Young Myeloma Patients: A Systematic Review of Manifestations and Outcomes

 ,
,  , and
, and
Abstract
:1. Introduction
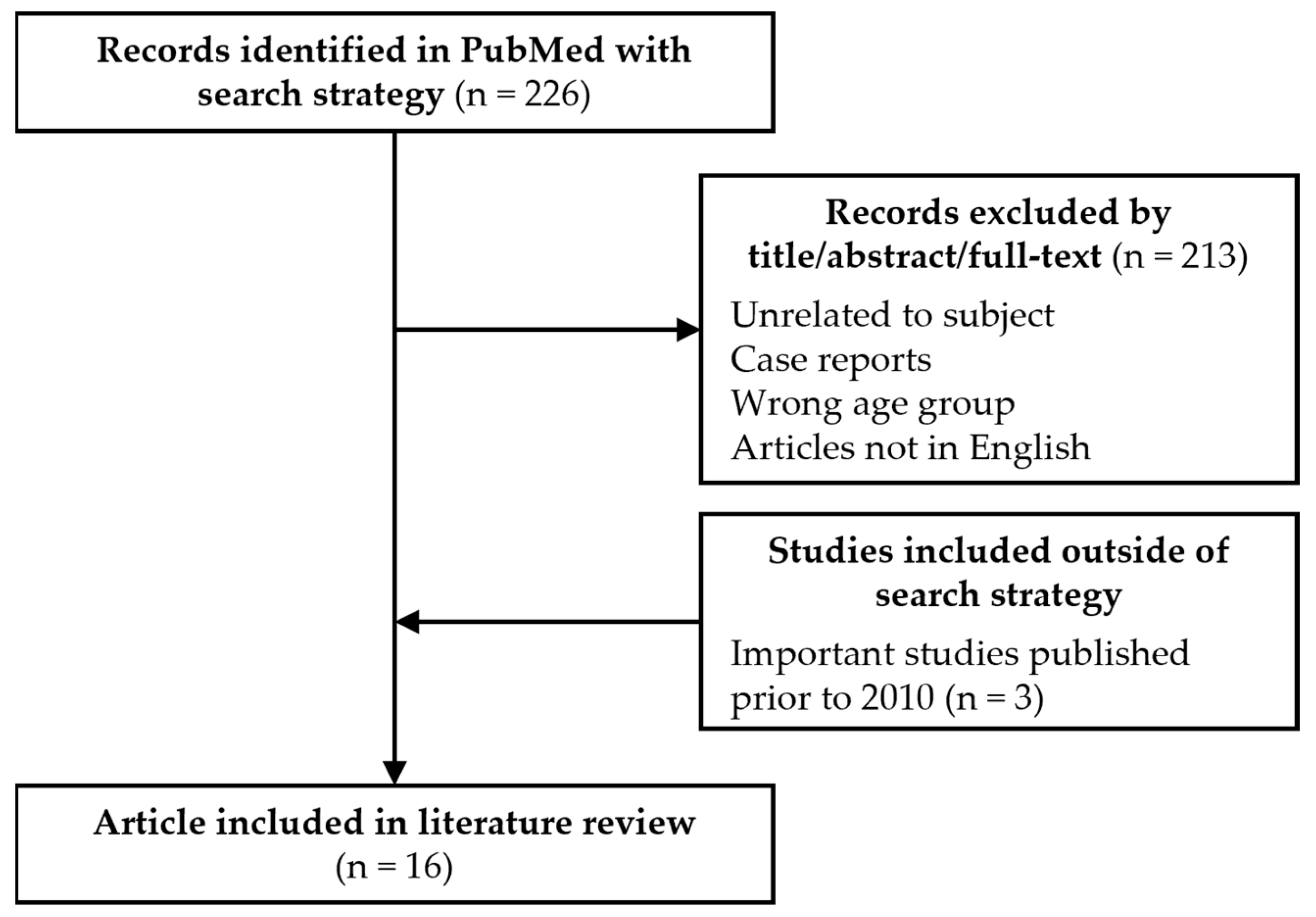
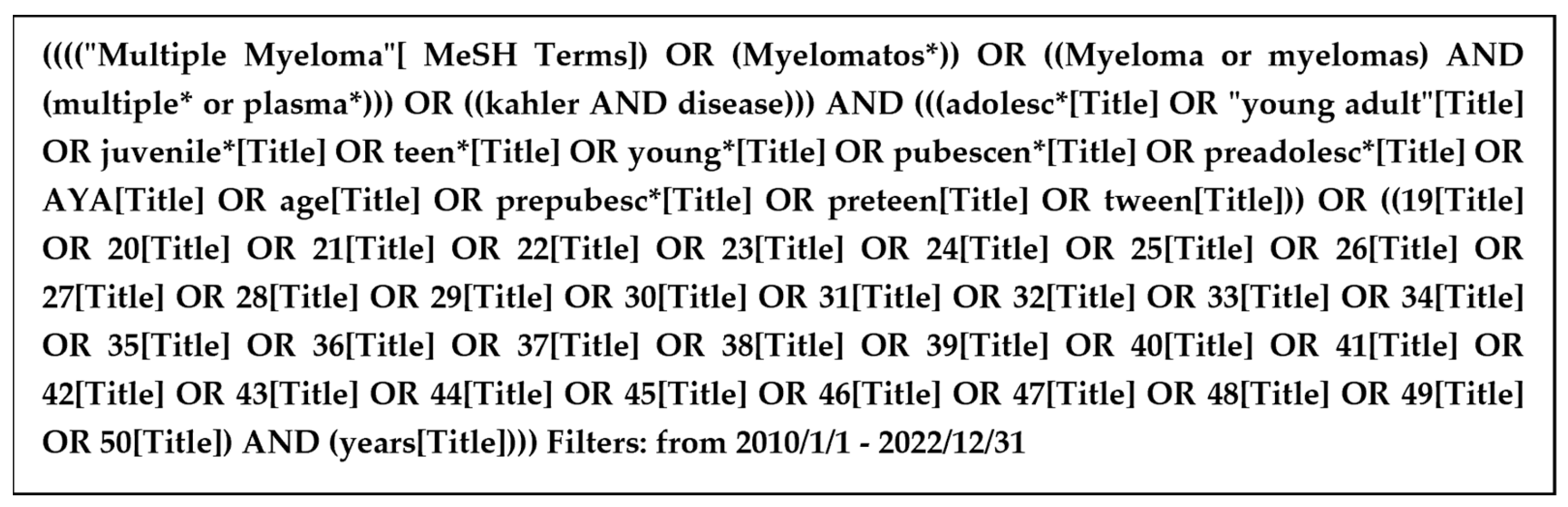
2. Methods
3. Results
3.1. Disease Characteristics at Diagnosis
3.2. Cytogenetics
3.3. Treatments and Outcomes
4. Discussion
5. Conclusions and Future Directions
Author Contributions
Funding
Conflicts of Interest
References
- Blimark, C.H.; Turesson, I.; Genell, A.; Ahlberg, L.; Björkstrand, B.; Carlson, K.; Forsberg, K.; Juliusson, G.; Linder, O.; Mellqvist, U.-H.; et al. Outcome and survival of myeloma patients diagnosed 2008–2015. Real-world data on 4904 patients from the Swedish Myeloma Registry. Haematologica 2018, 103, 506–513. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. SEER Cancer Statistics Factsheets: Multiple Myeloma. Available online: https://seer.cancer.gov/statfacts/html/mulmy.html (accessed on 3 January 2023).
- Kyle, R.A.; Gertz, M.A.; Witzig, T.E.; Lust, J.A.; Lacy, M.Q.; Dispenzieri, A.; Fonseca, R.; Rajkumar, S.V.; Offord, J.R.; Larson, D.R.; et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin. Proc. 2003, 78, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, H.; Bolejack, V.; Crowley, J.; Bladé, J.; Miguel, J.S.; Kyle, R.A.; Rajkumar, S.V.; Shimizu, K.; Turesson, I.; Westin, J.; et al. Survival and Years of Life Lost in Different Age Cohorts of Patients with Multiple Myeloma. J. Clin. Oncol. 2010, 28, 1599–1605. [Google Scholar] [CrossRef] [PubMed]
- Van der Poel, M.W.M.; Oerlemans, S.; Schouten, H.C.; van de Poll-Franse, L.V. Elderly multiple myeloma patients experience less deterioration in health-related quality of life than younger patients compared to a normative population: A study from the population-based PROFILES registry. Ann. Hematol. 2015, 94, 651–661. [Google Scholar] [CrossRef]
- Lenhoff, S.; Hjorth, M.; Westin, J.; Brinch, L.; Bäckström, B.; Carlson, K.; Christiansen, I.; Dahl, I.M.; Gimsing, P.; Hammerström, J.; et al. Impact of age on survival after intensive therapy for multiple myeloma: A population-based study by the Nordic Myeloma Study Group. Br. J. Haematol. 2006, 133, 389–396. [Google Scholar] [CrossRef]
- Bladé, J.; Kyle, R.A.; Greipp, P.R. Presenting features and prognosis in 72 patients with multiple myeloma who were younger than 40 years. Br. J. Haematol. 1996, 93, 345–351. [Google Scholar] [CrossRef]
- Corso, A.; Klersy, C.; Lazzarino, M.; Bernasconi, C. Multiple myeloma in younger patients: The role of age as prognostic factor. Ann. Hematol. 1998, 76, 67–72. [Google Scholar] [CrossRef]
- Ludwig, H.; Durie, B.G.; Bolejack, V.; Turesson, I.; Kyle, R.A.; Blade, J.; Fonseca, R.; Dimopoulos, M.; Shimizu, K.; San Miguel, J.; et al. Myeloma in patients younger than age 50 years presents with more favorable features and shows better survival: An analysis of 10 549 patients from the International Myeloma Working Group. Blood 2008, 111, 4039–4047. [Google Scholar] [CrossRef]
- Shin, J.; Koh, Y.; Youk, J.; Kim, M.; Kim, B.S.; Choi, C.W.; Sung, H.J.; Park, Y.; Yoon, S.S.; Kim, I. Clinicopathological characteristics of extremely young Korean multiple myeloma patients: Therapeutic implications. Korean J. Intern. Med. 2017, 32, 722–730. [Google Scholar] [CrossRef]
- Ravi, P.; Kumar, S.K.; Cerhan, J.R.; Maurer, M.J.; Dingli, D.; Ansell, S.M.; Rajkumar, S.V. Defining cure in multiple myeloma: A comparative study of outcomes of young individuals with myeloma and curable hematologic malignancies. Blood Cancer J. 2018, 8, 26. [Google Scholar] [CrossRef]
- Yanamandra, U.; Saini, N.; Chauhan, P.; Sharma, T.; Khadwal, A.; Prakash, G.; Varma, N.; Lad, D.; Varma, S.; Malhotra, P. AYA-Myeloma: Real-World, Single-Center Experience Over Last 5 Years. J. Adolesc. Young Adult Oncol. 2018, 7, 120–124. [Google Scholar] [CrossRef]
- Jurczyszyn, A.; Davila, J.; Kortüm, K.M.; Jayabalan, D.S.; Vij, R.; Fiala, M.; Milunovic, V.; Chim, C.S.; Wiśniewska-Piąty, K.; Waszczuk-Gajda, A.; et al. Multiple myeloma in patients up to 30 years of age: A multicenter retrospective study of 52 cases. Leuk. Lymphoma 2019, 60, 471–476. [Google Scholar] [CrossRef]
- Pál, I.; Illés, Á.; Váróczy, L. Multiple Myeloma of the Young—A Single Center Experience Highlights Future Directions. Pathol. Oncol. Res. 2020, 26, 419–424. [Google Scholar] [CrossRef]
- Duek, A.; Trakhtenbrot, L.; Avigdor, A.; Nagler, A.; Leiba, M. Multiple Myeloma Presenting in Patients Younger than 50 Years of Age: A Single Institution Experience. Acta Haematol. 2021, 144, 58–65. [Google Scholar] [CrossRef]
- Caulier, A.; Roussel, M.; Morel, P.; Lombion, N.; Branco, B.; Galtier, J.; Hulin, C.; Perrot, A.; Richez, V.; Michaud-Robert, A.V.; et al. Epidemiological landscape of young multiple myeloma patients diagnosed earlier than 40 years: The french experience. Blood 2021, 138, 2686–2695. [Google Scholar] [CrossRef]
- Bao, A.; Zhao, Q.; Merritt, E.; Bumma, N.; Devarakonda, S.; Khan, A.M.; Umyarova, E.; Rosko, A.E.; Benson, D.M.; Cottini, F. Racial differences as predictors of outcomes in young patients with multiple myeloma. Blood Cancer J. 2022, 12, 114. [Google Scholar] [CrossRef]
- Lu, J.; Lu, J.; Chen, W.; Wang, J.; Huo, Y.; Hou, J.; Huang, X. More frequent IgD and reduced CD200 expression in Chinese patients younger than 50 years old with multiple myeloma: A multicenter analysis. Drug Des. Dev. 2016, 10, 3673–3679. [Google Scholar] [CrossRef]
- Jurczyszyn, A.; Nahi, H.; Avivi, I.; Gozzetti, A.; Niesvizky, R.; Yadlapati, S.; Jayabalan, D.S.; Robak, P.; Pika, T.; Andersen, K.T.; et al. Characteristics and outcomes of patients with multiple myeloma aged 21–40 years versus 41–60 years: A multi-institutional case-control study. Br. J. Haematol. 2016, 175, 884–891. [Google Scholar] [CrossRef]
- Dhakal, B.; Nelson, A.; Murthy, G.S.G.; Fraser, R.; Eastwood, D.; Hamadani, M.; Pasquini, M.; D’Souza, A.; Hari, P. Autologous Hematopoietic Cell Transplantation in Patients with Multiple Myeloma: Effect of Age. Clin. Lymphoma Myeloma Leuk. 2017, 17, 165–172. [Google Scholar] [CrossRef]
- Nakaya, A.; Kohara, T.; Shibayama, H.; Onda, Y.; Kanda, J.; Kaneko, H.; Imada, K.; Kida, T.; Kosugi, S.; Ishikawa, J.; et al. Retrospective multi-center study of Adolescent and Young Adult (AYA) Multiple Myeloma in Kansai Myeloma Forum registry. Int. J. Hematol. 2020, 112, 435–438. [Google Scholar] [CrossRef]
- Pydi, V.R.; Bala, S.C.; Kuruva, S.P.; Chennamaneni, R.; Konatam, M.L.; Gundeti, S. Multiple Myeloma in Young Adults: A Single Centre Real World Experience. Indian J. Hematol. Blood Transfus. Off. J. Indian Soc. Hematol. Blood Transfus. 2021, 37, 679–683. [Google Scholar] [CrossRef]
- Rafae, A.; Malik, M.N.; Abu Zar, M.; Durer, S.; Durer, C. An Overview of Light Chain Multiple Myeloma: Clinical Characteristics and Rarities, Management Strategies, and Disease Monitoring. Cureus 2018, 10, e3148. [Google Scholar] [CrossRef] [PubMed]
- Kastritis, E.; Terpos, E.; Roussou, M.; Gavriatopoulou, M.; Migkou, M.; Eleutherakis-Papaiakovou, E.; Fotiou, D.; Ziogas, D.; Panagiotidis, I.; Kafantari, E.; et al. Evaluation of the Revised International Staging System in an independent cohort of unselected patients with multiple myeloma. Haematologica 2017, 102, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Altieri, A.; Chen, B.; Bermejo, J.L.; Castro, F.; Hemminki, K. Familial risks and temporal incidence trends of multiple myeloma. Eur. J. Cancer 2006, 42, 1661–1670. [Google Scholar] [CrossRef] [PubMed]
- Vachon, C.M.; Kyle, R.A.; Therneau, T.M.; Foreman, B.J.; Larson, D.R.; Colby, C.L.; Phelps, T.K.; Dispenzieri, A.; Kumar, S.K.; Katzmann, J.A.; et al. Increased risk of monoclonal gammopathy in first-degree relatives of patients with multiple myeloma or monoclonal gammopathy of undetermined significance. Blood 2009, 114, 785–790. [Google Scholar] [CrossRef]
- Clay-Gilmour, A.I.; Kumar, S.; Rajkumar, S.V.; Rishi, A.; Kyle, R.A.; Katzmann, J.A.; Murray, D.L.; Norman, A.D.; Greenberg, A.J.; Larson, D.R.; et al. Risk of MGUS in relatives of multiple myeloma cases by clinical and tumor characteristics. Leukemia 2019, 33, 499–507. [Google Scholar] [CrossRef]
- Walker, B.A.; Wardell, C.P.; Murison, A.; Boyle, E.M.; Begum, D.B.; Dahir, N.M.; Proszek, P.Z.; Melchor, L.; Pawlyn, C.; Kaiser, M.F.; et al. APOBEC family mutational signatures are associated with poor prognosis translocations in multiple myeloma. Nat. Commun. 2015, 6, 6997. [Google Scholar] [CrossRef]
- Palumbo, A.; Avet-Loiseau, H.; Oliva, S.; Lokhorst, H.M.; Goldschmidt, H.; Rosinol, L.; Richardson, P.; Caltagirone, S.; Lahuerta, J.J.; Facon, T.; et al. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. J. Clin. Oncol. 2015, 33, 2863–2869. [Google Scholar] [CrossRef]
- Fonseca, R.; Blood, E.; Rue, M.; Harrington, D.; Oken, M.M.; Kyle, R.A.; Dewald, G.W.; Van Ness, B.; Van Wier, S.A.; Henderson, K.J.; et al. Clinical and biologic implications of recurrent genomic aberrations in myeloma. Blood 2003, 101, 4569–4575. [Google Scholar] [CrossRef]
- Fonseca, R.; Debes-Marun, C.S.; Picken, E.B.; Dewald, G.W.; Bryant, S.C.; Winkler, J.M.; Blood, E.; Oken, M.M.; Santana-Dávila, R.; González-Paz, N.; et al. The recurrent IgH translocations are highly associated with nonhyperdiploid variant multiple myeloma. Blood 2003, 102, 2562–2567. [Google Scholar] [CrossRef]
- Rajkumar, S.V. Multiple myeloma: 2020 update on diagnosis, risk-stratification and management. Am. J. Hematol. 2020, 95, 548–567. [Google Scholar] [CrossRef]
- Manier, S.; Salem, K.Z.; Park, J.; Landau, D.A.; Getz, G.; Ghobrial, I.M. Genomic complexity of multiple myeloma and its clinical implications. Nat. Rev. Clin. Oncol. 2017, 14, 100–113. [Google Scholar] [CrossRef]
- Singh, C.; Panakkal, V.; Sreedharanunni, S.; Jandial, A.; Jain, A.; Lad, D.; Prakash, G.; Khadwal, A.; Malhotra, P. Presentation and Impact of Double and Triple hit Cytogenetics in Patients With Multiple Myeloma in the Real World. Clin. Lymphoma Myeloma Leuk. 2022, 22, e685–e690. [Google Scholar] [CrossRef] [PubMed]
- Marcon, C.; Simeon, V.; Deias, P.; Facchin, G.; Corso, A.; Derudas, D.; Montefusco, V.; Offidani, M.; Petrucci, M.T.; Zambello, R.; et al. Experts’ consensus on the definition and management of high risk multiple myeloma. Front. Oncol. 2022, 12, 1096852. [Google Scholar] [CrossRef]
- Walker, B.A.; Mavrommatis, K.; Wardell, C.P.; Ashby, T.C.; Bauer, M.; Davies, F.; Rosenthal, A.; Wang, H.; Qu, P.; Hoering, A.; et al. A high-risk, Double-Hit, group of newly diagnosed myeloma identified by genomic analysis. Leukemia 2019, 33, 159–170. [Google Scholar] [CrossRef]
- Langseth, Ø.O.; Myklebust, T.; Johannesen, T.B.; Hjertner, Ø.; Waage, A. Incidence and survival of multiple myeloma: A population-based study of 10 524 patients diagnosed 1982–2017. Br. J. Haematol. 2020, 191, 418–425. [Google Scholar] [CrossRef]
- Attal, M.; Lauwers-Cances, V.; Hulin, C.; Leleu, X.; Caillot, D.; Escoffre, M.; Arnulf, B.; Macro, M.; Belhadj, K.; Garderet, L.; et al. Lenalidomide, Bortezomib, and Dexamethasone with Transplantation for Myeloma. N. Engl. J. Med. 2017, 376, 1311–1320. [Google Scholar] [CrossRef]
- Rosiñol, L.; Oriol, A.; Rios, R.; Sureda, A.; Blanchard, M.J.; Hernández, M.T.; Martínez-Martínez, R.; Moraleda, J.M.; Jarque, I.; Bargay, J.; et al. Bortezomib, lenalidomide, and dexamethasone as induction therapy prior to autologous transplant in multiple myeloma. Blood 2019, 134, 1337–1345. [Google Scholar] [CrossRef]
- Roussel, M.; Lauwers-Cances, V.; Robillard, N.; Hulin, C.; Leleu, X.; Benboubker, L.; Marit, G.; Moreau, P.; Pegourie, B.; Caillot, D.; et al. Front-Line Transplantation Program With Lenalidomide, Bortezomib, and Dexamethasone Combination As Induction and Consolidation Followed by Lenalidomide Maintenance in Patients With Multiple Myeloma: A Phase II Study by the Intergroupe Francophone du Myélome. J. Clin. Oncol. 2014, 32, 2712–2717. [Google Scholar] [CrossRef]
- Richardson, P.G.; Weller, E.; Lonial, S.; Jakubowiak, A.J.; Jagannath, S.; Raje, N.S.; Avigan, D.E.; Xie, W.; Ghobrial, I.M.; Schlossman, R.L.; et al. Lenalidomide, bortezomib, and dexamethasone combination therapy in patients with newly diagnosed multiple myeloma. Blood 2010, 116, 679–686. [Google Scholar] [CrossRef]
- Moreau, P.; Attal, M.; Hulin, C.; Arnulf, B.; Belhadj, K.; Benboubker, L.; Béné, M.C.; Broijl, A.; Caillon, H.; Caillot, D.; et al. Bortezomib, thalidomide, and dexamethasone with or without daratumumab before and after autologous stem-cell transplantation for newly diagnosed multiple myeloma (CASSIOPEIA): A randomised, open-label, phase 3 study. Lancet 2019, 394, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Voorhees, P.M.; Kaufman, J.L.; Laubach, J.P.; Sborov, D.W.; Reeves, B.; Rodriguez, C.; Chari, A.; Silbermann, R.W.; Costa, L.J.; Anderson, L.D.; et al. Depth of Response to Daratumumab (DARA), Lenalidomide, Bortezomib, and Dexamethasone (RVd) Improves over Time in Patients (pts) with Transplant-Eligible Newly Diagnosed Multiple Myeloma (NDMM): Griffin Study Update. Blood 2019, 134, 691. [Google Scholar] [CrossRef]
- Landgren, O.; Hultcrantz, M.; Diamond, B.; Lesokhin, A.M.; Mailankody, S.; Hassoun, H.; Tan, C.; Shah, U.A.; Lu, S.X.; Salcedo, M.; et al. Safety and Effectiveness of Weekly Carfilzomib, Lenalidomide, Dexamethasone, and Daratumumab Combination Therapy for Patients With Newly Diagnosed Multiple Myeloma: The MANHATTAN Nonrandomized Clinical Trial. JAMA Oncol. 2021, 7, 862–868. [Google Scholar] [CrossRef]
- Rajkumar, S.V. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am. J. Hematol. 2022, 97, 1086–1107. [Google Scholar] [CrossRef] [PubMed]
- Durie, B.G.M.; Hoering, A.; Abidi, M.H.; Rajkumar, S.V.; Epstein, J.; Kahanic, S.P.; Thakuri, M.; Reu, F.; Reynolds, C.M.; Sexton, R.; et al. Bortezomib with lenalidomide and dexamethasone versus lenalidomide and dexamethasone alone in patients with newly diagnosed myeloma without intent for immediate autologous stem-cell transplant (SWOG S0777): A randomised, open-label, phase 3 trial. Lancet 2017, 389, 519–527. [Google Scholar] [CrossRef]
- Facon, T.; Kumar, S.; Plesner, T.; Orlowski, R.Z.; Moreau, P.; Bahlis, N.; Basu, S.; Nahi, H.; Hulin, C.; Quach, H.; et al. Daratumumab plus Lenalidomide and Dexamethasone for Untreated Myeloma. N. Engl. J. Med. 2019, 380, 2104–2115. [Google Scholar] [CrossRef]
- Claveau, J.-S.; Buadi, F.K.; Kumar, S. Current Role of Allogeneic Stem Cell Transplantation in Multiple Myeloma. Oncol. Ther. 2022, 10, 105–122. [Google Scholar] [CrossRef]
- LeBlanc, R.; Ahmad, I.; Terra, R.; Boudreault, J.-S.; Ogez, D.; Lamore, K.; Delisle, J.-S.; Bambace, N.; Bernard, L.; Cohen, S.; et al. Outcomes in newly diagnosed young or high-risk myeloma patients receiving tandem autologous/allogeneic transplant followed by bortezomib maintenance: A phase II study. Bone Marrow Transplant. 2022, 57, 252–260. [Google Scholar] [CrossRef]
- Munshi, N.C.; Avet-Loiseau, H.; Anderson, K.C.; Neri, P.; Paiva, B.; Samur, M.; Dimopoulos, M.; Kulakova, M.; Lam, A.; Hashim, M.; et al. A large meta-analysis establishes the role of MRD negativity in long-term survival outcomes in patients with multiple myeloma. Blood Adv. 2020, 4, 5988–5999. [Google Scholar] [CrossRef]
- Goicoechea, I.; Puig, N.; Cedena, M.-T.; Burgos, L.; Cordón, L.; Vidriales, M.-B.; Flores-Montero, J.; Gutierrez, N.C.; Calasanz, M.-J.; Ramos, M.-L.M.; et al. Deep MRD profiling defines outcome and unveils different modes of treatment resistance in standard- and high-risk myeloma. Blood 2021, 137, 49–60. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Bladé 1996 [7] | Shin 2017 [10] | Ravi 2018 [11] | Yanamandra 2018 [12] | Jurczyszyn 2019 [13] | Pál 2020 [14] | Duek 2021 [15] | Caulier 2021 [16] | Bao 2022 [17] | |
|---|---|---|---|---|---|---|---|---|---|
| n | 72 | 32 | 212 | 40 | 52 | 16 | 23 | 214 | 258 |
| Country | USA | South Korea | USA | India | Europe, USA, Brazil, Hong Kong | Hungary | Israel | France, Belgium | USA |
| Years of diagnosis | 1956–1992 | 2000–2015 | 2005–2015 | 2010–2015 | 1989–2016 | 2006–2015 | 2009–2014 | 2000–2015 | 1992–2019 |
| Patients’ age (years) | <40 | ≤40 | ≤50 | <40 | ≤30 | ≤40 | <50 | ≤40 | <50 |
| Median age (range) | 36 (19–39) | 37 (17–40) | 45 (22–49) | 38 (18–39) | 28 (8–30) | 39 (31–40) | 41.5 (27–49) | 37.2 (18.6–40.9) | 46 (17–50) |
| Male/female | 50/22 | 19/13 | 129/83 | 26/14 | 35/17 | 10/6 | 17/6 | 137/77 | 165/93 |
| ISS | |||||||||
| I | NA | 10/31 (32) | 74/212 (35) b | 5/40 (13) | 32/47 (68) | 7/16 (44) | 5/14 (36) | 99/189 (52) | 89/212 (42) |
| II | NA | 15/31 (48) | 46/212 (22) b | 7/40 (18) | 7/47 (15) | 5/16 (31) | 6/14 (43) | 52/189 (28) | 66/212 (31) |
| III | NA | 6/31 (19) | 48/212 (23) b | 28/40 (70) | 8/47 (17) | 4/16 (25) | 3/14 (21) | 38/189 (20) | 57/212 (27) |
| Disease features at diagnosis | |||||||||
| Anemia (<100 g/L) | NA | 9/31 (29) | NA | 21/40 (53) | 13/43 (30) | 2/16 (13) | 6/18 (33) | 71/202 (35) | NA |
| Kidney disease a | 15/52 (29) | 4/32 (13) | NA | 12/40 (30) | 4/22 (18) | 2/16 (13) | 3/18 (17) | 34/200 (17) | NA |
| Low albumin a | 8/49 (16) | 9/32 (28) | NA | NA | 11/41 (27) | NA | 8/18 (44) | NA | NA |
| Hypercalcemia a | 16/53 (30) | 9/32 (28) | NA | 9/37 (24) | 6/42 (14) | 3/16 (19) | 1/18 (6) | 25/195 (13) | NA |
| Lytic bone lesions | 44/65 (68) | 27/31 (87) | NA | 16/37 (59) | 36/44 (82) | 14/16 (88) | 16/18 (89) | 149/200 (75) | NA |
| Elevated ß2MG a | 18/33 (55) | 14/29 (48) | NA | NA | 11/41 (27) | NA | NA | NA | NA |
| Protein isotype | |||||||||
| Heavy chain | NA | ||||||||
| IgG | 34/66 (51) | 14/30 (47) | NA | (76) | 27/49 (55) | 8/16 (50) | 11/22 (50) | 130/162 (80) | 121/258 (47) |
| IgA | 7/66 (11) | 5/30 (17) | NA | (11) | 9/49 (18) | 3/16 (19) | 2/22 (9) | 28/162 (17) | 53/258 (21) |
| IgD | 4/66 (6) | 2/30 (7) | NA | NA | NA | 0/16 (0) | NA | 3/162 (2) | NA |
| IgM | NA | NA | NA | (3) | NA | 0/16 (0) | NA | 1/162 (0.6) | NA |
| Light chain only | 21/66 (32) | 9/30 (30) | NA | (11) | 11/49 (22) | 3/16 (19) | 10/22 (45) c | 51/213 (24) | 72/258 (28) |
| Corso 1998 [8] | Ludwig 2008 [9] | Lu 2016 [18] | Jurczyszyn 2016 [19] | Dhakal 2017 [20] | Nakaya 2020 [21] | Pydi 2021 [22] | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | 356 | 10,549 | 940 | 1089 | 191 | 2303 | 280 | |||||||
| Country | Italy | North America, Europe, Japan | China | Europe, USA | USA | Japan | India | |||||||
| Years of diagnosis | 1973–1994 | 1981–2002 | 2008–2011 | 2000–2015 | 2000 to 2015 | 1998–2018 | 2013–2018 | |||||||
| Age studied (years) | <50 | ≥50 | <50 | ≥50 | <50 | ≥50 | 21–40 | 41–60 | ≤50 | >70 | <40 | All | ≤40 | All patients |
| n (by age group) | 61 | 295 | 1689 | 8860 | 194 | 746 | 173 | 916 | 86 | 105 | 26 | 2277 | 22 | 258 |
| Median age (range) | 45 (33–49) | 63 (50–87) | 36 (20–49) | 62 (50–93) | 46 (20–49) | 62 (50–88) | 37 (21–40) | 55 (41–60) | 46 (32–50) | 73 (71–79) | 36 (20–39) | 74 (20–96) | 33.5 (18–40) | 56 (18–84) |
| Male/female | 32/29 | 169/126 | 1023/666 | 5014/3846 | 113/81 | 457/289 | 104/69 | 510/406 | 70/16 | 58/47 | 13/13 | 1116/1161 | 14:8 | NA |
| ISS | ||||||||||||||
| I | NA | NA | 492/1267 (39) | 1790/6776 (26) p < 0.001 | (30) | (17) p < 0.001 | 71/151 (47) | 303/729 (42) p = 0.40 | 15/86 (17) d | 29/105 (27) p = 0.31 d | (43) | (23) p = 0.019 | (18) | (17) |
| II | NA | NA | 438/1267 (35) | 2675/6776 (39) p < 0.001 | (31) | (32) p = 0.774 | 50/151 (33) | 280/729 (38) | 22/86 (26) d | 22/105 (21) d | (38) | (40) p = 0.910 | (32) | (33) |
| III | NA | NA | 337/1267 (27) | 2311/6776 (34) p < 0.001 | (39) | (51) p 0.007 | 30/151 (20) | 149/729 (20) | 20/86 (23) d | 28/105 (27) d | (19) | (37) p = 0.022 | (50) | (50) |
| Disease features at diagnosis | ||||||||||||||
| Anemia (<100 g/L) | NA | NA | 596/1614 (37) | 3465/8539 (41) p = 0.006 | (56) | (61) p = 0.265 | 53/173 (31) | 247/925 (27) p = 0.29 | NA | NA | 6/26 (23) | NA | (68) | (63) |
| Kidney disease a | 5/61 (8) | 41/295 (14) | 240/1594 (15) | 1484/8573 (17) p = 0.028 | (21) | (25) p = 0.300 | 40/160 (25) | 265/855 (31) p = 0.13 | NA | NA | 11/26 (42) | NA | (50) | (36) |
| Low albumin a | NA | NA | 458/1396 (33) | 3276/7912 (41) p < 0.001 | (37) | (58) p < 0.001 | NA | NA | NA | NA | NA | NA | NA | NA |
| Hypercalcemia a | 4/61 (6) | 17/295 (6) | 481/1445 (33) | 2652/7870 (34) p = 0.762 | NA | NA | 26/160 (16) | 86/668 (13) p = 0.26 | NA | NA | 1/26 (4) | NA | (9) | (26) |
| Lytic bone lesions | 26/61 (43) b | 100/295 (34) b | 617/1292 (48) c | 3457/7423 (47) c p = 0.431 | 82/109 (75) c | 334/403 (83) p = 0.569 c | 139/170 (82) | 644/868 (74) p = 0.04 | NA | NA | 18/26 (69) | NA | (59) | (76) |
| Elevated ß2MG a | NA | NA | 613/1377 (45) | 4141/7061 (59) p < 0.001 | (46) | (62) p < 0.001 | NA | NA | NA | NA | NA | NA | NA | NA |
| Protein isotype | ||||||||||||||
| Heavy chain | ||||||||||||||
| IgG | 40/61 (65) | 197/295 (67) | 924/1538 (60) | 4853/8091 (60) p = 0.943 | 75/194 (39) | 341/746 (46) p = 0.078 | 107/156 (69) | 375/632 (59) p = 0.10 | 34/86 (40) | 56/105 (53) p = 0.06 | (45) | (58) p = 0.237 | (50) | (55) |
| IgA | 11/61 (18) | 59/295 (20) | 318/1538 (21) | 2009/8091 (25) p < 0.001 | 28/194 (14) | 141/746 (19) p = 0.149 | 26/156 (17) | 127/632 (20) | 9/86 (10) | 21/105 (20) | (11) | (22) p = 0.080 | (5) | (12) |
| IgD | 1/61 (1) | 3/295 (1) | 43/1538 (3) | 251/8091 (3) p = 0.522 | 20/194 (10) | 41/746 (5.5) p = 0.015 | 1/156 (0.6) | 16/632 (3) | NA | NA | (4) | (1) p = 0.375 | NA | NA |
| IgM | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Light chain only | 8/61 (12) | 26/295 (8) | 197/1538 (13) | 824/8091 (10) p = 0.002 | 64/194 (33) | 195/746 (26) p = 0.057 | NA | NA | 26/86 (30) | 19/105 (18) | (33) | (16) p = 0.021 | (41) | (33) |
| Studies without a Comparator | Studies with a Comparator | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Shin 2017 [10] | Jurczyszyn 2019 [13] | Pál 2020 [14,15] | Duek 2021 [15] | Caulier 2021 [16] | Pydi 2021 [22] | Bao 2022 [17] h | Ludwig 2008 [9] | Jurczyszyn 2016 [19] | Lu 2016 [18] | Nakaya 2020 [21] | |||||
| Age studied (years) | ≤40 | ≤30 | ≤40 | <50 | ≤40 | ≤40 | <50 | <50 | ≥50 | 21–40 | 41–60 | <50 | ≥50 | <40 years | All patients Median 74 |
| Hyperdiploid | NA | NA | 6/11 (55) | 1/22 (4.5) | NA | NA | NA | NA | NA | NA | NA | 3/33 (9) | 8/120 (7) | NA | NA |
| Non-hyperdiploid | NA | 19/21 (90) | NA | NA | NA | NA | Hypodiploid 5/210 (2) | NA | NA | NA | NA | 4/33 (12) | 24/120 (20) | NA | NA |
| t(11;14) | NA | 1/20 (5) | NA | 15/22 (68) a,b | 9/35 (26) | 2/7 (29) | 42/210 (20) | NA | NA | NA | NA | NA | NA | 1/5 (20) | 83/316 (26) p = 0.461 |
| t(14;16) | 0/11 (0) | NA | NA | 0/22 (0) | 1/39 (2.5) | 1/7 (14) | NA | NA | NA | NA | NA | NA | NA | 0/7 (0) | 27/532 (5) p = 0.063 |
| t(14;20) | 0/6 (0) | NA | NA | 0/22 (0) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| t(8;14) | NA | NA | NA | NA | NA | NA | 4/210 (2) | NA | NA | NA | NA | NA | NA | NA | NA |
| t(4;14) | 1/10 (10) | 0/20 (0) | 3/11 (27) | 0/22 (0) | 19/156 (12) e | 1/7 (14) | 15/210 (7) | NA | NA | 26/81 (32) j | 31/181 (17) j p = 0.007 | NA | NA | 2/8 (25) | 168/802 (21) p = 0.659 |
| del (17p)/17 delp53 | 1/9 (11) | 2/21 (10) | 2/11 (18) | 1/22 (4.5) | 17/141 (12) e | 1/7 (14) | 15/210 (7) | NA | NA | 17/91 (19) i | 61/351 (17) p 0.771 i | 3/9 (33) | 86/606 (14) p = 0.008 | ||
| + or amp 1q21/1q gain | 4/15 (27) | 2/17 (12) | NA | NA | 17/56 (30) f | NA | 48/210 (23) | NA | NA | NA | NA | 49/87 (56) i | 139/313 (44) p = 0.064 i | NA | NA |
| del (1p32) | NA | NA | NA | 1/22 (4.5) c | 8/46 (17) g | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| del (13q)/ del 13 | 4/17 (24) | 8/26 (31) | NA | 9/22 (40) d | NA | 3/7 (43) | 72/210 (34) | 32/53 (60) i | 150/320 (47) p = 0.069 i | NA | NA | 13/37 (35) i | 58/141 (41) p = 0.507 i | 4/8 (50) | 211/435 (49) p = 1.000 |
| 17/109 (16) ii | 45/345 (13) p = 0.499 ii | 3/33 (9) ii | 9/120 (8) p = 0.767 ii | ||||||||||||
| del (9) | 1/16 (6) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Studies without a Comparator | Studies with a Comparator | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Shin 2017 [10] | Ravi 2018 [11] | Jurczyszyn 2019 [13] | Caulier 2021 [16] | Bao 2022 [17] | Jurczyszyn 2016 [19] | Nakaya 2020 [21] | Pál 2020 [14] | ||||
| n | 32 | 212 | 52 | 214 | 258 | 173 | 916 | 26 | 2277 | 16 | 296 |
| Age studied (years) | ≤40 | ≤50 | ≤30 | ≤40 | <50 | 21–40 | 41–60 | <40 | All | ≤40 | >40 |
| Year of diagnosis | 2000–2015 | 2005–2015 | 2006–2016 | 2000–2015 | 1992–2019 | 2000–2015 | 1998–2018 | 2006–2015 | |||
| Induction treatments (%) | Novel agents, unspecified | ||||||||||
| PI based | 10 | 45 b | 41 | 30 | 22 | NA | NA | NA | NA | 6 | NA |
| IMID based | 37 | 32 b | 24 | 1 | 10 | NA | NA | NA | NA | 13 | NA |
| PI + IMIDs | 40 a | 15 b | 21 | 37 | 27 | NA | NA | NA | NA | 69 | NA |
| Other (chemotherapy, melphalan, dexamethasone only) | 13 | 6 b | 15 | 26 | 41 | NA | NA | NA | NA | 13 | NA |
| Radiotherapy only | NA | NA | NA | 6 | NA | NA | NA | NA | NA | NA | NA |
| Transplant | |||||||||||
| ASCT (%) 1st line | 62 | NA | 62 | NA | NA | NA | NA | NA | NA | 88 | NA |
| ASCT (%)—at any stage | 79 | 52 | NA | 93 | 87 | 11 | 89 | 39 | NA | NA | NA |
| Allo-SCT (%) | 0 | NA | 3 | 25 | 5 c | NA | NA | 42 d | NA | NA | NA |
| Survival data | |||||||||||
| Median follow-up (months) | 64 | 69.6 | 86 | 76 | 93.6 | 51 | 78 | NA | NA | ||
| Median OS (months) | 61 | NA | 166 | 175 | 112.8 | NA | NA | NA | NA | NA | NA |
| 5-years OS (%) | 54 | 70 | 77 | 84 | 86 (NHBP) 66 (NHWP) | 83 | 67 p < 0.001 | 71 | 56 | 83 | 53 |
| Median PFS (months) | 16 | NA | NA | 41 | 38.4 (NHWP), 70.8 (NHPB) | NA | NA | NA | NA | NA | NA |
| 5-years PFS (%) | 14 | 28 | NA | NA | NA | NA | NA | NA | NA | 48 | 35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanguay, M.; Dagenais, C.; LeBlanc, R.; Ahmad, I.; Claveau, J.-S.; Roy, J. Young Myeloma Patients: A Systematic Review of Manifestations and Outcomes. Curr. Oncol. 2023, 30, 5214-5226. https://doi.org/10.3390/curroncol30060396
Tanguay M, Dagenais C, LeBlanc R, Ahmad I, Claveau J-S, Roy J. Young Myeloma Patients: A Systematic Review of Manifestations and Outcomes. Current Oncology. 2023; 30(6):5214-5226. https://doi.org/10.3390/curroncol30060396
Chicago/Turabian StyleTanguay, Mégane, Christophe Dagenais, Richard LeBlanc, Imran Ahmad, Jean-Sébastien Claveau, and Jean Roy. 2023. "Young Myeloma Patients: A Systematic Review of Manifestations and Outcomes" Current Oncology 30, no. 6: 5214-5226. https://doi.org/10.3390/curroncol30060396
APA StyleTanguay, M., Dagenais, C., LeBlanc, R., Ahmad, I., Claveau, J.-S., & Roy, J. (2023). Young Myeloma Patients: A Systematic Review of Manifestations and Outcomes. Current Oncology, 30(6), 5214-5226. https://doi.org/10.3390/curroncol30060396