Association between Inflammatory Markers and Local Recurrence in Patients with Giant Cell Tumor of Bone: A Preliminary Result

 ,
,  , , , ,
, , , ,  ,
,  ,
, 
Abstract
1. Introduction
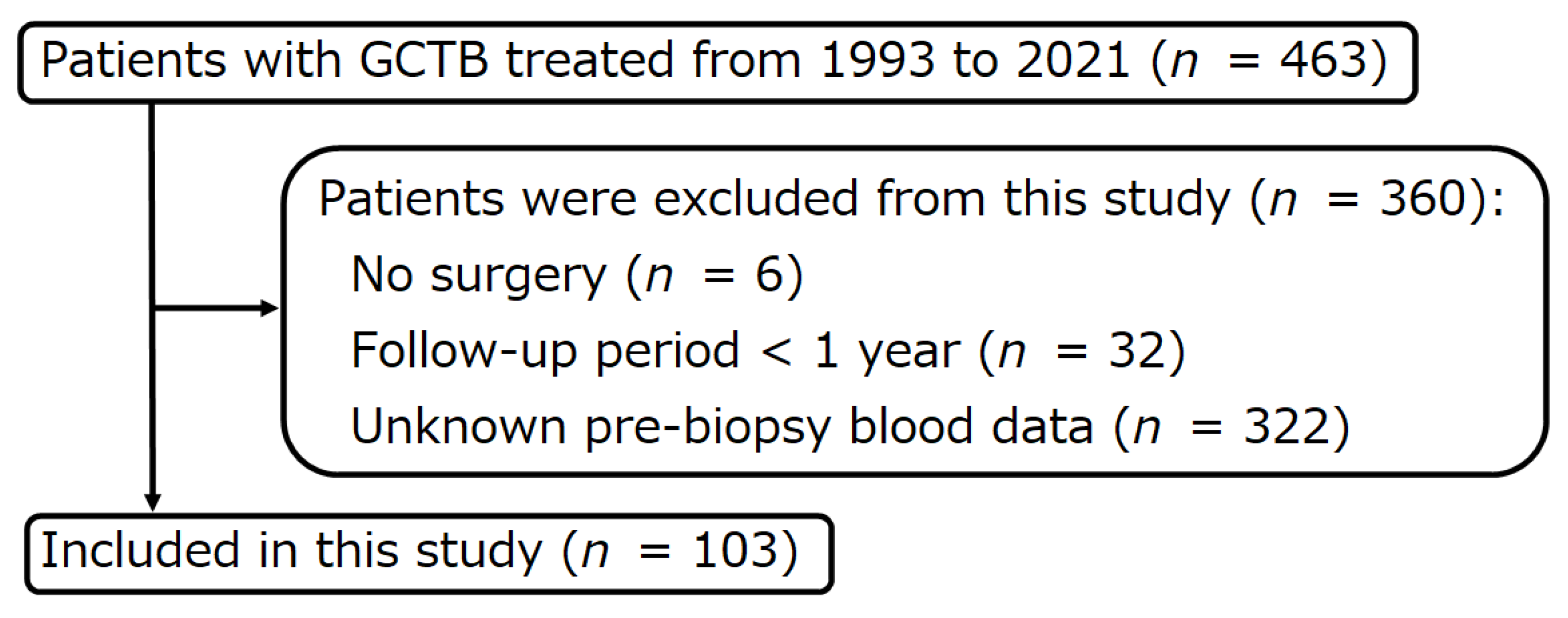
2. Materials and Methods
2.1. Curettage
2.2. En Bloc Resection
2.3. Denosumab
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flanagan, A.M.; Larousserie, F.; O’Donnell, P.G.; Yoshida, A. Giant cell tumour of bone. In Soft Tissue and Bone Tumours. WHO Classification of Tumours, 5th ed.; The WHO Classification of Tumours Editorial Board, Ed.; IARC: Lyon, France, 2020; pp. 440–446. [Google Scholar]
- Campanacci, M.; Baldini, N.; Boriani, S.; Sudanese, A. Giant-Cell Tumor of Bone. J. Bone Joint Surg. Am. 1987, 69, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Machak, G.N.; Snetkov, A.I. The Impact of Curettage Technique on Local Control in Giant Cell Tumour of Bone. Int. Orthop. 2021, 45, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, S.; Mavrogenis, A.F.; Tanaka, Y.; Kido, A.; Honoki, K.; Tanaka, Y.; Errani, C. Metastasectomy Versus Non-Metastasectomy for Giant Cell Tumor of Bone Lung Metastases. Orthopedics 2021, 44, e707–e712. [Google Scholar] [CrossRef] [PubMed]
- Palmerini, E.; Picci, P.; Reichardt, P.; Downey, G. Malignancy in Giant Cell Tumor of Bone: A Review of the Literature. Technol. Cancer Res. Treat. 2019, 18, 1533033819840000. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, T.; Ricci, M.; Scarpi, E.; Bongiovanni, A.; Ricci, R.; Riva, N.; Liverani, C.; De Vita, A.; La Manna, F.; Oboldi, D.; et al. RANKL: A Promising Circulating Marker for Bone Metastasis Response. Oncol. Lett. 2016, 12, 2970–2975. [Google Scholar] [CrossRef] [PubMed]
- Wülling, M.; Delling, G.; Kaiser, E. The Origin of the Neoplastic Stromal Cell in Giant Cell Tumor of Bone. Hum. Pathol. 2003, 34, 983–993. [Google Scholar] [CrossRef]
- Heymann, D. Anti-RANKL Therapy for Bone Tumours: Basic, Pre-Clinical and Clinical Evidence. J. Bone Oncol. 2012, 1, 2–11. [Google Scholar] [CrossRef]
- Palmerini, E.; Pazzaglia, L.; Cevolani, L.; Pratelli, L.; Pierini, M.; Quattrini, I.; Carretta, E.; Manara, M.C.; Pasello, M.; Frega, G.; et al. Bone Turnover Marker (BTM) Changes after Denosumab in Giant Cell Tumors of Bone (GCTB): A Phase II Trial Correlative Study. Cancers 2022, 14, 2863. [Google Scholar] [CrossRef]
- Liu, J.; Lin, P.C.; Zhou, B.P. Inflammation Fuels Tumor Progress and Metastasis. Curr. Pharm. Des. 2015, 21, 3032–3040. [Google Scholar] [CrossRef]
- Yamamoto, T.; Kawada, K.; Obama, K. Inflammation-Related Biomarkers for the Prediction of Prognosis in Colorectal Cancer Patients. Int. J. Mol. Sci. 2021, 22, 8002. [Google Scholar] [CrossRef]
- Yapar, A.; Atalay, İ.B.; Tokgöz, M.A.; Ulucaköy, C.; Güngör, B.Ş. Prognostic Significance of the Preoperative Neutrophil-to-Lymphocyte Ratio Patients with Giant Cell Tumor of Bone. Afr. Health Sci. 2021, 21, 1250–1258. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Li, B.; Zhou, P.; Zhao, J.; Wu, Z.; Yang, X.; Wei, H.; Chen, T.; Xiao, J. Nomograms for Prognostic Factors of Spinal Giant Cell Tumor Combining Traditional Clinical Characteristics with Inflammatory Biomarkers after Gross Total Resection. Oncotarget 2017, 8, 86934–86946. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Zhao, G.; Chen, F.; Xia, J.; Jiang, L. The Prognostic Significance of the Neutrophil-to-Lymphocyte Ratio and the Platelet-to-Lymphocyte Ratio in Giant Cell Tumor of the Extremities. BMC Cancer 2019, 19, 329. [Google Scholar] [CrossRef]
- Liang, S.; Li, Y.; Liu, H.; Wang, B. Pre-Operative Prognostic Nutritional Index Was Associated with Recurrence after Surgery in Giant Cell Tumor of Bone Patients. J. Bone Oncol. 2020, 25, 100324. [Google Scholar] [CrossRef]
- Huang, Y.; Wei, S.; Jiang, N.; Zhang, L.; Wang, S.; Cao, X.; Zhao, Y.; Wang, P. The Prognostic Impact of Decreased Pretreatment Haemoglobin Level on the Survival of Patients with Lung Cancer: A Systematic Review and Meta-Analysis. BMC Cancer 2018, 18, 1235. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, T.; Kawada, T.; Rajwa, P.; Mostafaei, H.; Motlagh, R.S.; Quhal, F.; Laukhtina, E.; König, F.; Pallauf, M.; Pradere, B.; et al. Sequencing Impact and Prognostic Factors in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Cabazitaxel: A Systematic Review and Meta-Analysis. Urol. Oncol. 2022, in press. [Google Scholar] [CrossRef]
- Mori, K.; Miura, N.; Mostafaei, H.; Quhal, F.; Motlagh, R.S.; Lysenko, I.; Kimura, S.; Egawa, S.; Karakiewicz, P.I.; Shariat, S.F. Prognostic Value of Preoperative Hematologic Biomarkers in Urothelial Carcinoma of the Bladder Treated with Radical Cystectomy: A Systematic Review and Meta-Analysis. Int. J. Clin. Oncol. 2020, 25, 1459–1474. [Google Scholar] [CrossRef]
- Pergialiotis, V.; Daskalakis, G.; Thomakos, N.; Bellos, I.; Haidopoulos, D.; Loutradis, D.; Rodolakis, A. Prechemotherapy Hemoglobin Levels as a Predictive Factor of Ovarian Cancer Survival: A Systematic Review and Meta-Analysis. Am. J. Clin. Oncol. 2019, 42, 725–731. [Google Scholar] [CrossRef]
- Liu, F.; Zhao, J.; Xie, J.; Xie, L.; Zhu, J.; Cai, S.; Zheng, H.; Xu, Y. Prognostic Risk Factors in Patients with Bone Metastasis from Colorectal Cancer. Tumour Biol. 2016, 37, 16127–16134. [Google Scholar] [CrossRef]
- Lim, S.M.; Kim, Y.N.; Park, K.H.; Kang, B.; Chon, H.J.; Kim, C.; Kim, J.H.; Rha, S.Y. Bone Alkaline Phosphatase as a Surrogate Marker of Bone Metastasis in Gastric Cancer Patients. BMC Cancer 2016, 16, 385. [Google Scholar] [CrossRef]
- Huang, P.; Lan, M.; Peng, A.-F.; Yu, Q.-F.; Chen, W.-Z.; Liu, Z.-L.; Liu, J.-M.; Huang, S.-H. Serum Calcium, Alkaline Phosphatase and Hemoglobin as Risk Factors for Bone Metastases in Bladder Cancer. PLoS ONE 2017, 12, e0183835. [Google Scholar] [CrossRef]
- Ren, H.-Y.; Sun, L.-L.; Li, H.-Y.; Ye, Z.-M. Prognostic Significance of Serum Alkaline Phosphatase Level in Osteosarcoma: A Meta-Analysis of Published Data. BioMed Res. Int. 2015, 2015, 160835. [Google Scholar] [CrossRef]
- Comandatore, A.; Franczak, M.; Smolenski, R.T.; Morelli, L.; Peters, G.J.; Giovannetti, E. Lactate Dehydrogenase and Its Clinical Significance in Pancreatic and Thoracic Cancers. Semin. Cancer Biol. 2022, 86, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Forkasiewicz, A.; Dorociak, M.; Stach, K.; Szelachowski, P.; Tabola, R.; Augoff, K. The Usefulness of Lactate Dehydrogenase Measurements in Current Oncological Practice. Cell. Mol. Biol. Lett. 2020, 25, 35. [Google Scholar] [CrossRef] [PubMed]
- Errani, C.; Tsukamoto, S.; Leone, G.; Akahane, M.; Cevolani, L.; Tanzi, P.; Kido, A.; Honoki, K.; Tanaka, Y.; Donati, D.M. Higher Local Recurrence Rates after Intralesional Surgery for Giant Cell Tumor of the Proximal Femur Compared to Other Sites. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 813–819. [Google Scholar] [CrossRef] [PubMed]
- Hindiskere, S.; Errani, C.; Doddarangappa, S.; Ramaswamy, V.; Rai, M.; Chinder, P.S. Is a Short-Course of Preoperative Denosumab as Effective as Prolonged Therapy for Giant Cell Tumor of Bone? Clin. Orthop. Relat. Res. 2020, 478, 2522–2533. [Google Scholar] [CrossRef]
- O’Donnell, R.J.; Springfield, D.S.; Motwani, H.K.; Ready, J.E.; Gebhardt, M.C.; Mankin, H.J. Recurrence of Giant-Cell Tumors of the Long Bones after Curettage and Packing with Cement. J. Bone Joint Surg. Am. 1994, 76, 1827–1833. [Google Scholar] [CrossRef]
- McMillan, D.C. The Systemic Inflammation-Based Glasgow Prognostic Score: A Decade of Experience in Patients with Cancer. Cancer Treat. Rev. 2013, 39, 534–540. [Google Scholar] [CrossRef]
- McMillan, D.C.; Crozier, J.E.M.; Canna, K.; Angerson, W.J.; McArdle, C.S. Evaluation of an Inflammation-Based Prognostic Score (GPS) in Patients Undergoing Resection for Colon and Rectal Cancer. Int. J. Colorectal Dis. 2007, 22, 881–886. [Google Scholar] [CrossRef]
- Tsukamoto, S.; Mavrogenis, A.F.; Tanzi, P.; Leone, G.; Akahane, M.; Tanaka, Y.; Errani, C. Curettage as First Surgery for Bone Giant Cell Tumor: Adequate Surgery Is More Important than Oncology Training or Surgical Management by High Volume Specialized Teams. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 3–9. [Google Scholar] [CrossRef]
- Tsukamoto, S.; Mavrogenis, A.F.; Tanzi, P.; Leone, G.; Ciani, G.; Righi, A.; Akahane, M.; Honoki, K.; Tanaka, Y.; Donati, D.M.; et al. Denosumab for Bone Giant Cell Tumor of the Distal Radius. Orthopedics 2020, 43, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Chawla, S.; Henshaw, R.; Seeger, L.; Choy, E.; Blay, J.-Y.; Ferrari, S.; Kroep, J.; Grimer, R.; Reichardt, P.; Rutkowski, P.; et al. Safety and Efficacy of Denosumab for Adults and Skeletally Mature Adolescents with Giant Cell Tumour of Bone: Interim Analysis of an Open-Label, Parallel-Group, Phase 2 Study. Lancet Oncol. 2013, 14, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, P.; Ferrari, S.; Grimer, R.J.; Stalley, P.D.; Dijkstra, S.P.D.; Pienkowski, A.; Vaz, G.; Wunder, J.S.; Seeger, L.L.; Feng, A.; et al. Surgical Downstaging in an Open-Label Phase II Trial of Denosumab in Patients with Giant Cell Tumor of Bone. Ann. Surg. Oncol. 2015, 22, 2860–2868. [Google Scholar] [CrossRef] [PubMed]
- Jabłońska, E.; Kiluk, M.; Markiewicz, W.; Piotrowski, L.; Grabowska, Z.; Jabłoński, J. TNF-Alpha, IL-6 and Their Soluble Receptor Serum Levels and Secretion by Neutrophils in Cancer Patients. Arch. Immunol. Ther. Exp. 2001, 49, 63–69. [Google Scholar]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar]
- Oñate-Ocaña, L.F.; Becker, M.; Carrillo, J.F.; Aiello-Crocifoglio, V.; Gallardo-Rincón, D.; Brom-Valladares, R.; Herrera-Goepfert, R.; Ochoa-Carrillo, F.; Beltrán-Ortega, A. Selection of Best Candidates for Multiorgan Resection among Patients with T4 Gastric Carcinoma. J. Surg. Oncol. 2008, 98, 336–342. [Google Scholar] [CrossRef]
- Li, Y.; Jia, H.; Yu, W.; Xu, Y.; Li, X.; Li, Q.; Cai, S. Nomograms for Predicting Prognostic Value of Inflammatory Biomarkers in Colorectal Cancer Patients after Radical Resection. Int. J. Cancer 2016, 139, 220–231. [Google Scholar] [CrossRef]
- Cheng, C.Y.; Shih, H.N.; Hsu, K.Y.; Hsu, R.W. Treatment of Giant Cell Tumor of the Distal Radius. Clin. Orthop. Relat. Res. 2001, 383, 221–228. [Google Scholar] [CrossRef]
- Sheth, D.S.; Healey, J.H.; Sobel, M.; Lane, J.M.; Marcove, R.C. Giant Cell Tumor of the Distal Radius. J. Hand Surg. Am. 1995, 20, 432–440. [Google Scholar] [CrossRef]
- Errani, C.; Ruggieri, P.; Asenzio, M.A.N.; Toscano, A.; Colangeli, S.; Rimondi, E.; Rossi, G.; Longhi, A.; Mercuri, M. Giant Cell Tumor of the Extremity: A Review of 349 Cases from a Single Institution. Cancer Treat. Rev. 2010, 36, 1–7. [Google Scholar] [CrossRef]
- Errani, C.; Tsukamoto, S.; Leone, G.; Righi, A.; Akahane, M.; Tanaka, Y.; Donati, D.M. Denosumab May Increase the Risk of Local Recurrence in Patients with Giant-Cell Tumor of Bone Treated with Curettage. J. Bone Joint Surg. Am. 2018, 100, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, S.; Tanaka, Y.; Mavrogenis, A.F.; Kido, A.; Kawaguchi, M.; Errani, C. Is Treatment with Denosumab Associated with Local Recurrence in Patients with Giant Cell Tumor of Bone Treated with Curettage? A Systematic Review. Clin. Orthop. Relat Res 2020, 478, 1076–1085. [Google Scholar] [CrossRef]
- Mak, I.W.Y.; Evaniew, N.; Popovic, S.; Tozer, R.; Ghert, M. A Translational Study of the Neoplastic Cells of Giant Cell Tumor of Bone Following Neoadjuvant Denosumab. J. Bone Joint Surg. Am. 2014, 96, e127. [Google Scholar] [CrossRef] [PubMed]
- Traub, F.; Singh, J.; Dickson, B.C.; Leung, S.; Mohankumar, R.; Blackstein, M.E.; Razak, A.R.; Griffin, A.M.; Ferguson, P.C.; Wunder, J.S. Efficacy of Denosumab in Joint Preservation for Patients with Giant Cell Tumour of the Bone. Eur. J. Cancer 2016, 59, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hock, B.D.; Taylor, K.G.; Cross, N.B.; Kettle, A.J.; Hampton, M.B.; McKenzie, J.L. Effect of Activated Human Polymorphonuclear Leucocytes on T Lymphocyte Proliferation and Viability. Immunology 2012, 137, 249–258. [Google Scholar] [CrossRef]
- Dunn, G.P.; Old, L.J.; Schreiber, R.D. The Immunobiology of Cancer Immunosurveillance and Immunoediting. Immunity 2004, 21, 137–148. [Google Scholar] [CrossRef]
- Armistead, P.M.; Wieder, E.; Akande, O.; Alatrash, G.; Quintanilla, K.; Liang, S.; Molldrem, J. Cyclic Neutropenia Associated with T Cell Immunity to Granulocyte Proteases and a Double de Novo Mutation in GFI1, a Transcriptional Regulator of ELANE. Br. J. Haematol. 2010, 150, 716–719. [Google Scholar] [CrossRef]
- Zhao, N.; Xu, H.; Zhou, D.; Xu, X.; Ge, W.; Cao, D. The Prognostic Role of Neutrophil-to-Lymphocyte Ratio and C-Reactive Protein in Metastatic Colorectal Cancer Using Regorafenib: A Systematic Review and Meta-Analysis. J. Gastrointest. Oncol. 2022, 13, 1772–1781. [Google Scholar] [CrossRef]
- Hu, X.; Tian, T.; Sun, Q.; Jiang, W. Prognostic Value of the Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio in Laryngeal Cancer: What Should We Expect from a Meta-Analysis? Front. Oncol. 2022, 12, 945820. [Google Scholar] [CrossRef]
- Platini, H.; Ferdinand, E.; Kohar, K.; Prayogo, S.A.; Amirah, S.; Komariah, M.; Maulana, S. Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio as Prognostic Markers for Advanced Non-Small-Cell Lung Cancer Treated with Immunotherapy: A Systematic Review and Meta-Analysis. Medicina 2022, 58, 1069. [Google Scholar] [CrossRef]
- Leng, J.; Wu, F.; Zhang, L. Prognostic Significance of Pretreatment Neutrophil-to-Lymphocyte Ratio, Platelet-to-Lymphocyte Ratio, or Monocyte-to-Lymphocyte Ratio in Endometrial Neoplasms: A Systematic Review and Meta-Analysis. Front. Oncol. 2022, 12, 734948. [Google Scholar] [CrossRef]
- Lee, S.J.; Kim, K.; Park, H.J. Meta-Analysis on the Neutrophil-Lymphocyte Ratio in Rectal Cancer Treated With Preoperative Chemoradiotherapy: Prognostic Value of Pre- and Post-Chemoradiotherapy Neutrophil-Lymphocyte Ratio. Front. Oncol. 2022, 12, 778607. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, Y.; Oya, R.; Takemoto, N.; Inohara, H. Neutrophil-to-Lymphocyte Ratio as a Prognostic Marker for Head and Neck Squamous Cell Carcinoma Treated with Immune Checkpoint Inhibitors: Meta-Analysis. Head Neck 2022, 44, 1237–1245. [Google Scholar] [CrossRef]
- El Bairi, K.; Al Jarroudi, O.; Afqir, S. Inexpensive Systemic Inflammatory Biomarkers in Ovarian Cancer: An Umbrella Systematic Review of 17 Prognostic Meta-Analyses. Front. Oncol. 2021, 11, 694821. [Google Scholar] [CrossRef]
- Forrest, L.M.; McMillan, D.C.; McArdle, C.S.; Angerson, W.J.; Dunlop, D.J. Evaluation of Cumulative Prognostic Scores Based on the Systemic Inflammatory Response in Patients with Inoperable Non-Small-Cell Lung Cancer. Br. J. Cancer 2003, 89, 1028–1030. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Wu, Z.; Wang, Z.; Wu, C.; Huang, X.; Tian, B. Prognostic Role of the Prognostic Nutritional Index in Patients with Pancreatic Cancer Who Underwent Curative Resection without Preoperative Neoadjuvant Treatment: A Systematic Review and Meta-Analysis. Front. Surg. 2022, 9, 992641. [Google Scholar] [CrossRef]
- Ni, L.; Huang, J.; Ding, J.; Kou, J.; Shao, T.; Li, J.; Gao, L.; Zheng, W.; Wu, Z. Prognostic Nutritional Index Predicts Response and Prognosis in Cancer Patients Treated With Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Front. Nutr. 2022, 9, 823087. [Google Scholar] [CrossRef]
- Mao, C.; Xu, W.; Ma, W.; Wang, C.; Guo, Z.; Yan, J. Prognostic Value of Pretreatment Prognostic Nutritional Index in Patients With Renal Cell Carcinoma: A Meta-Analysis. Front. Oncol. 2021, 11, 719941. [Google Scholar] [CrossRef] [PubMed]
- Hao, J.; Chen, C.; Wan, F.; Zhu, Y.; Jin, H.; Zhou, J.; Chen, N.; Yang, J.; Pu, Q. Prognostic Value of Pre-Treatment Prognostic Nutritional Index in Esophageal Cancer: A Systematic Review and Meta-Analysis. Front. Oncol. 2020, 10, 797. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.; Yang, L.; Liu, D.; Li, W.M. Prognostic Value of Pretreatment Lymphocyte-to-Monocyte Ratio in Lung Cancer: A Systematic Review and Meta-Analysis. Technol. Cancer Res. Treat. 2021, 20, 1533033820983085. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Fang, Y.; Mo, Z.; Lin, Y.; Ji, C.; Jian, Z. Prognostic Value of Lymphocyte to Monocyte Ratio in Pancreatic Cancer: A Systematic Review and Meta-Analysis Including 3338 Patients. World J. Surg. Oncol. 2020, 18, 186. [Google Scholar] [CrossRef] [PubMed]
- Wagner, D.D. New Links between Inflammation and Thrombosis. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1321–1324. [Google Scholar] [CrossRef] [PubMed]
- Stone, R.L.; Nick, A.M.; McNeish, I.A.; Balkwill, F.; Han, H.D.; Bottsford-Miller, J.; Rupairmoole, R.; Armaiz-Pena, G.N.; Pecot, C.V.; Coward, J.; et al. Paraneoplastic Thrombocytosis in Ovarian Cancer. N. Engl. J. Med. 2012, 366, 610–618. [Google Scholar] [CrossRef]
- Zhou, K.; Cao, J.; Lin, H.; Liang, L.; Shen, Z.; Wang, L.; Peng, Z.; Mei, J. Prognostic Role of the Platelet to Lymphocyte Ratio (PLR) in the Clinical Outcomes of Patients with Advanced Lung Cancer Receiving Immunotherapy: A Systematic Review and Meta-Analysis. Front. Oncol. 2022, 12, 962173. [Google Scholar] [CrossRef]
- Taylor, R.M.; Kashima, T.G.; Knowles, H.J.; Athanasou, N.A. VEGF, FLT3 Ligand, PlGF and HGF Can Substitute for M-CSF to Induce Human Osteoclast Formation: Implications for Giant Cell Tumour Pathobiology. Lab. Investig. 2012, 92, 1398–1406. [Google Scholar] [CrossRef] [PubMed]
- Kumta, S.M.; Huang, L.; Cheng, Y.Y.; Chow, L.T.C.; Lee, K.M.; Zheng, M.H. Expression of VEGF and MMP-9 in Giant Cell Tumor of Bone and Other Osteolytic Lesions. Life Sci. 2003, 73, 1427–1436. [Google Scholar] [CrossRef]
- De Vita, A.; Vanni, S.; Miserocchi, G.; Fausti, V.; Pieri, F.; Spadazzi, C.; Cocchi, C.; Liverani, C.; Calabrese, C.; Casadei, R.; et al. A Rationale for the Activity of Bone Target Therapy and Tyrosine Kinase Inhibitor Combination in Giant Cell Tumor of Bone and Desmoplastic Fibroma: Translational Evidence. Biomedicines 2022, 10, 372. [Google Scholar] [CrossRef]
- Ibrahim, U.A.; Yusuf, A.A.; Ahmed, S.G. The Pathophysiologic Basis of Anaemia in Patients with Malignant Diseases. Gulf J. Oncol. 2016, 1, 80–89. [Google Scholar]
- Baburao, A.; Narayanswamy, H. Clinico-Pathological Profile and Haematological Abnormalities Associated with Lung Cancer in Bangalore, India. Asian Pac. J. Cancer Prev. 2015, 16, 8235–8238. [Google Scholar] [CrossRef]
- Buck, I.; Morceau, F.; Grigorakaki, C.; Dicato, M.; Diederich, M. Linking Anemia to Inflammation and Cancer: The Crucial Role of TNFalpha. Biochem. Pharmacol. 2009, 77, 1572–1579. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable (n = 103) | No. of Patients |
|---|---|
| Sex | |
| Male | 54 (52.4%) |
| Female | 49 (47.6%) |
| Age (years) | Median, 33.6 (IQR, 23.6–44.4) |
| Site | |
| Distal radius | 13 (12.6%) |
| Proximal femur | 6 (5.8%) |
| Distal femur | 36 (35.0%) |
| Proximal tibia | 27 (26.2%) |
| Proximal fibula | 4 (3.9%) |
| Proximal humerus | 4 (3.9%) |
| Hand and foot | 3 (2.9%) |
| Others * | 10 (9.7%) |
| Campanacci classification | |
| Stage I | 0 |
| Stage II | 63 (61.2%) |
| Stage III | 40 (38.8%) |
| Lung metastasis at presentation | |
| No | 99 (96.1%) |
| Yes | 4 (3.9%) |
| Pathological fracture at presentation | |
| No | 88 (85.4%) |
| Yes | 15 (14.6%) |
| Denosumab administration | |
| No | 86 (83.5%) |
| Yes | 17 (16.5%) |
| Previous surgery | |
| No | 84 (81.6%) |
| Yes | 19 (18.4%) |
| Surgery | |
| Curettage | 63 (61.2%) |
| En bloc resection | 40 (38.8%) |
| C-reactive protein (mg/L) | Median, 2 (IQR, 0–5.3) |
| Neutrophil count (×109/L) | Median, 4.3 (IQR, 3.4–5.6) |
| Lymphocyte count (×109/L) | Median, 1.9 (IQR, 1.4–2.3) |
| Monocyte count (×109/L) | Median, 0.5 (IQR, 0.4–0.6) |
| Platelet count (×109/L) | Median, 244 (IQR, 207–288) |
| Serum hemoglobin (g/L) | Median, 140 (IQR, 130–153) |
| Alkaline phosphatase (U/L) | Median, 106 (IQR, 63–200) |
| Lactate dehydrogenase (U/L) | Median, 281 (IQR, 180–334) |
| Neutrophil-lymphocyte ratio (NLR) | Median, 2.41 (IQR, 1.59–3.42) |
| Modified Glasgow prognostic score (mGPS) | |
| 0 | 89 (86.4%) |
| 1 | 14 (13.6%) |
| 2 | 0 |
| Prognostic nutritional index (PNI) | Median, 55.5 (IQR, 53–58.7) |
| Lymphocyte-monocyte ratio (LMR) | Median, 3.83 (IQR, 2.86–4.67) |
| Platelet-lymphocyte ratio (PLR) | Median, 135.5 (IQR, 105.6–178.6) |
| Local recurrence | |
| None | 73 (70.9%) |
| ≥1 | 30 (29.1%) |
| Lung metastasis | |
| None | 94 (91.3%) |
| ≥1 | 9 (8.7%) |
| Follow-up (months) | Median, 66 (IQR, 9.5–543) |
| Variable (n = 103) | No. of Patients | Hazard Ratio (95% CI) | p-Value |
|---|---|---|---|
| Sex | 0.307 | ||
| Male | 54 | 1 | |
| Female | 49 | 1.45 (0.71–2.98) | |
| Age (years) | 103 | 0.98 (0.96–1.01) | 0.195 |
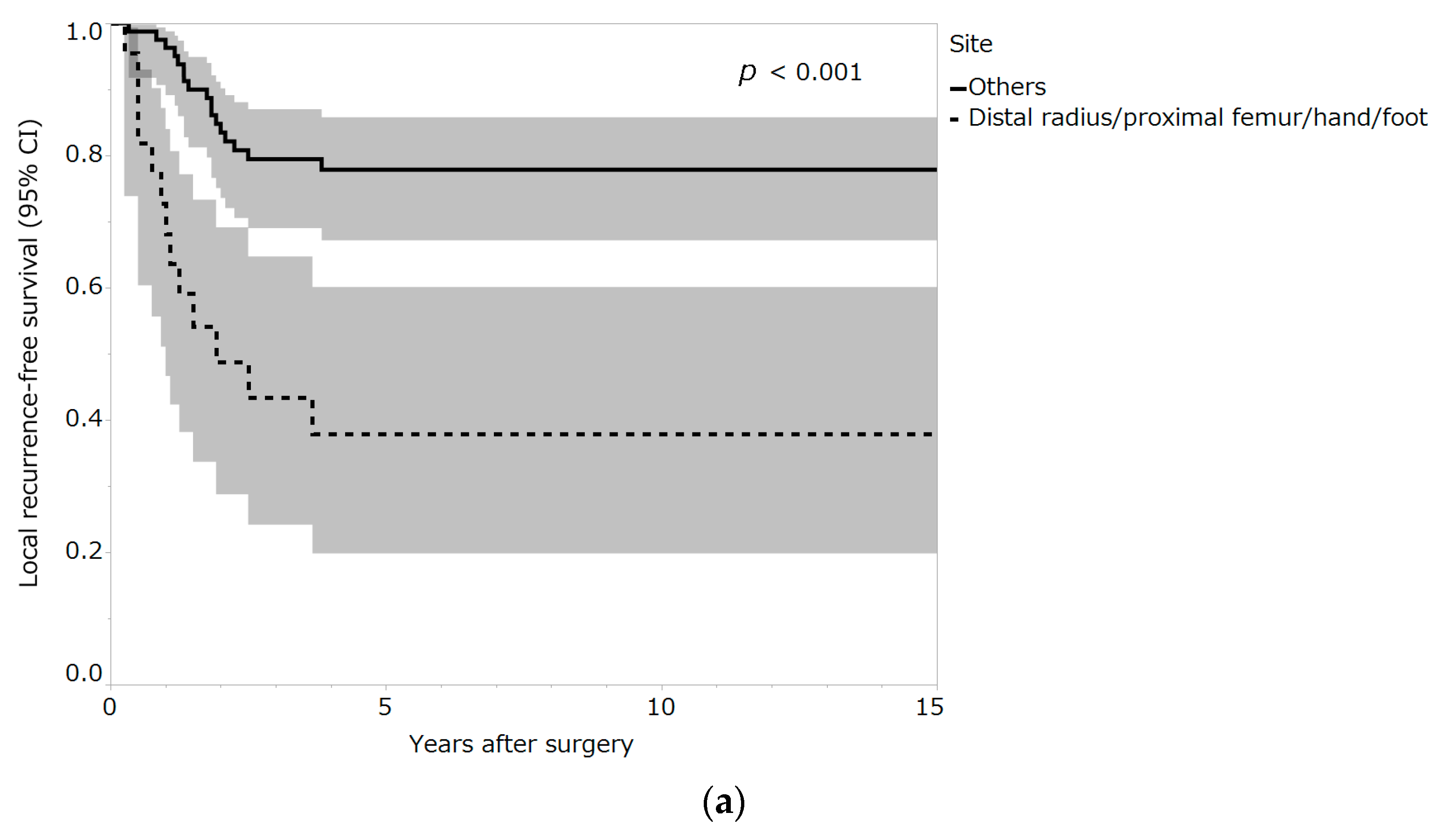
| Site | <0.001 * | ||
| Distal radius/proximal femur/hand/foot | 22 | 4.16 (2.01–8.59) | |
| Others | 81 | 1 | |
| Campanacci classification | 0.806 | ||
| Stages I and II | 63 | 1 | |
| Stage III | 40 | 0.91 (0.43–1.92) | |
| Pathological fracture at presentation | 0.962 | ||
| No | 88 | 1 | |
| Yes | 15 | 0.97 (0.34–2.79) | |
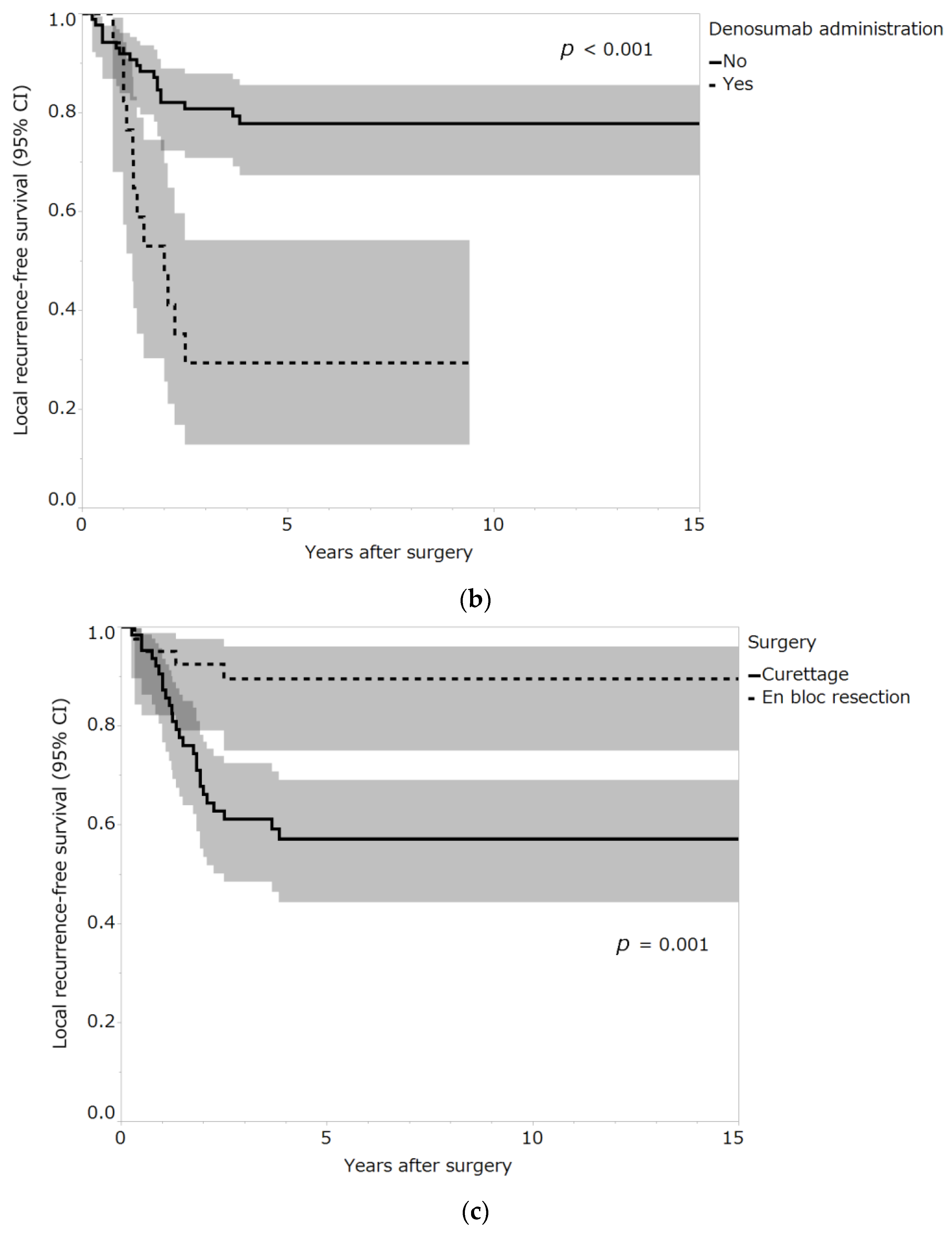
| Denosumab administration | <0.001 * | ||
| No | 86 | 1 | |
| Yes | 17 | 4.42 (2.11–9.22) | |
| Previous surgery | 0.366 | ||
| No | 84 | 1 | |
| Yes | 19 | 1.48 (0.63–3.45) | |
| Surgery | <0.001 * | ||
| Curettage | 63 | 1 | |
| En bloc resection | 40 | 0.21 (0.07–0.60) | |
| C-reactive protein (mg/L) | 103 | 0.99 (0.97–1.01) | 0.546 |
| Neutrophil count (×109/L) | 103 | 0.96 (0.85–1.09) | 0.553 |
| Lymphocyte count (×109/L) | 103 | 0.97 (0.79–1.20) | 0.796 |
| Monocyte count (×109/L) | 103 | 0.42 (0.05–3.34) | 0.410 |
| Platelet count (×109/L) | 103 | 1.00 (0.99–1.00) | 0.308 |
| Serum hemoglobin (g/L) | 103 | 1.00 (0.97–1.02) | 0.637 |
| Alkaline phosphatase (U/L) | 103 | 1.00 (0.99–1.00) | 0.526 |
| Lactate dehydrogenase (U/L) | 103 | 0.994 (0.990–0.998) | 0.009 * |
| Neutrophil-lymphocyte ratio (NLR) | 103 | 0.96 (0.81–1.14) | 0.616 |
| Modified Glasgow prognostic score (mGPS) | 0.235 | ||
| 0 | 89 | 1 | |
| 1 | 14 | 0.42 (0.10–1.76) | |
| Prognostic nutritional index (PNI) | 103 | 0.99 (0.96–1.03) | 0.740 |
| Lymphocyte-monocyte ratio (LMR) | 103 | 1.09 (0.89–1.35) | 0.401 |
| Platelet-lymphocyte ratio (PLR) | 103 | 1.00 (0.99–1.00) | 0.411 |
| Variable | Hazard Ratio (95% CI) | p-Value |
|---|---|---|
| Site | ||
| Distal radius/proximal femur/hand/foot versus others | 4.36 (2.03–9.35) | <0.001 * |
| Denosumab administration | ||
| Yes versus no | 2.27 (1.02–5.06) | 0.046 * |
| Surgery | ||
| En bloc resection versus curettage | 0.22 (0.07–0.68) | 0.008 * |
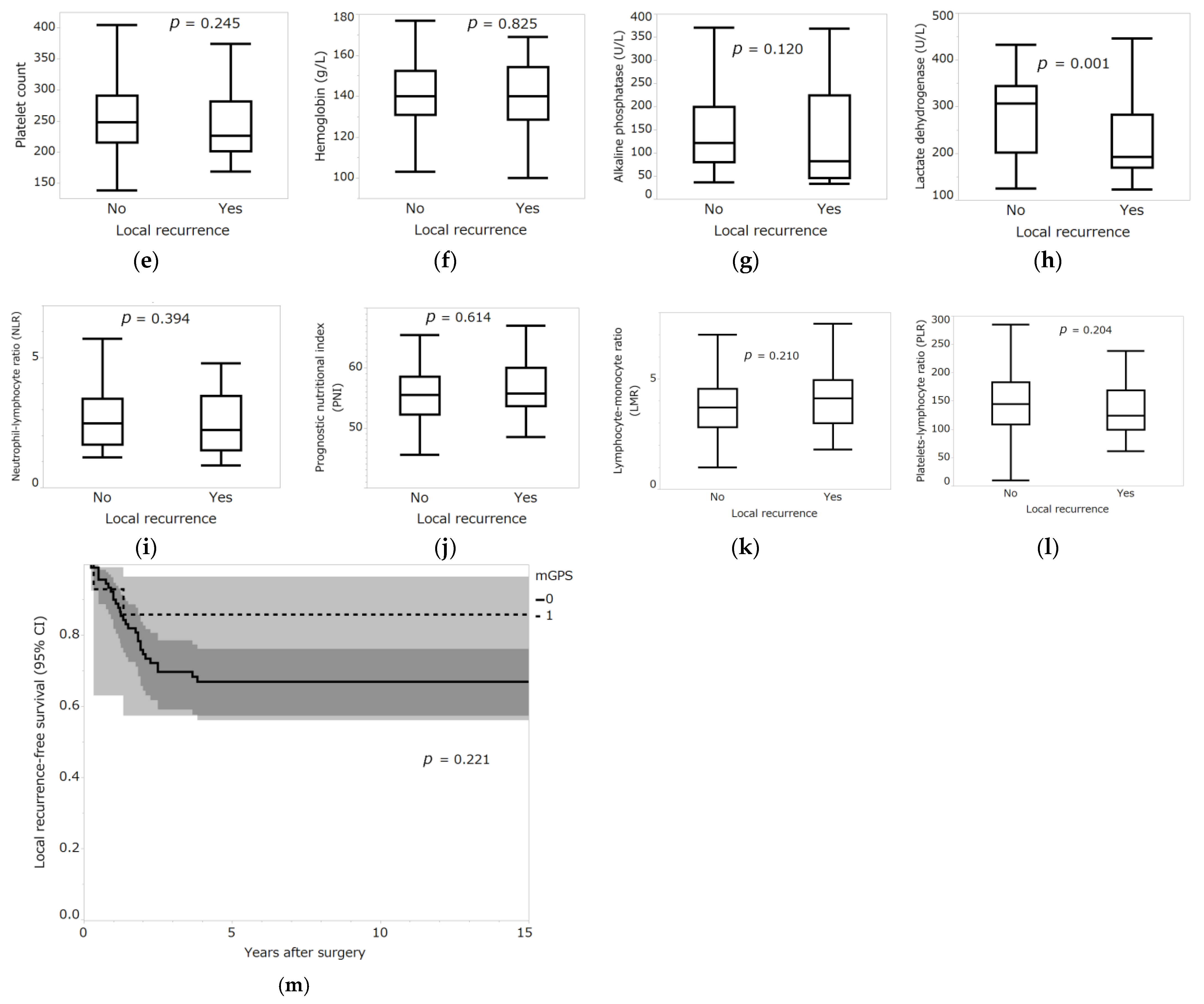
| Variable | Local Recurrence: No (Median (IQR)) | Local Recurrence: Yes (Median (IQR)) | p-Value |
|---|---|---|---|
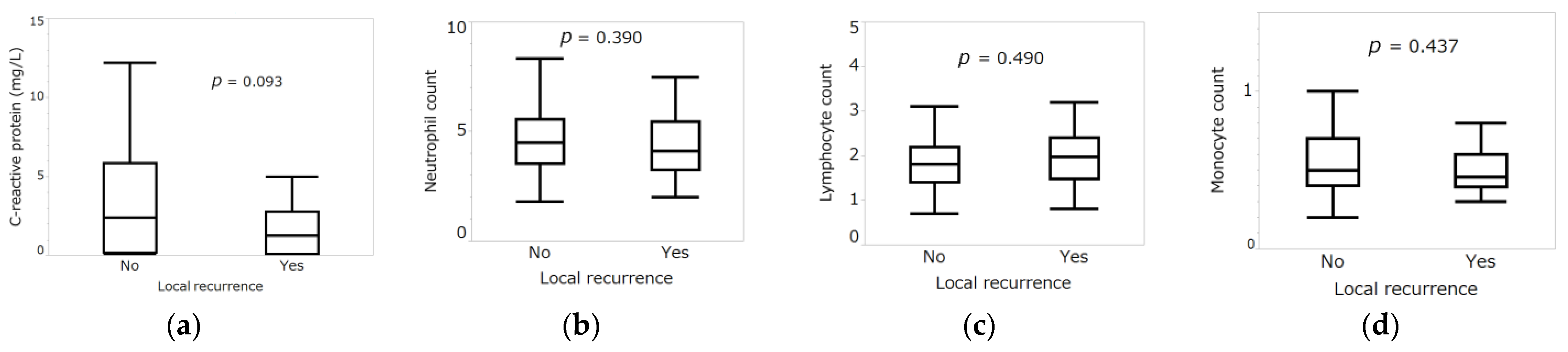
| C-reactive protein (mg/L) | 2.4 (0.2–5.85) | 1.25 (0.1–2.78) | 0.093 |
| Neutrophil count (×109/L) | 4.5 (3.55–5.55) | 4.1 (3.25–5.45) | 0.390 |
| Lymphocyte count (×109/L) | 2 (1.55–2.5) | 2.25 (1.58–3.05) | 0.490 |
| Monocyte count (×109/L) | 0.5 (0.4–0.7) | 0.46 (0.39–0.6) | 0.437 |
| Platelet count (×109/L) | 248 (215–291) | 226 (201–282) | 0.245 |
| Hemoglobin (g/L) | 140 (131–152.5) | 140 (128.5–154.3) | 0.825 |
| Alkaline phosphatase (U/L) | 122 (79.5–199.5) | 82 (45.5–224) | 0.120 |
| Lactate dehydrogenase (U/L) | 307 (202–344.5) | 192 (169.5–283.3) | 0.001 * |
| Neutrophil–lymphocyte ratio (NLR) | 2.48 (1.65–3.41) | 2.21 (1.44–3.53) | 0.394 |
| Prognostic nutritional index (PNI) | 55.5 (52.3–58.6) | 55.8 (53.6–60) | 0.614 |
| Lymphocyte-monocyte ratio (LMR) | 3.71 (2.82–4.55) | 4.13 (3–4.95) | 0.210 |
| Platelet-lymphocyte ratio (PLR) | 144 (109–183) | 124 (100–169) | 0.204 |
| Modified Glasgow prognostic score (mGPS) | No. of patients (n = 103) | 5-year local recurrence-free survival (95% CI) (%) | p-value |
| 0 | 89 | 66.8 (56–76.1) | 0.221 |
| 1 | 14 | 85.7 (57.3–96.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsukamoto, S.; Mavrogenis, A.F.; Alvarado, R.A.; Traversari, M.; Akahane, M.; Honoki, K.; Tanaka, Y.; Donati, D.M.; Errani, C. Association between Inflammatory Markers and Local Recurrence in Patients with Giant Cell Tumor of Bone: A Preliminary Result. Curr. Oncol. 2023, 30, 1116-1131. https://doi.org/10.3390/curroncol30010085
Tsukamoto S, Mavrogenis AF, Alvarado RA, Traversari M, Akahane M, Honoki K, Tanaka Y, Donati DM, Errani C. Association between Inflammatory Markers and Local Recurrence in Patients with Giant Cell Tumor of Bone: A Preliminary Result. Current Oncology. 2023; 30(1):1116-1131. https://doi.org/10.3390/curroncol30010085
Chicago/Turabian StyleTsukamoto, Shinji, Andreas F. Mavrogenis, Rebeca Angulo Alvarado, Matteo Traversari, Manabu Akahane, Kanya Honoki, Yasuhito Tanaka, Davide Maria Donati, and Costantino Errani. 2023. "Association between Inflammatory Markers and Local Recurrence in Patients with Giant Cell Tumor of Bone: A Preliminary Result" Current Oncology 30, no. 1: 1116-1131. https://doi.org/10.3390/curroncol30010085
APA StyleTsukamoto, S., Mavrogenis, A. F., Alvarado, R. A., Traversari, M., Akahane, M., Honoki, K., Tanaka, Y., Donati, D. M., & Errani, C. (2023). Association between Inflammatory Markers and Local Recurrence in Patients with Giant Cell Tumor of Bone: A Preliminary Result. Current Oncology, 30(1), 1116-1131. https://doi.org/10.3390/curroncol30010085