The Predictive Significance of Prognostic Nutritional Index and Serum Albumin/Globulin Ratio on the Overall Survival of Penile Cancer Patients Undergoing Penectomy

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Data Collection
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patients’ Information
3.2. The Best Cut-Off Values of PNI, AGR, SII, and PLR before Treatment
3.3. Comparison of Clinical Data of Patients in Different Groups
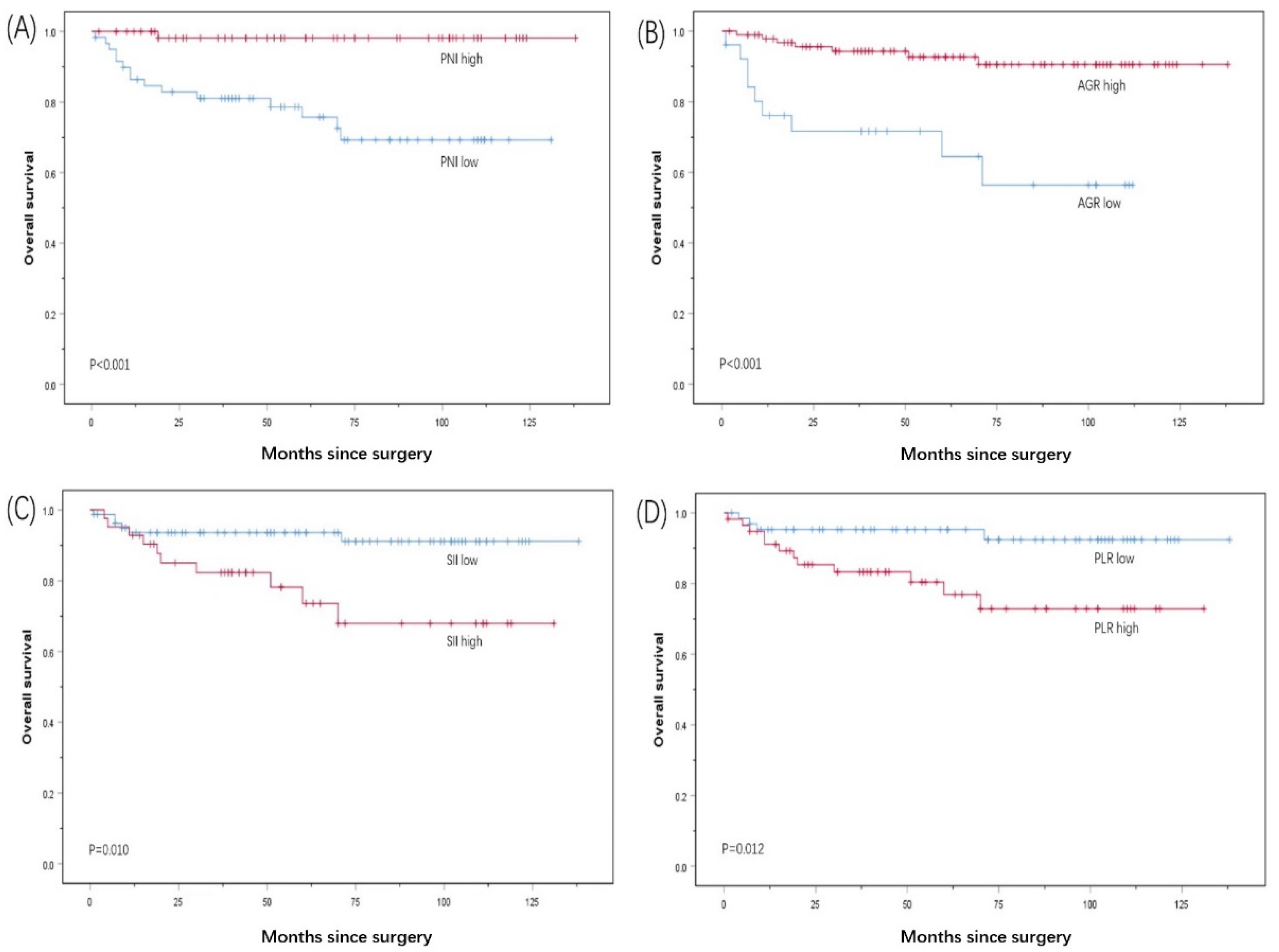
3.4. Kaplan–Meier Survival Analysis
3.5. Univariable and Multivariable Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mobilio, G.; Ficarra, V. Genital treatment of penile carcinoma. Curr. Opin. Urol. 2001, 11, 299–304. [Google Scholar]
- Mulherkar, R.; Hasan, S.; Wegner, R.E.; Verma, V.; Glaser, S.M.; Kalash, R.; Beriwal, S.; Horne, Z.D. National patterns of care for early-stage penile cancers in the United States: How is radiation and brachytherapy utilized?—ScienceDirect. Brachytherapy 2019, 18, 503–509. [Google Scholar]
- Marchioni, M.; Berardinelli, F.; de Nunzio, C.; Spiess, P.; Porpiglia, F.; Schips, L.; Cindolo, L. New insight in penile cancer. Minerva Urol. E Nefrol. 2018, 70, 559–569. [Google Scholar]
- Van Berckelaer, C.; Van Geyt, M.; Linders, S.; Rypens, C.; Trinh, X.B.; Tjalma, W.A.A.; Van Laere, S.; Colpaert, C.; Dirix, L.; Van Dam, P.A. A high neutrophil- lymphocyte ratio and platelet-lymphocyte ratio are associated with a worse outcome in inflammatory breast cancer. Breast 2020, 53, 212–220. [Google Scholar]
- Kawata, A.; Taguchi, A.; Baba, S.; Miyamoto, Y.; Tanikawa, M.; Sone, K.; Tsuruga, T.; Mori, M.; Oda, K.; Kawana, K.; et al. A low preoperative albumin-to- globulin ratio is a negative prognostic factor in patients with surgically treated cervical cancer. Int. J. Clin. Oncol. 2021, 26, 980–985. [Google Scholar]
- Huang, X.; Hu, H.; Zhang, W.; Shao, Z. Prognostic value of prognostic nutritional index and systemic immune-inflammation index in patients with osteosarcoma. J. Cell. Physiol. 2019, 234, 18408–18414. [Google Scholar]
- Edge, S.B.; Byrd, D.R.; Compton, C.C.; Fritz, A.G.; Greene, F.L.; Trotti, A. (Eds.) AJCC Cancer Staging Manual, 7th ed.; Springer: New York, NY, USA, 2010. [Google Scholar]
- Wei, C.K.; Wu, C.C.; Su, Y.C.; Yu, C.H.; Lee, C.C. Adjusted Age-Adjusted Charlson Comorbidity Index Score as a Risk Measure of Perioperative Mortality before Cancer Surgery. PLoS ONE 2016, 11, e0148076. [Google Scholar]
- Huang, J.; Yuan, Y.; Wang, Y.; Chen, Y.; Kong, W.; Xue, W.; Chen, H.; Zhang, J.; Huang, Y. Preoperative prognostic nutritional index is a significant predictor of survival in patients with localized upper tract urothelial carcinoma after radical nephroureterectomy. Urol. Oncol. 2017, 35, 671.e1–671.e9. [Google Scholar]
- Song, W.; Tian, C.; Kai, W.; Zhang, R.; Zou, S. Preoperative platelet lymphocyte ratio as independent predictors of prognosis in pancreatic cancer: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0178762. [Google Scholar]
- Nanjappa, V.; Thomas, J.K.; Marimuthu, A.; Muthusamy, B.; Radhakrishnan, A.; Sharma, R.; Khan, A.A.; Balakrishnan, L.; Sahasrabuddhe, N.A.; Kumar, S.; et al. Plasma Proteome Database as a resource for proteomics research: 2014 update. Nucleic Acids Res. 2013, 42, D959–D965. [Google Scholar]
- Doweiko, J.P.; Nompleggi, D. Reviews: The Role of Albumin in Human Physiology and Pathophysiology, Part III: Albumin and Disease States. J. Parenter. Enter. Nutr. 1991, 15, 476–483. [Google Scholar]
- Yu, J.; Hong, B.; Park, J.Y.; Hwang, J.H.; Kim, Y.K. Impact of Prognostic Nutritional Index on Postoperative Pulmonary Complications in Radical Cystectomy: A Propensity Score-Matched Analysis. Ann. Surg. Oncol. 2021, 28, 1859–1869. [Google Scholar]
- Gupta, D.; Lis, C.G. Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature. Nutr. J. 2010, 9, 69. [Google Scholar]
- Guthrie, G.; Roxburgh, C.; Farhan-Alanie, O.; Horgan, P.; McMillan, D. Comparison of the prognostic value of longitudinal measurements of systemic inflammation in patients undergoing curative resection of colorectal cancer. Br. J. Cancer 2013, 109, 24–28. [Google Scholar]
- Wang, N.; Liu, J.Y.; Li, X.; Deng, M.H.; Long, Z.; Tang, J.; Yao, K.; Zhang, Y.C.; He, L.Y. Pretreatment serum albumin/globulin ratio as a prognostic biomarker in metastatic prostate cancer patients treated with maximal androgen blockade. Asian J. Androl. 2018, 21, 56–61. [Google Scholar]
- Masafumi, O.; Tomohiko, K.; Toshihiro, U.; Nobushige, T.; Tetsuo, S.; Masayuki, K.; Atsushi, K.; Satoshi, F. Prognostic role of the preoperative serum albumin: Globulin ratio after radical nephroureterectomy for upper tract urothelial carcinoma. Int. J. Urol. 2018, 25, 871–878. [Google Scholar]
- Gregg, J.R.; Cookson, M.S.; Phillips, S.; Salem, S.; Chang, S.S.; Clark, P.E.; Davis, R.; Stimson, C.J., Jr.; Aghazadeh, M.; Smith, J.A., Jr.; et al. Effect of preoperative nutritional deficiency on mortality after radical cystectomy for bladder cancer. J. Urol. 2011, 185, 90–96. [Google Scholar]
- Suh, B.; Park, S.; Shin, D.W.; Yun, J.M.; Keam, B.; Yang, H.-K.; Ahn, E.; Lee, H.; Park, J.K.; Cho, B. Low albumin-to-globulin ratio associated with cancer incidence and mortality in generally healthy adults. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2014, 25, 2260–2266. [Google Scholar]
- Barbosa-Silva, M.C. Subjective and objective nutritional assessment methods: What do they really assess? Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 248–254. [Google Scholar]
- Elinav, E.; Nowarski, R.; Thaiss, C.A.; Hu, B.; Jin, C.C.; Flavell, R.A. Inflammation-induced cancer: Crosstalk between tumors, immune cells, and microorganisms. Nat. Rev. Cancer 2013, 13, 759–771. [Google Scholar]
- Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar]
- Park, J.H.; Watt, D.G.; Roxburgh, C.S.; Horgan, P.G.; McMillan, D.C. Colorectal cancer, systemic inflammation, and outcome: Staging the tumor and staging the host. Ann. Surg. 2016, 263, 326–336. [Google Scholar]
- Toiyama, Y.; Inoue, Y.; Saigusa, S.; Kawamura, M.; Kawamoto, A.; Okugawa, Y.; Koji, J.; Tanaka, K.; Mohri, Y.; Kusunoki, M. C-reactive protein as a predictor of recurrence in patients with rectal cancer undergoing chemoradiotherapy followed by surgery. Anticancer Res. 2013, 33, 5065–5074. [Google Scholar]
- Dunn, G.P.; Old, L.J.; Schreiber, R.D. The immunobiology of cancer immunosurveillance and immunoediting. Immunity 2004, 21, 137–148. [Google Scholar]
- Wu, X.; Jiang, Y.; Ge, H.; Diao, P.F.; Wang, D.M.; Wang, Y.L.; Cheng, J. Predictive value of prognostic nutritional index in patients with oral squamous cell carcinoma. Oral Dis. 2020, 26, 903–911. [Google Scholar]
- Ucar, G.; Ergun, Y.; Acikgoz, Y.; Uncu, D. The prognostic value of the prognostic nutritional index in patients with metastatic colorectal cancer. Asia Pac. J. Clin. Oncol. 2020, 16, e179–e184. [Google Scholar]
- Li, N.; Song, W.; Gao, J.; Xu, Z.; Long, Z.; Liu, J.; He, L. The prognostic nutritional index predicts the biochemical recurrence of patients treated with robot-assisted laparoscopic radical prostatectomy. Prostate 2022, 82, 221–226. [Google Scholar]
- Grimm, T.; Buchner, A.; Schneevoigt, B.; Kretschmer, A.; Apfelbeck, M.; Grabbert, M.; Jokisch, J.F.; Stief, C.G.; Karl, A. Impact of preoperative hemoglobin and CRP levels on cancer-specific survival in patients undergoing radical cystectomy for transitional cell carcinoma of the bladder: Results of a single-center study. World J. Urol. 2016, 34, 703–708. [Google Scholar]
- Cohen, M.H.; Makuch, R.; Johnston-Early, A.; Ihde, D.C.; Bunn, P.A., Jr.; Fossieck, B.E.; Minna, J.D. Laboratory parameters as an alternative to performance status in prognostic stratification of patients with small cell lung cancer. Cancer Treat Rep. 1981, 65, 187–195. [Google Scholar]
- Codina Cazador, A.; Salva Lacombe, J.A.; Fernandez-Llamazares Rodriguez, J.; Ruiz Feliu, B.; Codina Barreras, A.; Moreno Aguado, V. Immunoglobulins and the complement system in colorectal cancer. Rev. Esp. Enferm. Apar. Dig. 1989, 75, 143–148. [Google Scholar]
- Chung, J.W.; Dong, J.P.; Chun, S.Y.; Choi, S.H.; Lee, J.N.; Kim, B.S.; Kim, H.T.; Kim, T.H.; Yoo, E.S.; Byun, S.S.; et al. The prognostic role of preoperative serum albumin/globulin ratio in patients with non-metastatic renal cell carcinoma undergoing partial or radical nephrectomy. Sci. Rep. 2020, 10, 11999. [Google Scholar]
- Liu, J.; Dai, Y.; Zhou, F.; Long, Z.; Li, Y.; Liu, B.; Xie, D.; Tang, J.; Tan, J.; Yao, K.; et al. The prognostic role of preoperative serum albumin/globulin ratio in patients with bladder urothelial carcinoma undergoing radical cystectomy. Urol. Oncol. Semin. Orig. Investig. 2016, 34, 484.e1–484.e8. [Google Scholar]
- Noh, J.H.; Na, H.K.; Kim, Y.H.; Song, H.J.; Kim, H.R.; Choi, K.D.; Lee, G.H.; Jung, H.Y. Influence of Preoperative Nutritional Status on Patients Who Undergo Upfront Surgery for Esophageal Squamous Cell Carcinoma. Nutr. Cancer 2022, 74, 2910–2919. [Google Scholar]
- Li, X.H.; Gu, W.S.; Wang, X.P.; Lin, J.H.; Zheng, X.; Zhang, L.; Kang, T.; Zhang, Z.X.; Liu, W.L. Low Preoperative albumin-to-globulin ratio Predict Poor Survival and Negatively Correlated with Fibrinogen in Resectable Esophageal Squamous Cell Carcinoma. J. Cancer 2017, 8, 1833–1842. [Google Scholar]
- Tu, I.W.; Shannon, N.B.; Thankappan, K.; Balasubramanian, D.; Pillai, V.; Shetty, V.; Rangappa, V.; Chandrasekhar, N.H.; Kekatpure, V.; Kuriakose, M.A.; et al. Risk Stratification in Oral Cancer: A Novel Approach. Front. Oncol. 2022, 12, 836803. [Google Scholar] [CrossRef]
- Wang, Y.T.; Fang, K.H.; Hsu, C.M.; Chang, G.H.; Lai, C.H.; Lee, Y.C.; Tsai, M.S.; Huang, E.I.; Tsai, Y.T. Retrospective study on the potential of albumin/globulin ratio as a prognostic biomarker for oral cavity cancer patients. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 227–238. [Google Scholar]
- Fu, Y.; Chen, S.W.; Chen, S.Q.; Ou-Yang, D.; Liu, W.W.; Song, M.; Yang, A.K.; Zhang, Q. A Preoperative Nutritional Index for Predicting Cancer-Specific and Overall Survival in Chinese Patients with Laryngeal Cancer: A Retrospective Study. Medicine 2016, 95, e2962. [Google Scholar]
- Chen, W.Z.; Yu, S.T.; Xie, R.; Lv, Y.X.; Xu, D.B.; Yu, J.C. Preoperative albumin/globulin ratio has predictive value for patients with laryngeal squamous cell carcinoma. Oncotarget 2017, 8, 48240–48247. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total n = 123 | % |
|---|---|---|
| Age, y | ||
| ˂60 | 64 | 52 |
| ≥60 | 59 | 48 |
| aCCI median (IQR) | 3.00 (3.00–4.00) | |
| ZPS | ||
| 0 | 120 | 97.6 |
| 1 | 3 | 2.4 |
| Penis removal range | ||
| Part | 101 | 82.1 |
| Entire | 22 | 17.9 |
| Necrosis | ||
| No | 113 | 91.9 |
| Yes | 10 | 8.1 |
| T stage | ||
| T < 2 | 94 | 76.4 |
| T ≥ 2 | 29 | 23.6 |
| Clinical n stage | ||
| n = 0 | 115 | 93.5 |
| n > 0 | 8 | 6.5 |
| Pathological type | ||
| Carcinoma in situ | 12 | 9.8 |
| Squamous cell carcinoma | 111 | 90.2 |
| Verrucous | 46 | 37.4 |
| Highly differentiated | 35 | 28.5 |
| Moderately differentiated | 26 | 21.1 |
| Poorly differentiated | 4 | 3.2 |
| PNI median (IQR) | 49.30 (45.20–52.90) | |
| AGR median (IQR) | 1.51 (1.32–1.72) | |
| SII median (IQR) | 464.53 (358.50–757.33) | |
| PLR median (IQR) | 118.52 (92.14–149.19) | |
| NLR median (IQR) | 2.33 (1.78–3.20) | |
| Follow-up time (months) median (IQR) | 58.00 (27.00–97.00) |
| PNI | AGR | SII | PLR | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Low | High | p | Low | High | p | Low | High | p | Low | High | p |
| (60) | (63) | (26) | (97) | (81) | (42) | (65) | (58) | |||||
| Age, y | 0.061 | 0.501 | 0.279 | 0.671 | ||||||||
| ˂60 | 26 | 38 | 12 | 52 | 45 | 19 | 35 | 29 | ||||
| ≥60 | 34 | 25 | 14 | 45 | 36 | 23 | 30 | 29 | ||||
| ZPS | 0.532 | 0.602 | 0.231 | 0.064 | ||||||||
| 0 | 58 | 62 | 25 | 95 | 80 | 40 | 65 | 55 | ||||
| 1 | 2 | 1 | 1 | 2 | 1 | 2 | 0 | 3 | ||||
| Penis removal range | 0.125 | 0.178 | 0.027 | 0.089 | ||||||||
| Part | 46 | 55 | 19 | 82 | 71 | 30 | 57 | 44 | ||||
| Entire | 14 | 8 | 7 | 15 | 10 | 12 | 8 | 14 | ||||
| Necrosis | 0.461 | 0.476 | 0.272 | 0.398 | ||||||||
| No | 54 | 59 | 23 | 90 | 76 | 37 | 61 | 52 | ||||
| Yes | 6 | 4 | 3 | 7 | 5 | 5 | 4 | 6 | ||||
| T stage | 0.565 | 0.966 | 0.843 | 0.732 | ||||||||
| T < 2 | 45 | 49 | 20 | 74 | 62 | 32 | 50 | 44 | ||||
| T ≥ 2 | 15 | 14 | 6 | 23 | 19 | 10 | 15 | 14 | ||||
| Clinical N stage | 0.943 | 0.039 | 0.330 | 0.104 | ||||||||
| n = 0 | 56 | 59 | 22 | 93 | 77 | 38 | 63 | 52 | ||||
| n > 0 | 4 | 4 | 4 | 4 | 4 | 4 | 2 | 6 | ||||
| Histological type | 0.751 | 0.396 | 0.303 | 0.267 | ||||||||
| Carcinoma in situ | 6 | 6 | 3 | 9 | 8 | 4 | 6 | 6 | ||||
| Squamous cell carcinoma | 54 | 57 | 23 | 88 | 73 | 38 | 59 | 52 | ||||
| Verrucous | 24 | 22 | 7 | 39 | 32 | 14 | 26 | 20 | ||||
| Highly differentiated | 12 | 23 | 8 | 27 | 24 | 11 | 22 | 13 | ||||
| Moderately differentiated | 14 | 12 | 7 | 19 | 16 | 10 | 10 | 16 | ||||
| Poorly differentiated | 4 | 0 | 1 | 3 | 1 | 3 | 1 | 3 |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age, y | 0.077 | |||||
| ˂60 | 1 | |||||
| ≥60 | 2.596 | 0.901–7.481 | ||||
| aCCI | 2.676 | 1.544–4.637 | <0.001 | 1.327 | 0.623–2.823 | 0.463 |
| ZPS | 0.082 | |||||
| 0 | 1 | |||||
| 1 | 6.276 | 0.792–49.751 | ||||
| Penis removal range | 0.107 | |||||
| Part | 1 | |||||
| Entire | 2.393 | 0.828–6.913 | ||||
| Necrosis | 0.226 | |||||
| No | 1 | |||||
| Yes | 2.543 | 0.561–11.524 | ||||
| T stage | 0.324 | |||||
| T < 2 | 1 | |||||
| T ≥ 2 | 1.703 | 0.591–4.901 | ||||
| Clinical n stage | 0.011 | 0.033 | ||||
| n = 0 | 1 | 1 | ||||
| n > 0 | 5.243 | 1.454–18.898 | 7.553 | 1.178–48.415 | ||
| Pathological type | <0.001 | 0.045 | ||||
| Carcinoma in situ | 1 | 1 | ||||
| Squamous cell carcinoma | ||||||
| Verrucous | 0.934 | 0.104–8.356 | 1.424 | 0.149–13.635 | ||
| Highly differentiated | 1.994 | 0.240–16.581 | 3.133 | 0.366–26.786 | ||
| Moderately differentiated | 0.449 | 0.028–7.184 | 0.321 | 0.013–7.954 | ||
| Poorly differentiated | 32.025 | 3.418–300.096 | 20.158 | 1.571–258.591 | ||
| NLR | 1.077 | 0.950–1.221 | 0.243 | |||
| PNI | 0.007 | 0.036 | ||||
| Low | 1 | 1 | ||||
| High | 0.061 | 0.008–0.462 | 0.091 | 0.010–0.853 | ||
| AGR | <0.001 | 0.012 | ||||
| Low | 1 | 1 | ||||
| High | 0.160 | 0.059–0.429 | 0.171 | 0.043–0.680 | ||
| SII | 0.017 | 0.146 | ||||
| Low | 1 | 1 | ||||
| High | 3.457 | 1.251–9.551 | 2.512 | 0.725–8.703 | ||
| PLR | 0.022 | 0.321 | ||||
| Low | 1 | 1 | ||||
| High | 3.772 | 1.212–11.737 | 0.449 | 0.093–2.180 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, W.-J.; Li, N.-C.; Gao, J.; Xu, Z.-P.; Liu, J.-Y.; Long, Z.; He, L.-Y. The Predictive Significance of Prognostic Nutritional Index and Serum Albumin/Globulin Ratio on the Overall Survival of Penile Cancer Patients Undergoing Penectomy. Curr. Oncol. 2022, 29, 7569-7578. https://doi.org/10.3390/curroncol29100596
Song W-J, Li N-C, Gao J, Xu Z-P, Liu J-Y, Long Z, He L-Y. The Predictive Significance of Prognostic Nutritional Index and Serum Albumin/Globulin Ratio on the Overall Survival of Penile Cancer Patients Undergoing Penectomy. Current Oncology. 2022; 29(10):7569-7578. https://doi.org/10.3390/curroncol29100596
Chicago/Turabian StyleSong, Wei-Jie, Ni-Chujie Li, Jun Gao, Zhi-Peng Xu, Jian-Ye Liu, Zhi Long, and Le-Ye He. 2022. "The Predictive Significance of Prognostic Nutritional Index and Serum Albumin/Globulin Ratio on the Overall Survival of Penile Cancer Patients Undergoing Penectomy" Current Oncology 29, no. 10: 7569-7578. https://doi.org/10.3390/curroncol29100596
APA StyleSong, W. -J., Li, N. -C., Gao, J., Xu, Z. -P., Liu, J. -Y., Long, Z., & He, L. -Y. (2022). The Predictive Significance of Prognostic Nutritional Index and Serum Albumin/Globulin Ratio on the Overall Survival of Penile Cancer Patients Undergoing Penectomy. Current Oncology, 29(10), 7569-7578. https://doi.org/10.3390/curroncol29100596