Prognostic Impact of Resection Margin Status on Distal Pancreatectomy for Ductal Adenocarcinoma


Abstract
:1. Introduction
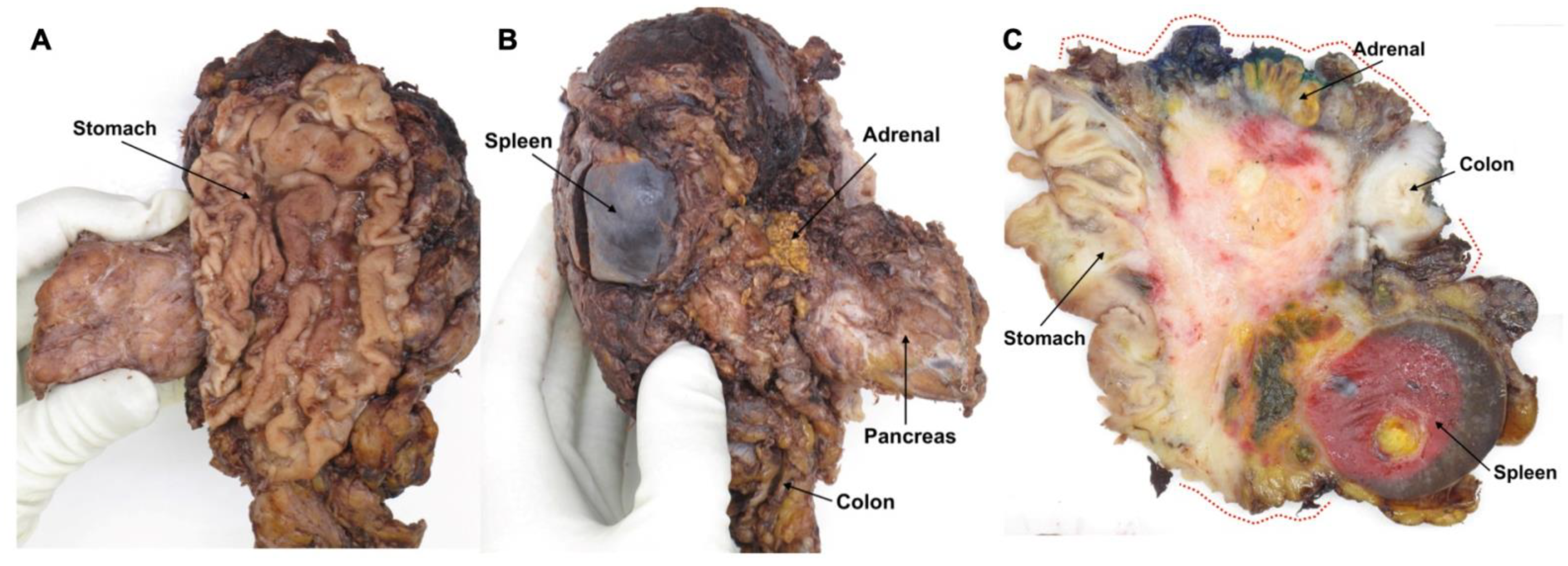
2. Pathology Examination of the Margin Status—Specimen Grossing
3. Pathology Examination of the Margin Status—Microscopic Examination
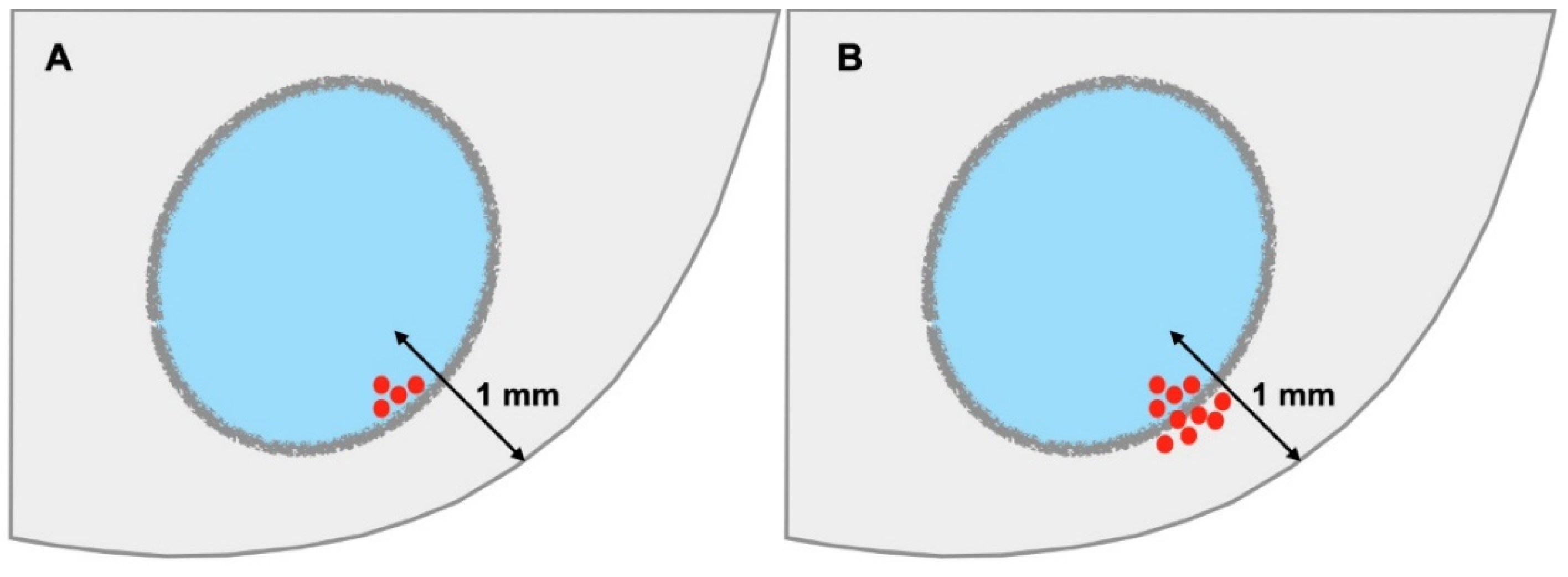
3.1. Definition of R1
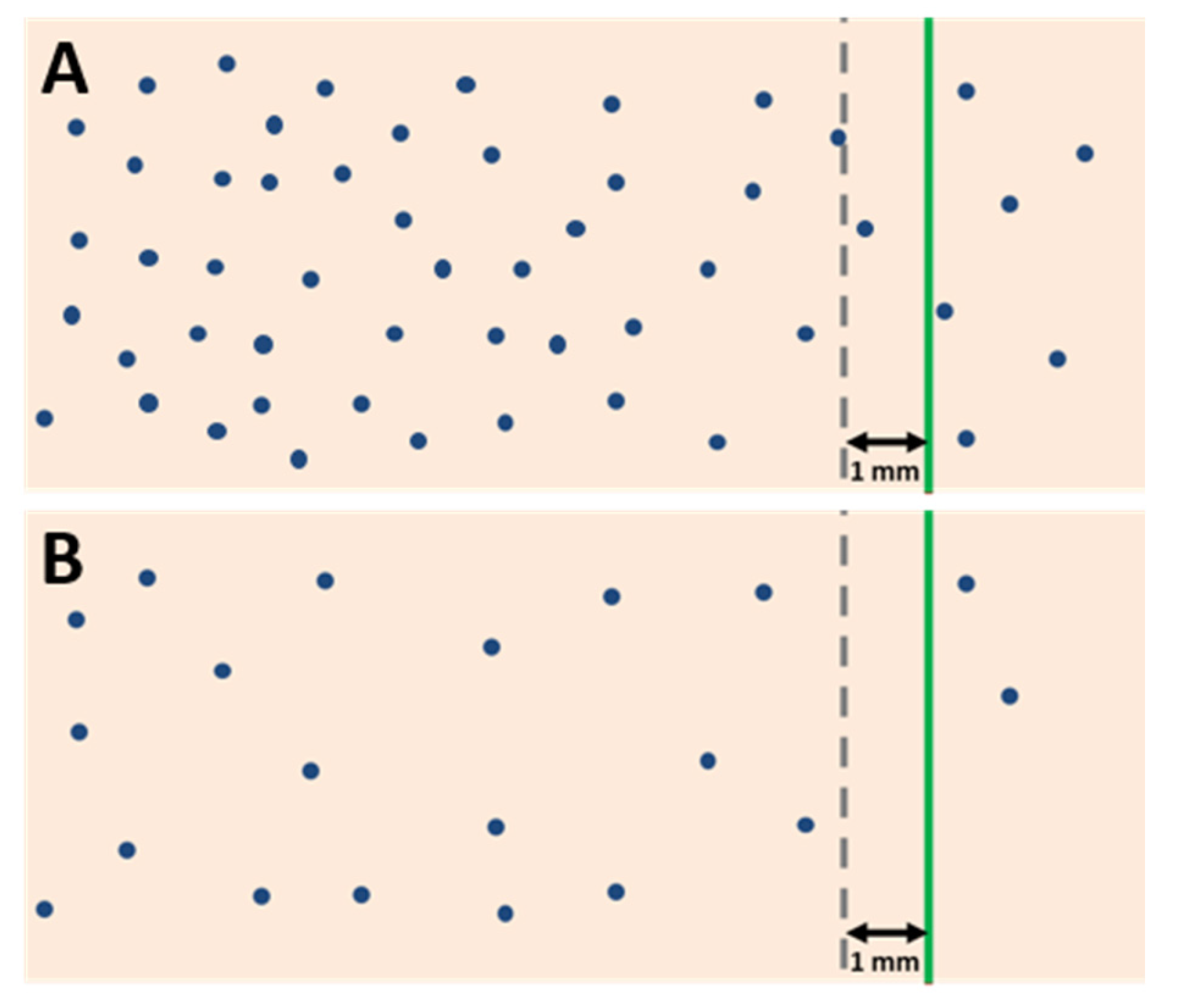
3.2. R1 and the Mode of Cancer Spread Close to a Margin
4. Prognostic Impact of Resection Margin Status in Distal Pancreatectomy
4.1. Limitations of Current Published Data
4.2. Burden of Residual Disease and Time to Recurrence
4.3. Prognostic Impact of R1 at Specific Margins
4.4. Involvement of the Anterior Surface
4.5. Prognostic Impact of Resection Margin Status on Extended Distal Pancreatectomy
5. Resection Margin Status and Neoadjuvant Treatment
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Strobel, O.; Neoptolemos, J.; Jäger, D.; Büchler, M.W. Optimizing the outcomes of pancreatic cancer surgery. Nat. Rev. Clin. Oncol. 2019, 16, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Niesen, W.; Hank, T.; Büchler, M.; Strobel, O. Local radicality and survival outcome of pancreatic cancer surgery. Ann. Gastroenterol. Surg. 2019, 3, 464–475. [Google Scholar] [CrossRef] [PubMed]
- Chandrasegaram, M.D.; Goldstein, D.; Simes, J.; Gebski, V.; Kench, J.G.; Gill, A.J.; Samra, J.S.; Merrett, N.D.; Richardson, A.J.; Barbour, A.P. Meta-analysis of radical resection rates and margin assessment in pancreatic cancer. Br. J. Surg. 2015, 102, 1459–1472. [Google Scholar] [CrossRef] [PubMed]
- Verbeke, C.S.; Menon, K.V. Redefining resection margin status in pancreatic cancer. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2009, 11, 282–289. [Google Scholar] [CrossRef]
- Leonhardt, C.S.; Niesen, W.; Kalkum, E.; Klotz, R.; Hank, T.; Büchler, M.W.; Strobel, O.; Probst, P. Prognostic relevance of the revised R status definition in pancreatic cancer: Meta-analysis. BJS Open 2022, 6, zrac010. [Google Scholar] [CrossRef]
- Tomasello, G.; Ghidini, M.; Costanzo, A.; Ghidini, A.; Russo, A.; Barni, S.; Passalacqua, R.; Petrelli, F. Outcome of head compared to body and tail pancreatic cancer: A systematic review and meta-analysis of 93 studies. J. Gastrointest. Oncol. 2019, 10, 259–269. [Google Scholar] [CrossRef]
- Sahakyan, M.A.; Verbeke, C.S.; Tholfsen, T.; Ignjatovic, D.; Kleive, D.; Buanes, T.; Lassen, K.; Røsok, B.I.; Labori, K.J.; Edwin, B. Prognostic Impact of Resection Margin Status in Distal Pancreatectomy for Ductal Adenocarcinoma. Ann. Surg. Oncol. 2022, 29, 366–375. [Google Scholar] [CrossRef]
- Verbeke, C.S.; Leitch, D.; Menon, K.V.; McMahon, M.J.; Guillou, P.J.; Anthoney, A. Redefining the R1 resection in pancreatic cancer. Br. J. Surg. 2006, 93, 1232–1237. [Google Scholar] [CrossRef]
- Lof, S.; Rajak, R.; Vissers, F.; Korrel, M.; Bateman, A.; Verheij, J.; Verbeke, C.; Cataldo, I.; Besselink, M.G.; Abu Hilal, M. DIPLOMA Approach for Standardized Pathology Assessment of Distal Pancreatectomy Specimens. J. Vis. Exp. 2020, 156, e60343. [Google Scholar] [CrossRef]
- College of American Pathologists (CAP). Protocol for the Examination of Specimens from Patients with Carcinoma of the Pancreas. 2021. Available online: https://documents.cap.org/protocols/Panc.Exo_4.2.0.2.REL_CAPCP.pdf (accessed on 4 July 2022).
- Kakar, S.; Pawlik, T.M.; Allen, P.J.; Vauthey, J.N. AJCC Cancer Staging Manual, 8th ed.; Amin, M.B., Edge, S.B., Greene, F.L., Byrd, D.R., Brookland, R.K., Washington, M.K., Gershenwald, J.E., Compton, C.C., Hess, K.R., Sullivan, D.C., Eds.; American Joint Committee on Cancer: Chicago, IL, USA, 2017; pp. 337–347. [Google Scholar]
- NCCN Guidelines version 2.2021. Pancreatic Adenocarcinoma. Available online: https://www.nccn.org/professionals/physician_gls/pdf/pancreatic_blocks.pdf (accessed on 14 June 2022).
- The Royal College of Pathologists of Australasia (RCPA). Cancer of the Exocrine Pancreas, Ampulla of Vater and Distal Common Bile Duct. Structured Reporting Protocol (2nd ed.). 2020. Available online: https://www.rcpa.edu.au/Library/Practising-Pathology/Structured-Pathology-Reporting-of-Cancer/Cancer-Protocols/Gastrointestinal/Protocol-pancreatic-cancer.aspx (accessed on 4 July 2022).
- The Royal College of Pathologists. Dataset for the Histopathological Reporting of Carcinoma of the Pancreas, Ampulla of Vater and Common Bileduct. 2019. Available online: https://www.rcpath.org/uploads/assets/34910231-c106-4629-a2de9e9ae6f87ac1/G091-Dataset-for-histopathological-reporting-of-carcinomas-of-the-pancreas-ampulla-of-Vater-and-common-bile-duct.pdf (accessed on 4 July 2022).
- Verbeke, C.B.; Brosens, L.; Campbell, F.; Del Chiaro, M.; Esposito, I.; Feakins, R.M.; Fukushima, N.; Gill, A.; Kakar, S.; Kench, J.; et al. Carinoma of the Exocrine Pancreas Histopathology Reporting Guide; International Collaboration on Cancer Reporting: Sydney, NAW, Australia, 2020; ISBN 978-1-922324-03-0. [Google Scholar]
- Korrel, M.; Lof, S.; van Hilst, J.; Alseidi, A.; Boggi, U.; Busch, O.R.; van Dieren, S.; Edwin, B.; Fuks, D.; Hackert, T.; et al. Predictors for Survival in an International Cohort of Patients Undergoing Distal Pancreatectomy for Pancreatic Ductal Adenocarcinoma. Ann. Surg. Oncol. 2021, 28, 1079–1087. [Google Scholar] [CrossRef]
- de Rooij, T.; Tol, J.A.; van Eijck, C.H.; Boerma, D.; Bonsing, B.A.; Bosscha, K.; van Dam, R.M.; Dijkgraaf, M.G.; Gerhards, M.F.; van Goor, H.; et al. Outcomes of Distal Pancreatectomy for Pancreatic Ductal Adenocarcinoma in the Netherlands: A Nationwide Retrospective Analysis. Ann. Surg. Oncol. 2016, 23, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Paye, F.; Micelli Lupinacci, R.; Bachellier, P.; Boher, J.M.; Delpero, J.R. Distal pancreatectomy for pancreatic carcinoma in the era of multimodal treatment. Br. J. Surg. 2015, 102, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Panzeri, F.; Marchegiani, G.; Malleo, G.; Malpaga, A.; Maggino, L.; Marchese, T.; Salvia, R.; Bassi, C.; Butturini, G. Distal pancreatectomy associated with multivisceral resection: Results from a single centre experience. Langenbeck’s Arch. Surg. 2017, 402, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Roch, A.M.; Singh, H.; Turner, A.P.; Ceppa, E.P.; House, M.G.; Zyromski, N.J.; Nakeeb, A.; Schmidt, C.M. Extended distal pancreatectomy for pancreatic adenocarcinoma with splenic vein thrombosis and/or adjacent organ invasion. Am. J. Surg. 2015, 209, 564–569. [Google Scholar] [CrossRef]
- Sahakyan, M.A.; Kleive, D.; Kazaryan, A.M.; Aghayan, D.L.; Ignjatovic, D.; Labori, K.J.; Røsok, B.I.; Edwin, B. Extended laparoscopic distal pancreatectomy for adenocarcinoma in the body and tail of the pancreas: A single-center experience. Langenbeck’s Arch. Surg. 2018, 403, 941–948. [Google Scholar] [CrossRef]
- Brierly, J.D.; Gospodarowicz, M.K.; Wittekind, D. UICC: TNM Classification of Malignant Tumors, 8th ed.; Wiley-Blackwell: Oxford, UK, 2017; pp. 93–95. [Google Scholar]
- Chang, D.K.; Johns, A.L.; Merrett, N.D.; Gill, A.J.; Colvin, E.K.; Scarlett, C.J.; Nguyen, N.Q.; Leong, R.W.; Cosman, P.H.; Kelly, M.I.; et al. Margin clearance and outcome in resected pancreatic cancer. J. Clin. Oncol.Off. J. Am. Soc. Clin. Oncol. 2009, 27, 2855–2862. [Google Scholar] [CrossRef]
- Jamieson, N.B.; Chan, N.I.; Foulis, A.K.; Dickson, E.J.; McKay, C.J.; Carter, C.R. The prognostic influence of resection margin clearance following pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2013, 17, 511–521. [Google Scholar] [CrossRef]
- Osipov, A.; Nissen, N.; Rutgers, J.; Dhall, D.; Naziri, J.; Chopra, S.; Li, Q.; Hendifar, A.E.; Tuli, R. Redefining the Positive Margin in Pancreatic Cancer: Impact on Patterns of Failure, Long-Term Survival and Adjuvant Therapy. Ann. Surg. Oncol. 2017, 24, 3674–3682. [Google Scholar] [CrossRef]
- Verbeke, C.S.; Knapp, J.; Gladhaug, I.P. Tumour growth is more dispersed in pancreatic head cancers than in rectal cancer: Implications for resection margin assessment. Histopathology 2011, 59, 1111–1121. [Google Scholar] [CrossRef]
- Weyhe, D.; Obonyo, D.; Uslar, V.N.; Stricker, I.; Tannapfel, A. Predictive factors for long-term survival after surgery for pancreatic ductal adenocarcinoma: Making a case for standardized reporting of the resection margin using certified cancer center data. PLoS ONE 2021, 16, e0248633. [Google Scholar]
- Sohn, H.J.; Kim, H.; Kim, S.J.; Lee, K.B.; Han, Y.; Lee, J.M.; Kang, J.S.; Kwon, W.; Chie, E.K.; Kim, H.; et al. Oncologic outcomes according to the location and status of resection margin in pancreas head cancer: Role of radiation therapy in R1 resection. Ann. Surg. Treat. Res. 2022, 102, 10–19. [Google Scholar] [CrossRef]
- Crippa, S.; Giannone, F.; Schiavo Lena, M.; Belfiori, G.; Partelli, S.; Tamburrino, D.; Delpini, R.; Pagnanelli, M.; Pecorelli, N.; Balzano, G.; et al. R Status is a Relevant Prognostic Factor for Recurrence and Survival After Pancreatic Head Resection for Ductal Adenocarcinoma. Ann. Surg. Oncol. 2021, 28, 4602–4612. [Google Scholar] [CrossRef]
- Strobel, O.; Hank, T.; Hinz, U.; Bergmann, F.; Schneider, L.; Springfeld, C.; Jäger, D.; Schirmacher, P.; Hackert, T.; Büchler, M.W. Pancreatic Cancer Surgery: The New R-status Counts. Ann. Surg. 2017, 265, 565–573. [Google Scholar] [CrossRef]
- Hank, T.; Hinz, U.; Tarantino, I.; Kaiser, J.; Niesen, W.; Bergmann, F.; Hackert, T.; Büchler, M.W.; Strobel, O. Validation of at least 1 mm as cut-off for resection margins for pancreatic adenocarcinoma of the body and tail. Br. J. Surg. 2018, 105, 1171–1181. [Google Scholar] [CrossRef]
- Demir, I.E.; Jäger, C.; Schlitter, A.M.; Konukiewitz, B.; Stecher, L.; Schorn, S.; Tieftrunk, E.; Scheufele, F.; Calavrezos, L.; Schirren, R.; et al. R0 Versus R1 Resection Matters after Pancreaticoduodenectomy, and Less after Distal or Total Pancreatectomy for Pancreatic Cancer. Ann. Surg. 2018, 268, 1058–1068. [Google Scholar] [CrossRef]
- Sahakyan, M.A.; Kim, S.C.; Kleive, D.; Kazaryan, A.M.; Song, K.B.; Ignjatovic, D.; Buanes, T.; Røsok, B.I.; Labori, K.J.; Edwin, B. Laparoscopic distal pancreatectomy for pancreatic ductal adenocarcinoma: Long-term oncologic outcomes after standard resection. Surgery 2017, 162, 802–811. [Google Scholar] [CrossRef]
- Yamamoto, J.; Saiura, A.; Koga, R.; Seki, M.; Katori, M.; Kato, Y.; Sakamoto, Y.; Kokudo, N.; Yamaguchi, T. Improved survival of left-sided pancreas cancer after surgery. Jpn. J. Clin. Oncol. 2010, 40, 530–536. [Google Scholar] [CrossRef]
- Shimada, K.; Sakamoto, Y.; Sano, T.; Kosuge, T. Prognostic factors after distal pancreatectomy with extended lymphadenectomy for invasive pancreatic adenocarcinoma of the body and tail. Surgery 2006, 139, 288–295. [Google Scholar] [CrossRef]
- Tummers, W.S.; Groen, J.V.; Sibinga Mulder, B.G.; Farina-Sarasqueta, A.; Morreau, J.; Putter, H.; van de Velde, C.J.; Vahrmeijer, A.L.; Bonsing, B.A.; Mieog, J.S.; et al. Impact of resection margin status on recurrence and survival in pancreatic cancer surgery. Br. J. Surg. 2019, 106, 1055–1065. [Google Scholar] [CrossRef]
- Felsenstein, M.; Lindhammer, F.; Feist, M.; Hillebrandt, K.H.; Timmermann, L.; Benzing, C.; Globke, B.; Zocholl, D.; Hu, M.; Fehrenbach, U.; et al. Perineural Invasion in Pancreatic Ductal Adenocarcinoma (PDAC): A Saboteur of Curative Intended Therapies? J. Clin. Med. 2022, 11, 2367. [Google Scholar] [CrossRef]
- Ghaneh, P.; Kleeff, J.; Halloran, C.M.; Raraty, M.; Jackson, R.; Melling, J.; Jones, O.; Palmer, D.H.; Cox, T.F.; Smith, C.J.; et al. The Impact of Positive Resection Margins on Survival and Recurrence Following Resection and Adjuvant Chemotherapy for Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2019, 269, 520–529. [Google Scholar] [CrossRef]
- Kleive, D.; Labori, K.J.; Line, P.D.; Gladhaug, I.P.; Verbeke, C.S. Pancreatoduodenectomy with venous resection for ductal adenocarcinoma rarely achieves complete (R0) resection. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2020, 22, 50–57. [Google Scholar] [CrossRef]
- Zhang, Y.; Frampton, A.E.; Cohen, P.; Kyriakides, C.; Bong, J.J.; Habib, N.A.; Spalding, D.R.; Ahmad, R.; Jiao, L.R. Tumor infiltration in the medial resection margin predicts survival after pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2012, 16, 1875–1882. [Google Scholar] [CrossRef]
- Kalisvaart, M.; Broadhurst, D.; Marcon, F.; Pande, R.; Schlegel, A.; Sutcliffe, R.; Marudanayagam, R.; Mirza, D.; Chatzizacharias, N.; Abradelo, M.; et al. Recurrence patterns of pancreatic cancer after pancreatoduodenectomy: Systematic review and a single-centre retrospective study. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2020, 22, 1240–1249. [Google Scholar] [CrossRef]
- Reinehr, M.D.; Vuille-Dit-Bille, R.N.; Soll, C.; Mittal, A.; Samra, J.S.; Staerkle, R.F. Anatomy of the neural fibers at the superior mesenteric artery-a cadaver study. Langenbeck’s Arch. Surg. 2022, 407, 2347–2354. [Google Scholar] [CrossRef]
- Nagakawa, T.; Sanada, H.; Inagaki, M.; Sugama, J.; Ueno, K.; Konishi, I.; Ohta, T.; Kayahara, M.; Kitagawa, H. Long-term survivors after resection of carcinoma of the head of the pancreas: Significance of histologically curative resection. J Hepatobiliary Pancreat Surg 2004, 11, 402–408. [Google Scholar] [CrossRef]
- Tsuchiya, R.; Noda, T.; Harada, N.; Miyamoto, T.; Tomioka, T.; Yamamoto, K.; Yamaguchi, T.; Izawa, K.; Tsunoda, T.; Yoshino, R.; et al. Collective review of small carcinomas of the pancreas. Ann. Surg. 1986, 203, 77–81. [Google Scholar] [CrossRef]
- van Hilst, J.; de Rooij, T.; Klompmaker, S.; Rawashdeh, M.; Aleotti, F.; Al-Sarireh, B.; Alseidi, A.; Ateeb, Z.; Balzano, G.; Berrevoet, F.; et al. Minimally Invasive versus Open Distal Pancreatectomy for Ductal Adenocarcinoma (DIPLOMA): A Pan-European Propensity Score Matched Study. Ann. Surg. 2019, 269, 10–17. [Google Scholar] [CrossRef]
- Sulpice, L.; Farges, O.; Goutte, N.; Bendersky, N.; Dokmak, S.; Sauvanet, A.; Delpero, J.R. Laparoscopic Distal Pancreatectomy for Pancreatic Ductal Adenocarcinoma: Time for a Randomized Controlled Trial? Results of an All-inclusive National Observational Study. Ann. Surg. 2015, 262, 868–873. [Google Scholar] [CrossRef]
- Shin, S.H.; Kim, S.C.; Song, K.B.; Hwang, D.W.; Lee, J.H.; Park, K.M.; Lee, Y.J. Appraisal of Laparoscopic Distal Pancreatectomy for Left-Sided Pancreatic Cancer: A Large Volume Cohort Study of 152 Consecutive Patients. PLoS ONE 2016, 11, e0163266. [Google Scholar]
- Tran, M.L.; Holm, M.B.; Verbeke, C.S. Tumour Size and T-Stage in Pancreatic Cancer Resection Specimens Depend on the Pathology Examination Approach. Cancers 2022, 14, 2471. [Google Scholar] [CrossRef] [PubMed]
- Soer, E.C.; Verbeke, C.S. Pathology reporting of margin status in locally advanced pancreatic cancer: Challenges and uncertainties. J. Gastrointest. Oncol. 2021, 12, 2512–2520. [Google Scholar] [CrossRef]
- Schmocker, R.K.; Delitto, D.; Wright, M.J.; Ding, D.; Cameron, J.L.; Lafaro, K.J.; Burns, W.R.; Wolfgang, C.L.; Burkhart, R.A.; He, J. Impact of Margin Status on Survival in Patients with Pancreatic Ductal Adenocarcinoma Receiving Neoadjuvant Chemotherapy. J. Am. Coll. Surg. 2021, 232, 405–413. [Google Scholar] [CrossRef]
- Addeo, P.; Cusumano, C.; Dufour, P.; Avérous, G.; Bachellier, P. Upfront versus resection after neoadjuvant chemotherapy for pancreatic adenocarcinomas with venous contact: Comparative analysis of operative and survival outcomes. Surgery 2022, 172, 702–707. [Google Scholar] [CrossRef]
- Villano, A.M.; O’Halloran, E.; Goel, N.; Ruth, K.; Barrak, D.; Lefton, M.; Reddy, S.S. Total neoadjuvant therapy is associated with improved overall survival and pathologic response in pancreatic adenocarcinoma. J. Surg. Oncol. 2022, 126, 502–512. [Google Scholar] [CrossRef]
- Nelson, D.W.; Chang, S.C.; Grunkemeier, G.; Dehal, A.N.; Lee, D.Y.; Fischer, T.D.; DiFronzo, L.A.; O’Connor, V.V. Resectable Distal Pancreas Cancer: Time to Reconsider the Role of Upfront Surgery. Ann. Surg. Oncol. 2018, 25, 4012–4019. [Google Scholar] [CrossRef]
- Nassour, I.; Adam, M.A.; Kowalsky, S.; Al Masri, S.; Bahary, N.; Singhi, A.D.; Lee, K.; Zureikat, A.; Paniccia, A. Neoadjuvant therapy versus upfront surgery for early-stage left-sided pancreatic adenocarcinoma: A propensity-matched analysis from a national cohort of distal pancreatectomies. J. Surg. Oncol. 2021, 123, 245–251. [Google Scholar] [CrossRef]
- Yoshitomi, H.; Sakai, N.; Kagawa, S.; Takano, S.; Ueda, A.; Kato, A.; Furukawa, K.; Takayashiki, T.; Kuboki, S.; Miyzaki, M.; et al. Feasibility and safety of distal pancreatectomy with en bloc celiac axis resection (DP-CAR) combined with neoadjuvant therapy for borderline resectable and unresectable pancreatic body/tail cancer. Langenbeck’s Arch. Surg. 2019, 404, 451–458. [Google Scholar] [CrossRef]
- Baumgartner, J.M.; Krasinskas, A.; Daouadi, M.; Zureikat, A.; Marsh, W.; Lee, K.; Bartlett, D.; Moser, A.J.; Zeh, H.J., 3rd. Distal pancreatectomy with en bloc celiac axis resection for locally advanced pancreatic adenocarcinoma following neoadjuvant therapy. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2012, 16, 1152–1159. [Google Scholar] [CrossRef]
- Yoshiya, S.; Fukuzawa, K.; Inokuchi, S.; Kosai-Fujimoto, Y.; Sanefuji, K.; Iwaki, K.; Motohiro, A.; Itoh, S.; Harada, N.; Ikegami, T.; et al. Efficacy of Neoadjuvant Chemotherapy in Distal Pancreatectomy with En Bloc Celiac Axis Resection (DP-CAR) for Locally Advanced Pancreatic Cancer. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2020, 24, 1605–1611. [Google Scholar] [CrossRef]
- van Hilst, J.; Korrel, M.; Lof, S.; de Rooij, T.; Vissers, F.; Al-Sarireh, B.; Alseidi, A.; Bateman, A.C.; Björnsson, B.; Boggi, U.; et al. Minimally invasive versus open distal pancreatectomy for pancreatic ductal adenocarcinoma (DIPLOMA): Study protocol for a randomized controlled trial. Trials 2021, 22, 608. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gerota’s fascia |
| Adrenal gland |
| Stomach |
| Small bowel |
| Large bowel |
| Kidney |
| Large blood vessels |
| Study | n | R1 Rate (%) | R1 Definition | Dissection Technique | NAT (%) | Prognostic Impact of R-Status |
|---|---|---|---|---|---|---|
| Sahakyan 2022 [7] Entire cohort Period 1 | ||||||
| 124 | 73.4 | ≤1 mm | 7.3 | No 1 | ||
| 53 | 60.4 | Sagittal slicing, not specified | ||||
| Period 2 | 71 | 83.1 | Sagittal slicing, standardized | |||
| Korrel 2021 [16] | 1200 | 43.2 | <1 mm | Sagittal slicing, standardized | 10.7 | Yes |
| Hank 2018 [31] | 218 | 71.1 | <1 mm | Sagittal slicing, standardized | - | Yes |
| Demir 2018 [32] (Institutional cohort) | 44 | 36.4 | 0 mm | Not specified | - | No |
| 59.1 | <1 mm | |||||
| Sahakyan 2017 [33] | 186 | 9.5 | 0 mm | Not specified | 1.0 | No |
| De Rooij 2016 [17] | 141 | 45.0 | <1 mm | Not specified | - | Yes |
| (5.0 R2) | ||||||
| Paye 2015 [18] (Multicentre study) | 278 | 25.2 2 | <1 mm | Not specified | 7.2 | No |
| Yamamoto 2010 [34] | 73 3 | 16.4 | Not specified | Not specified | - | Yes |
| (8.2 R2) | ||||||
| Chang 2009 [23] | 70 | 47.1 | 0 mm | Not specified | - | No |
| 57.2 | <1 mm | |||||
| Shimada 2006 [35] | 884 | 25.0 | Not specified | Not specified | - | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holm, M.B.; Verbeke, C.S. Prognostic Impact of Resection Margin Status on Distal Pancreatectomy for Ductal Adenocarcinoma. Curr. Oncol. 2022, 29, 6551-6563. https://doi.org/10.3390/curroncol29090515
Holm MB, Verbeke CS. Prognostic Impact of Resection Margin Status on Distal Pancreatectomy for Ductal Adenocarcinoma. Current Oncology. 2022; 29(9):6551-6563. https://doi.org/10.3390/curroncol29090515
Chicago/Turabian StyleHolm, Maia Blomhoff, and Caroline Sophie Verbeke. 2022. "Prognostic Impact of Resection Margin Status on Distal Pancreatectomy for Ductal Adenocarcinoma" Current Oncology 29, no. 9: 6551-6563. https://doi.org/10.3390/curroncol29090515
APA StyleHolm, M. B., & Verbeke, C. S. (2022). Prognostic Impact of Resection Margin Status on Distal Pancreatectomy for Ductal Adenocarcinoma. Current Oncology, 29(9), 6551-6563. https://doi.org/10.3390/curroncol29090515