HMGA1 Has Predictive Value in Response to Chemotherapy in Gastric Cancer

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Tissue Microarrays and Immunohistochemistry
2.3. Statistical Analysis
3. Results
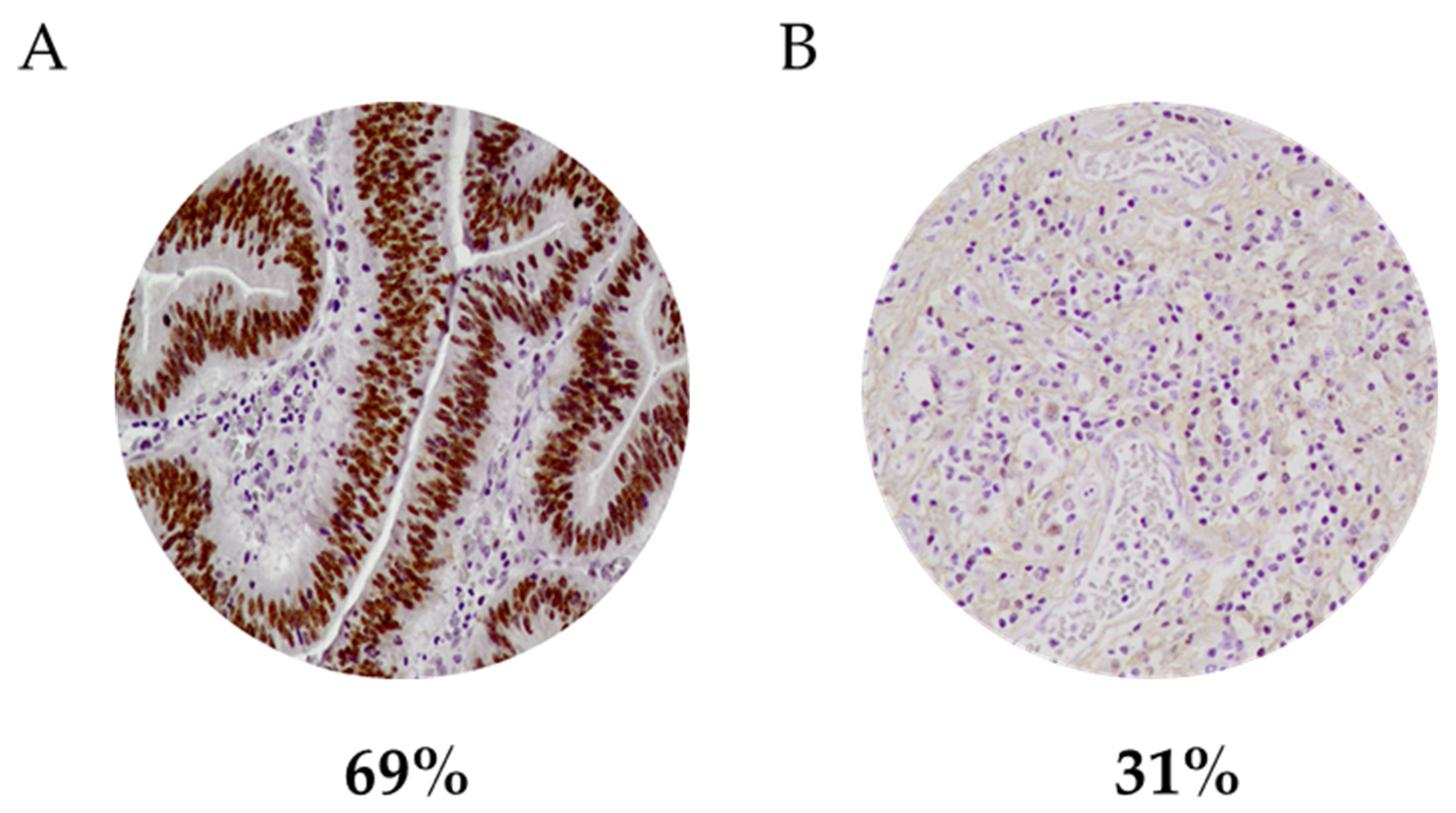
3.1. Association of HMGA1 Expression with Clinicopathological Features in Gastric Carcinomas
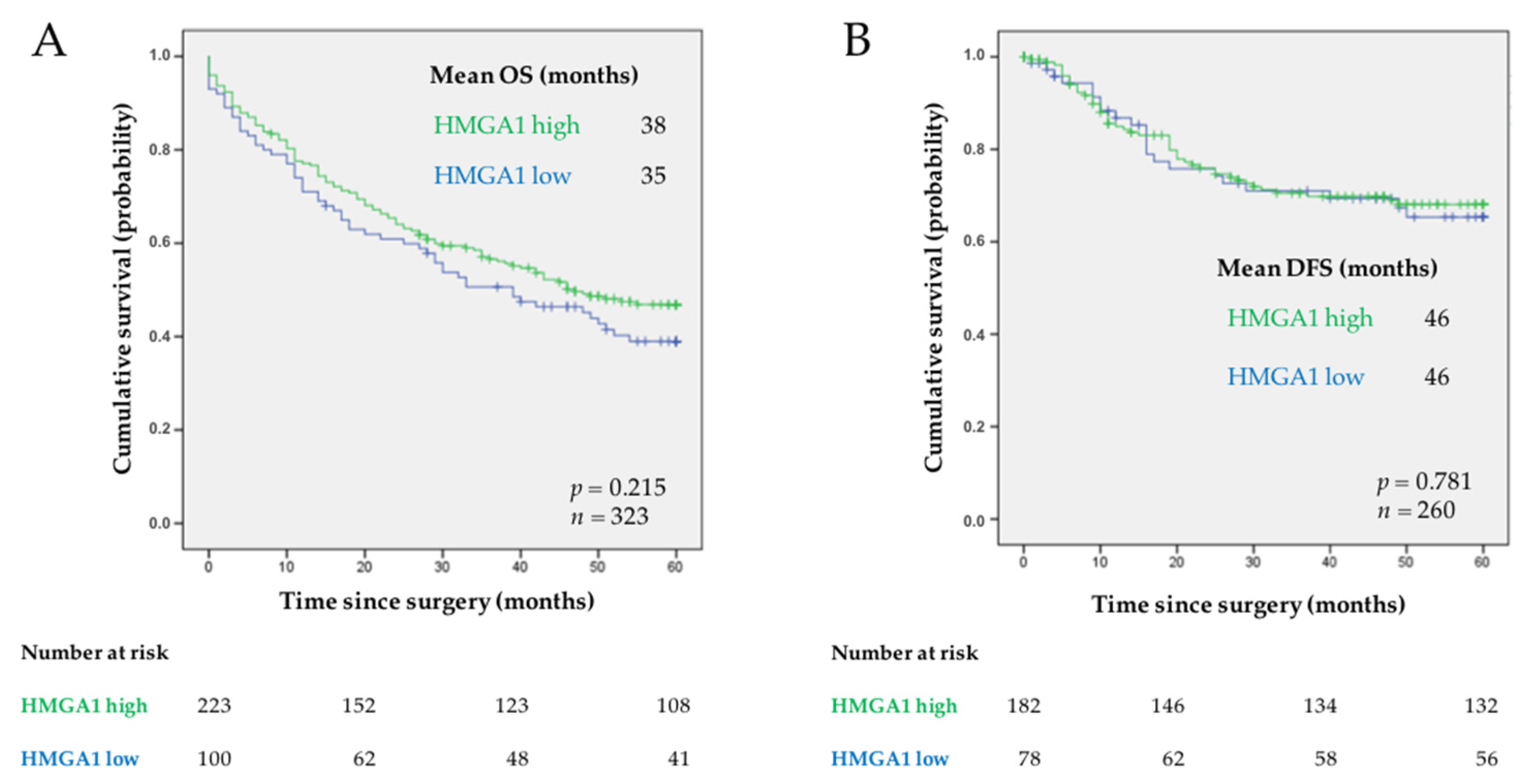
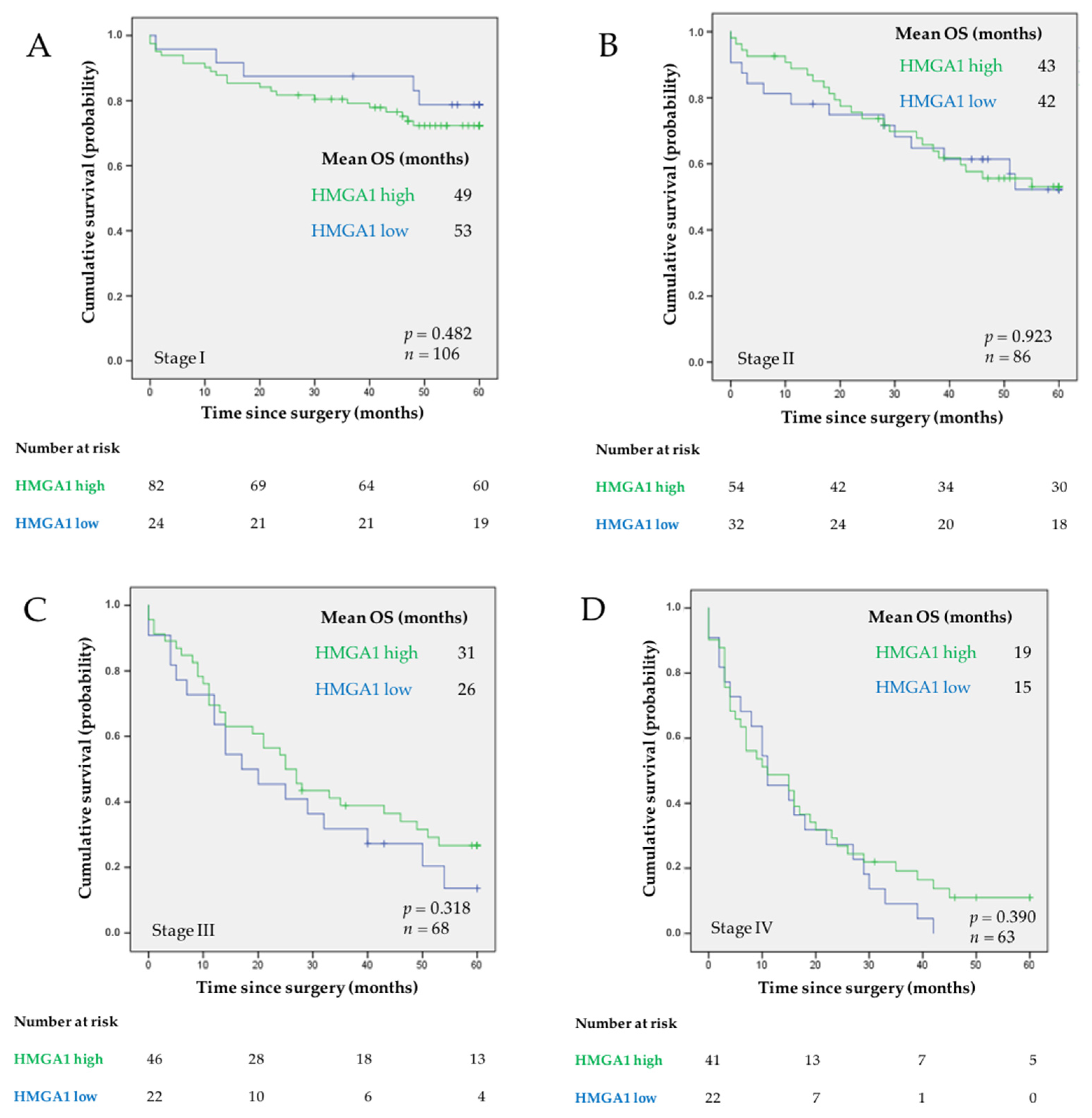
3.2. Evaluation of the Prognostic Significance of HMGA1 Expression in GC
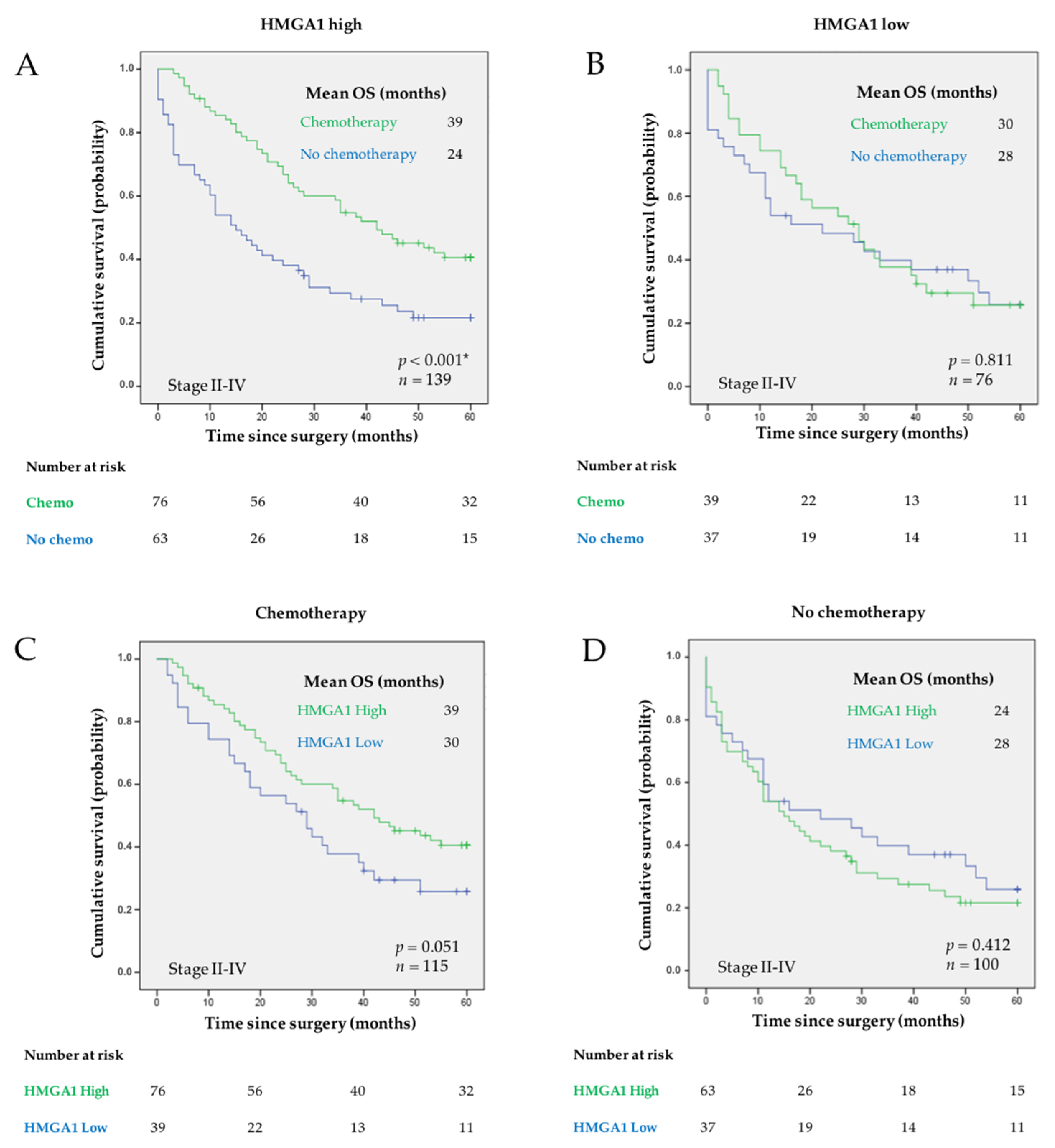
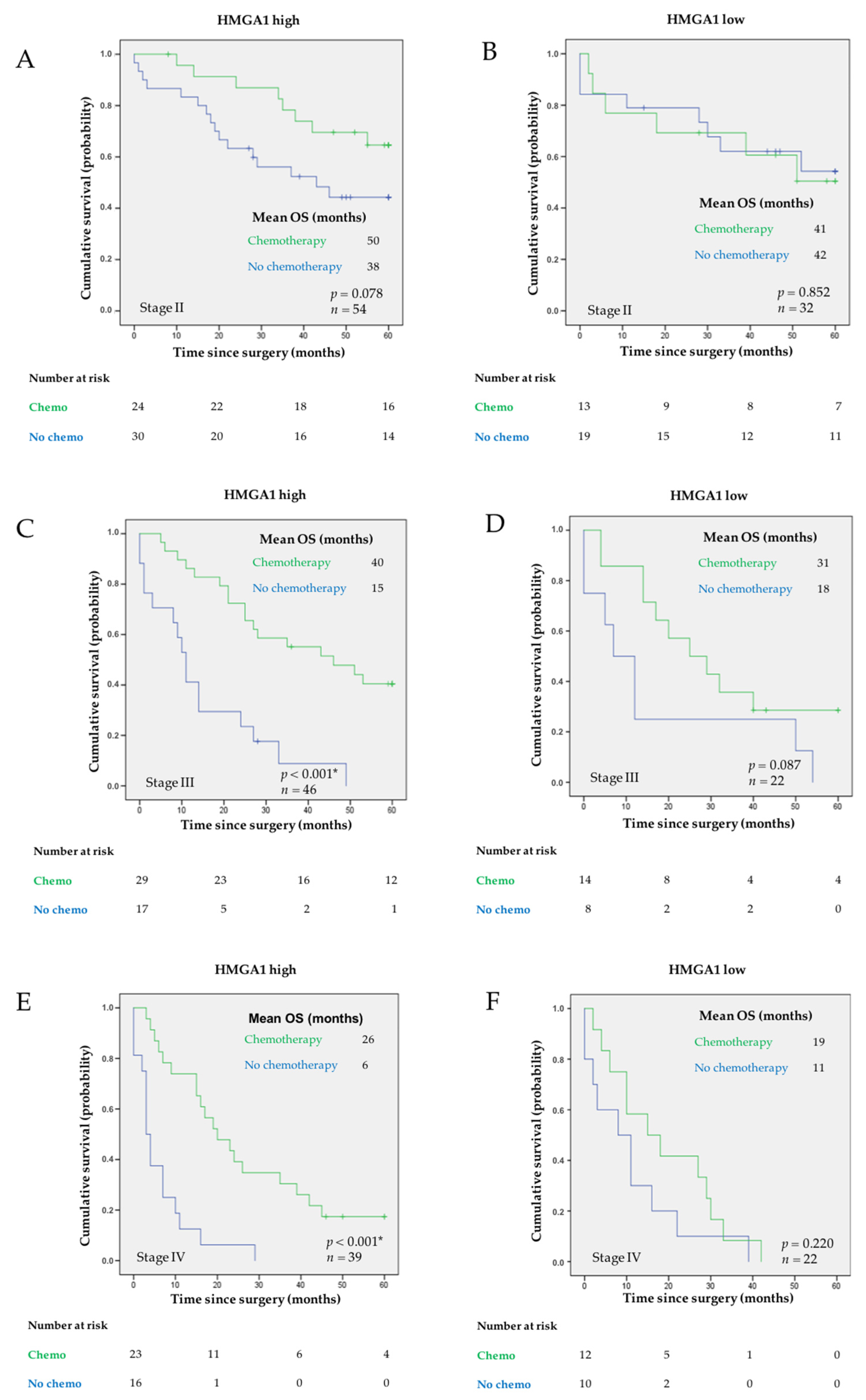
3.3. Evaluation of the Predictive Value of HMGA1 for Response to Chemotherapy in GC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Laurén, P. The two histological main types of gastric carcinoma: Diffuse and so-called intestinal-type carcinoma. An Attempt at a Histo-Clinical Classification. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef] [PubMed]
- Laurén, P. Histogenesis of intestinal and diffuse types of gastric carcinoma. Scand. J. Gastroenterol. Suppl. 1991, 180, 160–164. [Google Scholar] [PubMed]
- Smyth, E.C.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A.; Arnold, D.; ESMO Guidelines Committee. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v38–v49. [Google Scholar] [CrossRef] [PubMed]
- Song, Z.; Wu, Y.; Yang, J.; Yang, D.; Fang, X. Progress in the treatment of advanced gastric cancer. Tumor Biol. 2017, 39, 1010428317714626. [Google Scholar] [CrossRef] [Green Version]
- Correa, P.; Piazuelo, M.B.; Camargo, M.C. The future of gastric cancer prevention. Gastric Cancer 2004, 7, 9–16. [Google Scholar] [CrossRef]
- Digestive Cancers Europe (DiCE). Available online: https://digestivecancers.eu/gastric-cancer-map/ (accessed on 16 November 2021).
- Gao, J.-P.; Xu, W.; Liu, W.-T.; Yan, M.; Zhu, Z.-G. Tumor heterogeneity of gastric cancer: From the perspective of tumor-initiating cell. World J. Gastroenterol. 2018, 24, 2567–2581. [Google Scholar] [CrossRef]
- Gullo, I.; Carneiro, F.; Oliveira, C.; Almeida, G.M. Heterogeneity in Gastric Cancer: From Pure Morphology to Molecular Classifications. Pathobiology 2018, 85, 50–63. [Google Scholar] [CrossRef]
- Zou, J.; Wang, E. Cancer Biomarker Discovery for Precision Medicine: New Progress. Curr. Med. Chem. 2019, 26, 7655–7671. [Google Scholar] [CrossRef]
- Pádua, D.; Figueira, P.; Ribeiro, I.; Almeida, R.; Mesquita, P. The Relevance of Transcription Factors in Gastric and Colorectal Cancer Stem Cells Identification and Eradication. Front. Cell Dev. Biol. 2020, 8, 442. [Google Scholar] [CrossRef]
- Bushweller, J.H. Targeting transcription factors in cancer—From undruggable to reality. Nat. Rev. Cancer 2019, 19, 611–624. [Google Scholar] [CrossRef] [PubMed]
- Islam, Z.; Ali, A.M.; Naik, A.; Eldaw, M.; Decock, J.; Kolatkar, P.R. Transcription Factors: The Fulcrum Between Cell Development and Carcinogenesis. Front. Oncol. 2021, 11, 681377. [Google Scholar] [CrossRef]
- Ozturk, N.; Singh, I.; Mehta, A.; Braun, T.; Barreto, G. HMGA proteins as modulators of chromatin structure during transcriptional activation. Front. Cell Dev. Biol. 2014, 2, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombo, D.F.; Burger, L.; Baubec, T.; Schübeler, D. Binding of high mobility group A proteins to the mammalian genome occurs as a function of AT-content. PLoS Genet. 2017, 13, e1007102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, F.; Zhang, T.; Deng, S.-C.; Wei, J.-C.; Yang, P.; Wang, Q.; Chen, Z.-P.; Li, W.-L.; Chen, H.-C.; Hu, H.; et al. PD-L1 promotes colorectal cancer stem cell expansion by activating HMGA1-dependent signaling pathways. Cancer Lett. 2019, 450, 1–13. [Google Scholar] [CrossRef]
- Cao, X.P.; Cao, Y.; Zhao, H.; Yin, J.; Hou, P. HMGA1 promoting gastric cancer oncogenic and glycolytic phenotypes by regulating c-myc expression. Biochem. Biophys. Res. Commun. 2019, 516, 457–465. [Google Scholar] [CrossRef]
- Akaboshi, S.-I.; Watanabe, S.; Hino, Y.; Sekita, Y.; Xi, Y.; Araki, K.; Yamamura, K.-I.; Oshima, M.; Ito, T.; Baba, H.; et al. HMGA1 Is Induced by Wnt/β-Catenin Pathway and Maintains Cell Proliferation in Gastric Cancer. Am. J. Pathol. 2009, 175, 1675–1685. [Google Scholar] [CrossRef] [Green Version]
- Parisi, S.; Piscitelli, S.; Passaro, F.; Russo, T. HMGA Proteins in Stemness and Differentiation of Embryonic and Adult Stem Cells. Int. J. Mol. Sci. 2020, 21, 362. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.N.; Kerr, C.; Cope, L.; Zambidis, E.; Liu, C.; Hillion, J.; Belton, A.; Huso, D.L.; Resar, L.M.S. HMGA1 Reprograms Somatic Cells into Pluripotent Stem Cells by Inducing Stem Cell Transcriptional Networks. PLoS ONE 2012, 7, e48533. [Google Scholar] [CrossRef] [Green Version]
- Ben-Porath, I.; Thomson, M.W.; Carey, V.J.; Ge, R.; Bell, G.W.; Regev, A.; Weinberg, R.A. An embryonic stem cell–like gene expression signature in poorly differentiated aggressive human tumors. Nat. Genet. 2008, 40, 499–507. [Google Scholar] [CrossRef]
- Fusco, A.; Fedele, M. Roles of HMGA proteins in cancer. Nat. Rev. Cancer 2007, 7, 899–910. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Hu, L.; Zheng, Y.; Guo, L. HMGA1 in cancer: Cancer classification by location. J. Cell. Mol. Med. 2019, 23, 2293–2302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.N.; Cope, L.; Poh, W.; Belton, A.; Roy, S.; Talbot, C.C., Jr.; Sukumar, S.; Huso, D.L.; Resar, L.M. HMGA1: A Master Regulator of Tumor Progression in Triple-Negative Breast Cancer Cells. PLoS ONE 2013, 8, e63419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumter, T.F.; Xian, L.; Huso, T.; Koo, M.; Chang, Y.T.; Almasri, T.N.; Chia, L.; Inglis, C.; Reid, D.; Resar, L.M.S. The High Mobility Group A1 (HMGA1) Transcriptome in Cancer and Development. Curr. Mol. Med. 2016, 16, 353–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.N.; Resar, L.M. High mobility group A1 and cancer: Potential biomarker and therapeutic target. Histol. Histopathol. 2012, 27, 567–579. [Google Scholar]
- Jin, G.-H.; Shi, Y.; Tian, Y.; Cao, T.-T.; Mao, Y.; Tang, T.-Y. HMGA1 accelerates the malignant progression of gastric cancer through stimulating EMT. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 3642–3647. [Google Scholar]
- Yang, Q.; Wang, Y.; Li, M.; Wang, Z.; Zhang, J.; Dai, W.; Pei, M.; Hong, L.; Xiao, Y.; Hu, H.; et al. HMGA1 promotes gastric cancer growth and metastasis by transactivating SUZ12 and CCDC43 expression. Aging 2021, 13, 16043–16061. [Google Scholar] [CrossRef]
- Huang, R.; Huang, D.; Dai, W.; Yang, F. Overexpression of HMGA1 correlates with the malignant status and prognosis of breast cancer. Mol. Cell. Biochem. 2015, 404, 251–257. [Google Scholar] [CrossRef]
- Nam, E.S.; Kim, D.H.; Cho, S.J.; Chae, S.W.; Kim, H.Y.; Kim, S.M.; Han, J.J.; Shin, H.S.; Park, Y.E. Expression of HMGI(Y) associated with malignant phenotype of human gastric tissue. Histopathology 2003, 42, 466–471. [Google Scholar] [CrossRef]
- Resar, L.M.S. TheHigh Mobility Group A1Gene: Transforming Inflammatory Signals into Cancer? Cancer Res. 2010, 70, 436–439. [Google Scholar] [CrossRef] [Green Version]
- Chiappetta, G.; Botti, G.; Monaco, M.; Pasquinelli, R.; Pentimalli, F.; Di Bonito, M.; D’Aiuto, G.; Fedele, M.; Iuliano, R.; Palmieri, E.A.; et al. HMGA1 Protein Overexpression in Human Breast Carcinomas: Correlation with ErbB2 expression. Clin. Cancer Res. 2004, 10, 7637–7644. [Google Scholar] [CrossRef] [Green Version]
- Masciullo, V.; Baldassarre, G.; Pentimalli, F.; Berlingieri, M.T.; Boccia, A.; Chiappetta, G.; Palazzo, J.; Manfioletti, G.; Giancotti, V.; Viglietto, G.; et al. HMGA1 protein over-expression is a frequent feature of epithelial ovarian carcinomas. Carcinogenesis 2003, 24, 1191–1198. [Google Scholar] [CrossRef] [Green Version]
- Fu, F.; Wang, T.; Wu, Z.; Feng, Y.; Wang, W.; Zhou, S.; Ma, X.; Wang, S. HMGA1 exacerbates tumor growth through regulating the cell cycle and accelerates migration/invasion via targeting miR-221/222 in cervical cancer. Cell Death Dis. 2018, 9, 594. [Google Scholar] [CrossRef]
- Sgarra, R.; Pegoraro, S.; Ros, G.; Penzo, C.; Chiefari, E.; Foti, D.; Brunetti, A.; Manfioletti, G. High Mobility Group A (HMGA) proteins: Molecular instigators of breast cancer onset and progression. Biochim. Biophys. Acta Rev. Cancer 2018, 1869, 216–229. [Google Scholar] [CrossRef]
- Liang, L.; Li, X.; Zhang, X.; Lv, Z.; He, G.; Zhao, W.; Ren, X.; Li, Y.; Bian, X.; Liao, W.; et al. MicroRNA-137, an HMGA1 Target, Suppresses Colorectal Cancer Cell Invasion and Metastasis in Mice by Directly Targeting FMNL2. Gastroenterology 2013, 144, 624–635.e4. [Google Scholar] [CrossRef]
- Zhong, J.; Liu, C.; Chen, Y.-J.; Zhang, Q.-H.; Yang, J.; Kang, X.; Chen, S.-R.; Wen, G.-B.; Zu, X.-Y.; Cao, R.-X. The association between S100A13 and HMGA1 in the modulation of thyroid cancer proliferation and invasion. J. Transl. Med. 2016, 14, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, B.; Zhang, Y.; Zhou, L.; Yin, L.; Li, F.; Li, C.; Xia, J. The proliferation of cervical cancer is promoted by miRNA-125b through the regulation of the HMGA1. OncoTargets Ther. 2019, 12, 2767–2776. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.N.; Ren, C.C.; Yang, L.; Nai, M.M.; Xu, Y.M.; Zhang, F.; Liu, Y. MicroRNA let-7d-5p rescues ovarian cancer cell apoptosis and restores chemosensitivity by regulating the p53 signaling pathway via HMGA1. Int. J. Oncol. 2019, 54, 1771–1784. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Wang, H. HCP5 Promotes Proliferation and Contributes to Cisplatin Resistance in Gastric Cancer Through miR-519d/HMGA1 Axis. Cancer Manag. Res. 2021, 13, 787–794. [Google Scholar] [CrossRef]
- Wang, C.-Q. MiR-195 reverses 5-FU resistance through targeting HMGA1 in gastric cancer cells. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 3771–3778. [Google Scholar] [PubMed]
- Mesquita, P.; Freire, A.F.; Lopes, N.; Gomes, R.; Azevedo, D.; Barros, R.; Pereira, B.; Cavadas, B.; Pópulo, H.; Boaventura, P.; et al. Expression and Clinical Relevance of SOX9 in Gastric Cancer. Dis. Markers 2019, 2019, 8267021. [Google Scholar] [CrossRef] [PubMed]
- Jun, K.-H.; Jung, J.-H.; Choi, H.-J.; Shin, E.-Y.; Chin, H.-M. HMGA1/HMGA2 protein expression and prognostic implications in gastric cancer. Int. J. Surg. 2015, 24, 39–44. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, D.; Mussnich, P.; Rosa, R.; Bianco, R.; Tortora, G.; Fusco, A. High mobility group A1 protein expression reduces the sensitivity of colon and thyroid cancer cells to antineoplastic drugs. BMC Cancer 2014, 14, 851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loria, R.; Laquintana, V.; Bon, G.; Trisciuoglio, D.; Frapolli, R.; Covello, R.; Amoreo, C.A.; Ferraresi, V.; Zoccali, C.; Novello, M.; et al. HMGA1/E2F1 axis and NFkB pathways regulate LPS progression and trabectedin resistance. Oncogene 2018, 37, 5926–5938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Angelo, D.; Mussnich, P.; Arra, C.; Battista, S.; Fusco, A. Critical role of HMGA proteins in cancer cell chemoresistance. J. Mol. Med. 2017, 95, 353–360. [Google Scholar] [CrossRef]
- Dalerba, P.; Sahoo, D.; Paik, S.; Guo, X.; Yothers, G.; Song, N.; Wilcox-Fogel, N.; Forgó, E.; Rajendran, P.S.; Miranda, S.P.; et al. CDX2 as a Prognostic Biomarker in Stage II and Stage III Colon Cancer. N. Engl. J. Med. 2016, 374, 211–222. [Google Scholar] [CrossRef]
- Lee, H.; Lee, H.H.; Lim, C.Y.; Lee, J. The utility of high-mobility group A2 overexpression for predicting the prognosis of gastric cancer patients and its contribution to poor prognosis via chemoresistance and the propensity for the occurrence of carcinomatosis peritonei. Surgery 2021, 169, 1213–1220. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Cases | HMGA1 High | HMGA1 Low | p | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Patients | 323 | 223 | 69.0 | 100 | 31.0 | ||
| Age | |||||||
| Mean ± SD | 67.68 ± 11.85 | 68.26 ± 11.61 | 66.39 ± 12.32 | 0.19 | |||
| Range | 32–95 | 33–95 | 32–87 | ||||
| Gender | |||||||
| Female | 140 | 43.3 | 100 | 71.4 | 40 | 28.6 | 0.47 |
| Male | 183 | 56.7 | 123 | 67.2 | 60 | 32.8 | |
| Laurén Classification | |||||||
| Intestinal | 151 | 46.8 | 117 | 77.5 | 34 | 22.5 | <0.001 * |
| Diffuse | 41 | 12.7 | 18 | 43.9 | 23 | 56.1 | |
| Mixed | 85 | 26.3 | 60 | 70.6 | 25 | 29.4 | |
| Unclassified | 46 | 14.2 | |||||
| Growth Pattern | |||||||
| Expansive | 58 | 18.0 | 38 | 65.5 | 20 | 34.5 | 0.53 |
| Infiltrative | 252 | 78.0 | 176 | 69.8 | 76 | 30.2 | |
| Unclassified | 13 | 4.0 | |||||
| TNM | |||||||
| I | 106 | 32.8 | 82 | 77.4 | 24 | 22.6 | 0.14 |
| II | 86 | 26.6 | 54 | 62.8 | 32 | 37.2 | |
| III | 68 | 21.1 | 46 | 67.6 | 22 | 32.4 | |
| IV | 63 | 19.5 | 41 | 65.1 | 22 | 34.9 | |
| Vascular Invasion | |||||||
| No | 134 | 41.5 | 93 | 69.4 | 41 | 30.6 | 1.00 |
| Yes | 186 | 57.6 | 128 | 68.8 | 58 | 31.2 | |
| ND | 3 | 0.9 | |||||
| Perineural Invasion | |||||||
| No | 167 | 51.7 | 120 | 71.9 | 47 | 28.1 | 0.28 |
| Yes | 156 | 48.3 | 103 | 66.0 | 53 | 34.0 | |
| Chemotherapy treatment | |||||||
| No | 200 | 61.9 | 141 | 70.5 | 59 | 29.5 | 0.46 |
| Yes | 121 | 37.5 | 80 | 66.1 | 41 | 33.9 | |
| ND | 2 | 0.6 | |||||
| Number of Events | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| HMGA1 | |||||||
| Low | 28 | 1 | 1 | ||||
| High | 44 | 0.63 | 0.39–1.01 | 0.06 | 0.53 | 0.30–0.95 | 0.03 * |
| Laurén Classification | |||||||
| Intestinal | 23 | 1 | 1 | ||||
| Diffuse | 15 | 1.75 | 0.91–3.36 | 0.09 | 1.33 | 0.61–2.89 | 0.47 |
| Mixed | 23 | 1.51 | 0.84–2.27 | 0.17 | 1.06 | 0.56–1.98 | 0.87 |
| Growth pattern | |||||||
| Infiltrative | 65 | 1 | 1 | ||||
| Expansive | 5 | 0.74 | 0.30–1.83 | 0.51 | 0.82 | 0.31–2.16 | 0.68 |
| TNM | |||||||
| II | 14 | 1 | 1 | ||||
| III | 27 | 2.04 | 1.07–3.89 | 0.03 * | 2.03 | 0.96–4.29 | 0.06 |
| IV | 32 | 4.40 | 2.31–8.38 | <0.001 * | 4.41 | 2.08–9.34 | <0.01 * |
| Vascular Invasion | |||||||
| No | 20 | 1 | 1 | ||||
| Yes | 52 | 1.34 | 0.80–2.24 | 0.27 | 1.81 | 0.97–3.38 | 0.06 |
| Perineural Invasion | |||||||
| No | 20 | 1 | 1 | ||||
| Yes | 52 | 1.65 | 0.99–2.78 | 0.06 | 1.09 | 0.58–2.03 | 0.80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pádua, D.; Pinto, D.F.; Figueira, P.; Pereira, C.F.; Almeida, R.; Mesquita, P. HMGA1 Has Predictive Value in Response to Chemotherapy in Gastric Cancer. Curr. Oncol. 2022, 29, 56-67. https://doi.org/10.3390/curroncol29010005
Pádua D, Pinto DF, Figueira P, Pereira CF, Almeida R, Mesquita P. HMGA1 Has Predictive Value in Response to Chemotherapy in Gastric Cancer. Current Oncology. 2022; 29(1):56-67. https://doi.org/10.3390/curroncol29010005
Chicago/Turabian StylePádua, Diana, Débora Filipa Pinto, Paula Figueira, Carlos Filipe Pereira, Raquel Almeida, and Patrícia Mesquita. 2022. "HMGA1 Has Predictive Value in Response to Chemotherapy in Gastric Cancer" Current Oncology 29, no. 1: 56-67. https://doi.org/10.3390/curroncol29010005
APA StylePádua, D., Pinto, D. F., Figueira, P., Pereira, C. F., Almeida, R., & Mesquita, P. (2022). HMGA1 Has Predictive Value in Response to Chemotherapy in Gastric Cancer. Current Oncology, 29(1), 56-67. https://doi.org/10.3390/curroncol29010005