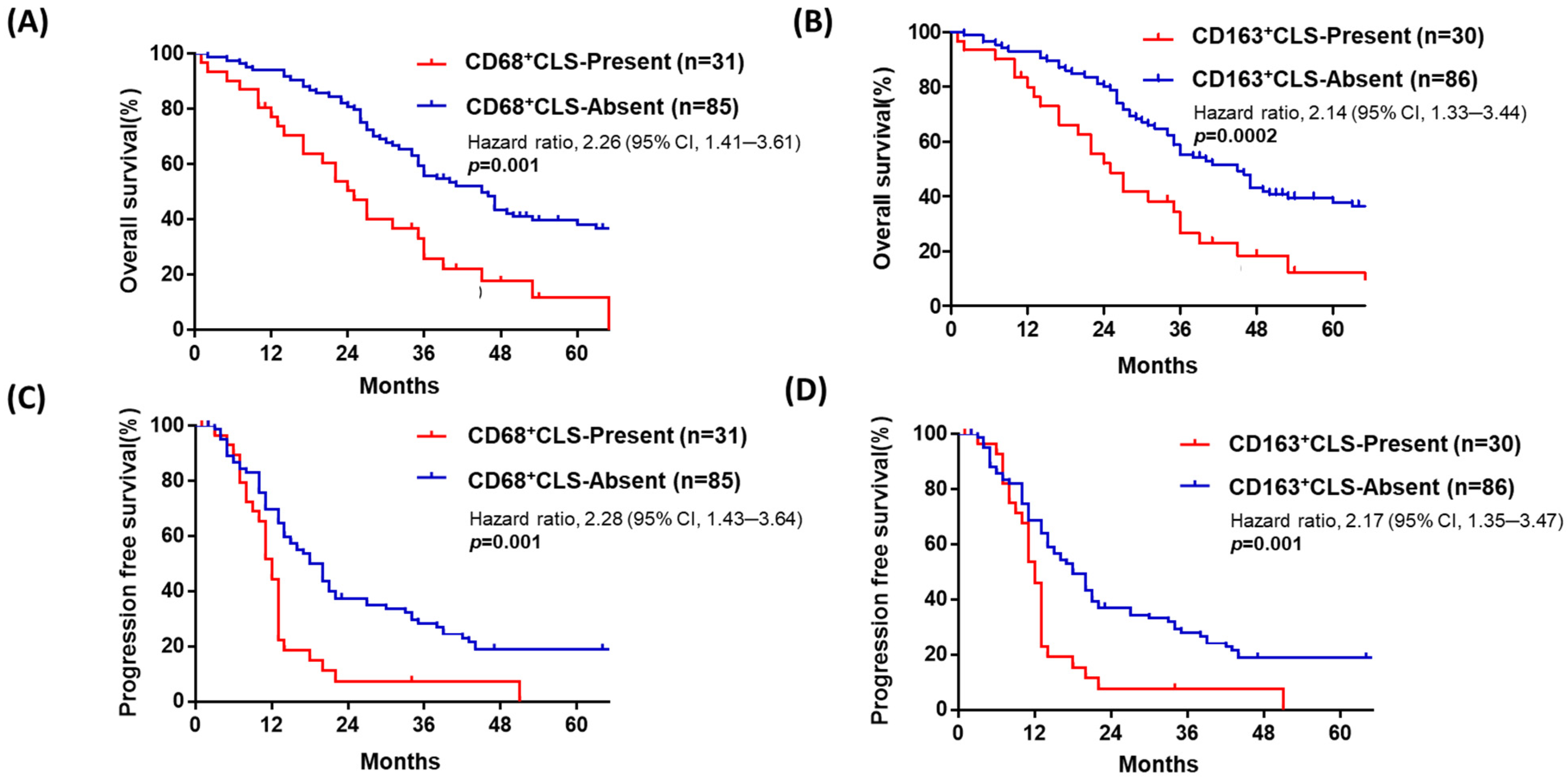
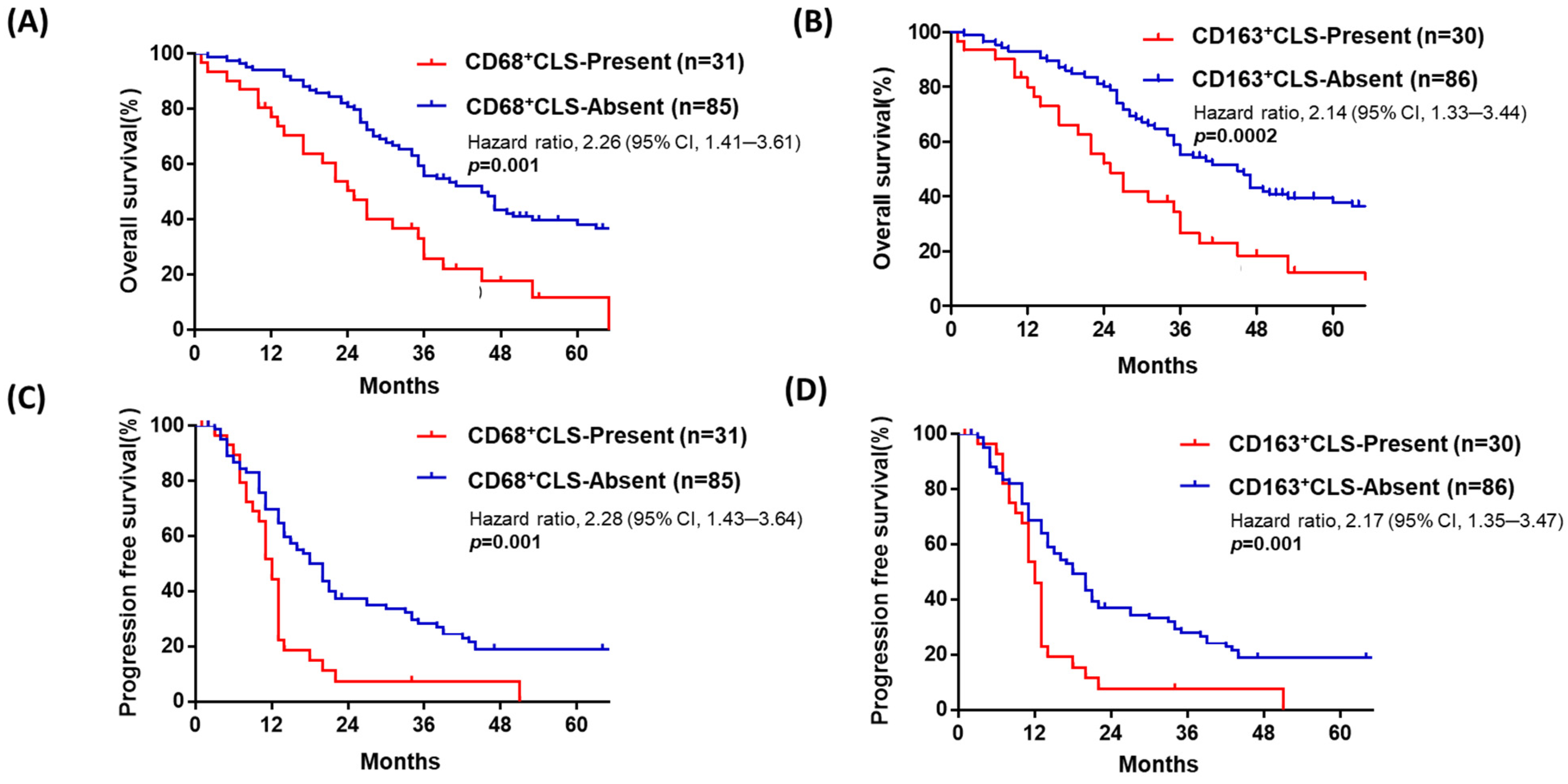
4.3. Advanced-Stage HGSOC with Omental CD68+ or CD163+ CLSs Is Associated with Poor Prognosis
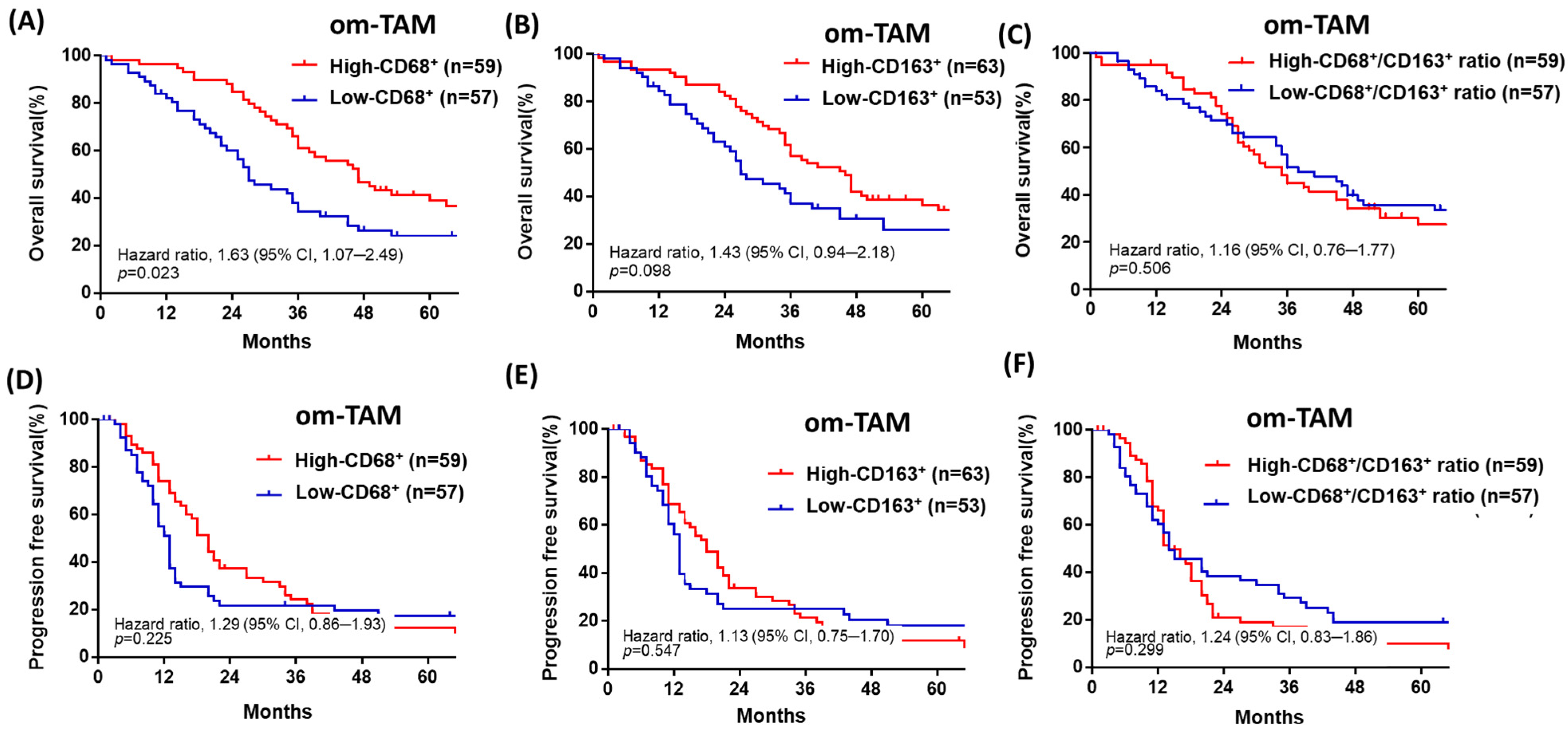
4.4. Patients with Advanced-Stage HGSOC with a Low Density of Omental CD68+ or CD163+ om-TAMs Have Poor OS, though the Ovarian Tumor Density of CD68+ or CD163+ ov-TAMs Is Not Associated with Patient Prognosis
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mantovani, A.; Marchesi, F.; Malesci, A.; Laghi, L.; Allavena, P. Tumour-associated macrophages as treatment targets in oncology. Nat. Rev. Clin. Oncol 2017, 14, 399–416. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, L.; Pollard, J.W. Targeting macrophages: Therapeutic approaches in cancer. Nat. Rev. Drug Discov. 2018, 17, 887–904. [Google Scholar] [CrossRef]
- Zhang, Q.W.; Liu, L.; Gong, C.Y.; Shi, H.S.; Zeng, Y.H.; Wang, X.Z.; Zhao, Y.W.; Wei, Y.Q. Prognostic significance of tumor-associated macrophages in solid tumor: A meta-analysis of the literature. PLoS ONE 2012, 7, e50946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruffell, B.; Coussens, L.M. Macrophages and therapeutic resistance in cancer. Cancer Cell 2015, 27, 462–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kübler, K.; Ayub, T.H.; Weber, S.K.; Zivanovic, O.; Abramian, A.; Keyver-Paik, M.D.; Mallmann, M.R.; Kaiser, C.; Serçe, N.B.; Kuhn, W.; et al. Prognostic significance of tumor-associated macrophages in endometrial adenocarcinoma. Gynecol. Oncol. 2014, 135, 176–183. [Google Scholar] [CrossRef]
- Forssell, J.; Oberg, A.; Henriksson, M.L.; Stenling, R.; Jung, A.; Palmqvist, R. High macrophage infiltration along the tumor front correlates with improved survival in colon cancer. Clin. Cancer Res. 2007, 13, 1472–1479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malesci, A.; Bianchi, P.; Celesti, G.; Basso, G.; Marchesi, F.; Grizzi, F.; Di Caro, G.; Cavalleri, T.; Rimassa, L.; Palmqvist, R.; et al. Tumor-associated macrophages and response to 5-fluorouracil adjuvant therapy in stage III colorectal cancer. Oncoimmunology 2017, 6, e1342918. [Google Scholar] [CrossRef]
- Yin, S.; Huang, J.; Li, Z.; Zhang, J.; Luo, J.; Lu, C.; Xu, H.; Xu, H. The Prognostic and Clinicopathological Significance of Tumor-Associated Macrophages in Patients with Gastric Cancer: A Meta-Analysis. PLoS ONE 2017, 12, e0170042. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.N.; Wang, C.J.; Chao, Y.J.; Lai, M.D.; Shan, Y.S. The significance of the co-existence of osteopontin and tumor-associated macrophages in gastric cancer progression. BMC Cancer 2015, 15, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; He, Y.; Sun, X.; Li, Q.; Wang, W.; Zhao, A.; Di, W. A high M1/M2 ratio of tumor-associated macrophages is associated with extended survival in ovarian cancer patients. J. Ovarian Res. 2014, 7, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, X.; Zhang, J.; Li, D.; Mao, Y.; Mo, F.; Du, W.; Ma, X. Prognostic significance of tumor-associated macrophages in ovarian cancer: A meta-analysis. Gynecol. Oncol. 2017, 147, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Shah, C.A.; Allison, K.H.; Garcia, R.L.; Gray, H.J.; Goff, B.A.; Swisher, E.M. Intratumoral T cells, tumor-associated macrophages, and regulatory T cells: Association with p53 mutations, circulating tumor DNA and survival in women with ovarian cancer. Gynecol. Oncol. 2008, 109, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Ojalvo, L.S.; Thompson, E.D.; Wang, T.L.; Meeker, A.K.; Shih, I.M.; Fader, A.N.; Cimino-Mathews, A.; Emens, L.A. Tumor-associated macrophages and the tumor immune microenvironment of primary and recurrent epithelial ovarian cancer. Hum. Pathol. 2018, 74, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available online: https://gco.iarc.fr/today (accessed on 25 May 2021).
- Lengyel, E. Ovarian cancer development and metastasis. Am. J. Pathol. 2010, 177, 1053–1064. [Google Scholar] [CrossRef] [PubMed]
- Sehouli, J.; Senyuva, F.; Fotopoulou, C.; Neumann, U.; Denkert, C.; Werner, L.; Gülten, O.O. Intra-abdominal tumor dissemination pattern and surgical outcome in 214 patients with primary ovarian cancer. J. Surg. Oncol. 2009, 99, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Meza-Perez, S.; Randall, T.D. Immunological Functions of the Omentum. Trends. Immunol. 2017, 38, 526–536. [Google Scholar] [CrossRef]
- Pearce, O.; Delaine-Smith, R.M.; Maniati, E.; Nichols, S.; Wang, J.; Böhm, S.; Rajeeve, V.; Ullah, D.; Chakravarty, P.; Jones, R.R.; et al. Deconstruction of a Metastatic Tumor Microenvironment Reveals a Common Matrix Response in Human Cancers. Cancer Discov. 2018, 8, 304–319. [Google Scholar] [CrossRef] [Green Version]
- Nieman, K.M.; Kenny, H.A.; Penicka, C.V.; Ladanyi, A.; Buell-Gutbrod, R.; Zillhardt, M.R.; Romero, I.L.; Carey, M.S.; Mills, G.B.; Hotamisligil, G.S.; et al. Adipocytes promote ovarian cancer metastasis and provide energy for rapid tumor growth. Nat. Med. 2011, 17, 1498–1503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieman, K.M.; Romero, I.L.; Van Houten, B.; Lengyel, E. Adipose tissue and adipocytes support tumorigenesis and metastasis. Biochim. Biophys. Acta. 2013, 1831, 1533–1541. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.; Cha, Y.J.; Koo, J.S. Adipocyte biology in breast cancer: From silent bystander to active facilitator. Prog. Lipid. Res. 2018, 69, 11–20. [Google Scholar] [CrossRef]
- Corrêa, L.H.; Corrêa, R.; Farinasso, C.M.; de Sant’Ana Dourado, L.P.; Magalhães, K.G. Adipocytes and Macrophages Interplay in the Orchestration of Tumor Microenvironment: New Implications in Cancer Progression. Front. Immunol. 2017, 8, 1129. [Google Scholar] [CrossRef]
- Weisberg, S.P.; McCann, D.; Desai, M.; Rosenbaum, M.; Leibel, R.L.; Ferrante, A.W., Jr. Obesity is associated with macrophage accumulation in adipose tissue. J. Clin. Invest. 2003, 112, 1796–1808. [Google Scholar] [CrossRef] [PubMed]
- Murano, I.; Barbatelli, G.; Parisani, V.; Latini, C.; Muzzonigro, G.; Castellucci, M.; Cinti, S. Dead adipocytes, detected as crown-like structures, are prevalent in visceral fat depots of genetically obese mice. J. Lipid. Res. 2008, 49, 1562–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, Y.E.; Kim, J.M.; Joung, K.H.; Lee, J.H.; You, B.R.; Choi, M.J.; Ryu, M.J.; Ko, Y.B.; Lee, M.A.; Lee, J.; et al. The Roles of Adipokines, Proinflammatory Cytokines, and Adipose Tissue Macrophages in Obesity-Associated Insulin Resistance in Modest Obesity and Early Metabolic Dysfunction. PLoS ONE 2016, 11, e0154003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, N.M.; Zhou, X.K.; Gucalp, A.; Morris, P.G.; Howe, L.R.; Giri, D.D.; Morrow, M.; Wang, H.; Pollak, M.; Jones, L.W.; et al. Systemic Correlates of White Adipose Tissue Inflammation in Early-Stage Breast Cancer. Clin. Cancer Res. 2016, 22, 2283–2289. [Google Scholar] [CrossRef] [Green Version]
- Koru-Sengul, T.; Santander, A.M.; Miao, F.; Sanchez, L.G.; Jorda, M.; Glück, S.; Ince, T.A.; Nadji, M.; Chen, Z.; Penichet, M.L.; et al. Breast cancers from black women exhibit higher numbers of immunosuppressive macrophages with proliferative activity and of crown-like structures associated with lower survival compared to non-black Latinas and Caucasians. Breast Cancer Res. Treat. 2016, 158, 113–126. [Google Scholar] [CrossRef]
- Carter, J.M.; Hoskin, T.L.; Pena, M.A.; Brahmbhatt, R.; Winham, S.J.; Frost, M.H.; Stallings-Mann, M.; Radisky, D.C.; Knutson, K.L.; Visscher, D.W.; et al. Macrophagic "Crown-like Structures" Are Associated with an Increased Risk of Breast Cancer in Benign Breast Disease. Cancer Prev. Res. 2018, 11, 113–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faria, S.S.; Corrêa, L.H.; Heyn, G.S.; de Sant’Ana, L.P.; Almeida, R.; Magalhães, K.G. Obesity and Breast Cancer: The Role of Crown-Like Structures in Breast Adipose Tissue in Tumor Progression, Prognosis, and Therapy. J. Breast Cancer 2020, 23, 233–245. [Google Scholar] [CrossRef]
- Iyengar, N.M.; Ghossein, R.A.; Morris, L.G.; Zhou, X.K.; Kochhar, A.; Morris, P.G.; Pfister, D.G.; Patel, S.G.; Boyle, J.O.; Hudis, C.A.; et al. White adipose tissue inflammation and cancer-specific survival in patients with squamous cell carcinoma of the oral tongue. Cancer 2016, 122, 3794–3802. [Google Scholar] [CrossRef] [Green Version]
- Gucalp, A.; Iyengar, N.M.; Zhou, X.K.; Giri, D.D.; Falcone, D.J.; Wang, H.; Williams, S.; Krasne, M.D.; Yaghnam, I.; Kunzel, B.; et al. Periprostatic adipose inflammation is associated with high-grade prostate cancer. Prostate Cancer Prostatic. Dis. 2017, 20, 418–423. [Google Scholar] [CrossRef]
- Itoh, M.; Suganami, T.; Kato, H.; Kanai, S.; Shirakawa, I.; Sakai, T.; Goto, T.; Asakawa, M.; Hidaka, I.; Sakugawa, H.; et al. CD11c+ resident macrophages drive hepatocyte death-triggered liver fibrosis in a murine model of nonalcoholic steatohepatitis. JCI Insight 2017, 2, e92902. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Rustin, G.J.; Vergote, I.; Eisenhauer, E.; Pujade-Lauraine, E.; Quinn, M.; Thigpen, T.; du Bois, A.; Kristensen, G.; Jakobsen, A.; Sagae, S.; et al. Definitions for response and progression in ovarian cancer clinical trials incorporating RECIST 1.1 and CA 125 agreed by the Gynecological Cancer Intergroup (GCIG). Int. J. Gynecol. Cancer 2012, 21, 419–423. [Google Scholar] [CrossRef]
- Hsu, K.F.; Shen, M.R.; Huang, Y.F.; Cheng, Y.M.; Lin, S.H.; Chow, N.H.; Cheng, S.W.; Chou, C.Y.; Ho, C.L. Overexpression of the RNA-binding proteins Lin28B and IGF2BP3 (IMP3) is associated with chemoresistance and poor disease outcome in ovarian cancer. Br. J. Cancer 2015, 113, 414–424. [Google Scholar] [CrossRef]
- Quail, D.F.; Dannenberg, A.J. The obese adipose tissue microenvironment in cancer development and progression. Nat. Rev. Endocrinol. 2019, 15, 139–154. [Google Scholar] [CrossRef] [PubMed]
- Cha, Y.J.; Kim, E.S.; Koo, J.S. Tumor-associated macrophages and crown-like structures in adipose tissue in breast cancer. Breast Cancer Res. Treat. 2018, 170, 15–25. [Google Scholar] [CrossRef]
- Liang, Y.L.; Wu, C.H.; Kang, C.Y.; Lin, C.N.; Shih, N.Y.; Lin, S.H.; Chen, Y.C.; Hsu, K.F. Downregulated Salt-inducible Kinase 3 Expression Promotes Chemoresistance in Serous Ovarian Cancer via the ATP-binding Cassette Protein ABCG2. J. Cancer 2019, 10, 6025–6036. [Google Scholar] [CrossRef] [PubMed]
- Jing, Y.; Liu, J.; Ye, Y.; Pan, L.; Deng, H.; Wang, Y.; Yang, Y.; Diao, L.; Lin, S.H.; Mills, G.B.; et al. Multiomics prediction of immune-related adverse events during checkpoint immunotherapy. Nat. Commun. 2020, 11, 4946. [Google Scholar] [CrossRef] [PubMed]
- Maliniak, M.L.; Cheriyan, A.M.; Sherman, M.E.; Liu, Y.; Gogineni, K.; Liu, J.; He, J.; Krishnamurti, U.; Miller-Kleinhenz, J.; Ashiqueali, R.; et al. Detection of crown-like structures in breast adipose tissue and clinical outcomes among African-American and White women with breast cancer. Breast Cancer Res. 2020, 22, 65. [Google Scholar] [CrossRef]
- Reinartz, S.; Schumann, T.; Finkernagel, F.; Wortmann, A.; Jansen, J.M.; Meissner, W.; Krause, M.; Schwörer, A.M.; Wagner, U.; Müller-Brüsselbach, S.; et al. Mixed-polarization phenotype of ascites-associated macrophages in human ovarian carcinoma: Correlation of CD163 expression, cytokine levels and early relapse. Int. J. Cancer 2014, 134, 32–42. [Google Scholar] [CrossRef]
- Yang, J.; Zaman, M.M.; Vlasakov, I.; Roy, R.; Huang, L.; Martin, C.R.; Freedman, S.D.; Serhan, C.N.; Moses, M.A. Adipocytes promote ovarian cancer chemoresistance. Sci. Rep. 2019, 9, 13316. [Google Scholar] [CrossRef] [Green Version]
- Macciò, A.; Madeddu, C. Inflammation and ovarian cancer. Cytokine 2012, 58, 133–147. [Google Scholar] [CrossRef] [Green Version]
- Flaherty, S.E., 3rd; Grijalva, A.; Xu, X.; Ables, E.; Nomani, A.; Ferrante, A.W., Jr. A lipase-independent pathway of lipid release and immune modulation by adipocytes. Science 2019, 363, 989–993. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Yang, M.; Huang, W.; Chen, W.; Zhao, Y.; Schulte, M.L.; Volberding, P.; Gerbec, Z.; Zimmermann, M.T.; Zeighami, A.; et al. Mitochondrial Metabolic Reprogramming by CD36 Signaling Drives Macrophage Inflammatory Responses. Circ. Res. 2019, 125, 1087–1102. [Google Scholar] [CrossRef]
- Xu, Z.Z.; Xu, S.; Kuhlmann, A.; Kaech, S.M. The role of CD36 in macrophage lipid metabolism and function in tumor microenvironment. J. Immunol. 2020, 204, 240.9. [Google Scholar]
- Su, P.; Wang, Q.; Bi, E.; Ma, X.; Liu, L.; Yang, M.; Qian, J.; Yi, Q. Enhanced Lipid Accumulation and Metabolism Are Required for the Differentiation and Activation of Tumor-Associated Macrophages. Cancer Res. 2020, 80, 1438–1450. [Google Scholar] [CrossRef]
- Rabold, K.; Aschenbrenner, A.; Thiele, C.; Boahen, C.K.; Schiltmans, A.; Smit, J.; Schultze, J.L.; Netea, M.G.; Adema, G.J.; Netea-Maier, R.T. Enhanced lipid biosynthesis in human tumor-induced macrophages contributes to their protumoral characteristics. J. Immunother. Cancer 2020, 8, e000638. [Google Scholar] [CrossRef] [PubMed]
- Tkach, M.; Théry, C. Communication by Extracellular Vesicles: Where We Are and Where We Need to Go. Cell 2016, 164, 1226–1232. [Google Scholar] [CrossRef] [Green Version]
- Vankerckhoven, A.; Wouters, R.; Mathivet, T.; Ceusters, J.; Baert, T.; Van Hoylandt, A.; Gerhardt, H.; Vergote, I.; Coosemans, A. Opposite Macrophage Polarization in Different Subsets of Ovarian Cancer: Observation from a Pilot Study. Cells 2020, 9, 305. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.; Hu, R.; Zeng, Y.; Zhang, W.; Zhou, H.H. Tumor immune cell infiltration and survival after platinum-based chemotherapy in high-grade serous ovarian cancer subtypes: A gene expression-based computational study. EBioMedicine 2020, 51, 102602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortese, N.; Carriero, R.; Laghi, L.; Mantovani, A.; Marchesi, F. Prognostic significance of tumor-associated macrophages: Past, present and future. Semin. Immunol. 2020, 48, 101408. [Google Scholar] [CrossRef] [PubMed]
- Tan, D.S.; Agarwal, R.; Kaye, S.B. Mechanisms of transcoelomic metastasis in ovarian cancer. Lancet Oncol. 2006, 7, 925–934. [Google Scholar] [CrossRef]
- Iyengar, N.M.; Brown, K.A.; Zhou, X.K.; Gucalp, A.; Subbaramaiah, K.; Giri, D.D.; Zahid, H.; Bhardwaj, P.; Wendel, N.K.; Falcone, D.J.; et al. Metabolic Obesity, Adipose Inflammation and Elevated Breast Aromatase in Women with Normal Body Mass Index. Cancer Prev. Res. 2017, 10, 235–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| CD68+ om-TAM | CD163+ om-TAM | Ratio of CD68+/CD163+ om-TAM | CD68+ CLS | CD163+ CLS | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Total | High | Low | p Value | High | Low | p Value | High | Low | p Value | Present | Absent | p value | Present | Absent | p Value |
| n= 116 | (n = 59) | (n = 57) | (n = 63) | (n = 53) | (n = 59) | (n = 57) | (n = 31) | (n = 85) | (n = 30) | (n = 86) | ||||||
| Age (y/o) | ||||||||||||||||
| Mean (range) | 57.1 (23~88) | 54.2 (23~88) | 60.1 (36~82) | 0.01 | 55.2 (23~88) | 59.2 (36~82) | 0.09 | 56.6 (30~88) | 57.5 (23~82) | 0.72 | 57.8 (30~82) | 57 (23~88) | 0.71 | 57.8 (30~82) | 56.7 (23~88) | 0.7 |
| BMI | ||||||||||||||||
| Mean (range) | 23 (15~34) | 21 (15~26) | 24 (18~34) | 0.01 | 21 (15~34) | 24 (18~34) | 0.01 | 23 (15~34) | 23 (15~31) | 0.63 | 27 (25~34) | 21 (15~25) | 0.01 | 27 (25~34) | 21 (15~27) | 0.01 |
| FIGO Stage (%) | 1 | 0.77 | 0.39 | 0.18 | 0.18 | |||||||||||
| IIIA | 4 (3) | 0 (0) | 4 (7) | 0 (0) | 4 (8) | 0 (9) | 4 (7) | 0 | 4 (5) | 0 (0) | 4 (5) | |||||
| IIIB | 17 (15) | 11 (19) | 6 (10) | 10 (16) | 7 (12) | 9 (15) | 8 (14) | 4 (13) | 13 (15) | 4 (13) | 13 (15) | |||||
| IIIC | 82 (71) | 41 (70) | 41 (72) | 45 (71) | 37 (70) | 45 (77) | 37 (65) | 26 (84) | 56 (66) | 25 (84) | 57 (66) | |||||
| IVA | 9 (8) | 5 (8) | 4 (7) | 5 (8) | 4 (8) | 3 (5) | 6 (11) | 1 (3) | 8 (9) | 1 (3) | 8 (9) | |||||
| IVB | 4 (3) | 2 (3) | 2 (4) | 3 (5) | 1 (2) | 2 (3) | 2 (3) | 0 (0) | 4 (5) | 0 (0) | 4 (5) | |||||
| Residual Disease (%) | 0.34 | 0.7 | 0.71 | 0.05 | 0.08 | |||||||||||
| Optimal (≤1 cm) | 71 (61) | 39 (66) | 32 (56) | 40 (64) | 31 (58) | 35 (59) | 36 (63) | 14 (45) | 57 (67) | 14 (47) | 57 (66) | |||||
| not-optimal (>1 cm) | 45 (39) | 20 (34) | 25 (44) | 23 (36) | 22 (42) | 24 (41) | 21 (37) | 17 (55) | 28 (33) | 16 (53) | 29 (34) | |||||
| Chemotherapy (%) | 0.002 | 0.006 | 0.44 | 0.006 | 0.006 | |||||||||||
| sensitive | 70 (60) | 45 (76) | 25 (44) | 46 (73) | 24 (45) | 38 (65) | 32 (56) | 11 (35) | 59 (70) | 11 (37) | 59 (69) | |||||
| resistant | 42 (36) | 14 (24) | 28 (49) | 16 (25) | 26 (49) | 19 (32) | 23 (40) | 17 (55) | 25 (29) | 17 (57) | 25 (29) | |||||
| No chemotherapy | 4 (4) | 0 (0) | 4 (7) | 1 (2) | 3 (6) | 2 (3) | 2 (4) | 3 (10) | 1 (1) | 2 (6) | 2 (2) | |||||
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Model 1 (CD68) a | Model 2 (CD163) b | |||||
| Variable | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value |
| Age | 1.03 (1.02–1.05) | <0.001 | 1.03 (1.01–1.05) | 0.004 | 1.03 (1.01–1.05) | 0.003 |
| FIGO Stage (Stage III vs. Stage IV) | 1.13 (0.58–2.19) | 0.727 | ||||
| Residual disease (suboptimal debulking vs. optimal debulking) | 1.65 (1.07–2.56) | 0.025 | 1.25 (0.79–1.99) | 0.346 | 1.26 (0.79–2.02) | 0.328 |
| ov-TAM (High-CD68+ vs. Low-CD68+) | 1.02 (0.67–1.55) | 0.933 | ||||
| ov-TAM (High-CD163+ vs. Low-CD163+) | 1.20 (0.79–1.83) | 0.403 | ||||
| Ratio of ov-TAM (High-CD68/CD163 vs. Low-CD68/CD163 ) | 1.32 (0.87–2.02) | 0.196 | ||||
| om-TAM (Low-CD68+ vs. High-CD68+) | 1.63 (1.07–2.49) | 0.023 | 1.07 (0.66–1.73) | 0.791 | ||
| om-TAM (Low-CD163+ vs. High-CD163+) | 1.43 (0.94–2.18) | 0.098 | 1.01 (0.62–1.64) | 0.982 | ||
| Ratio of om-TAM (Low-CD68/CD163 vs. High-CD68/CD163 ) | 1.16 (0.76–1.77) | 0.506 | ||||
| CD68+ CLS (present vs. absent) | 2.26 (1.41–3.61) | 0.001 | 2.03 (1.19–3.44) | 0.009 | ||
| CD163+ CLS (present vs. absent) | 2.14 (1.33–3.44) | 0.002 | 1.98 (1.14–3.41) | 0.015 | ||
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Model 1 (CD68) a | Model 2 (CD163) b | |||||
| Variable | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value |
| Age | 1.02 (1.01–1.04) | 0.01 | 1.01 (0.99–1.03) | 0.22 | 1.01 (0.99–1.03) | 0.22 |
| FIGO Stage (Stage III vs. Stage IV) | 1.20 (0.64–2.25) | 0.58 | ||||
| Residual disease (suboptimal debulking vs. optimal debulking) | 2.43 (1.59–3.71) | <0.001 | 1.97 (1.23–3.16) | 0.005 | 1.95 (1.21–3.15) | 0.007 |
| ov-TAM (High-CD68+ vs. Low-CD68+) | 1.17 (0.78–1.74) | 0.452 | ||||
| ov-TAM (High-CD163+ vs. Low-CD163+) | 1.23 (0.83–1.84) | 0.305 | ||||
| Ratio of ov-TAM (High-CD68/CD163 vs. Low-CD68/CD163 ) | 1.19 (0.80–1.78) | 0.392 | ||||
| om-TAM (High-CD68+ vs. Low-CD68+) | 1.29 (0.86–1.93) | 0.225 | 1.18 (0.72–1.89) | 0.522 | ||
| om-TAM (High-CD163+ vs. Low-CD163+) | 1.13 (0.75–1.70) | 0.547 | 1.19 (0.74–1.92) | 0.486 | ||
| Ratio of om-TAM (High-CD68/CD163 vs. Low-CD68/CD163) | 1.24 (0.83–1.86) | 0.299 | ||||
| CD68+ CLS (present vs. absent) | 2.28 (1.43–3.64) | 0.001 | 2.11 (1.23–3.64) | 0.007 | ||
| CD163+ CLS (present vs. absent) | 2.17 (1.35–3.47) | 0.001 | 2.02 (1.17–3.48) | 0.012 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, Y.-L.; Lin, C.-N.; Tsai, H.-F.; Wu, P.-Y.; Lin, S.-H.; Hong, T.-M.; Hsu, K.-F. Omental Macrophagic “Crown-like Structures” Are Associated with Poor Prognosis in Advanced-Stage Serous Ovarian Cancer. Curr. Oncol. 2021, 28, 4234-4246. https://doi.org/10.3390/curroncol28050359
Liang Y-L, Lin C-N, Tsai H-F, Wu P-Y, Lin S-H, Hong T-M, Hsu K-F. Omental Macrophagic “Crown-like Structures” Are Associated with Poor Prognosis in Advanced-Stage Serous Ovarian Cancer. Current Oncology. 2021; 28(5):4234-4246. https://doi.org/10.3390/curroncol28050359
Chicago/Turabian StyleLiang, Yu-Ling, Chang-Ni Lin, Hsing-Fen Tsai, Pei-Ying Wu, Sheng-Hsiang Lin, Tse-Ming Hong, and Keng-Fu Hsu. 2021. "Omental Macrophagic “Crown-like Structures” Are Associated with Poor Prognosis in Advanced-Stage Serous Ovarian Cancer" Current Oncology 28, no. 5: 4234-4246. https://doi.org/10.3390/curroncol28050359
APA StyleLiang, Y.-L., Lin, C.-N., Tsai, H.-F., Wu, P.-Y., Lin, S.-H., Hong, T.-M., & Hsu, K.-F. (2021). Omental Macrophagic “Crown-like Structures” Are Associated with Poor Prognosis in Advanced-Stage Serous Ovarian Cancer. Current Oncology, 28(5), 4234-4246. https://doi.org/10.3390/curroncol28050359