Histologic and Genotypic Characterization of Lung Cancer in the Inuit Population of the Eastern Canadian Arctic

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Histology
2.3. Molecular Analysis
2.4. CBioPortal
2.5. Statistical Considerations
3. Results
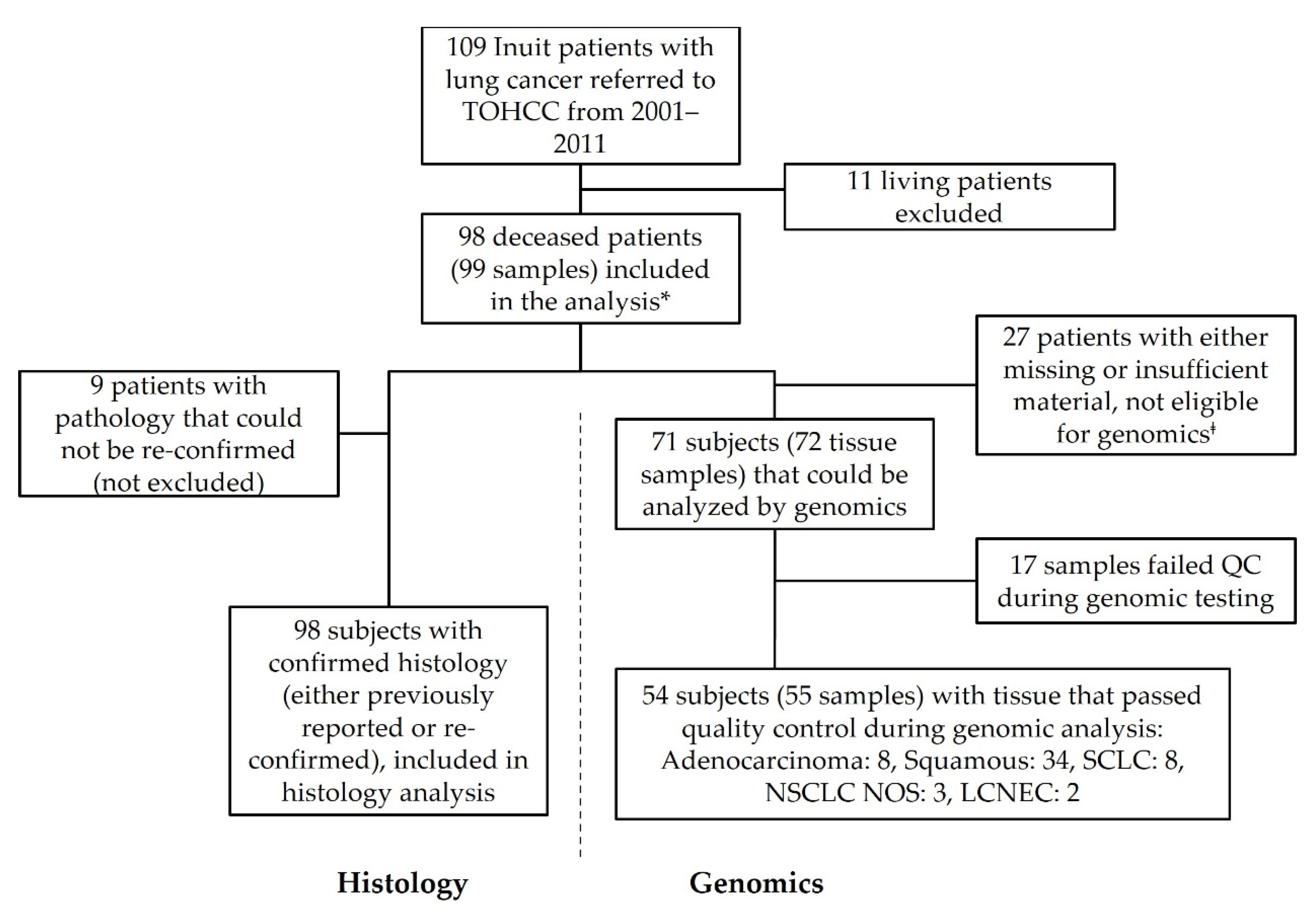
3.1. Participant Selection and Study Flow
3.2. Patient Demographics
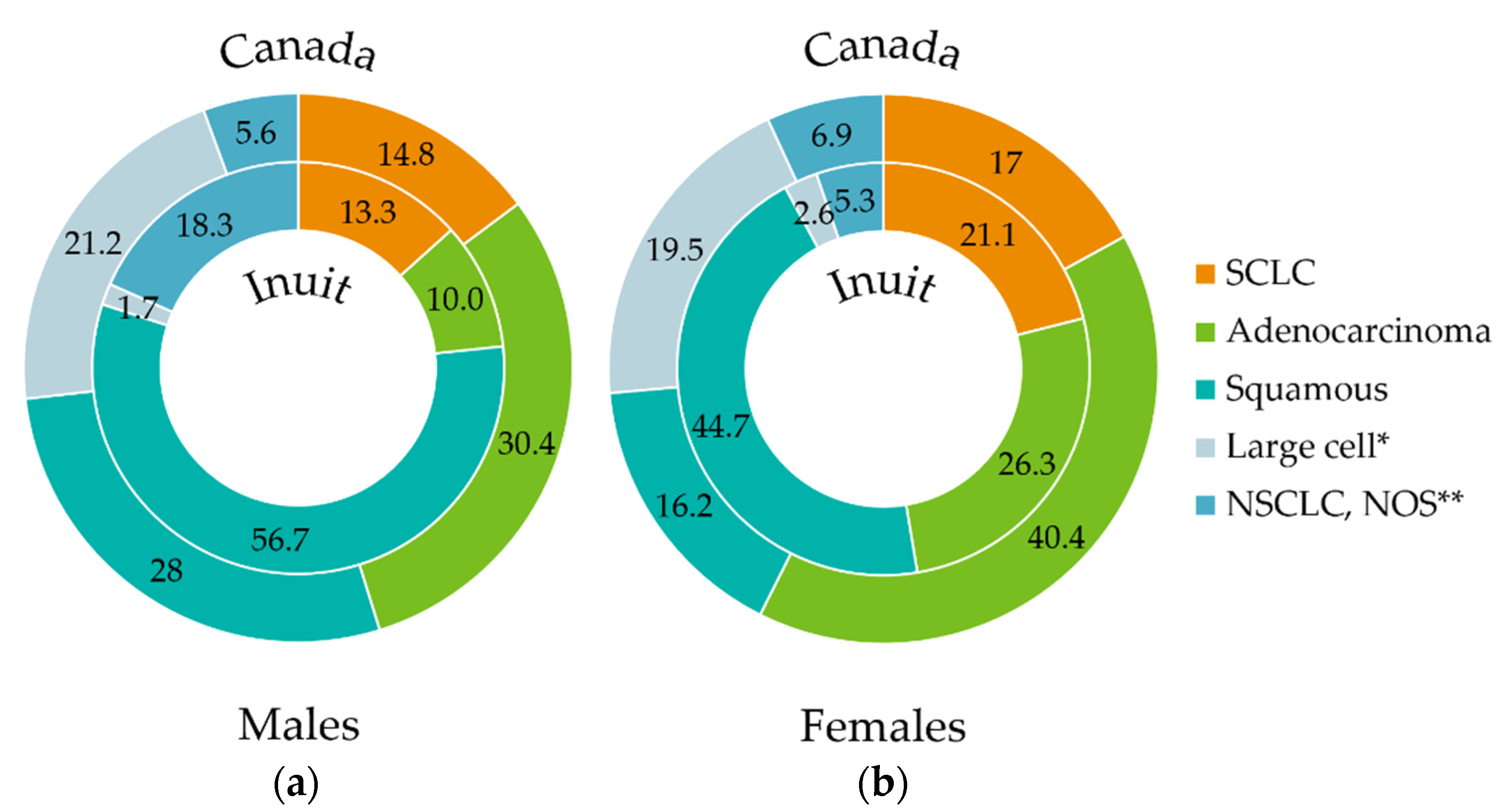
3.3. SCC of the Lung Is the Most Common Histological Subtype in This Cohort

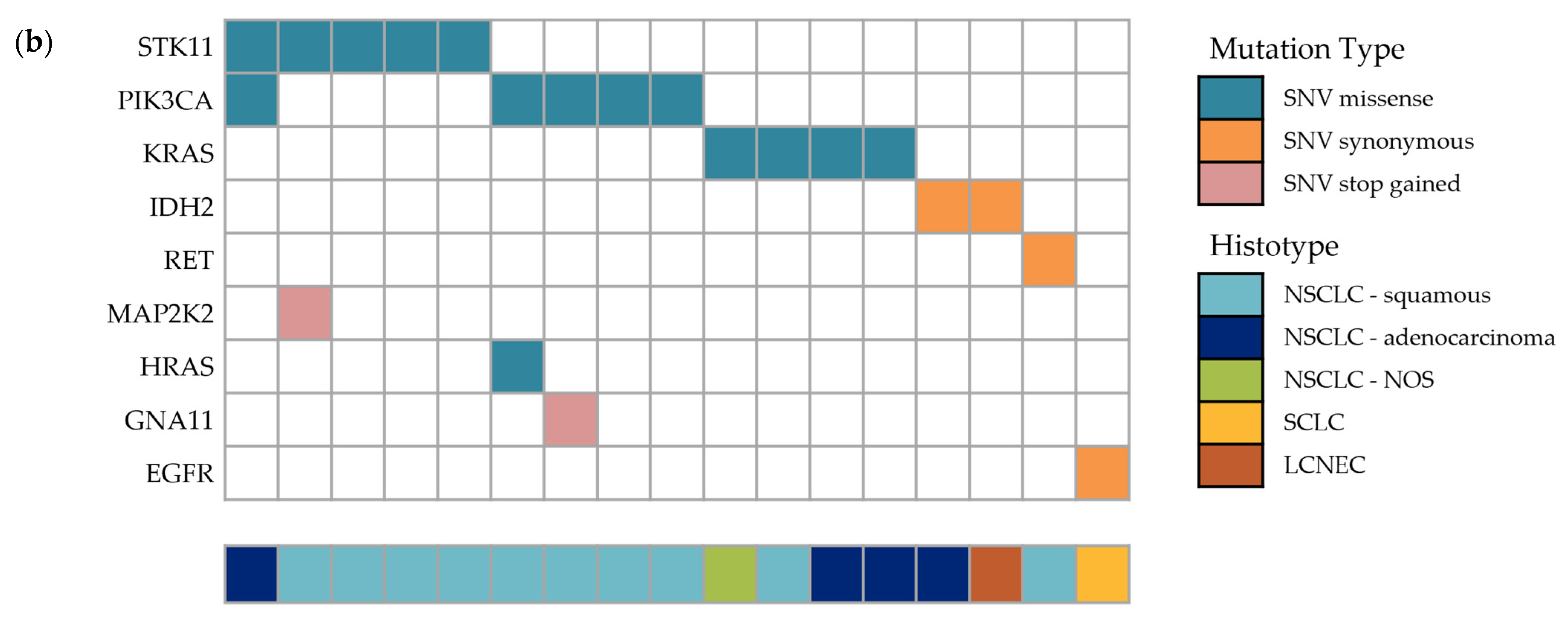
3.4. Genomic Analysis Highlights Missense Mutations in STK11, PIK3CA and KRAS
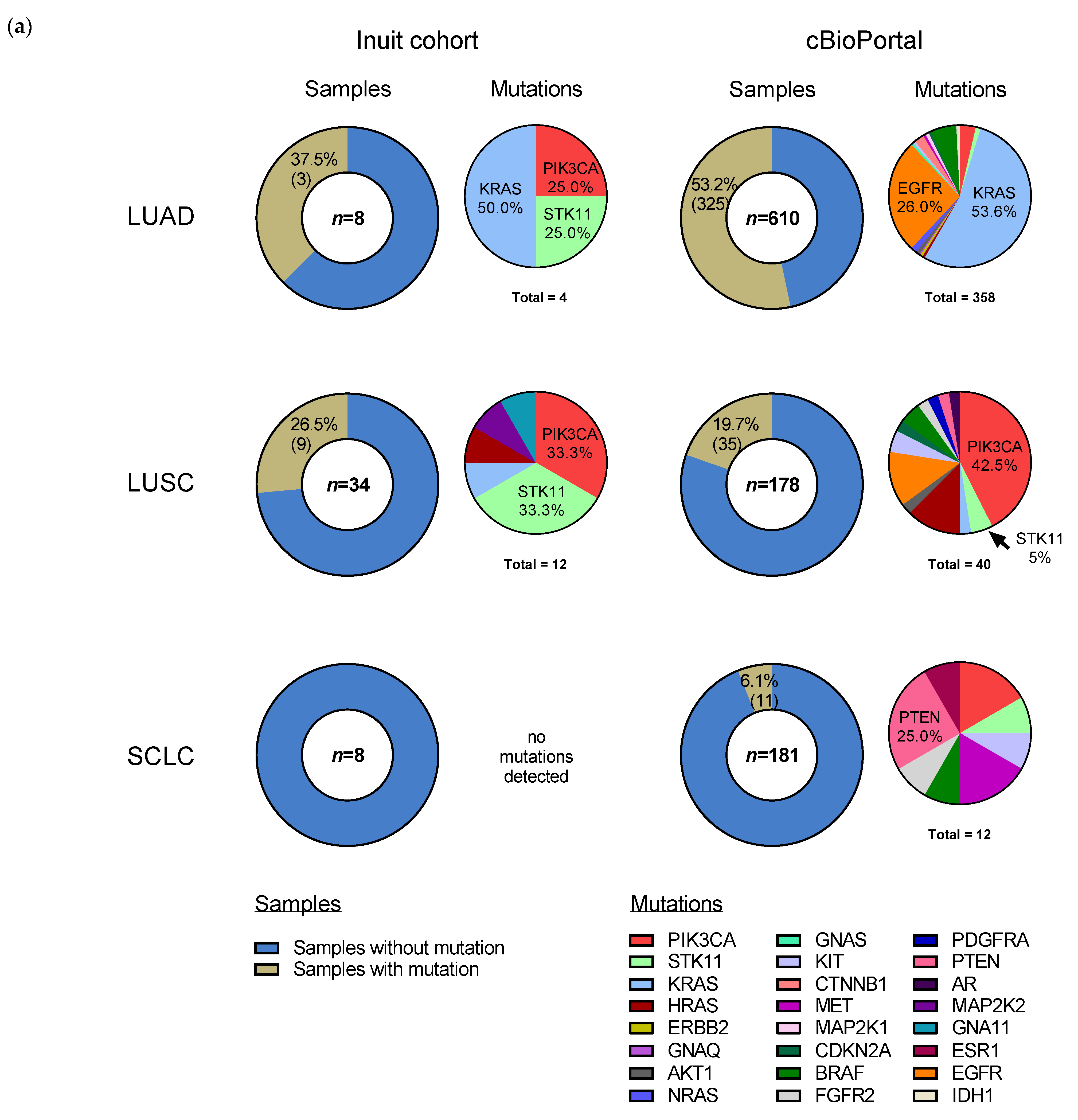
3.5. Somatic Mutation Profile from Genomic Analysis Varies by Histology and Is Similar to cBioPortal Data
4. Discussion
4.1. The Elevated Prevalence of SCC Histology Is Consistent with Determinants of Health Affecting This Cohort/Population
4.2. Genomic Analysis Shows Similar Mutational Profiles in Each Histological Subtype When Compared to cBioPortal Data
4.3. STK11 F354L Mutation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Statistics Canada. Available online: https://www150.statcan.gc.ca/n1/en/catalogue/99-011-X2011001 (accessed on 15 March 2022).
- Young, T.K.; Kelly, J.J.; Friborg, J.; Soininen, L.; Wong, K.O. Cancer among Circumpolar Populations: An Emerging Public Health Concern. Int. J. Circumpolar Health 2016, 75, 29787. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer. Available online: https://www.iarc.who.int/news-events/latest-world-cancer-statistics-globocan-2012-estimated-cancer-incidence-mortality-and-prevalence-worldwide-in-2012/ (accessed on 15 March 2022).
- Ontario Local Health Integration Network Champlain. Available online: http://healthcareathome.ca/champlain/en/Documents/Reports%2C%20Plans%20and%20Agreements/201819ABPEN%20%282%29.pdf (accessed on 15 March 2022).
- Statistics Canada. Available online: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/prof/details/Page.cfm?Lang=E&Geo1=PR&Code1=62&Geo2=&Code2=&SearchText=Nunavut&SearchType=Begins&SearchPR=01&B1=All&GeoLevel=PR&GeoCode=62&type=0 (accessed on 15 March 2022).
- Asmis, T.R.; Febbraro, M.; Alvarez, G.G.; Spaans, J.N.; Ruta, M.; Lalany, A.; Osborne, G.; Goss, G.D. A Retrospective Review of Cancer Treatments and Outcomes among Inuit Referred from Nunavut, Canada. Curr. Oncol. 2015, 22, 246–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houston, K.A.; Henley, S.J.; Li, J.; White, M.C.; Richards, T.B. Patterns in Lung Cancer Incidence Rates and Trends by Histologic Type in the United States, 2004–2009. Lung Cancer 2014, 86, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travis, W.; Brambilla, E.; Burke, A.; Marx, A.; Nicholson, A. WHO Classification of the Tumours of the Lung, Pleura, Thymus and Heart, 4th ed.; IARC Press: Lyon, France, 2015; Volume 7, pp. 150–190. [Google Scholar]
- Pesch, B.; Kendzia, B.; Gustavsson, P.; Jöckel, K.-H.; Johnen, G.; Pohlabeln, H.; Olsson, A.; Ahrens, W.; Gross, I.M.; Brüske, I.; et al. Cigarette Smoking and Lung Cancer-Relative Risk Estimates for the Major Histological Types from a Pooled Analysis of Case-Control Studies. Int. J. Cancer 2012, 131, 1210–1219. [Google Scholar] [CrossRef]
- Ho, C.; Tong, K.M.; Ramsden, K.; Ionescu, D.N.; Laskin, J. Histologic Classification of Non-Small-Cell Lung Cancer over Time: Reducing the Rates of Not-Otherwise-Specified. Curr. Oncol. 2015, 22, 164–170. [Google Scholar] [CrossRef] [Green Version]
- Devesa, S.S.; Shaw, G.L.; Blot, W.J. Changing Patterns of Lung Cancer Incidence by Histological Type. Cancer Epidemiol. Biomark. Prev. 1991, 1, 29–34. [Google Scholar]
- The Cancer Genome Atlas Research Network Comprehensive Genomic Characterization of Squamous Cell Lung Cancers. Nature 2012, 489, 519–525. [CrossRef]
- The Cancer Genome Atlas Research Network Comprehensive Molecular Profiling of Lung Adenocarcinoma. Nature 2014, 511, 543–550. [CrossRef]
- Shaw, A.T.; Kim, D.-W.; Nakagawa, K.; Seto, T.; Crinó, L.; Ahn, M.-J.; De Pas, T.; Besse, B.; Solomon, B.J.; Blackhall, F.; et al. Crizotinib versus Chemotherapy in Advanced ALK -Positive Lung Cancer. N. Engl. J. Med. 2013, 368, 2385–2394. [Google Scholar] [CrossRef] [Green Version]
- Shepherd, F.A.; Rodrigues Pereira, J.; Ciuleanu, T.; Tan, E.H.; Hirsh, V.; Thongprasert, S.; Campos, D.; Maoleekoonpiroj, S.; Smylie, M.; Martins, R.; et al. Erlotinib in Previously Treated Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2005, 353, 123–132. [Google Scholar] [CrossRef] [Green Version]
- Lynch, T.J.; Bell, D.W.; Sordella, R.; Gurubhagavatula, S.; Okimoto, R.A.; Brannigan, B.W.; Harris, P.L.; Haserlat, S.M.; Supko, J.G.; Haluska, F.G.; et al. Activating Mutations in the Epidermal Growth Factor Receptor Underlying Responsiveness of Non–Small-Cell Lung Cancer to Gefitinib. N. Engl. J. Med. 2004, 350, 2129–2139. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Kim, D.-W.; Mehra, R.; Tan, D.S.W.; Felip, E.; Chow, L.Q.M.; Camidge, D.R.; Vansteenkiste, J.; Sharma, S.; De Pas, T.; et al. Ceritinib in ALK -Rearranged Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2014, 370, 1189–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Planchard, D.; Smit, E.F.; Groen, H.J.M.; Mazieres, J.; Besse, B.; Helland, Å.; Giannone, V.; D’Amelio, A.M.; Zhang, P.; Mookerjee, B.; et al. Dabrafenib plus Trametinib in Patients with Previously Untreated BRAFV600E-Mutant Metastatic Non-Small-Cell Lung Cancer: An Open-Label, Phase 2 Trial. Lancet Oncol. 2017, 18, 1307–1316. [Google Scholar] [CrossRef]
- Midha, A.; Dearden, S.; McCormack, R. EGFR Mutation Incidence in Non-Small-Cell Lung Cancer of Adenocarcinoma Histology: A Systematic Review and Global Map by Ethnicity (MutMapII). Am. J. Cancer Res. 2015, 5, 2892–2911. [Google Scholar] [PubMed]
- Bollig-Fischer, A.; Chen, W.; Gadgeel, S.M.; Wenzlaff, A.S.; Cote, M.L.; Schwartz, A.G.; Bepler, G. Racial Diversity of Actionable Mutations in Non–Small Cell Lung Cancer. J. Thorac. Oncol. 2015, 10, 250–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biankin, A.V.; Piantadosi, S.; Hollingsworth, S.J. Patient-Centric Trials for Therapeutic Development in Precision Oncology. Nature 2015, 526, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191. [Google Scholar] [CrossRef] [Green Version]
- Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada and SS and HRC of C. Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans. Available online: http://www.pre.ethics.gc.ca/pdf/eng/tcps2-2014/TCPS_2_FINAL_Web.pdf (accessed on 4 May 2017).
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [Green Version]
- Contextual Genomics Press Release: Contextual Genomics and the Personalized Medicine Initiative Launch Phase 2 Testing of Its National Access Program Cancer Genomics Test. Available online: https://contextualgenomics.com/2016/03/14/contextual-genomics-personalized-medicine-initiative-launch-phase-2-testing-national-access-program-cancer-genomics-test/ (accessed on 15 March 2019).
- Harismendy, O.; Schwab, R.B.; Bao, L.; Olson, J.; Rozenzhak, S.; Kotsopoulos, S.K.; Pond, S.; Crain, B.; Chee, M.S.; Messer, K.; et al. Detection of Low Prevalence Somatic Mutations in Solid Tumors with Ultra-Deep Targeted Sequencing. Genome Biol. 2011, 12, R124. [Google Scholar] [CrossRef] [Green Version]
- Ding, J.; Bashashati, A.; Roth, A.; Oloumi, A.; Tse, K.; Zeng, T.; Haffari, G.; Hirst, M.; Marra, M.A.; Condon, A.; et al. Feature-Based Classifiers for Somatic Mutation Detection in Tumour–Normal Paired Sequencing Data. Bioinformatics 2012, 28, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.; Aksoy, B.A.; Dogrusoz, U.; Dresdner, G.; Gross, B.; Sumer, S.O.; Sun, Y.; Jacobsen, A.; Sinha, R.; Larsson, E.; et al. Integrative Analysis of Complex Cancer Genomics and Clinical Profiles Using the CBioPortal. Sci. Signal. 2013, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Agency for Research on Cancer. Cancer Incidence in Five Continents, Vol. IX; Curado, M., Edwards, B., Shin, H., Storm, H., Ferlay, J., Heanue, M., Boyle, P., Eds.; IARC Scientific Publications: Lyon, France, 2007; ISBN 978 92 832 2160 9. [Google Scholar]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The CBio Cancer Genomics Portal: An Open Platform for Exploring Multidimensional Cancer Genomics Data: Figure 1. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youlden, D.R.; Cramb, S.M.; Baade, P.D. The International Epidemiology of Lung Cancer: Geographical Distribution and Secular Trends. J. Thorac. Oncol. 2008, 3, 819–831. [Google Scholar] [CrossRef] [PubMed]
- Lortet-Tieulent, J.; Soerjomataram, I.; Ferlay, J.; Rutherford, M.; Weiderpass, E.; Bray, F. International Trends in Lung Cancer Incidence by Histological Subtype: Adenocarcinoma Stabilizing in Men but Still Increasing in Women. Lung Cancer 2014, 84, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Government of Nunavut Lung Cancer. Available online: http://www.gov.nu.ca/health/information/health-statistics (accessed on 3 April 2017).
- Sun, S.; Schiller, J.H.; Gazdar, A.F. Lung Cancer in Never Smokers—A Different Disease. Nat. Rev. Cancer 2007, 7, 778–790. [Google Scholar] [CrossRef]
- Kenfield, S.A.; Wei, E.K.; Stampfer, M.J.; Rosner, B.A.; Colditz, G.A. Comparison of Aspects of Smoking among the Four Histological Types of Lung Cancer. Tob. Control 2008, 17, 198–204. [Google Scholar] [CrossRef]
- Friborg, J.T.; Melbye, M. Cancer Patterns in Inuit Populations. Lancet Oncol. 2008, 9, 892–900. [Google Scholar] [CrossRef]
- Bougie, E.; Kohen, D. Smoking Prevalence among Inuit in Canada. Health Rep. 2017, 28, 10–14. [Google Scholar]
- Office of the Chief Medical Officer of Health. Available online: https://www.gov.nu.ca/sites/default/files/files/health_profile_nunavut.pdf (accessed on 15 March 2022).
- Physicians for a Smoke-Free Canada. Available online: http://www.smoke-free.ca/pdf_1/2011/Canada-2010-smokingratesbyprovince.pdf (accessed on 15 March 2022).
- Weiss, W. Cigarette Smoking and Lung Cancer Trends. A Light at the End of the Tunnel? Chest 1997, 111, 1414–1416. [Google Scholar] [CrossRef] [Green Version]
- Office of the Chief Medical Officer of Health. Available online: https://www.gov.nu.ca/sites/default/files/nu_communicable_diseases_manual_-_complete_2020apr.pdf (accessed on 15 March 2022).
- Brenner, D.R.; McLaughlin, J.R.; Hung, R.J. Previous Lung Diseases and Lung Cancer Risk: A Systematic Review and Meta-Analysis. PLoS ONE 2011, 6, e17479. [Google Scholar] [CrossRef]
- Wu, C.-Y.; Hu, H.-Y.; Pu, C.-Y.; Huang, N.; Shen, H.-C.; Li, C.-P.; Chou, Y.-J. Pulmonary Tuberculosis Increases the Risk of Lung Cancer: A Population-Based Cohort Study. Cancer 2011, 117, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Skillrud, D.M.; Offord, K.; Miller, R. Higher Risk of Lung Cancer in Chronic Obstructive Pulmonary Disease: A Prospective, Matched, Controlled Study. Ann. Intern. Med. 1986, 105, 503. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.-H.; Liao, C.-C.; Hsu, W.-H.; Chen, H.-J.; Liao, W.-C.; Muo, C.-H.; Sung, F.-C.; Chen, C.-Y. Increased Lung Cancer Risk among Patients with Pulmonary Tuberculosis: A Population Cohort Study. J. Thorac. Oncol. 2011, 6, 32–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nalbandian, A.; Yan, B.-S.; Pichugin, A.; Bronson, R.T.; Kramnik, I. Lung Carcinogenesis Induced by Chronic Tuberculosis Infection: The Experimental Model and Genetic Control. Oncogene 2009, 28, 1928–1938. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Cespedes, M.; Parrella, P.; Esteller, M.; Nomoto, S.; Trink, B.; Engles, J.M.; Westra, W.H.; Herman, J.G.; Sidransky, D. Inactivation of LKB1/STK11 Is a Common Event in Adenocarcinomas of the Lung. Cancer Res. 2002, 62, 3659–3662. [Google Scholar]
- Avizienyte, E.; Loukola, A.; Roth, S.; Hemminki, A.; Tarkkanen, M.; Salovaara, R.; Arola, J.; Bützow, R.; Husgafvel-Pursiainen, K.; Kokkola, A.; et al. LKB1 Somatic Mutations in Sporadic Tumors. Am. J. Pathol. 1999, 154, 677–681. [Google Scholar] [CrossRef] [Green Version]
- Koivunen, J.P.; Kim, J.; Lee, J.; Rogers, A.M.; Park, J.O.; Zhao, X.; Naoki, K.; Okamoto, I.; Nakagawa, K.; Yeap, B.Y.; et al. Mutations in the LKB1 Tumour Suppressor Are Frequently Detected in Tumours from Caucasian but Not Asian Lung Cancer Patients. Br. J. Cancer 2008, 99, 245–252. [Google Scholar] [CrossRef]
- Matsumoto, S.; Iwakawa, R.; Takahashi, K.; Kohno, T.; Nakanishi, Y.; Matsuno, Y.; Suzuki, K.; Nakamoto, M.; Shimizu, E.; Minna, J.D.; et al. Prevalence and Specificity of LKB1 Genetic Alterations in Lung Cancers. Oncogene 2007, 26, 5911–5918. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Hua, X.; Zhu, B.; Ravichandran, S.; Wang, M.; Nguyen, C.; Brodie, S.A.; Palleschi, A.; Alloisio, M.; Pariscenti, G.; et al. Somatic Genomics and Clinical Features of Lung Adenocarcinoma: A Retrospective Study. PLoS Med. 2016, 13, e1002162. [Google Scholar] [CrossRef]
- Onozato, R.; Kosaka, T.; Achiwa, H.; Kuwano, H.; Takahashi, T.; Yatabe, Y.; Mitsudomi, T. LKB1 Gene Mutations in Japanese Lung Cancer Patients. Cancer Sci. 2007, 98, 1747–1751. [Google Scholar] [CrossRef]
- Ji, H.; Ramsey, M.R.; Hayes, D.N.; Fan, C.; McNamara, K.; Kozlowski, P.; Torrice, C.; Wu, M.C.; Shimamura, T.; Perera, S.A.; et al. LKB1 Modulates Lung Cancer Differentiation and Metastasis. Nature 2007, 448, 807–810. [Google Scholar] [CrossRef] [PubMed]
- Launonen, V.; Avizienyte, E.; Loukola, A.; Laiho, P.; Salovaara, R.; Järvinen, H.; Mecklin, J.P.; Oku, A.; Shimane, M.; Kim, H.C.; et al. No Evidence of Peutz-Jeghers Syndrome Gene LKB1 Involvement in Left-Sided Colorectal Carcinomas. Cancer Res. 2000, 60, 546–548. [Google Scholar] [PubMed]
- Stražišar, M.; Mlakar, V.; Rott, T.; Glavač, D. Somatic Alterations of the Serine/Threonine Kinase LKB1 Gene in Squamous Cell (SCC) and Large Cell (LCC) Lung Carcinoma. Cancer Investig. 2009, 27, 407–416. [Google Scholar] [CrossRef]
- Chen, L.; Engel, B.E.; Welsh, E.A.; Yoder, S.J.; Brantley, S.G.; Chen, D.-T.; Beg, A.A.; Cao, C.; Kaye, F.J.; Haura, E.B.; et al. A Sensitive NanoString-Based Assay to Score STK11 (LKB1) Pathway Disruption in Lung Adenocarcinoma. J. Thorac. Oncol. 2016, 11, 838–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forcet, C.; Etienne-Manneville, S.; Gaude, H.; Fournier, L.; Debilly, S.; Salmi, M.; Baas, A.; Olschwang, S.; Clevers, H.; Billaud, M. Functional Analysis of Peutz–Jeghers Mutations Reveals That the LKB1 C-Terminal Region Exerts a Crucial Role in Regulating Both the AMPK Pathway and the Cell Polarity. Hum. Mol. Genet. 2005, 14, 1283–1292. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Men n = 60 | Women n = 38 | Total n = 98 | |||
|---|---|---|---|---|---|---|
| Age, y | ||||||
| Median | 66 | 66 | 66 | |||
| Range | 35–82 | 44–87 | 35–87 | |||
| Tobacco use history, n (%) | ||||||
| Current | 35 | (58) | 18 | (47) | 53 | (54) |
| Previous | 18 | (30) | 14 | (37) | 32 | (33) |
| Never | 0 | (0) | 1 | (3) | 1 | (1) |
| Unknown | 7 | (12) | 5 | (13) | 12 | (12) |
| History of lung disease, n (%) | ||||||
| Reported (any) | 40 | (67) | 28 | (74) | 68 | (69) |
| Tuberculosis | 27 | (45) | 19 | (50) | 46 | (47) |
| Other lung disease (i.e., pneumonia, COPD, etc.) | 27 | (45) | 24 | (63) | 51 | (52) |
| Stage at diagnosis, n (%) | ||||||
| Solid tumor 1, n | 52 | 30 | 82 | |||
| I | 3 | (6) | 6 | (20) | 9 | (11) |
| II | 2 | (4) | 1 | (3) | 3 | (4) |
| III | 20 | (38) | 10 | (33) | 30 | (37) |
| IV | 26 | (50) | 12 | (40) | 38 | (46) |
| Unknown | 1 | (2) | 1 | (3) | 2 | (2) |
| Pathology/histology, n (%) | ||||||
| Non-Small Cell Lung Cancer (NSCLC) | 50 | (83) | 29 | (76) | 79 | (81) |
| Adenocarcinoma | 6 | (10) | 10 | (26) | 16 | (16) |
| Squamous Cell | 34 | (57) | 17 | (45) | 51 | (52) |
| NOS | 10 | (17) | 2 | (5) | 12 | (12) |
| Small Cell NEC (SCLC) | 8 | (13) | 8 | (21) | 16 | (16) |
| Large Cell NEC (LCNEC) | 1 | (2) | 1 | (3) | 2 | (2) |
| Carcinoma, undifferentiated | 1 | (2) | 0 | (0) | 1 | (1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goss, G.D.; Spaans, J.N.; Huntsman, D.; Asmis, T.; Andrews Wright, N.M.; Duciaume, M.; Kaurah, P.; Miller, R.R.; Banerji, S.; Sekhon, H.S.; et al. Histologic and Genotypic Characterization of Lung Cancer in the Inuit Population of the Eastern Canadian Arctic. Curr. Oncol. 2022, 29, 3171-3186. https://doi.org/10.3390/curroncol29050258
Goss GD, Spaans JN, Huntsman D, Asmis T, Andrews Wright NM, Duciaume M, Kaurah P, Miller RR, Banerji S, Sekhon HS, et al. Histologic and Genotypic Characterization of Lung Cancer in the Inuit Population of the Eastern Canadian Arctic. Current Oncology. 2022; 29(5):3171-3186. https://doi.org/10.3390/curroncol29050258
Chicago/Turabian StyleGoss, Glenwood D., Johanna N. Spaans, David Huntsman, Timothy Asmis, Natalie M. Andrews Wright, Marc Duciaume, Pardeep Kaurah, Ruth R. Miller, Shantanu Banerji, Harmanjatinder S. Sekhon, and et al. 2022. "Histologic and Genotypic Characterization of Lung Cancer in the Inuit Population of the Eastern Canadian Arctic" Current Oncology 29, no. 5: 3171-3186. https://doi.org/10.3390/curroncol29050258