Matrix for Mucosal Regeneration in Transoral Glossectomy for Squamous Cell Carcinoma: Objective and Subjective Functional Evaluation

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
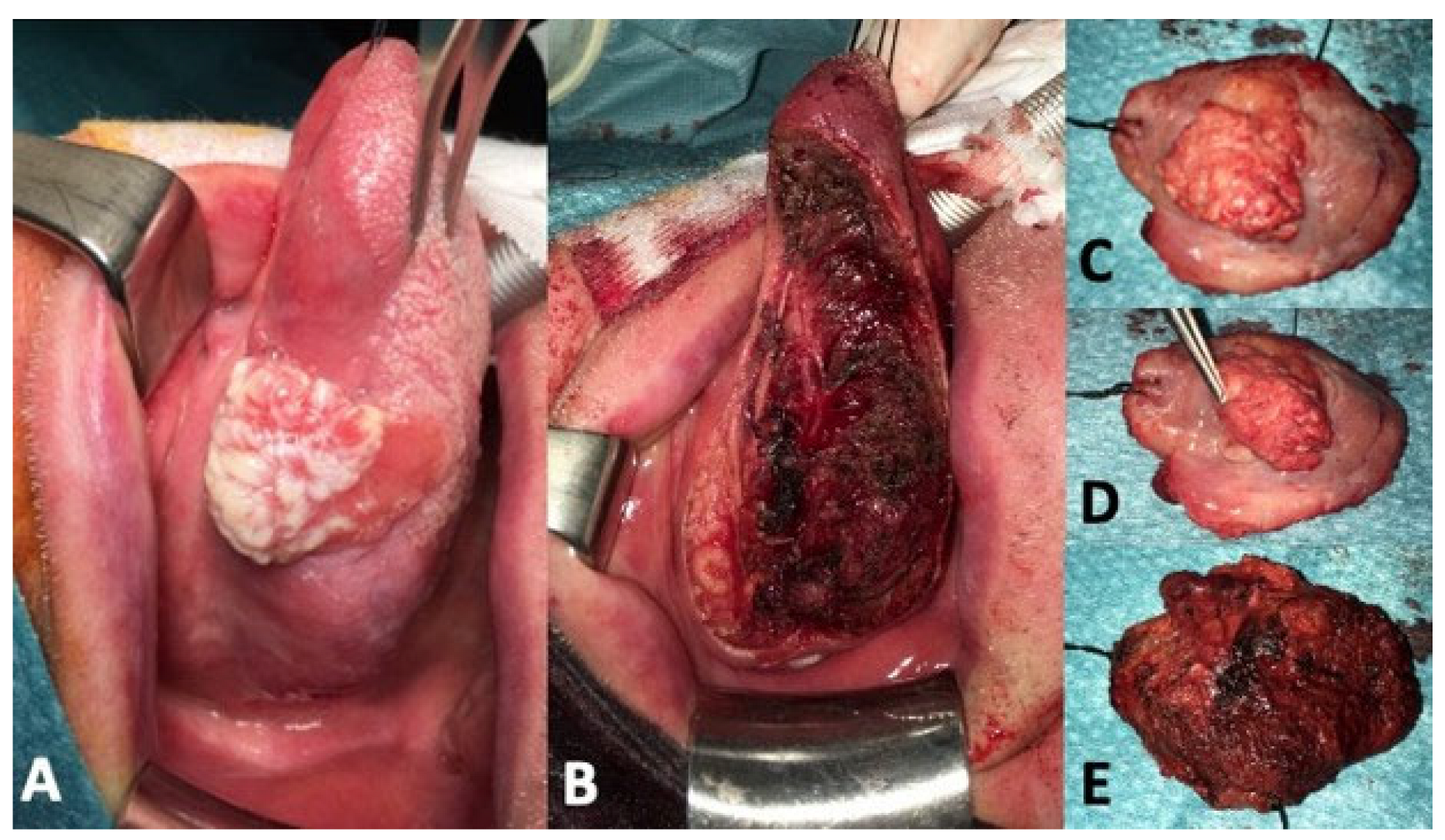
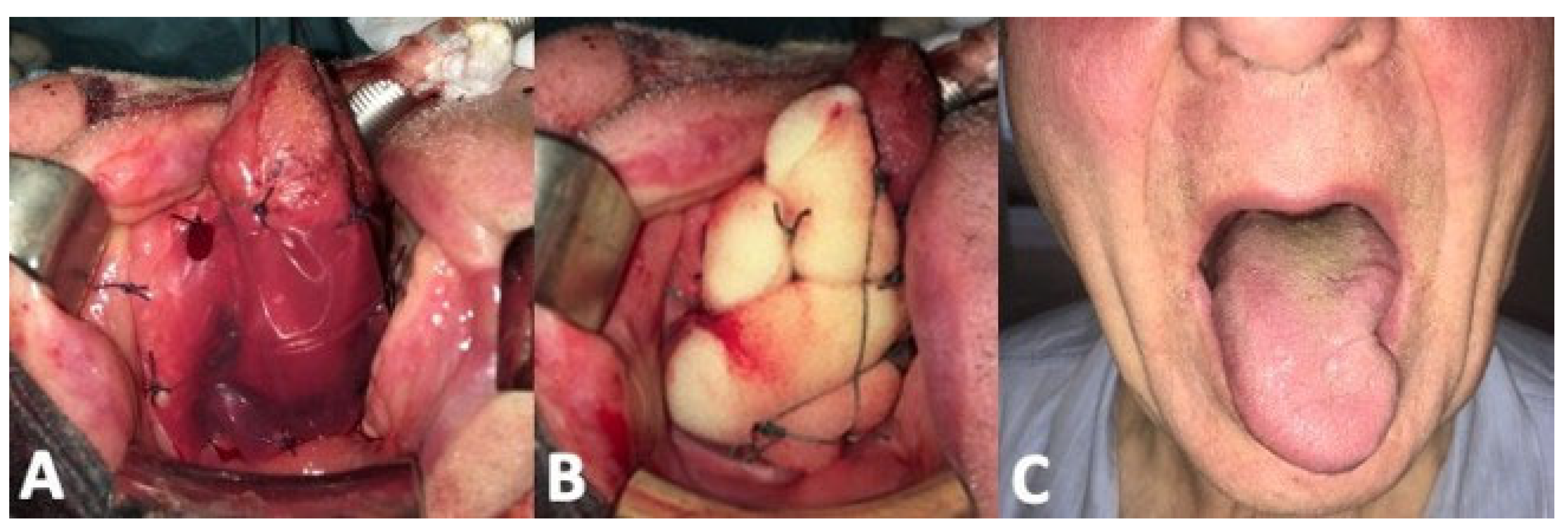
3.1. Clinical Results
3.2. Functional Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deganello, A. Modern oral cavity reconstruction with free flaps and pedicled flaps. J. Aesth. Reconstr. Surg. 2015, 1, 4. [Google Scholar] [CrossRef] [Green Version]
- Deganello, A.; Rampinelli, V.; Gualtieri, T.; Piazza, C. Versatility of the subscapular system of flaps in head and neck oncologic reconstruction. Curr. Opin. Otolaryngol. Head Neck Surg. 2022, 30, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.S.; Wells, M.; Ascha, M.; Duggal, R.; Gatherwright, J.; Chepla, K. Head and Neck Wound Reconstruction Using Biodegradable Temporizing Matrix versus Collagen-Chondroitin Silicone Bilayer. Eplasty 2022, 22, e31. [Google Scholar] [PubMed]
- Ching, J.A.; Gould, L. Giant scalp melanoma: A case report and review of the literature. Eplasty 2012, 12, e51. [Google Scholar] [PubMed]
- Srivastava, A.; Maniakas, A.; Myers, J.; Chambers, M.S.; Cardoso, R. Reconstruction of intraoral oncologic surgical defects with Integra® bilayer wound matrix. Clin. Case Rep. 2020, 9, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Mattavelli, D.; Ferrari, M.; Taboni, S.; Morello, R.; Paderno, A.; Rampinelli, V.; Del Bon, F.; Lombardi, D.; Grammatica, A.; Bossi, P.; et al. The 8th TNM classification for oral squamous cell carcinoma: What is gained, what is lost, and what is missing. Oral Oncol. 2020, 111, 104937. [Google Scholar] [CrossRef] [PubMed]
- Gualtieri, T.; Verzeletti, V.; Ferrari, M.; Perotti, P.; Morello, R.; Taboni, S.; Palumbo, G.; Ravanelli, M.; Rampinelli, V.; Mattavelli, D.; et al. A new landmark for lingual artery identification during transoral surgery: Anatomic-radiologic study. Head Neck 2021, 43, 1487–1498. [Google Scholar] [CrossRef] [PubMed]
- Donzelli, J.; Brady, S.; Wesling, M.; Craney, M. Predictive value of accumulated oropharyngeal secretions for aspiration during video nasal endoscopic evaluation of the swallow. Ann. Otol. Rhinol. Laryngol. 2003, 112, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Grammatica, A.; Piazza, C.; Montalto, N.; Del Bon, F.; Frittoli, B.; Mazza, M.; Paderno, A.; Lancini, D.; Fior, M.; Deganello, A.; et al. Compartmental Surgery for Oral Tongue Cancer: Objective and Subjective Functional Evaluation. Laryngoscope 2021, 131, E176–E183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahieu, R.; Colletti, G.; Bonomo, P.; Parrinello, G.; Iavarone, A.; Dolivet, G.; Livi, L.; Deganello, A. Head and neck reconstruction with pedicled flaps in the free flap era. Acta Otorhinolaryngol. Ital. 2016, 36, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Deganello, A.; Leemans, C.R. The infrahyoid flap: A comprehensive review of an often overlooked reconstructive method. Oral Oncol. 2014, 50, 704–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deganello, A.; Gitti, G.; Parrinello, G.; Larotonda, G.; Meccariello, G.; Leemans, C.R.; Gallo, O. Infrahyoid flap reconstruction of oral cavity and oropharyngeal defects in elderly patients with severe general comorbidities. Head Neck 2012, 34, 1299–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gore, D.C. Outcome and cost analysis for outpatient skin grafting. J. Trauma 1997, 43, 597–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hulsey, A.; Linneman, P.; Litt, J. Clinical Usage and Economic Effectiveness of a Recently Developed Epidermal Autograft Harvesting System in 13 Chronic Wound Patients in a University Based Wound Center. Cureus 2016, 8, e878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fatah, M.F.; Ward, C.M. The morbidity of split-skin graft donor sites in the elderly: The case for mesh-grafting the donor site. Br. J. Plast. Surg. 1984, 37, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Petrie, K.; Cox, C.T.; Becker, B.C.; MacKay, B.J. Clinical applications of acellular dermal matrices: A review. Scars Burn. Heal. 2022, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.I.; Yu, P.; Skoracki, R.J.; Liu, J.; Hanasono, M.M. Comprehensive analysis of functional outcomes and survival after microvascular reconstruction of glossectomy defects. Ann. Surg. Oncol. 2015, 22, 3061–3069. [Google Scholar] [CrossRef] [PubMed]
- Lwin, C.T.; Hanlon, R.; Lowe, D.; Brown, J.S.; Woolgar, J.A.; Triantafyllou, A.; Rogers, S.N.; Bekiroglu, F.; Lewis-Jones, H.; Wieshmann, H.; et al. Accuracy of MRI in prediction of tumour thickness and nodal stage in oral squamous cell carcinoma. Oral Oncol. 2012, 48, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Mair, M.; Raj, L.; Mahmood, S.; Fagiry, R.; Ahmed, M.M.; Menon, I.; Ibrahim, N.; Ameerally, P.; Baker, A.; Vaidhyanath, R. Diagnostic accuracy of magnetic resonance imaging in detecting depth of invasion of tongue cancers. Br. J. Oral Maxillofac. Surg. 2021, 59, 1275–1279. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, O.; Knutsson, J.; Landström, F.J.; Magnuson, A.; von Beckerath, M. Ultrasound accurately assesses depth of invasion in T1–T2 oral tongue cancer. Laryngoscope Investig. Otolaryngol. 2022, 24, 1448–1455. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| pT | Margins | PnI 1 | LvI 2 | Subsite | Initial Defect Size (cm2) | Final Defect Size (cm2) | Non-Evidence of Disease (Months) | |
|---|---|---|---|---|---|---|---|---|
| Pt.1 | 2 | Close | + | - | Ant | 20 | 12 | 60 |
| Pt.2 | 3 | Negative | + | Middle | 22 | 13 | 56 | |
| Pt.3 | 1 | Negative | - | - | Ant | 19 | 9 | 47 |
| Pt.4 | 1 | Close | + | + | Middle | 15 | 8 | 40 |
| Pt.5 | 1 | Close | - | - | Middle | 18 | 10 | 33 |
| Pt.6 | Tis | Negative | // | // | Ant | 15 | 7 | 29 |
| Pt.7 | 1 | Negative | - | - | Ant | 17 | 9 | 23 |
| Pt.8 | 1 | Negative | - | - | Middle | 18 | 11 | 18 |
| Pt.9 | Tis | Negative | // | // | Middle | 12 | 7 | 15 |
| Pt.10 | 1 | Negative | + | - | Ant | 18 | 11 | 9 |
| Pt.11 | Tis | Negative | // | // | Middle | 16 | 10 | 7 |
| Pt.12 | 1 | Negative | + | - | Middle | 21 | 13 | 4 |
| Pt.13 | 2 | Negative | // | // | Ant | 20 | 14 | 3 |
| Test | Results | |
|---|---|---|
| Donzelli Score | I | 100% |
| II | 0% | |
| III | 0% | |
| Post-Swallowing pooling | Yes | 16.7% |
| No | 83.3% | |
| Speech Evaluation | Average recognized words | 70.5/75 |
| Lingual Motility Score | Superior | 2.67/3 |
| Inferior | 1.83/3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deganello, A.; Bosio, P.; Giannini, L.; Parolini, F.; Berretti, G.; Sordi, A.; Rampinelli, V.; Gualtieri, T. Matrix for Mucosal Regeneration in Transoral Glossectomy for Squamous Cell Carcinoma: Objective and Subjective Functional Evaluation. Curr. Oncol. 2023, 30, 1354-1362. https://doi.org/10.3390/curroncol30020104
Deganello A, Bosio P, Giannini L, Parolini F, Berretti G, Sordi A, Rampinelli V, Gualtieri T. Matrix for Mucosal Regeneration in Transoral Glossectomy for Squamous Cell Carcinoma: Objective and Subjective Functional Evaluation. Current Oncology. 2023; 30(2):1354-1362. https://doi.org/10.3390/curroncol30020104
Chicago/Turabian StyleDeganello, Alberto, Paolo Bosio, Lorenzo Giannini, Federico Parolini, Giulia Berretti, Alessandra Sordi, Vittorio Rampinelli, and Tommaso Gualtieri. 2023. "Matrix for Mucosal Regeneration in Transoral Glossectomy for Squamous Cell Carcinoma: Objective and Subjective Functional Evaluation" Current Oncology 30, no. 2: 1354-1362. https://doi.org/10.3390/curroncol30020104
APA StyleDeganello, A., Bosio, P., Giannini, L., Parolini, F., Berretti, G., Sordi, A., Rampinelli, V., & Gualtieri, T. (2023). Matrix for Mucosal Regeneration in Transoral Glossectomy for Squamous Cell Carcinoma: Objective and Subjective Functional Evaluation. Current Oncology, 30(2), 1354-1362. https://doi.org/10.3390/curroncol30020104