Real-World Pattern of Treatment and Clinical Outcomes of EGFR-Mutant Non-Small Cell Lung Cancer in a Single Academic Centre in Quebec


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives
- To describe the treatment patterns and outcomes including real-world progression-free survival (rwPFS), response rate (RR) and overall survival (OS) for EGFRm NSCLC patients treated at an academic centre in Montreal, Canada
- To describe demographic and clinical characteristics at diagnosis of EGFRm NSCLC patients and their prognostic value
2.2. Study Design
2.3. Patients Selection Criteria
- Patient characteristics including date of metastatic NSCLC diagnosis, stage at the time of initial diagnosis, sex, age at the time of diagnosis, ethnicity, Eastern Cooperative Oncology Group performance status (ECOG PS), smoking history.
- Tumor characteristics include the stage of the disease, presence or absence of brain metastases, and type of EGFR mutations.
- Type of molecular tests: the evolution of the EGFR test for our center is recorded as: Denaturing high-pressure liquid chromatography (DHPLC) from 2004 to 2007; single gene sequencing from 2008 to 2010; real-time polymerase chain reaction (PCR) from 2011 to 2014 and next-generation sequencing (NGS) from 2014 to current.
- Real-world treatment patterns identified in our clinical practice include comprehensive treatment history from diagnosis to current treatment, treatment duration, and modality sequencing (targeted therapy, chemotherapy, radiotherapy, and best supportive care).
2.4. Outcome Measures and Definitions
- Treatment patterns are described by line of treatment. For the purpose of this study, first-line therapy was defined as EGFR-TKI treatment commencing after the index date.
- Duration of EGFR-TKI treatment was calculated as the time (in months) elapsed between the start and end dates of the treatment.
- Response to treatment was defined by the treating physician as per RECIST criteria and was based on radiographic imaging (CT/PET) and categorized for analysis purposes as an objective response (complete response (CR) + partial response (PR), stable disease (SD) and progressive disease (PD).
- rwPFS was defined as the time between initiation of EGFR-TKI and clinician-defined progression based on RECIST [24]. In patients who were initiated with chemotherapy, but subsequently were tested positive for EGFR mutation, disease progression was calculated from the start of EGFR-TKI treatment to the date of progression on this treatment.
- OS is defined as the time from index date to the date of death or last follow-up. Patients were censored if they were lost to follow-up or the event (death) did not occur within the study duration.
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. First Line EGFR-TKI Treatment at the Time of Diagnosis of Advanced Disease
3.3. Second Line Treatment for Advanced Disease
3.4. Third Line Treatment for Advanced Disease
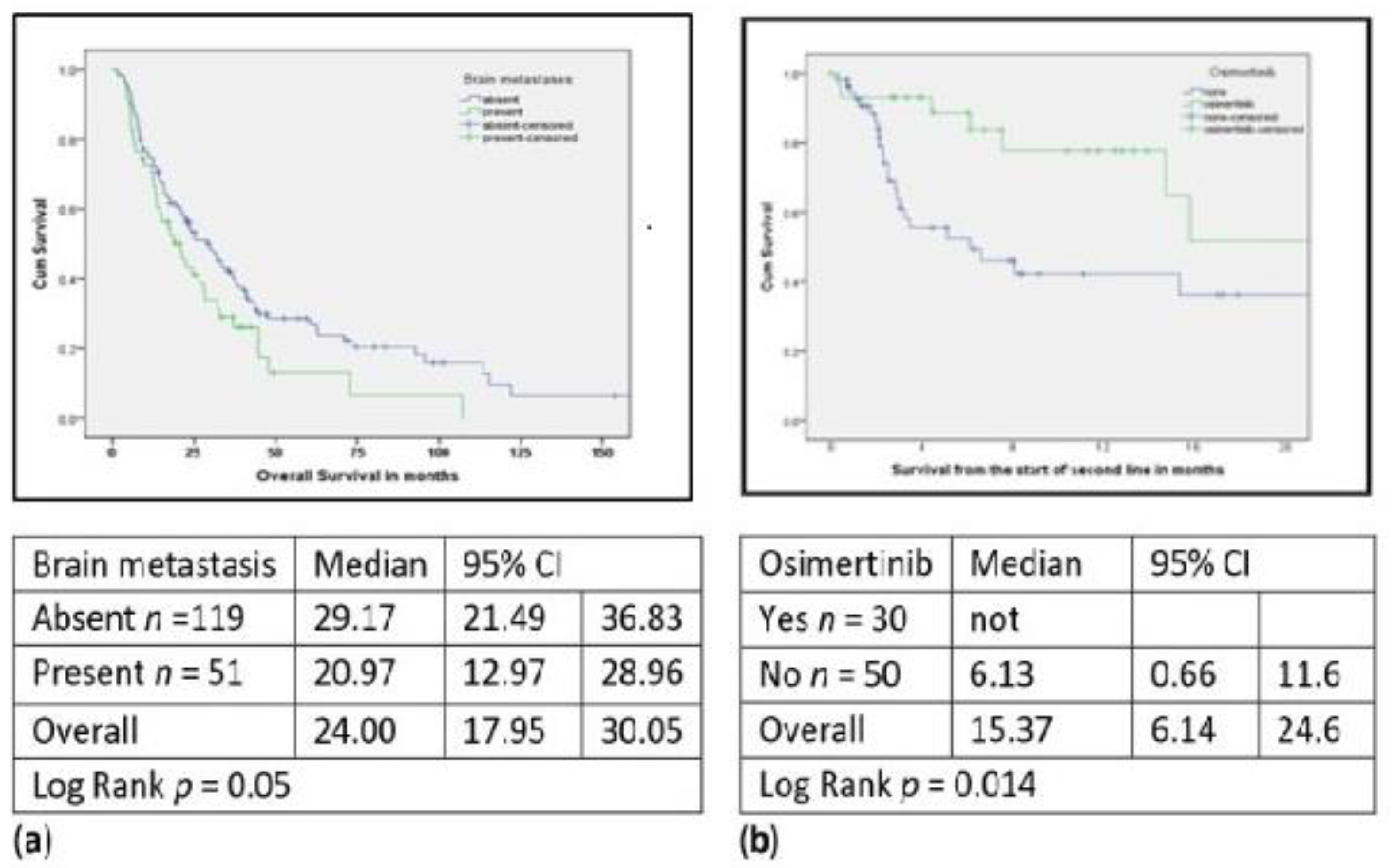
3.5. rwPFS and OS Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Cancer. Newsroom 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 10 September 2021).
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2019. 2019. Available online: https://cancer.ca/en/cancer-information/cancer-types/lung/statistics (accessed on 10 September 2019).
- Shepherd, F.A. Targeted Therapy: The New Frontier. 2019. Available online: https://meetinglibrary.asco.org/record/168046/slide (accessed on 10 September 2019).
- Kris, M.G.; Johnson, B.E.; Berry, L.D.; Kwiatkowski, D.J.; Iafrate, A.J.; Wistuba, I.I.; Varella-Garcia, M.; Franklin, W.A.; Aronson, S.L.; Su, P.-F.; et al. Using Multiplexed Assays of Oncogenic Drivers in Lung Cancers to Select Targeted Drugs. J. Am. Med. Assoc. 2014, 311, 1998–2006. Available online: https://www.ncbi.nlm.nih.gov/pubmed/24846037 (accessed on 15 August 2020). [CrossRef]
- Rosell, R.; Moran, T.; Queralt, C.; Porta, R.; Cardenal, F.; Camps, C.; Majem, M.; Lopez-Vivanco, G.; Isla, D.; Provencio, M.; et al. Screening for Epidermal Growth Factor Receptor Mutations in Lung Cancer. N. Engl. J. Med. 2009, 361, 958–967. Available online: https://www.ncbi.nlm.nih.gov/pubmed/19692684 (accessed on 15 August 2020). [CrossRef] [PubMed] [Green Version]
- Lim, C.; Tsao, M.; Le, L.W.; Shepherd, F.A.; Feld, R.; Burkes, R.L.; Liu, G.; Kamel-Reid, S.; Hwang, D.; Tanguay, J.; et al. Biomarker testing and time to treatment decision in patients with advanced nonsmall-cell lung cancer. Ann. Oncol. 2015, 26, 1415–1421. Available online: https://www.ncbi.nlm.nih.gov/pubmed/25922063 (accessed on 16 June 2020). [CrossRef] [PubMed]
- Savas, P.; Hughes, B.; Solomon, B. Targeted therapy in lung cancer: IPASS and beyond, keeping abreast of the explosion of targeted therapies for lung cancer. J. Thorac. Dis. 2013, 5 (Suppl. 5), S579–S592. Available online: https://www.ncbi.nlm.nih.gov/pubmed/24163750 (accessed on 15 September 2020). [PubMed]
- Mok, T.S.; Wu, Y.-L.; Thongprasert, S.; Yang, C.-H.; Chu, D.-T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or Carboplatin–Paclitaxel in Pulmonary Adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. Available online: https://www.ncbi.nlm.nih.gov/pubmed/19692680 (accessed on 10 September 2021). [CrossRef] [PubMed]
- Jänne, P.A.; Wang, X.; Socinski, M.A.; Crawford, J.; Stinchcombe, T.E.; Gu, L.; Capelletti, M.; Edelman, M.; Villalona-Calero, M.A.; Kratzke, R.; et al. Randomized Phase II Trial of Erlotinib Alone or With Carboplatin and Paclitaxel in Patients Who Were Never or Light Former Smokers With Advanced Lung Adenocarcinoma: CALGB 30406 Trial. J. Clin. Oncol. 2012, 30, 2063–2069. Available online: https://www.ncbi.nlm.nih.gov/pubmed/22547605 (accessed on 10 September 2021). [CrossRef] [PubMed]
- Riely, G.J.; Pao, W.; Pham, D.; Li, A.R.; Rizvi, N.; Venkatraman, E.S.; Zakowski, M.F.; Kris, M.G.; Ladanyi, M.; Miller, V.A. Clinical Course of Patients with Non–Small Cell Lung Cancer and Epidermal Growth Factor Receptor Exon 19 and Exon 21 Mutations Treated with Gefitinib or Erlotinib. Clin. Cancer Res. 2006, 12, 839–844. Available online: https://www.ncbi.nlm.nih.gov/pubmed/16467097 (accessed on 10 September 2021). [CrossRef] [PubMed] [Green Version]
- Fukuoka, M.; Wu, Y.-L.; Thongprasert, S.; Sunpaweravong, P.; Leong, S.-S.; Sriuranpong, V.; Chao, T.-Y.; Nakagawa, K.; Chu, D.-T.; Saijo, N.; et al. Biomarker Analyses and Final Overall Survival Results from a Phase III, Randomized, Open-Label, First-Line Study of Gefitinib Versus Carboplatin/Paclitaxel in Clinically Selected Patients With Advanced Non–Small-Cell Lung Cancer in Asia (IPASS). J. Clin. Oncol. 2011, 29, 2866–2874. Available online: https://www.ncbi.nlm.nih.gov/pubmed/21670455 (accessed on 10 September 2021). [CrossRef]
- Mitsudomi, T.; Morita, S.; Yatabe, Y.; Negoro, S.; Okamoto, I.; Tsurutani, J.; Seto, T.; Satouchi, M.; Tada, H.; Hirashima, T.; et al. Gefitinib versus Cisplatin Plus Docetaxel in Patients with Non-Small-Cell Lung Cancer Harbouring Mutations of the Epidermal Growth Factor Receptor (WJTOG3405): An Open Label, Randomised Phase 3 Trial. Lancet Oncol. 2010, 11, 121–128. Available online: https://www.ncbi.nlm.nih.gov/pubmed/20022809 (accessed on 10 September 2021). [CrossRef]
- Perol, M.; Chouaid, C.; Perol, D.; Barlési, F.; Gervais, R.; Westeel, V.; Crequit, J.; Léna, H.; Vergnenègre, A.; Zalcman, G.; et al. Randomized, Phase III Study of Gemcitabine or Erlotinib Maintenance Therapy versus Observation, with Predefined Second-Line Treatment, after Cisplatin-Gemcitabine Induction Chemotherapy in Advanced Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2012, 30, 3516–3524. Available online: https://www.ncbi.nlm.nih.gov/pubmed/22949150 (accessed on 10 September 2021). [CrossRef]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus Standard Chemotherapy as First-Line Treatment for European Patients with Advanced EGFR Mutation-Positive Non-Small-Cell Lung Cancer (EURTAC): A Multicentre, Open-Label, Randomised Phase 3 Trial. Lancet Oncol. 2012, 13, 239–246. Available online: https://www.ncbi.nlm.nih.gov/pubmed/22285168 (accessed on 10 September 2021). [CrossRef]
- Sequist, L.V.; Yang, J.C.-H.; Yamamoto, N.; Obyrne, K.; Hirsh, V.; Mok, T.; Geater, S.L.; Orlov, S.; Tsai, C.-M.; Boyer, M.; et al. Phase III Study of Afatinib or Cisplatin Plus Pemetrexed in Patients with Metastatic Lung Adenocarcinoma With EGFR Mutations. J. Clin. Oncol. 2013, 31, 3327–3334. Available online: https://www.ncbi.nlm.nih.gov/pubmed/23816960 (accessed on 10 September 2021). [CrossRef] [PubMed] [Green Version]
- Zhou, C.; Wu, Y.L.; Chen, G.; Feng, J.; Liu, X.Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus Chemotherapy as First-Line Treatment for Patients with Advanced EGFR Mutation-Positive Non-Small-Cell Lung Cancer (OPTIMAL, CTONG-0802): A Multicentre, Open-Label, Randomised, Phase 3 Study. Lancet Oncol. 2011, 12, 735–742. Available online: https://www.ncbi.nlm.nih.gov/pubmed/21783417 (accessed on 10 September 2021). [CrossRef]
- Wu, Y.-L.; Hirsh, V.; Sequist, L.V.; Hu, C.-P.; Feng, J.; Lu, S.; Huang, Y.; Schuler, M.; Mok, T.; Yamamoto, N.; et al. Does EGFR Mutation Type Influence Patient-Reported Outcomes in Patients with Advanced EGFR Mutation-Positive Non-Small-Cell Lung Cancer? Analysis of Two Large, Phase III Studies Comparing Afatinib with Chemotherapy (LUX-Lung 3 and LUX-Lung 6). Patient 2017, 11, 131–141. Available online: https://www.ncbi.nlm.nih.gov/pubmed/29178024 (accessed on 10 September 2021). [CrossRef] [PubMed] [Green Version]
- Hanna, N.; Johnson, D.; Temin, S.; Baker, S.; Brahmer, J.; Ellis, P.M.; Giaccone, G.; Hesketh, P.J.; Jaiyesimi, I.; Leighl, N.B.; et al. Systemic Therapy for Stage IV Non–Small-Cell Lung Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2017, 35, 3484–3515. Available online: https://www.ncbi.nlm.nih.gov/pubmed/28806116 (accessed on 10 September 2021). [CrossRef] [PubMed]
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S.; ESMO Guidelines Committee. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2017, 28 (Suppl. 4), iv1–iv21. Available online: https://www.ncbi.nlm.nih.gov/pubmed/28881918 (accessed on 10 September 2021). [CrossRef] [PubMed]
- Ramalingam, S.S.; Yang, J.C.-H.; Lee, C.K.; Kurata, T.; Kim, D.-W.; John, T.; Nogami, N.; Ohe, Y.; Mann, H.; Rukazenkov, Y.; et al. Osimertinib As First-Line Treatment of EGFR Mutation–Positive Advanced Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, 841–849. Available online: https://www.ncbi.nlm.nih.gov/pubmed/28841389 (accessed on 10 September 2021). [CrossRef] [Green Version]
- Mariano, C.; Bosdet, I.; Karsan, A.; Ionescu, D.; Murray, N.; Laskin, J.J.; Zhai, Y.; Melosky, B.; Sun, S.; Ho, C. A Population-Based Review of the Feasibility of Platinum-Based Combination Chemotherapy after Tyrosine Kinase Inhibition in EGFR Mutation Positive Non-Small Cell Lung Cancer Patients with Advanced Disease. Lung Cancer 2014, 83, 73–77. Available online: https://www.ncbi.nlm.nih.gov/pubmed/24192511 (accessed on 10 September 2021). [CrossRef]
- Law, S.C.; Chooback, N.; Cheryl, H.; Melosky, B. Outcome Differences Between First- and Second generation EGFR Inhibitors in Advanced EGFR Mutated NSCLC in a Large Population-based Cohort. Clin. Lung Cancer 2019, 20, e576–e583. Available online: https://pubmed.ncbi.nlm.nih.gov/31178389/ (accessed on 10 September 2021).
- Tudor, R.A.; D’Silva, A.; Tremblay, A.; MacEachern, P.; Morris, D.; Brenner, D.; Kopciuk, K.; Bebb, D.G. Beyond Disease-Progression: Clinical Outcomes after EGFR-TKIs in a Cohort of EGFR Mutated NSCLC Patients. PLoS ONE 2017, 12, e0181867. Available online: https://www.ncbi.nlm.nih.gov/pubmed/28777825 (accessed on 10 September 2021). [CrossRef] [PubMed] [Green Version]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; Van Oosterom, A.T.; Christian, M.C.; et al. New Guidelines to Evaluate the Response to Treatment in Solid Tumors. J. Natl. Cancer Inst. 2000, 92, 205–216. Available online: https://www.ncbi.nlm.nih.gov/pubmed/10655437 (accessed on 10 September 2021). [CrossRef] [Green Version]
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer. V7. 2019. Available online: https://www2.tri-kobe.org/nccn/guideline/lung/english/non_small.pdf (accessed on 10 September 2021).
- Soria, J.-C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. Available online: https://www.ncbi.nlm.nih.gov/pubmed/29151359 (accessed on 10 September 2021). [CrossRef]
- Zou, B.; Lee, V.H.F.; Chen, L.; Ma, L.; Wang, D.D.; Yan, H. Deciphering Mechanisms of Acquired T790M Mutation after EGFR Inhibitors for NSCLC by Computational Simulations. Sci. Rep. 2017, 7, 6595. Available online: https://www.ncbi.nlm.nih.gov/pubmed/28747773 (accessed on 10 September 2021). [CrossRef]
- Fogli, S.; Polini, B.; Del Re, M.; Petrini, I.; Passaro, A.; Crucitta, S.; Rofi, E.; Danesi, R. EGFR-TKIs in Non-Small-Cell Lung Cancer: Focus on Clinical Pharmacology and Mechanisms of Resistance. Pharmacogenomics 2018, 19, 727–740. Available online: https://www.ncbi.nlm.nih.gov/pubmed/29785875 (accessed on 10 September 2021). [CrossRef] [PubMed]
- Oxnard, G.R.; Arcila, M.E.; Sima, C.S.; Riely, G.J.; Chmielecki, J.; Kris, M.; Pao, W.; Ladanyi, M.; Miller, V.A. Acquired Resistance to EGFR Tyrosine Kinase Inhibitors in EGFR-Mutant Lung Cancer: Distinct Natural History of Patients with Tumors Harboring the T790M Mutation. Clin. Cancer Res. 2010, 17, 1616–1622. Available online: https://www.ncbi.nlm.nih.gov/pubmed/21135146 (accessed on 10 September 2021). [CrossRef] [Green Version]
- Marinis, F.; Wu, Y.L.; de Castro, G., Jr.; Chang, G.C.; Chen, Y.M.; Cho, B.C.; Freitas, H.C.; Jiang, L.; Kim, S.W.; Martin, C.; et al. ASTRIS: A Global Real-World Study of Osimertinib in >3000 Patients with EGFR T790M Positive Non-Small-Cell Lung Cancer. Future Oncol. 2019, 15, 3003–3014. Available online: https://www.ncbi.nlm.nih.gov/pubmed/31339357 (accessed on 10 September 2021). [CrossRef]
- Mok, T.S.; Wu, Y.L.; Ahn, M.J.; Garassino, M.C.; Kim, H.R.; Ramalingam, S.S.; Shepherd, F.A.; He, Y.; Akamatsu, H.; Theelen, W.M.S.E.; et al. Osimertinib or Platinum-Pemetrexed in EGFR T790M-Positive Lung Cancer. N. Engl. J. Med. 2017, 376, 629–640. Available online: https://www.ncbi.nlm.nih.gov/pubmed/27959700 (accessed on 10 September 2021). [CrossRef] [PubMed] [Green Version]
- Rossi, A.; Di Maio, M. LUX-Lung: Determining the Best EGFR Inhibitor in NSCLC? Lancet Oncol. 2015, 16, 118–119. Available online: https://www.ncbi.nlm.nih.gov/pubmed/25589190 (accessed on 10 September 2021). [CrossRef]
- Ahn, M.-J.; Tsai, C.-M.; Shepherd, F.A.; Bazhenova, L.; Sequist, L.V.; Hida, T.; Yang, J.C.H.; Ramalingam, S.S.; Mitsudomi, T.; Jänne, P.A.; et al. Osimertinib in Patients with T790M Mutation-Positive, Advanced Non–Small Cell Lung Cancer: Long-Term Follow-Up from a Pooled Analysis of 2 Phase 2 Studies. Cancer 2019, 125, 892–901. Available online: https://www.ncbi.nlm.nih.gov/pubmed/30512189 (accessed on 10 September 2021). [CrossRef]
- Seung, S.; Hurry, M.; Walton, R.; Evans, W. Real-World Treatment Patterns and Survival in Stage IV Non-Small-Cell Lung Cancer in Canada. Curr. Oncol. 2020, 27, 361–367. Available online: https://www.ncbi.nlm.nih.gov/pubmed/32905294 (accessed on 10 September 2021). [CrossRef] [PubMed]
- Hotta, K.; Suzuki, E.; Di Maio, M.; Chiodini, P.; Fujiwara, Y.; Takigawa, N.; Ichihara, E.; Reck, M.; Manegold, C.; Pilz, L.; et al. Progression-Free Survival and Overall Survival in Phase III Trials of Molecular-Targeted Agents in Advanced Non-Small-Cell Lung Cancer. Lung Cancer 2013, 79, 20–26. Available online: https://www.ncbi.nlm.nih.gov/pubmed/23164554 (accessed on 10 September 2021). [CrossRef] [PubMed]
- Yang, J.J.; Zhou, Q.; Yan, H.H.; Zhang, X.C.; Chen, H.J.; Tu, H.Y.; Wang, Z.; Xu, C.R.; Su, J.; Wang, B.C.; et al. A phase III Randomised Controlled Trial of Erlotinib vs Gefitinib in Advanced Non-Small Cell Lung Cancer with EGFR Mutations. Br. J. Cancer 2017, 116, 568–574. Available online: https://www.ncbi.nlm.nih.gov/pubmed/28103612 (accessed on 10 September 2021). [CrossRef] [PubMed] [Green Version]
- Yusuf, D.; Walton, R.N.; Hurry, M.; Farrer, C.; Bebb, D.G.; Cheung, W.Y. Population-Based Treatment Patterns and Outcomes for Stage III Non-Small Cell Lung Cancer Patients: A Real-World Evidence Study. Am. J. Clin. Oncol. 2020, 43, 615–620. Available online: https://www.ncbi.nlm.nih.gov/pubmed/32889830 (accessed on 10 September 2021). [CrossRef]
- Li, J.; Qu, L.; Wei, X.; Gao, H.; Wang, W.; Qin, H.; Tang, C.; Guo, W.; Wang, H.; Liu, X. Clinical observation of EGFR-TKI as a First-Line Therapy on Advanced Non-Small Cell Lung Cancer. Zhongguo Fei Ai Za Zhi 2012, 15, 299–304. Available online: https://www.ncbi.nlm.nih.gov/pubmed/22613337 (accessed on 10 September 2021). [PubMed]
- Fujita, Y.; Kinoshita, M.; Ozaki, T.; Takano, K.; Kunimasa, K.; Kimura, M.; Inoue, T.; Tamiya, M.; Nishino, K.; Kumagai, T.; et al. The Impact of EGFR Mutation Status and Single Brain Metastasis on the Survival of Non-Small-Cell Lung Cancer Patients with Brain Metastases. Neuro-Oncol. Adv. 2020, 2, vdaa064. Available online: https://www.ncbi.nlm.nih.gov/pubmed/32642715 (accessed on 10 September 2021). [CrossRef] [PubMed]
- Park, K.; Tan, E.-H.; O’Byrne, K.; Zhang, L.; Boyer, M.; Mok, T.; Hirsh, V.; Yang, J.C.-H.; Lee, K.H.; Lu, S.; et al. Afatinib versus Gefitinib as First-Line Treatment of Patients with EGFR Mutation-Positive Non-Small-Cell Lung Cancer (LUX-Lung 7): A Phase 2B, Open-Label, Randomised Controlled Trial. Lancet Oncol. 2016, 17, 577–589. Available online: https://www.ncbi.nlm.nih.gov/pubmed/27083334 (accessed on 10 September 2021). [CrossRef]
- Ezeife, D.A.; Melosky, B.; Tudor, R.; Lin, S.; Lau, A.; Panzarella, T.; Leighl, N.B. Afatinib in Advanced Pretreated Non-Small-Cell Lung Cancer—A Canadian Experience. Curr. Oncol. 2018, 25, 385–390. Available online: https://www.ncbi.nlm.nih.gov/pubmed/30464688 (accessed on 10 September 2021). [CrossRef] [Green Version]
- Katakami, N.; Atagi, S.; Goto, K.; Hida, T.; Horai, T.; Inoue, A.; Ichinose, Y.; Koboyashi, K.; Takeda, K.; Kiura, K.; et al. LUX-Lung 4: A Phase II Trial of Afatinib in Patients with Advanced Non–Small-Cell Lung Cancer Who Progressed during Prior Treatment with Erlotinib, Gefitinib, or Both. J. Clin. Oncol. 2013, 31, 3335–3341. Available online: https://www.ncbi.nlm.nih.gov/pubmed/23816963 (accessed on 10 September 2021). [CrossRef]
- Lin, J.J.; Cardarella, S.; Lydon, C.A.; Dahlberg, S.E.; Jackman, D.M.; Jänne, P.A.; Johnson, B.E. Five-Year Survival in EGFR -Mutant Metastatic Lung Adenocarcinoma Treated with EGFR-TKIs. J. Thorac. Oncol. 2016, 11, 556–565. Available online: https://www.ncbi.nlm.nih.gov/pubmed/26724471 (accessed on 10 September 2021). [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics | N = 170 N (%) |
|---|---|
| Age at diagnosis (y), interquartile range (IQR) | 65 (IQR: 18.25) |
| Sex | |
| Female | 121 (71) |
| Male | 49 (29) |
| Race | |
| Caucasian | 117 (69) |
| Asian | 45 (27) |
| Black | 8 (4) |
| Smoking | |
| Never-smoker | 106 (62) |
| Ever-smoker | 64 (38) |
| ECOG PS | |
| 0–1 | 151 (89) |
| 2 | 19 (11) |
| >2 | 0 |
| Stage at Diagnosis | |
| Early stage | 23 (14) |
| Locally advanced | 19 (11) |
| Metastatic | 128 (75) |
| EGFR mutation | |
| Exon 19 (E19 del) | 98 (58) |
| Exon 21 (L858R) | 64 (37) |
| Exon 18 (E181) 1 | 7 (4) |
| Exon 20 insertion (E20) | 1 (1) |
| Type of molecular test: | |
| DhPLC (2004–2007) | 32 (19) |
| Single gene sequencing (2008–2010) | 17 (10) |
| Real-time PCR (2011–2014) | 48 (28) |
| NGS (2015-current) | 73 (43) |
| Brain metastases at diagnosis | |
| Present | 51 (30) |
| Not present | 119 (70) |
| Prior therapies for advanced/metastatic NSCLC before TKI | |
| Yes | 26 (15) |
| No | 144 (85) |
| EGFR-TKI | Frequency N (%) | Duration of Treatment Median (95% CI) in Mo | p-Value |
|---|---|---|---|
| First Line | |||
| Gefitinib | 110 (64.7) | 11.7 (8.03–15.36) | 0.535 |
| Erlotinib | 56 (32.9) | 11.4 (7.4–15.29) | |
| Afatinib | 4 (2.4) | not reached | |
| Total | 170 (100) | 11.5 (9.62–13.44) | |
| Second Line | |||
| Osimertinib | 30 (37.5) | 14.8 (2.05–27.47) | 0.001 |
| Erlotinib/Gefitinib | 5(6.3) | 2.1 (0.45–3.89) | |
| Afatinib | 8 (10.0) | 1.9 (036–3.64 | |
| Systemic chemo | 37 (46.2) | 2.5 (1.83–3.24) | |
| Total | 80 (100) | 4.4 (1.47–7.39) | |
| Third Line | |||
| Osimertinib | 2 (10.0) | All censored | n/a |
| Gefitinib/Erlotinib | 4 (20.0) | All censored | |
| Afatinib | 2 (10.0) | All censored | |
| Systemic chemo | 12 (60.0) | 2.8 (1.29–5.91) | |
| Total | 20 (100) | 3.9 (0.74–6.46) | |
| First-Line Outcomes | n (%) | Reason for Discontinuation n (%) | |
|---|---|---|---|
| Continued on First line | 33 (19) | ||
| Discontinued | 137 (81) | Started second line | 80 (58) |
| BSC * | 16 (12) | ||
| Died | 41 (30) | ||
| Total n (%) | 170 (100) | 137 (100) | |
| Response Rate (RR) | Afatinib | Gefitinib | Erlotinib | Total |
|---|---|---|---|---|
| CR +PR n (%) | 4 (100%) | 61 (55.4%) | 18 (32.1%) | 83 (48.8%) |
| SD n (%) | 0 | 28 (25.4%) | 16 (28.6%) | 44 (25.8%) |
| PD n (%) | 0 | 21 (19.0%) | 22 (39.3%) | 43 (25.4%) |
| Total n (%) | 4 (100%) | 110 (100%) | 56 (100%) | 170 (100%) |
| Variable | Comparator | Cox Regression Analysis | |||||
|---|---|---|---|---|---|---|---|
| Univariate Analysis | p-Value | Multivariate Analysis | p-Value | ||||
| HR | 95%CI | HR | 95% CI | ||||
| Female | Male | 0.91 | 0.62–1.3 | 0.65 | 0.91 | 0.6–1.4 | 0.66 |
| Never-smoker | Ever-smoker | 0.83 | 0.58–1.2 | 0.33 | 1.29 | 0.8–1.9 | 0.21 |
| ECOG PS > 2 | ≤2 | 0.44 | 0.3–0.8 | 0.005 | 0.45 | 0.3–0.8 | 0.004 |
| Exon 21/20/18 | Exon 19 * | 1.39 | 1.0–1.9 | 0.03 | 1.27 | 1.1–2.4 | 0.05 |
| Gefitinib ** | Erlotinib | 0.83 | 0.5–1.2 | 0.31 | 1.10 | 0.7–1.7 | 0.67 |
| Brain metastasis present | Absent | 1.50 | 1.0–2.2 | 0.05 | 1.50 | 1.1–2.3 | 0.04 |
| Non-Asian | Asian | 1.26 | 0.8–1.9 | 0.28 | 1.21 | 0.8–1.9 | 0.43 |
| NGS | Alternate test type *** | 2.07 | 1.4–3.0 | <0.001 | 2.25 | 1.4–3.5 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agulnik, J.S.; Kasymjanova, G.; Pepe, C.; Hurry, M.; Walton, R.N.; Sakr, L.; Cohen, V.; Small, D. Real-World Pattern of Treatment and Clinical Outcomes of EGFR-Mutant Non-Small Cell Lung Cancer in a Single Academic Centre in Quebec. Curr. Oncol. 2021, 28, 5179-5191. https://doi.org/10.3390/curroncol28060434
Agulnik JS, Kasymjanova G, Pepe C, Hurry M, Walton RN, Sakr L, Cohen V, Small D. Real-World Pattern of Treatment and Clinical Outcomes of EGFR-Mutant Non-Small Cell Lung Cancer in a Single Academic Centre in Quebec. Current Oncology. 2021; 28(6):5179-5191. https://doi.org/10.3390/curroncol28060434
Chicago/Turabian StyleAgulnik, Jason S., Goulnar Kasymjanova, Carmela Pepe, Manjusha Hurry, Ryan N. Walton, Lama Sakr, Victor Cohen, and David Small. 2021. "Real-World Pattern of Treatment and Clinical Outcomes of EGFR-Mutant Non-Small Cell Lung Cancer in a Single Academic Centre in Quebec" Current Oncology 28, no. 6: 5179-5191. https://doi.org/10.3390/curroncol28060434
APA StyleAgulnik, J. S., Kasymjanova, G., Pepe, C., Hurry, M., Walton, R. N., Sakr, L., Cohen, V., & Small, D. (2021). Real-World Pattern of Treatment and Clinical Outcomes of EGFR-Mutant Non-Small Cell Lung Cancer in a Single Academic Centre in Quebec. Current Oncology, 28(6), 5179-5191. https://doi.org/10.3390/curroncol28060434