Loneliness in Breast Cancer Patients with Early Life Adversity: An Investigation of the Effects of Childhood Trauma and Self-Regulation


Abstract
:1. Introduction
1.1. Social Connectedness as a Conceptual Framework
1.2. Loneliness
1.3. Childhood Trauma
1.4. Self-Views
1.5. Emotional Expression
1.6. Research Aims
2. Method
Participants and Procedure
3. Measures
3.1. Interview for Traumatic Events in Childhood (ITEC)
3.2. Child Abuse and Self-Report Scale (CASRS)
3.3. Self-Discrepancies Scale (S-DS)
3.4. Ambivalence over Emotional Expression Questionnaire (AEQ)
3.5. UCLA Loneliness Scale-Version 3 (UCLA LS3)
3.6. Statistical Analysis
4. Results
4.1. Descriptive Statistics
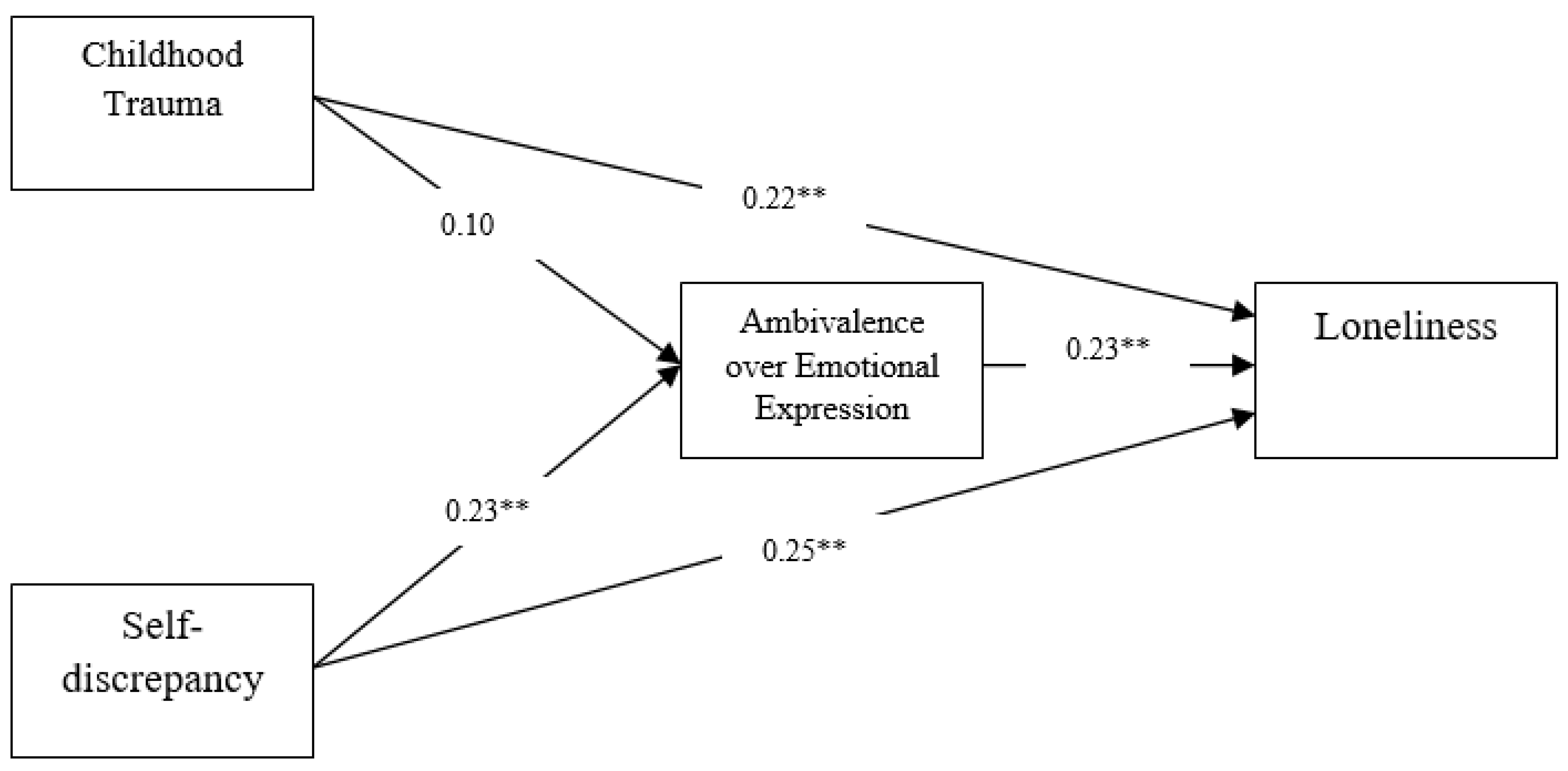
4.2. Evaluation of the Structural Model
4.3. Tests of Mediation Effects
5. Discussion
6. Clinical Implications
7. Limitations and Future Directions
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arnold, M.; Morgan, E.; Rumgay, H.; Mafra, A.; Singh, D.; Laversanne, M.; Vignat, J.; Gralow, J.R.; Cardoso, F.; Siesling, S.; et al. Current and Future Burden of Breast Cancer: Global Statistics for 2020 and 2040. Breast 2022, 66, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Haslam, D.; Mathews, B.; Pacella, R.; Scott, J.G.; Finkelhor, D.; Higgins, D.J.; Meinck, F.; Erskine, H.E.; Thomas, H.J.; Lawrence, D.; et al. The Prevalence and Impact of Child Maltreatment in Australia: Findings from the Australian Child Maltreatment Study: Brief Report; Australian Child Maltreatment Study, Queensland University of Technology: Brisbane, Australia, 2023; Available online: https://www.acms.au/resources/the-prevalence-and-impact-of-child-maltreatment-in-australia-findings-from-the-australian-child-maltreatment-study-2023-brief-report/ (accessed on 3 May 2023).
- Goldsmith, R.E.; Jandorf, L.; Valdimarsdottir, H.; Amend, K.L.; Stoudt, B.G.; Rini, C.; Hershman, D.; Neugut, A.; Reilly, J.J.; Tartter, P.I.; et al. Traumatic Stress Symptoms and Breast Cancer: The Role of Childhood Abuse. Child Abuse Negl. 2010, 34, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Kuhlman, K.R.; Boyle, C.C.; Irwin, M.R.; Ganz, P.A.; Crespi, C.M.; Asher, A.; Petersen, L.; Bower, J.E. Childhood Maltreatment, Psychological Resources, and Depressive Symptoms in Women with Breast Cancer. Child Abuse Negl. 2017, 72, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.; Nussey, A.E.; Helwig, C.C. The Importance of Social Connectedness for Self-Regulation and Emotional Wellbeing: Expanding the Definition of the Construct. In Post-Secondary Education Student Mental Health: A Global Perspective; Zangeneh, M., Nouroozifar, M., Chou, P., Eds.; Concurrent Disorders Society (CDS) Press: Toronto, ON, Canada, 2022; pp. 190–218. Available online: https://cdspress.ca/?page_id=6135 (accessed on 3 May 2023).
- Lo, C. A Developmental Perspective on Existential Distress and Adaptation to Advanced Disease. Psycho-Oncology 2018, 27, 2657–2660. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.B. Adult Mental Health Disorders and Their Age at Onset. Br. J. Psychiatry 2013, 202, s5–s10. [Google Scholar] [CrossRef] [PubMed]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness and Pathways to Disease. Brain Behav. Immun. 2003, 17, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Jewett, P.I.; Vogel, R.I.; Galchutt, P.; Everson-Rose, S.A.; Teoh, D.; Radomski, M.; Blaes, A.H. Associations between a Sense of Connection and Existential and Psychosocial Outcomes in Gynecologic and Breast Cancer Survivors. Support. Care Cancer 2022, 30, 3329–3336. [Google Scholar] [CrossRef]
- Jaremka, L.M.; Fagundes, C.P.; Glaser, R.; Bennett, J.M.; Malarkey, W.B.; Kiecolt-Glaser, J.K. Loneliness Predicts Pain, Depression, and Fatigue: Understanding the Role of Immune Dysregulation. Psychoneuroendocrinology 2013, 38, 1310–1317. [Google Scholar] [CrossRef]
- Olsson, U.; Bergbom, I.; Bosaeus, I. Patients’ Experiences of the Recovery Period 3 Months after Gastrointestinal Cancer Surgery. Eur. J. Cancer Care 2002, 11, 51–60. [Google Scholar] [CrossRef]
- Herzog, J.I.; Schmahl, C. Adverse Childhood Experiences and the Consequences on Neurobiological, Psychosocial, and Somatic Conditions across the Lifespan. Front. Psychiatry 2018, 9, 420. [Google Scholar] [CrossRef]
- Fagundes, C.P.; Lindgren, M.E.; Shapiro, C.L.; Kiecolt-Glaser, J.K. Child Maltreatment and Breast Cancer Survivors: Social Support Makes a Difference for Quality of Life, Fatigue and Cancer Stress. Eur. J. Cancer 2012, 48, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Guveli, H.; Guveli, M.E.; Sen, F.; Oflaz, S.; Gurdal, N.; Tambas, M.; Kucucuk, S.; Aydıner, A.; Ozkan, M. Effect of the Childhood Trauma on the Adjustment to Cancer in the Patients with Breast Cancer. Breast Cancer 2017, 24, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Coker, A.L.; Follingstad, D.; Garcia, L.S.; Williams, C.M.; Crawford, T.N.; Bush, H.M. Association of Intimate Partner Violence and Childhood Sexual Abuse with Cancer-related Well-being in Women. J. Womens Health 2012, 21, 1180–1188. [Google Scholar] [CrossRef]
- Phillips, A.G.; Silvia, P.J. Individual Differences in Self-Discrepancies and Emotional Experience: Do Distinct Discrepancies Predict Distinct Emotions? Pers. Individ. Dif. 2010, 49, 148–151. [Google Scholar] [CrossRef]
- McGinty, H.L.; Small, B.J.; Laronga, C.; Jacobsen, P.B. Predictors and Patterns of Fear of Cancer Recurrence in Breast Cancer Survivors. Health Psychol. 2016, 35, 1. [Google Scholar] [CrossRef] [PubMed]
- Nieto, M.; Navarro-Bravo, B.; Moreno, B.; Ocana, A.; Serrano, J.P.; Gras, C.B.; Ricarte, J.; Fernández-Aguilar, L.; Ros, L.; Latorre, J.M. Functioning of Autobiographical Memory Specificity and Self-Defining Memories in People with Cancer Diagnosis. PeerJ 2019, 7, e8126. [Google Scholar] [CrossRef]
- Triberti, S.; Savioni, L.; Sebri, V.; Pravettoni, G. EHealth for Improving Quality of Life in Breast Cancer Patients: A Systematic Review. Cancer Treat. Rev. 2019, 74, 1–14. [Google Scholar] [CrossRef]
- Veldhuis, J.; Alleva, J.M.; de Bij Vaate, A.J.D.; Keijer, M.; Konijn, E.A. Me, My Selfie, and I: The Relations between Selfie Behaviors, Body Image, Self-Objectification, and Self-Esteem in Young Women. Psychol. Pop. Media 2020, 9, 3. [Google Scholar] [CrossRef]
- Sansom-Daly, U.M.; Wakefield, C.E.; Robertson, E.G.; McGill, B.C.; Wilson, H.L.; Bryant, R.A. Adolescent and Young Adult Cancer Survivors’ Memory and Future Thinking Processes Place Them at Risk for Poor Mental Health. Psycho-Oncology 2018, 27, 2709–2716. [Google Scholar] [CrossRef]
- Kondylakis, H.; Bucur, A.; Dong, F.; Renzi, C.; Manfrinati, A.; Graf, N.; Hoffman, S.; Koumakis, L.; Pravettoni, G.; Marias, K.; et al. IManageCancer: Developing a Platform for Empowering Patients and Strengthening Self-Management in Cancer Diseases. In Proceedings of the 2017 IEEE 30th International Symposium on Computer-Based Medical Systems (CBMS); Thessaloniki, Greece, 22–24 June 2017, pp. 755–760. [CrossRef]
- Giffard, B.; Viard, A.; Dayan, J.; Morel, N.; Joly, F.; Eustache, F. Autobiographical Memory, Self, and Stress-Related Psychiatric Disorders: Which Implications in Cancer Patients? Neuropsychol. Rev. 2013, 23, 157–168. [Google Scholar] [CrossRef]
- Anderson, L.M.; Smith, K.M.; Schaefer, L.M.; Crosby, R.D.; Cao, L.; Engel, S.G.; Crow, S.J.; Wonderlich, S.A.; Peterson, C.B. Predictors and Moderators of Treatment Outcome in a Randomized Clinical Trial for Binge-Eating Disorder. J. Consult. Clin. Psychol. 2020, 88, 631. [Google Scholar] [CrossRef] [PubMed]
- King, L.A.; Emmons, R.A. Conflict over Emotional Expression: Psychological and Physical Correlates. J. Pers. Soc. Psychol. 1990, 58, 864. [Google Scholar] [CrossRef] [PubMed]
- Bashiri Nejadian, A.; Bayazi, M.H.; Johari Fard, R.; Rajaei, A.R. Correlations of Ambivalence over Emotional Expression and Social Support with Adherence to Treatment in Cancer Patients. Iran J. Nurs. 2021, 34, 33–46. [Google Scholar] [CrossRef]
- Servaes, P.; Vingerhoets, A.; Vreugdenhil, G.; Keuning, J.J.; Broekhuijsen, A.M. Inhibition of Emotional Expression in Breast Cancer Patients. Behav. Med. 1999, 25, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Heshmati, R.; Lo, C.; Khooy, M.P.; Naseri, E. Pathway Linking Emotional Suppression to Depression and Anxiety in Cancer Patients Undergoing Chemotherapy: The Mediating Role of Ego-Strength. Curr. Aging Sci. 2022. [Google Scholar] [CrossRef] [PubMed]
- Bashiri Nejadian, A.; Bayazi, M.H.; Johari Fard, R.; Rajaei, A.R. The Relationship between Ambivalence over Emotional Expression and Health-Related Quality of Life and Adherence to Treatment in Cancer Patients: The Mediating Role of Depression and Social Support: A Descriptive Study. J. Rafsanjan Univ. Med. Sci. 2021, 20, 163–186. [Google Scholar] [CrossRef]
- Lobbestael, J.; Arntz, A.; Harkema-Schouten, P.; Bernstein, D. Development and Psychometric Evaluation of a New Assessment Method for Childhood Maltreatment Experiences: The Interview for Traumatic Events in Childhood (ITEC). Child Abuse Negl. 2009, 33, 505–517. [Google Scholar] [CrossRef]
- Mohammadkhani, P.; Mohammadi, M.R.; Nazari, M.A.; Salavati, M.; Razzaghi, O.M. Development, Validation and Reliability of Child Abuse Self Report Scale (CASRS) in Iranian students. Med. J. Islam. Repub. Iran 2003, 17, 51–58. Available online: https://www.researchgate.net/publication/237836294_Development_validation_and_reliability_of_child_abuse_self_report_scale_CASRS_in_Iranian_students/citations (accessed on 3 May 2023).
- Philippot, P.; Dethier, V.; Baeyens, C.; Bouvard, M. Validation of the Self-Discrepancies Scale (S-DS). A Tool to Investigate the Self in Clinical and Research Settings. Eur. Rev. Appl. Psychol. 2018, 68, 69–77. [Google Scholar] [CrossRef]
- Alavi, K.; Asgharimoghadam, M.A.L.I.; Rahiminezhad, A.; Farahani, H. Psychometric Properties of Ambivalence over Emotional Expression Questionnaire. J. Res. Psychol. Health 2017, 11, 74–91. [Google Scholar] [CrossRef]
- Russell, D.; Peplau, L.A.; Cutrona, C.E. The Revised UCLA Loneliness Scale: Concurrent and Discriminant Validity Evidence. J. Pers. Soc. Psychol. 1980, 39, 472. [Google Scholar] [CrossRef] [PubMed]
- Deckx, L.; van den Akker, M.; Buntinx, F. Risk Factors for Loneliness in Patients with Cancer: A Systematic Literature Review and Meta-analysis. Eur. J. Oncol. Nurs. 2014, 18, 466–477. Available online: https://www.chicom.be/sites/default/files/risk_factors_for_loneliness_in_patients_with_cancer_lit_review_and_meta_analysis_eur_j_of_onc_nursing_2014_18_466.pdf (accessed on 3 May 2023). [CrossRef] [PubMed]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. Asymptotic and Resampling Strategies for Assessing and Comparing Indirect Effects in Multiple Mediator Models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Fritz, M.S.; Mackinnon, D.P. Required Sample Size to Detect the Mediated Effect. Psychol. Sci. 2007, 18, 233–239. [Google Scholar] [CrossRef]
- Mosaffa, N. Impact of Iran-Iraq War on Iranian Children. Iran. Rev. UN Stud. 2018, 1, 1–26. [Google Scholar] [CrossRef]
- Merz, E.-M.; Jak, S. The Long Reach of Childhood. Childhood Experiences Influence Close Relationships and Loneliness across Life. Adv. Life Course Res. 2013, 18, 212–222. [Google Scholar] [CrossRef]
- Slusarek, E.; Martin, V.; Sarker, T.; McCarthy, M.A.; Granton, J.; Tan, A.; Lo, C. The Mapping of Emotions in a Respiratory Illness: Transferability of Illness Experience from Pulmonary Arterial Hypertension to COVID-19. J. Concurr. Disord. 2021, 3, 66–81. [Google Scholar] [CrossRef]
- Marshall, D.; Green, S.; Jones, B.M.; Starrs, C.; Montgomery, G.H.; Minassian, K.; Wunder, B.; Force, J.; Schnur, J.B. Trauma-Informed Radiation Therapy: Implementation and Evaluation of a Sensitive Practice Tool for Female Patients Undergoing Radiotherapy for Breast Cancer. J. Am. Coll. Radiol. 2022, 19, 1236–1243. [Google Scholar] [CrossRef]
- Regal, R.A.; Wheeler, N.J.; Daire, A.P.; Spears, N. Childhood Sexual Abuse Survivors Undergoing Cancer Treatment: A Case for Trauma-Informed Integrated Care. J. Ment. Health Couns. 2020, 42, 15–31. [Google Scholar] [CrossRef]
- Bohus, M.; Kleindienst, N.; Hahn, C.; Müller-Engelmann, M.; Ludäscher, P.; Steil, R.; Fydrich, T.; Kuehner, C.; Resick, P.A.; Stiglmayr, C.; et al. Dialectical Behavior Therapy for Posttraumatic Stress Disorder (DBT-PTSD) Compared With Cognitive Processing Therapy (CPT) in Complex Presentations of PTSD in Women Survivors of Childhood Abuse: A Randomized Clinical Trial. JAMA Psychiatry 2020, 77, 1235–1245. [Google Scholar] [CrossRef] [PubMed]
- Connolly-Zubot, A.; Timulak, L.; Hession, N.; Coleman, N. Emotion-Focused Therapy for Anxiety and Depression in Women with Breast Cancer. J. Contemp. Psychother. 2020, 50, 113–122. [Google Scholar] [CrossRef]
- Bensimon, M. Integration of Trauma in Music Therapy: A Qualitative Study. Psychol. Trauma Theory Res. Pract. Policy 2022, 14, 367. [Google Scholar] [CrossRef] [PubMed]
- Marziliano, A.; Tuman, M.; Moyer, A. The Relationship between Post-traumatic Stress and Post-traumatic Growth in Cancer Patients and Survivors: A Systematic Review and Meta-analysis. Psychooncology 2020, 29, 604–616. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | N | % |
|---|---|---|
| Marital status | ||
| Married | 111 | 83.5 |
| Single | 7 | 5.3 |
| Widowed/Divorced | 15 | 11.3 |
| Education | ||
| Elementary | 35 | 26.3 |
| Diploma | 62 | 46.6 |
| Undergraduate or Graduate | 36 | 27.1 |
| Socioeconomic status | ||
| High | 8 | 6.0 |
| Middle | 122 | 91.7 |
| Low | 3 | 2.3 |
| Employment status | ||
| Employed | 17 | 12.8 |
| Unemployed | 95 | 71.4 |
| Retired | 21 | 15.8 |
| M | SD | |
| Age | 51.02 | 9.29 |
| Type | Attributes | % | |
|---|---|---|---|
| Ideal self | Positive | Spiritual | 11.1 |
| Cheerful, optimist, happy | 7.8 | ||
| Humble, modest | 7.3 | ||
| Grateful | 6.7 | ||
| Sympathetic, compassionate | 6.3 | ||
| Kind, friendliness, cordial, warm | 5.7 | ||
| Agreeable, conformist | 5.7 | ||
| Careful, cautious | 5.2 | ||
| Calm, gentle | 5.2 | ||
| Honest | 3.3 | ||
| Wise, calculating | 3.2 | ||
| Enthusiastic | 2.3 | ||
| Reasonable, logic | 2.3 | ||
| Clever, intellectual | 2.2 | ||
| Adventurous | 2.1 | ||
| Hardworking, achievement-focused, moral, serious | 1.9 | ||
| Helpful | 1.5 | ||
| Active, assertive | 1.3 | ||
| Liberal | 1.1 | ||
| Other | 17.8 | ||
| Frail, weak, tired | 13.1 | ||
| Negative | Solitary, shy, alone | 9.9 | |
| Anxious, worried, neurotic | 9.7 | ||
| Depressed, painful, pessimist | 9.1 | ||
| Disagreeable, disinterested | 8.7 | ||
| Childish, selfish | 5.1 | ||
| Aggressive | 4.4 | ||
| Sentimental, emotional, sensitive | 3.6 | ||
| Arrogant, proud, stubborn | 2.6 | ||
| Hard | 2.3 | ||
| Envious | 2.3 | ||
| Lazy | 2.2 | ||
| Obedient, submissive | 2.1 | ||
| Disorderly, impulsive | 1.3 | ||
| Other | 23.6 | ||
| Tolerant, patient | 14.1 | ||
| Ought self | Positive | Calm, gentle | 10.1 |
| Cheerful, optimist, happy | 9.3 | ||
| Spiritual | 8.1 | ||
| Wise, calculating | 7.3 | ||
| Dutiful | 7.1 | ||
| Humble, modest | 5.5 | ||
| Honest | 3.2 | ||
| Careful, cautious | 2.4 | ||
| Sympathetic, compassionate | 2.1 | ||
| Polite | 2.1 | ||
| Kind, friendliness, cordial, warm | 2.1 | ||
| Agreeable, conformist | 2.1 | ||
| Dependable, reliable | 1.7 | ||
| Altruist | 1.3 | ||
| Other | 21.5 | ||
| Frail, weak, tired | 13.1 | ||
| Depressed, painful, pessimist | 12.1 | ||
| Negative | Anxious, worried, neurotic | 11.5 | |
| Solitary, shy, alone | 10.2 | ||
| Obedient, submissive | 8.6 | ||
| Sentimental, emotional, sensitive | 7.2 | ||
| Lazy | 4.8 | ||
| Insensitive | 3.9 | ||
| Obstinate | 3.1 | ||
| Unpredictable | 2.5 | ||
| Stingy, spiteful | 2.3 | ||
| Credulous | 1.8 | ||
| Other | 18.9 |
| Predictors | Mediator | Outcome | ||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| 1. CASRS | 1 | |||
| 2. S-DS | 0.07 | 1 | ||
| 3. AEE | 0.15 * | 0.24 ** | 1 | |
| 4. UCLA LS3 | 0.26 ** | 0.30 ** | 0.21 * | 1 |
| Mean | 22.301 | 12.23 | 71.04 | 33.95 |
| SD | 13.87 | 5.79 | 13.53 | 9.46 |
| Min | 4 | 4 | 40 | 20 |
| Max | 89 | 28 | 113 | 70 |
| Cronbach’s Alpha | 0.83 | 0.84 | 0.72 | 0.70 |
| Path | Childhood Trauma to | Self-Discrepancy to | Ambivalence to | Total Effect: Trauma to Loneliness | Total Indirect: Trauma to Loneliness | Mediation Effect: Trauma →Ambivalence → Loneliness | Total Effect: Self-Discrepancy to Loneliness | Total Indirect: Self-Discrepancy to Loneliness | Mediation Effect: Self-Discrepancy → Ambivalence → Loneliness | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ambivalence | Loneliness | Ambivalence | Loneliness | Loneliness | |||||||
| B (SE) | 0.10 (0.08) | 0.15 (0.05) | 0.53 (0.18) | 0.41 (0.13) | 0.15 (0.05) | 0.16 (0.10) | 0.02 (0.01) | 0.01 (0.01) | 0.44 (0.15) | 0.10 (0.05) | 0.11 (0.04) |
| β | 0.10 | 0.22 ** | 0.23 ** | 0.25 ** | 0.23 ** | 0.24 ** | 0.02 | 0.015 | 0.28 ** | 0.06 * | 0.07 * |
| 95% CI | [−0.06 to 0.24] | [0.007 to 0.41] | [0.05 to 0.38] | [0.09 to 0.38] | [0.04 to 0.31] | [0.03 to 0.43] | [−0.006 to 0.08] | [−0.003 to 0.00] | [0.09 to 0.41] | [0.004 to 0.14] | [0.003 to 0.16] |
| Fit index | |||||||||||
| CFI | NFI | RMSEA | |||||||||
| Full mediation | 0.71 | 0.73 | 0.13 | ||||||||
| Partial mediation | 0.96 | 0.95 | 0.08 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heshmati, R.; Azmoodeh, S.; Kheiriabad, M.; Ghasemi, A.; Lo, C. Loneliness in Breast Cancer Patients with Early Life Adversity: An Investigation of the Effects of Childhood Trauma and Self-Regulation. Curr. Oncol. 2023, 30, 5145-5157. https://doi.org/10.3390/curroncol30050389
Heshmati R, Azmoodeh S, Kheiriabad M, Ghasemi A, Lo C. Loneliness in Breast Cancer Patients with Early Life Adversity: An Investigation of the Effects of Childhood Trauma and Self-Regulation. Current Oncology. 2023; 30(5):5145-5157. https://doi.org/10.3390/curroncol30050389
Chicago/Turabian StyleHeshmati, Rasoul, Shahin Azmoodeh, Mina Kheiriabad, Anis Ghasemi, and Chris Lo. 2023. "Loneliness in Breast Cancer Patients with Early Life Adversity: An Investigation of the Effects of Childhood Trauma and Self-Regulation" Current Oncology 30, no. 5: 5145-5157. https://doi.org/10.3390/curroncol30050389