Multisite Quality Improvement Initiative to Identify and Address Racial Disparities and Deficiencies in Delivering Equitable, Patient-Centered Care for Multiple Myeloma—Exploring the Differences between Academic and Community Oncology Centers

 , , and
, , and
Abstract
:1. Introduction
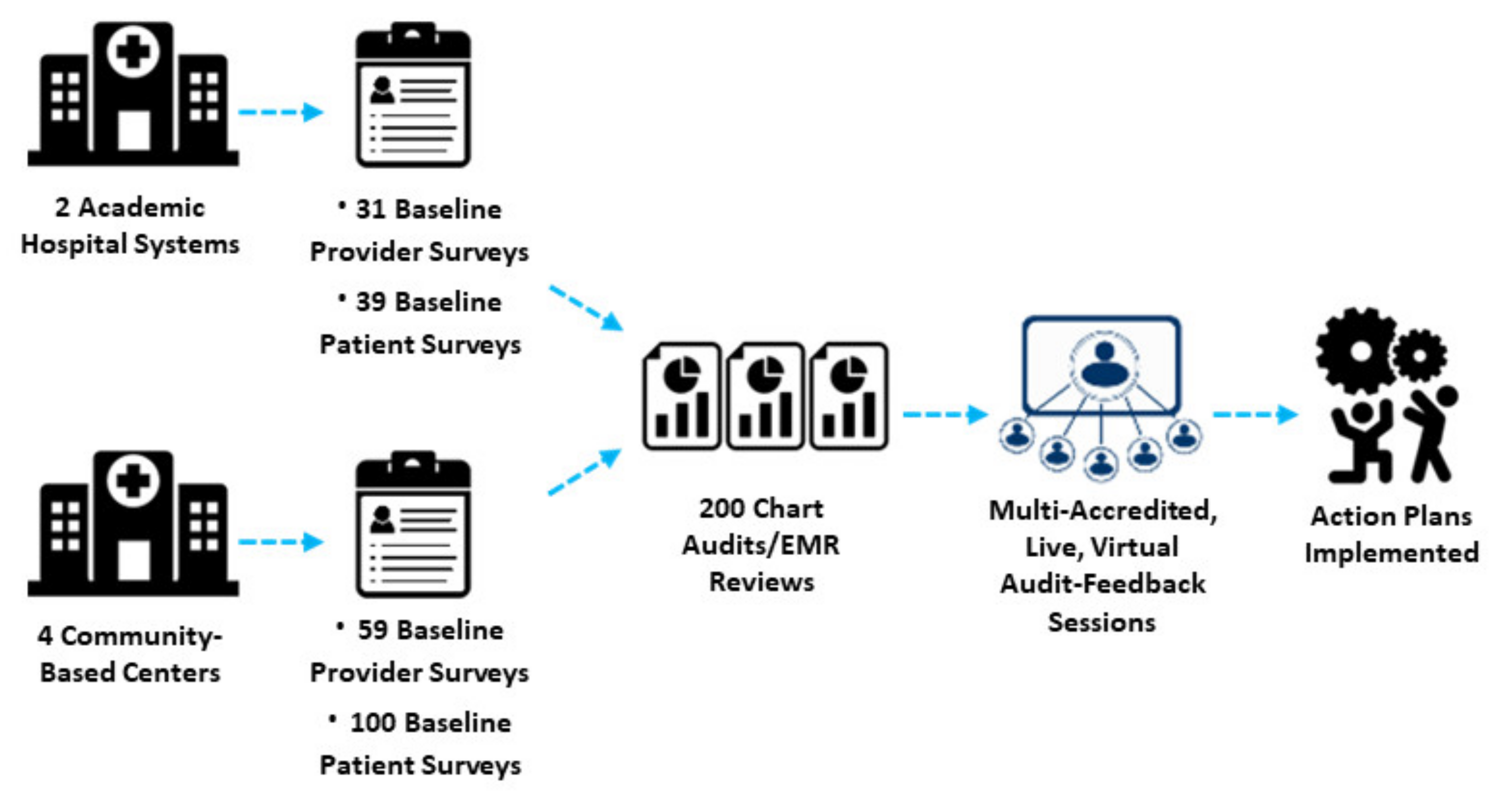
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Waxman, A.J.; Mink, P.J.; Devesa, S.S.; Anderson, W.F.; Weiss, B.M.; Kristinsson, S.Y.; McGlynn, K.A.; Landgren, O. Racial disparities in incidence and outcome in multiple myeloma: A population-based study. Blood 2010, 116, 5501–5506. [Google Scholar] [CrossRef] [Green Version]
- Ailawadhi, S.; Parikh, K.; Abouzaid, S.; Zhou, Z.; Tang, W.; Clancy, Z.; Cheung, C.; Zhou, Z.-Y.; Xie, J. Racial disparities in treatment patterns and outcomes among patients with multiple myeloma: A SEER-Medicare analysis. Blood Adv. 2019, 3, 2986–2994. [Google Scholar] [CrossRef] [Green Version]
- Goto, D.; Khairnar, R.; Yared, J.A.; Yong, C.; Romanus, D.; Onukwugha, E.; Slejko, J.F. Utilization of novel systemic therapies for multiple myeloma: A retrospective study of front-line regimens using the SEER-Medicare data. Cancer Med. 2019, 9, 626–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unger, J.M.; Hershman, D.L.; Osarogiagbon, R.U.; Gothwal, A.; Anand, S.; Dasari, A.; Overman, M.; Loree, J.M.; Raghav, K. Representativeness of Black Patients in Cancer Clinical Trials Sponsored by the National Cancer Institute Compared With Pharmaceutical Companies. JNCI Cancer Spectr. 2020, 4, pkaa034. [Google Scholar] [CrossRef]
- Ailawadhi, S.; Bhatia, K.; Aulakh, S.; Meghji, Z.; Chanan-Khan, A. Equal treatment and outcomes for everyone with multiple myeloma: Are we there yet? Curr. Hematol. Malig. Rep. 2017, 12, 309–316. [Google Scholar] [CrossRef]
- Ailawadhi, S.; Frank, R.D.; Advani, P.; Swaika, A.; Temkit, M.; Menghani, R.; Sharma, M.; Meghji, Z.; Paulus, S.; Khera, N.; et al. Racial disparity in utilization of therapeutic modalities among multiple myeloma patients: A SEER-medicare analysis. Cancer Med. 2017, 6, 2876–2885. [Google Scholar] [CrossRef] [PubMed]
- Ailawadhi, S.; Frank, R.D.; Sharma, M.; Menghani, R.; Temkit, M.; Paulus, S.; Khera, N.; Hashmi, S.; Advani, P.; Swaika, A.; et al. Trends in multiple myeloma presentation, management, cost of care, and outcomes in the Medicare population: A comprehensive look at racial disparities. Cancer 2018, 124, 1710–1721. [Google Scholar] [CrossRef] [Green Version]
- Ailawadhi, S.; Jacobus, S.; Sexton, R.; Stewart, A.K.; Dispenzieri, A.; Hussein, M.A.; Zonder, J.A.; Crowley, J.; Hoering, A.; Barlogie, B.; et al. Disease and outcome disparities in multiple myeloma: Exploring the role of race/ethnicity in the Cooperative Group clinical trials. Blood Cancer J. 2018, 8, 67. [Google Scholar] [CrossRef] [Green Version]
- Costa, L.J.; Brill, I.K.; Omel, J.; Godby, K.; Kumar, S.K.; Brown, E.E. Recent trends in multiple myeloma incidence and survival by age, race, and ethnicity in the United States. Blood Adv. 2017, 1, 282–287. [Google Scholar] [CrossRef] [Green Version]
- Fiala, M.A.; Wildes, T.M. Racial disparities in treatment use for multiple myeloma. Cancer 2017, 123, 1590–1596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirtane, K.; Lee, S.J. Racial and ethnic disparities in hematologic malignancies. Blood 2017, 130, 1699–1705. [Google Scholar] [CrossRef] [Green Version]
- Joseph, N.; Gupta, V.A.; Hofmeister, C.C.; Gleason, C.; Heffner, L.; Boise, L.H.; Kaufman, J.L.; Dhodapkar, M.V.; Lonial, S.; Nooka, A.K. Differences in Presentation and Survival Outcomes for African American Patients with Newly Diagnosed Multiple Myeloma. Blood 2018, 132, 5647. [Google Scholar] [CrossRef]
- Bhatnagar, V.; Wu, Y.; Goloubeva, O.G.; Ruehle, K.T.; Milliron, T.E.; Harris, C.G.; Rapoport, A.P.; Yanovich, S.; Sausville, E.A.; Baer, M.R.; et al. Disparities in black and white patients with multiple myeloma referred for autologous hematopoietic transplantation: A single center study. Cancer 2014, 121, 1064–1070. [Google Scholar] [CrossRef] [PubMed]
- Fillmore, N.R.; Yellapragada, S.V.; Ifeorah, C.; Mehta, A.; Cirstea, D.; White, P.S.; Rivero, G.; Zimolzak, A.; Pyarajan, S.; Do, N.; et al. With equal access, African American patients have superior survival compared to white patients with multiple myeloma: A VA study. Blood 2019, 133, 2615–2618. [Google Scholar] [CrossRef]
- Ganguly, S.; Mailankody, S.; Ailawadhi, S. Many Shades of Disparities in Myeloma Care. Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Alqazaqi, R.; Schinke, C.; Thanendrarajan, S.; Zangari, M.; Shaughnessy, J.; Zhan, F.; Tricot, G.; van Rhee, F.; Al Hadidi, S. Geographic and Racial Disparities in Access to Chimeric Antigen Receptor–T Cells and Bispecific Antibodies Trials for Multiple Myeloma. JAMA Netw. Open 2022, 5, e2228877. [Google Scholar] [CrossRef]
- LeBlanc, T.; Gasparetto, C.; Tuchman, S.A.; Sheldon, P.; Howson, A.; Turell, W.; Khan, Z.M.; Kaura, S.; Abernethy, A.P. Exploring variations in multiple myeloma management through in-practice research. J. Clin. Oncol. 2014, 32, e19534. [Google Scholar] [CrossRef]
- Melas, M.; Subbiah, S.; Saadat, S.; Rajurkar, S.; McDonnell, K.J. The Community Oncology and Academic Medical Center Alliance in the Age of Precision Medicine: Cancer Genetics and Genomics Considerations. J. Clin. Med. 2020, 9, 2125. [Google Scholar] [CrossRef]
- Levit, L.A.; Kim, E.S.; McAneny, B.L.; Nadauld, L.D.; Levit, K.; Schenkel, C.; Schilsky, R.L. Implementing Precision Medicine in Community-Based Oncology Programs: Three Models. J. Oncol. Pract. 2019, 15, 325–329. [Google Scholar] [CrossRef]
- Thompson, M.A.; Godden, J.J.; Weissman, S.M.; Wham, D.; Wilson, A.; Ruggeri, A.; Mullane, M.P.; Weese, J.L. Implementing an oncology precision medicine clinic in a large community health system. Am. J. Manag. Care 2017, 23, SP425–SP427. [Google Scholar]
- Roper, W.L.; Newton, W.P. The Role of Academic Health Centers in Improving Health. Ann. Fam. Med. 2006, 4, S55–S57. [Google Scholar] [CrossRef] [Green Version]
- Khotskaya, Y.B.; Mills, G.B.; Shaw, K.R.M. Next-Generation Sequencing and Result Interpretation in Clinical Oncology: Challenges of Personalized Cancer Therapy. Annu. Rev. Med. 2017, 68, 113–125. [Google Scholar] [CrossRef]
- Blazer, K.R.; Nehoray, B.; Solomon, I.; Niell-Swiller, M.; Culver, J.O.; Uman, G.C.; Weitzel, J.N. Next-Generation Testing for Cancer Risk: Perceptions, Experiences, and Needs Among Early Adopters in Community Healthcare Settings. Genet. Test. Mol. Biomark. 2015, 19, 657–665. [Google Scholar] [CrossRef] [Green Version]
- Thompson, M.A.; Godden, J.J.; Wham, D.; Ruggeri, A.; Mullane, M.P.; Wilson, A.; Virani, S.; Weissman, S.M.; Ramczyk, B.; Vanderwall, P.; et al. Coordinating an Oncology Precision Medicine Clinic Within an Integrated Health System: Lessons Learned in Year One. J. Patient-Cent. Res. Rev. 2019, 6, 36–45. [Google Scholar] [CrossRef] [Green Version]
- Davis, D.A.; Thomson, M.A.; Oxman, A.D.; Haynes, R.B. Changing physician performance. A systematic review of the effect of continuing medical education strategies. JAMA 1995, 274, 700–705. [Google Scholar] [CrossRef] [PubMed]
- Battat, R.; Galati, J.S.; Lukin, D.M.; Chabouni, F.; Sockolow, R.; Carter, J.; Fajardo, K.M.; Yang, S.B.; Reich, J.B.; Jacobs, V.; et al. A Quality Improvement Initiative Is Associated With Reduced Time to Administer Biologics and Small Molecules and Emergency Room Visits in Inflammatory Bowel Disease. J. Clin. Gastroenterol. 2022, 56, e176–e182. [Google Scholar] [CrossRef]
- Moreo, K.; Sapir, T.; Greene, L. Comparing Patient and Provider Perceptions of Engagement and Care in Chronic Diseases. J. Contin. Educ. Health Prof. 2016, 36, S44–S45. [Google Scholar] [CrossRef]
- Sapir, T.; Moreo, K.; Carter, J.D.; Greene, L.; Patel, B.; Higgins, P.D.R. Continuing Medical Education Improves Gastroenterologists’ Compliance with Inflammatory Bowel Disease Quality Measures. Dig. Dis. Sci. 2016, 61, 1862–1869. [Google Scholar] [CrossRef] [PubMed]
- Moreo, K.; Greene, L.; Sapir, T. Improving Interprofessional and Coproductive Outcomes of Care for Patients with Chronic Obstructive Pulmonary Disease. BMJ Qual. Improv. Rep. 2016, 5, u210329-w4679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penner, L.A.; Dovidio, J.F.; Hagiwara, N.; Foster, T.; Albrecht, T.L.; Chapman, R.A.; Eggly, S. An Analysis of Race-related Attitudes and Beliefs in Black Cancer Patients: Implications for Health Care Disparities. J. Health Care Poor Underserved 2016, 27, 1503–1520. [Google Scholar] [CrossRef] [Green Version]
- Suzanne Lea, C.; Bohra, S.; Moore, T.; Passwater, C.; Liles, D. Exploring behaviors, treatment beliefs, and barriers to oral chemotherapy adherence among adult leukemia patients in a rural outpatient setting. BMC Res. Notes 2018, 11, 1–6. [Google Scholar]
- Assari, S.; Khoshpouri, P.; Chalian, H. Combined Effects of Race and Socioeconomic Status on Cancer Beliefs, Cognitions, and Emotions. Healthcare 2019, 7, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White-Means, S.I.; Osmani, A.R. Racial and Ethnic Disparities in Patient-Provider Communication With Breast Cancer Patients: Evidence From 2011 MEPS and Experiences With Cancer Supplement. Inq. J. Health Care Organ. Provis. Financ. 2017, 54, 46958017727104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Check, D.K.; Chawla, N.; Kwan, M.L.; Pinheiro, L.; Roh, J.M.; Ergas, I.J.; Stewart, A.L.; Kolevska, T.; Ambrosone, C.; Kushi, L.H. Understanding racial/ethnic differences in breast cancer-related physical well-being: The role of patient–provider interactions. Breast Cancer Res. Treat. 2018, 170, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Benz, J.K.; Espinosa, O.; Welsh, V.; Fontes, A. Awareness Of Racial And Ethnic Health Disparities Has Improved Only Modestly Over A Decade. Health Aff. 2011, 30, 1860–1867. [Google Scholar] [CrossRef]
- Pritlove, C.; Jassi, M.; Burns, B.; McCurdy, A. The work of managing multiple myeloma and its implications for treatment-related decision making: A qualitative study of patient and caregiver experiences. BMC Cancer 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Janssens, R.; Lang, T.; Vallejo, A.; Galinsky, J.; Plate, A.; Morgan, K.; Cabezudo, E.; Silvennoinen, R.; Coriu, D.; Badelita, S.; et al. Patient Preferences for Multiple Myeloma Treatments: A Multinational Qualitative Study. Front. Med. 2021, 8, 686165. [Google Scholar] [CrossRef]
- Copur, M.S. Inadequate Awareness of and Participation in Cancer Clinical Trials in the Community Oncology Setting. Oncology 2019, 33, 54–57. [Google Scholar]
- Clauser, S.B.; Johnson, M.R.; O’Brien, D.M.; Beveridge, J.M.; Fennell, M.L.; Kaluzny, A.D. Improving clinical research and cancer care delivery in community settings: Evaluating the NCI community cancer centers program. Implement. Sci. 2009, 4, 63. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, B.R.; Locke, S.C.; Abernethy, A.P. Experience of the National Cancer Institute Community Cancer Centers Program on Community-Based Cancer Clinical Trials Activity. J. Oncol. Pract. 2016, 12, e350–e358. [Google Scholar] [CrossRef] [Green Version]
- Green, M.A.; Michaels, M.; Blakeney, N.; Odulana, A.A.; Isler, M.R.; Richmond, A.; Long, D.G.; Robinson, W.S.; Taylor, Y.J.; Corbie-Smith, G. Evaluating a community-partnered cancer clinical trials pilot intervention with African American communities. J. Cancer Educ. 2015, 30, 158–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierre, A.; Williams, T.H. African American Patients With Multiple Myeloma: Optimizing Care to Decrease Racial Disparities. Clin. J. Oncol. Nurs. 2020, 24, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Marinac, C.R.; Ghobrial, I.M.; Birmann, B.M.; Soiffer, J.; Rebbeck, T.R. Dissecting racial disparities in multiple myeloma. Blood Cancer J. 2020, 10, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gormley, N.; Fashoyin-Aje, L.; Locke, T.; Unger, J.M.; Little, R.F.; Nooka, A.; Mezzi, K.; Popa-McKiver, M.; Kobos, R.; Biru, Y.; et al. Recommendations on Eliminating Racial Disparities in Multiple Myeloma Therapies: A Step toward Achieving Equity in Healthcare. Blood Cancer Discov. 2021, 2, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Maignan, K.; Fashoyin-Aje, L.A.; Torres, A.Z.; Fernandes, L.L.; Gwise, T.; Baxi, S.B.; Roose, J.P.; Rivera, D.R.; Shen, Y.L.; Kluetz, P.G.; et al. Exploring racial disparities in treatment patterns and outcomes for patients with multiple myeloma using real world data. Blood Cancer J. 2022, 12, 1–6. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Baseline Chart Audits | |||
| Academic Patients (n = 200) | Community Patients (n = 200) | p-Value 1 | |
| African American/Black | 105 (53%) | 32 (16%) | <0.001 |
| Non-African American | 95 (47%) | 133 (67%) | |
| Race Not Documented | 0 (0%) | 35 (17%) | |
| Mean age | 70 years | 71 years | 0.285 |
| Male sex | 68% | 46% | 0.001 |
| Patient and Provider Surveys | |||
| Academic Patients (n = 39) | Community Patients (n = 100) | ||
| Mean age | 63 years | 62 years | 0.676 |
| African American/Black | 67% | 47% | 0.001 |
| Hispanic/Latino | 18% | 3% | |
| Asian/Pacific Islander | 10% | 0% | |
| Native American/Alaska Native | 5% | 0% | |
| White | 0% | 50% | |
| Mean years attending clinic for MM care | 3.5 years | 5.5 years | 0.032 |
| Academic Providers (n = 31) | Community Providers (n = 59) | ||
| Hematologist/Oncologist | 65% | 29% | 0.011 |
| Primary Care Physician/Other Physician | 0% | 14% | |
| NP/PA | 12% | 22% | |
| Nurse | 23% | 32% | |
| Other | 0% | 3% | |
| African American/Black | 45% | 8% | 0.001 |
| Caucasian/White | 29% | 75% | |
| Hispanic/Latino | 16% | 0% | |
| Asian/Pacific Islander | 10% | 17% | |
| Mean patients with MM seen per month | 9 patients | 49 patients | 0.001 |
| Mean years caring for patients with MM | 17 years | 9 years | 0.001 |
| Feedback-Focused Educational Sessions | |||
| Academic Providers (n = 58) | Community Providers (n = 59) | ||
| Hematologist/Oncologist | 84% | 29% | 0.001 |
| NP/PA | 5% | 22% | |
| Nurse/Patient navigator/Case manager | 10% | 31% | |
| Primary Care Physician | 0% | 14% | |
| Other | 0% | 5% | |
| Learners’ self-reported monthly caseload of patients with MM (mean) | 514 patients | 1699 patients | 0.001 |
| Academic Patients (n = 200) | Community Patients (n = 200) | p-Value 2 | |
|---|---|---|---|
| Disease Characteristics | |||
| Disease Stage | 48% | 29% | <0.001 |
| Stage 1 | 24% | 8% | <0.001 |
| Stage 2 | 20% | 8% | <0.001 |
| Stage 3 | 4% | 14% | <0.001 |
| Stage Not Documented | 52% | 71% | <0.001 |
| Cytogenetics | 40% | 8% | <0.001 |
| t(4;14) | 6% | 4% | 0.359 |
| Imaging | 97% | 79% | <0.001 |
| Patient-Centered Care Practices | |||
| Referrals/ongoing management of comorbidities | 20% | 5% | <0.001 |
| Response evaluation | 85% | 84% | 0.777 |
| Provision of patient education | 24% | 22% | 0.634 |
| Involvement of interprofessional team in diagnostic and prognostic tests | 24% | 47% | <0.001 |
| Advance care planning documentation | 25% | 70% | <0.001 |
| Assessment of side effects | 25% | 27% | 0.648 |
| Assessment of adherence | 30% | 37% | 0.138 |
| Assessment of patient-reported function | 38% | 49% | 0.026 |
| Assessment of patient-reported quality of life | 39% | 45% | 0.224 |
| Assessment of alcohol | 68% | 91% | <0.001 |
| Shared Decision-Making Practices | |||
| Checking for the patient/caregiver understanding of treatment options | 24% | 26% | 0.644 |
| Exploring patient/caregiver expectations for treatment outcomes | 27% | 26% | 0.821 |
| Ask patient or caregiver about treatment goals | 28% | 30% | 0.659 |
| Exploring patient/caregiver concerns and fears | 31% | 29% | 0.663 |
| Explaining pros and cons of treatment options | 34% | 41% | 0.148 |
| Providing treatment options | 35% | 37% | 0.677 |
| Providing opportunities for patient or caregiver to ask questions | 52% | 35% | <0.001 |
| Academic | Community | |||||
|---|---|---|---|---|---|---|
| Providers (n = 31) | Patients (n = 39) | p-value 3 | Providers (n = 59) | Patients (n = 100) | p-Value 3 | |
| Challenges for Patients with MM | ||||||
| Patient prompt: What is the biggest challenge you have faced in your MM care? Provider prompt: What is the biggest challenge your patients have faced in their MM care? | ||||||
| Feeling confident in the treatment plan | 22% | 10% | 0.196 * | 18% | 32% | 0.067 |
| Choosing whether to have/worry about complications of SCT | 11% | 0% | 0.082 * | 16% | 7% | 0.095 |
| Lack of reliable transportation to and from care center | 19% | 20% | 0.920 | 5% | 10% | 0.375 * |
| Worry about working or meeting responsibilities at home | 22% | 20% | 0.841 | 18% | 18% | 0.920 |
| Difficulty communicating with care team about concerns | 15% | 25% | 0.335 | 5% | 5% | >0.999 |
| Worry about not having family/caregivers who can help | 4% | 18% | 0.069 * | 5% | 14% | 0.079 |
| Worry about the cost of treatment/financial concerns | 7% | 7% | >0.999 | 32% | 9% | <0.001 |
| Goals of Treatment | ||||||
| Patient prompt: What are your top 2 goals for MM treatment? Provider prompt: What do you believe are your patients’ top 2 goals for MM treatment? | ||||||
| Controlling symptoms | 26% | 49% | 0.050 | 34% | 24% | 0.177 |
| Improving quality of life | 52% | 49% | 0.807 | 59% | 37% | 0.006 |
| Surviving as long as possible | 56% | 33% | 0.071 | 63% | 47% | 0.055 |
| Preventing progression or recurrence | 22% | 18% | 0.623 | 25% | 43% | 0.026 |
| Maintaining independence in daily activities | 33% | 15% | 0.095 | 16% | 16% | 0.888 |
| Staying out of the emergency room/hospital | 11% | 15% | 0.721 * | 4% | 12% | 0.032 |
| Avoiding the need for a stem cell transplant | 0% | 5% | 0.499 * | 0% | 3% | 0.295 * |
| Treatment Decision-Making | ||||||
| Patient prompt: Which of the following factors are the most important for your treatment-decision making? Provider prompt: Which of the following factors are the most important for your patients’ treatment decision-making? | ||||||
| How well it will work against my/their cancer | 56% | 39% | 0.171 | 50% | 57% | 0.450 |
| Effects on quality of life | 56% | 44% | 0.351 | 54% | 45% | 0.260 |
| Risks/complications/side effects associated with the treatment | 37% | 46% | 0.532 | 57% | 29% | <0.001 |
| Cost of treatment | 19% | 26% | 0.532 | 21% | 18% | 0.718 |
| Advice from loved ones | 19% | 31% | 0.277 | 0% | 13% | 0.005 * |
| Advice/education from treatment team members | 7% | 13% | 0.452 * | 11% | 22% | 0.110 |
| Clinical Trial Experience | ||||||
| Patient prompt: Please describe your experience with clinical trials for MM (select all that apply). Provider prompt: Please rate how often you and your team do the following. | ||||||
| Patient prompt: My doctor has asked about my interest in clinical trials Provider prompt: Discuss the possibility of clinical trial enrollment | 93% | 15% | <0.001 | 88% | 21% | <0.001 |
| Patient prompt: My doctor has referred me to a clinical trial Provider prompt: Refer patients for clinical trial enrollment | 89% | 15% | <0.001 | 87% | 17% | <0.001 |
| Patient prompt: I enrolled in a clinical trial | -- | 15% | -- | -- | 15% | -- |
| Patient prompt: No experience with clinical trials | -- | 59% | -- | -- | 47% | -- |
| Topics of Discussion | ||||||
| Patient prompt: Please describe whether and how much your MM care team discussed the following topics with you. Provider prompt: Please rate how often you and your team discuss the following with your patients. | ||||||
| Long-term side effects of cancer treatment for MM | 85% | 77% | 0.474 | 96% | 83% | 0.011 |
| The need for regular follow-up care and monitoring after completing treatment for MM | 85% | 67% | 0.102 | 79% | 83% | 0.597 |
| The pros and cons of different treatment options for MM | 81% | 65% | 0.128 | 93% | 88% | 0.290 |
| Patient’s goals and preference for treatment | 81% | 70% | 0.277 | 100% | 84% | 0.001 |
| Barriers to Care Access | ||||||
| Patient prompt: Thinking about people like yourself, how much of a problem are these issues? Provider prompt: Please rate the degree of each problem (if present) for African American/Black patients relative to other patients. | ||||||
| Having enough MM doctors or treatment centers near where patients live | ||||||
| Problem (any degree) | 56% | 34% | 0.071 | 49% | 61% | 0.145 |
| Major problem | 7% | 13% | 0.452 * | 15% | 42% | <0.001 |
| Minor problem | 49% | 21% | 0.014 | 34% | 19% | 0.035 |
| Not a problem | 11% | 10% | >0.999 | 34% | 17% | 0.015 |
| Don’t know | 33% | 56% | 0.044 | 18% | 23% | 0.517 |
| Having difficulty getting the best care because of their race/ethnic background | ||||||
| Problem (any degree) | 63% | 30% | 0.005 | 44% | 40% | 0.617 |
| Major problem | 30% | 10% | 0.277 | 13% | 20% | 0.303 |
| Minor problem | 33% | 20% | 0.264 | 21% | 20% | >0.999 |
| Not a problem | 15% | 15% | >0.999 | 47% | 29% | 0.019 |
| Don’t know | 22% | 55% | 0.004 | 19% | 32% | 0.067 |
| Being able to afford the cost of health insurance and needed medical care | ||||||
| Problem (any degree) | 86% | 12% | <0.001 | 75% | 75% | >0.999 |
| Major problem | 41% | 5% | <0.001 | 31% | 44% | 0.092 |
| Minor problem | 45% | 7% | <0.001 | 44% | 31% | 0.097 |
| Not a problem | 7% | 10% | 0.687 * | 7% | 12% | 0.290 |
| Don’t know | 7% | 78% | <0.001 | 19% | 14% | 0.439 |
| Community Providers (n = 59) | Black/Latinx Patients (n = 50) | White Patients (n = 50) | |
|---|---|---|---|
| Goals of Treatment | |||
| Patient prompt: What are your top 2 goals for MM treatment? Provider prompt: What do you believe are your patients’ top 2 goals for MM treatment? | |||
| Controlling symptoms | 34% | 26% | 22% |
| Improving quality of life | 59% | 46% | 28% |
| Surviving as long as possible | 63% | 38% | 56% |
| Preventing progression or recurrence | 25% | 32% | 54% |
| Maintaining independence in daily activities | 16% | 18% | 14% |
| Staying out of the emergency room/hospital | 4% | 16% | 8% |
| Avoiding the need for a stem cell transplant | 0% | 6% | 4% |
| Treatment Decision-Making | |||
| Patient prompt: Which of the following factors are the most important for your treatment decision-making? Provider prompt: Which of the following factors are the most important for your patients’ treatment decision-making? | |||
| How well it will work against my/their cancer | 50% | 42% | 56% |
| Effects on quality of life | 54% | 60% | 42% |
| Risks/complications/side effects associated with the treatment | 57% | 36% | 30% |
| Cost of treatment | 21% | 20% | 16% |
| Advice from loved ones | 0% | 22% | 8% |
| Advice/education from treatment team members | 11% | 10% | 24% |
| Shared Decision-Making (SDM) | |||
| Patient prompt: What keeps you from being more involved in treatment decision-making? | |||
| I trust my care team to make the best decisions for me | -- | 64% | 30% |
| I am too overwhelmed/worried to make a decision | -- | 28% | 8% |
| I do not speak the same first language as my treating physician/treatment team members | -- | 18% | 10% |
| I don’t know a lot about medicine or health, so I don’t really understand what my care team is telling me or I don’t know what to ask | -- | 14% | 12% |
| My care team never asked what is important to me or what my goals of treatment are | -- | 14% | 8% |
| I do not feel that my team values my opinions/listens to my concerns for my care | -- | 2% | 6% |
| I feel that I am completely involved in my treatment decision making | -- | 14% | 54% |
| Areas of Improvement | |||
| Patient prompt: Which one aspect of your care do you think your MM care team could most improve? | |||
| Education about MM and treatment options | -- | 34% | 16% |
| Better provision of a translator/educational materials provided in my first language | -- | 26% | 4% |
| Discussion about realistic treatment expectations and prognosis | -- | 28% | 24% |
| Empathy throughout the emotional journey of managing my MM | -- | 32% | 13% |
| Counseling to help me cope with my diagnosis and treatment | -- | 28% | 16% |
| Insurance/financial counseling | -- | 14% | 18% |
| Audit Feedback Sessions | ||||
|---|---|---|---|---|
| Pre-Activity | Post-Activity | |||
| Academic Providers (n = 59) | Community Providers (n = 58) | Academic Providers (n = 41) | Community Providers (n = 49) | |
| Pre-Activity: What is the biggest challenge to equitable MM care in your system? Post-Activity: Following this program, which challenge to equitable MM care do you intend to address with your team? | ||||
| Engaging patients in SDM | 22% | 17% | 29% | 38% |
| Individualizing treatment decision-making based on patient- and disease-related factors | 16% | 25% | 37% | 18% |
| Providing adequate patient education about treatment options and potential side effects | 16% | 17% | 6% | 28% |
| Integrating distress screening into patient monitoring | 5% | 12% | 4% | 13% |
| Ensuring equitable access to novel therapies for all patients | 36% | 29% | 24% | 3% |
| Other | 5% | 0% | 0% | 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mikhael, J.R.; Sullivan, S.L.; Carter, J.D.; Heggen, C.L.; Gurska, L.M. Multisite Quality Improvement Initiative to Identify and Address Racial Disparities and Deficiencies in Delivering Equitable, Patient-Centered Care for Multiple Myeloma—Exploring the Differences between Academic and Community Oncology Centers. Curr. Oncol. 2023, 30, 1598-1613. https://doi.org/10.3390/curroncol30020123
Mikhael JR, Sullivan SL, Carter JD, Heggen CL, Gurska LM. Multisite Quality Improvement Initiative to Identify and Address Racial Disparities and Deficiencies in Delivering Equitable, Patient-Centered Care for Multiple Myeloma—Exploring the Differences between Academic and Community Oncology Centers. Current Oncology. 2023; 30(2):1598-1613. https://doi.org/10.3390/curroncol30020123
Chicago/Turabian StyleMikhael, Joseph R., Shelby L. Sullivan, Jeffrey D. Carter, Cherilyn L. Heggen, and Lindsay M. Gurska. 2023. "Multisite Quality Improvement Initiative to Identify and Address Racial Disparities and Deficiencies in Delivering Equitable, Patient-Centered Care for Multiple Myeloma—Exploring the Differences between Academic and Community Oncology Centers" Current Oncology 30, no. 2: 1598-1613. https://doi.org/10.3390/curroncol30020123