Workforce Implications of Increased Referrals to Hereditary Cancer Services in Canada: A Scenario-Based Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
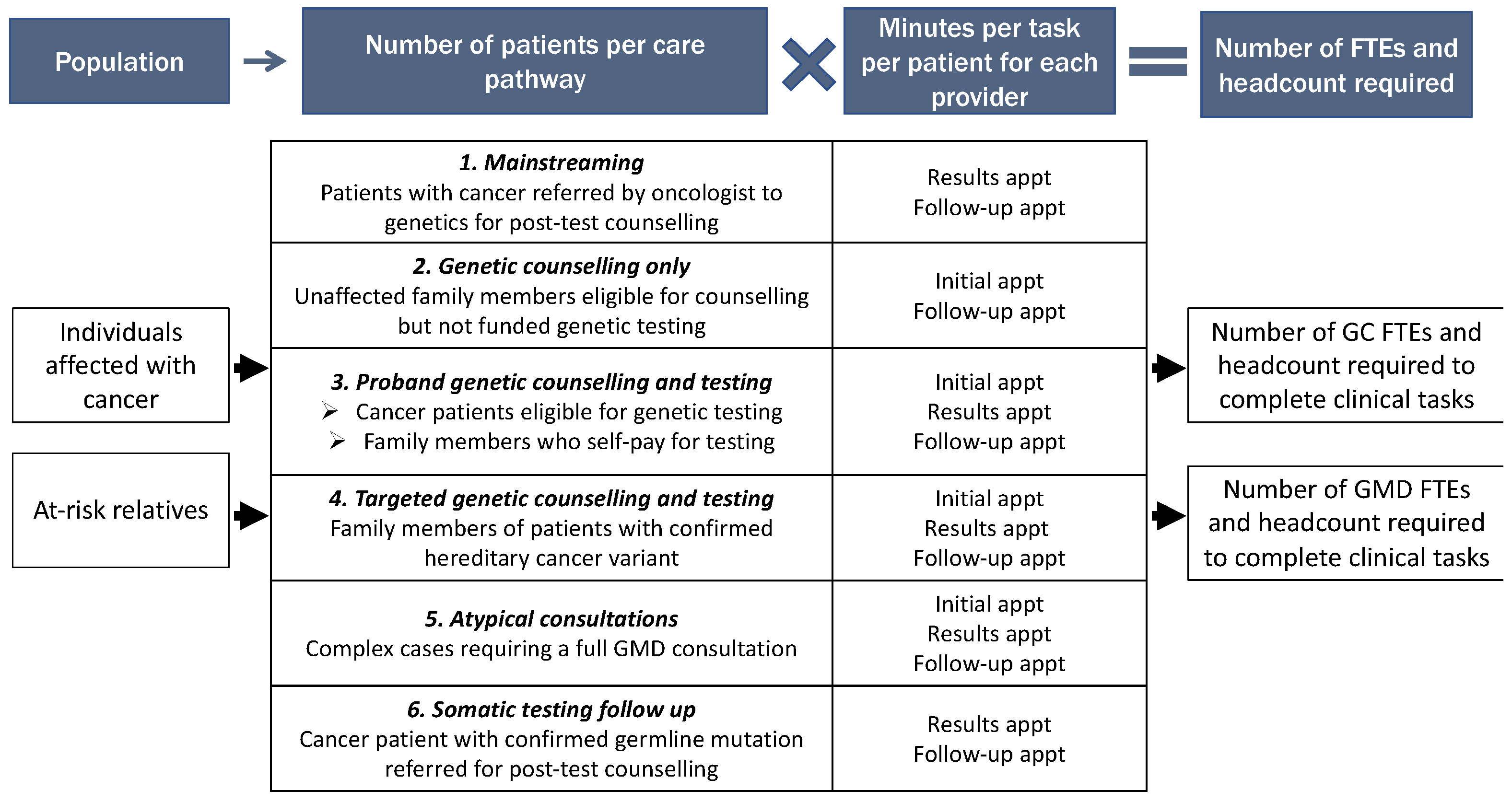
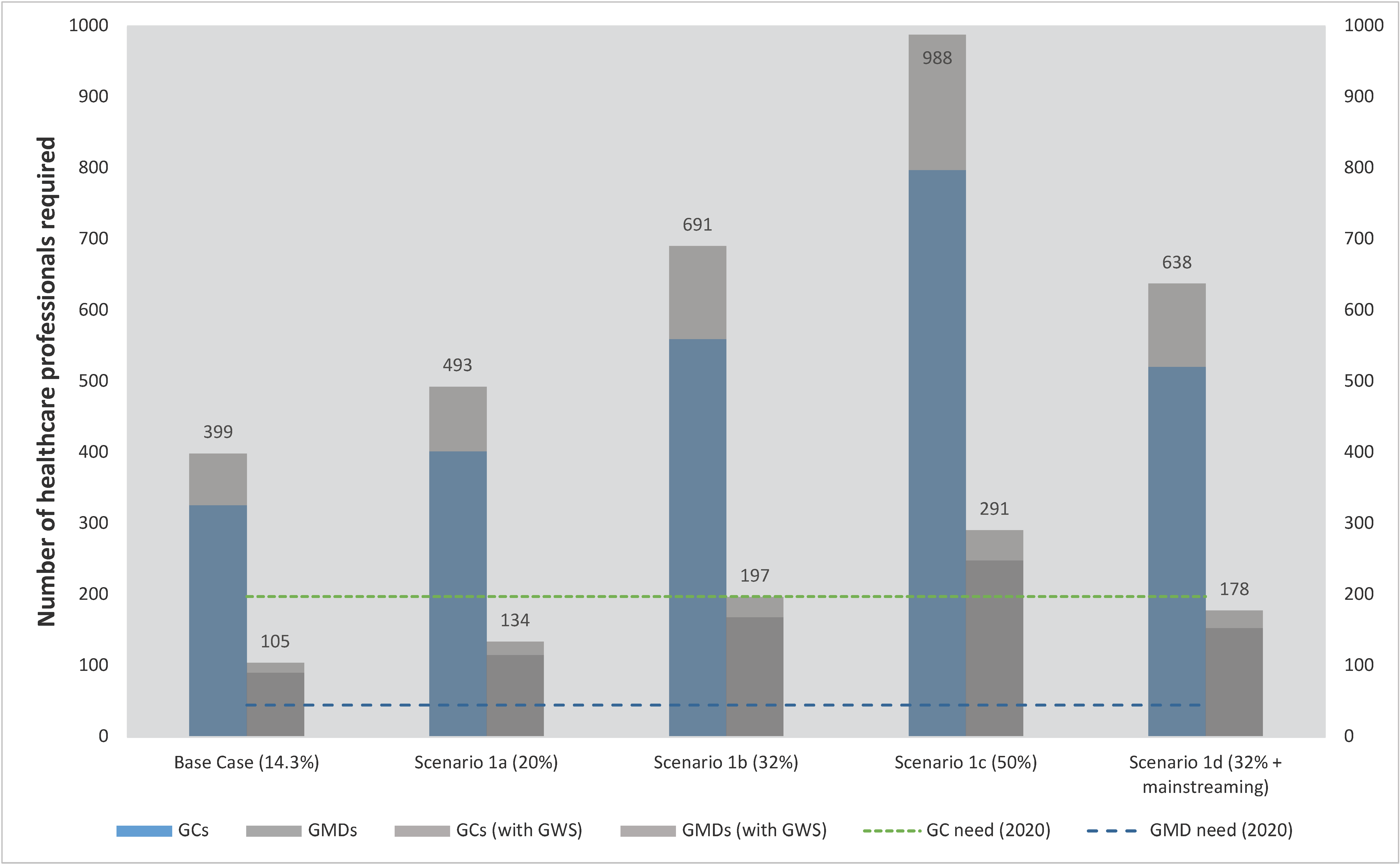
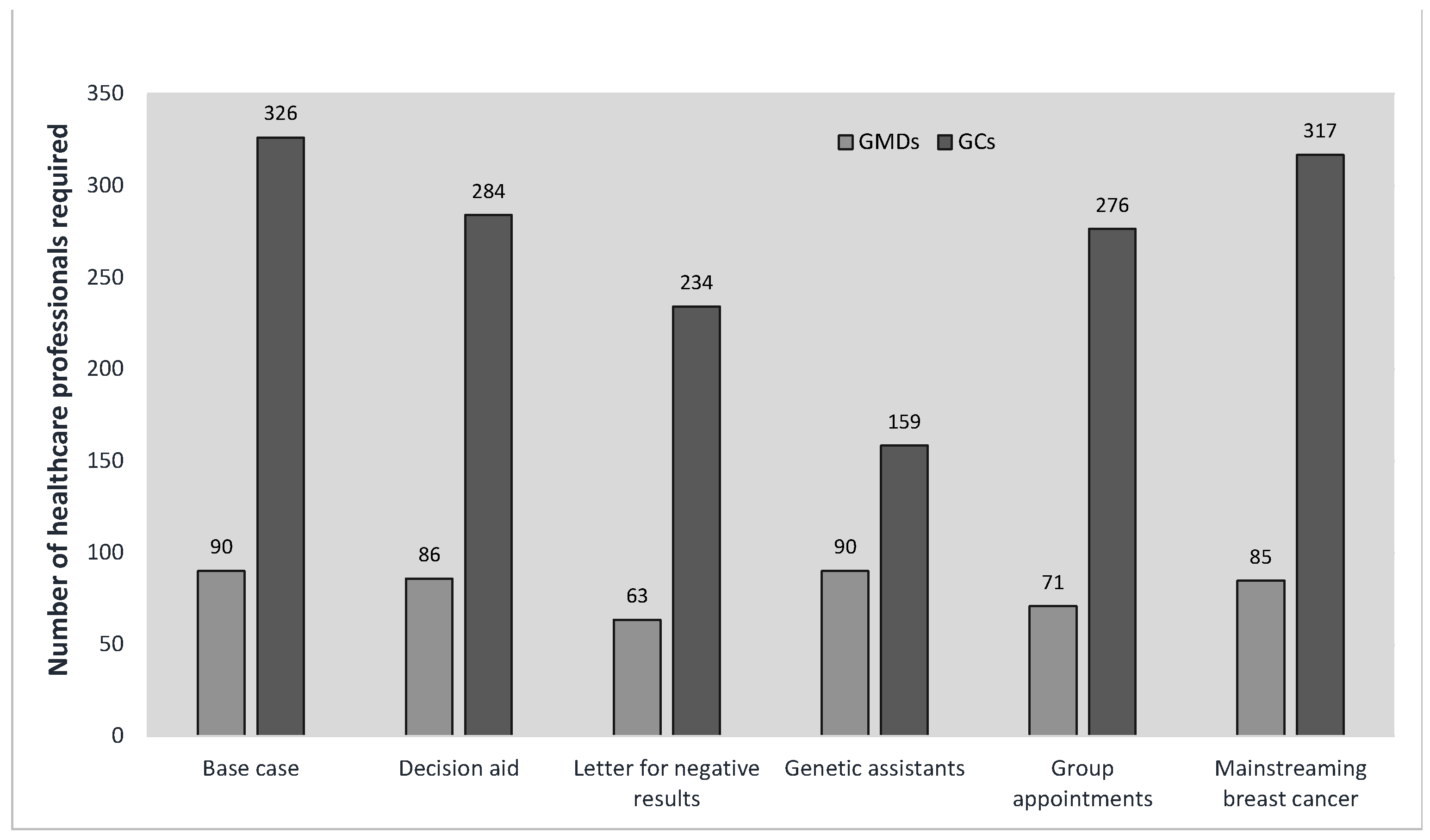
Scenarios
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Cancer Institute. The Genetics of Cancer. Available online: https://www.cancer.gov/about-cancer/causes-prevention/genetics (accessed on 6 July 2023).
- Valencia, O.M.; Samuel, S.E.; Viscusi, R.K.; Riall, T.S.; Neumayer, L.A.; Aziz, H. The Role of Genetic Testing in Patients With Breast Cancer: A Review. JAMA Surg. 2017, 152, 589. [Google Scholar] [CrossRef] [PubMed]
- Trepanier, A.; Ahrens, M.; McKinnon, W.; Peters, J.; Stopfer, J.; Grumet, S.C.; Manley, S.; Culver, J.O.; Acton, R.; Larsen-Haidle, J.; et al. Genetic Cancer Risk Assessment and Counseling: Recommendations of the National Society of Genetic Counselors. J. Genet. Couns. 2004, 13, 83–114. [Google Scholar] [CrossRef] [PubMed]
- Cancer Care Ontario. Recommendation Report for Ontario’s Clinical Genetic Services; Cancer Care Ontario: Toronto, Canada, 2018; pp. 1–28. [Google Scholar]
- Dragojlovic, N.; Kopac, N.; Borle, K.; Tandun, R.; Ellis, S.S.; Birch, P.; Adam, S.; Friedman, J.M.; GenCOUNSEL Study; Elliott, A.M.; et al. Utilization and Uptake of Clinical Genetics Services in High-Income Countries: A Scoping Review. Health Policy 2021, 125, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Costa, T.; Gillies, B.; Oh, T.; Scott, J. The Canadian Genetic Counseling Workforce: Perspectives from Employers and Recent Graduates. J. Genet. Couns. 2021, 30, 406–417. [Google Scholar] [CrossRef] [PubMed]
- Canadian Medical Association Medical Genetics Profile 2019. Available online: https://www.cma.ca/sites/default/files/2019-01/medical-genetics-e.pdf (accessed on 10 July 2023).
- Lambert, D.M.; Patrinos, D.; Knoppers, B.M.; GenCOUNSEL Study; Zawati, M.H. Genetic Counselors and Legal Recognition: A Made-for-Canada Approach. J. Genet. Couns. 2022, 31, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Enns, E.A.; Wainstein, T.; Dragojlovic, N.; Kopac, N.; GenCOUNSEL Study; Lynd, L.D.; Elliott, A.M. Far and Wide: Exploring Provider Utilization of Remote Service Provision for Genome-wide Sequencing in Canada. Mol. Genet. Genomic Med. 2021, 9, e1784. [Google Scholar] [CrossRef]
- National Society of Genetic Counselors. 2021 Professional Status Survey: Work Environment; National Society of Genetic Counselors: Chicago, IL, USA, 2021. [Google Scholar]
- Birch, S.; Kephart, G.; Murphy, G.T.; O’Brien-Pallas, L.; Alder, R.; MacKenzie, A. Health Human Resources Planning and the Production of Health: Development of an Extended Analytical Framework for Needs-Based Health Human Resources Planning. J. Public Health Manag. Pract. JPHMP 2009, 15, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Hurley, J. Chapter 2 An Overview of the Normative Economics of the Health Sector. In Handbook of Health Economics; Elsevier: Amsterdam, The Netherlands, 2000; Volume 1, pp. 55–118. ISBN 978-0-444-50470-8. [Google Scholar]
- Nisselle, A.; Macciocca, I.; McKenzie, F. Professional Status Survey of Genetic Counsellors and Clinical Geneticists; 2018; pp. 1–73. Available online: https://www.australiangenomics.org.au/publications/professional-status-survey-of-genetic-counsellors-and-clinical-geneticists/ (accessed on 15 March 2019).
- Borle, K.; Kopac, N.; Dragojlovic, N.; Rodriguez Llorian, E.; Friedman, J.M.; GenCOUNSEL Study; Elliott, A.M.; Lynd, L.D. Where Is Genetic Medicine Headed? Exploring the Perspectives of Canadian Genetic Professionals on Future Trends Using the Delphi Method. Eur. J. Hum. Genet. 2022, 30, 496–504. [Google Scholar] [CrossRef]
- Deveaux, S.; Le Ricousse, S. Oncogénétique En 2018—Consultations, Laboratoires et Suivi (2017 et 2018); Institute National du Cancer: Boulogne, France, 2018; Available online: https://www.e-cancer.fr/Expertises-et-publications/Catalogue-des-publications/Oncogenetique-en-2018-Consultations-laboratoires-et-suivi-2017-et-2018 (accessed on 15 November 2019).
- Elliott, A.M.; Friedman, J.M. The Importance of Genetic Counselling in Genome-Wide Sequencing. Nat. Rev. Genet. 2018, 19, 735–736. [Google Scholar] [CrossRef]
- Canadian Institute for Health Information. Health Workforce in Canada, 2017 to 2021: Overview—Data Tables 2022. Available online: https://www.cihi.ca/sites/default/files/document/health-workforce-canada-2017-2021-overview-meth-notes-en.pdf (accessed on 23 January 2023).
- Nisselle, A.; Macciocca, I.; McKenzie, F.; Vuong, H.; Dunlop, K.; McClaren, B.; Metcalfe, S.; Gaff, C. Readiness of Clinical Genetic Healthcare Professionals to Provide Genomic Medicine: An Australian Census. J. Genet. Couns. 2019, 28, 367–377. [Google Scholar] [CrossRef]
- Adam, F.; Fluri, M.; Scherz, A.; Rabaglio, M. Occurrence of Variants of Unknown Clinical Significance in Genetic Testing for Hereditary Breast and Ovarian Cancer Syndrome and Lynch Syndrome: A Literature Review and Analytical Observational Retrospective Cohort Study. BMC Med. Genom. 2023, 16, 7. [Google Scholar] [CrossRef] [PubMed]
- Burns, K.; Swanson, A.; Hoskovec, J.; Leonhard, J.; Hahn, S.; Stein, Q.P. Genetic Counseling Job Market in the United States and Canada: An Analysis of Job Advertisements 2014–2016. J. Genet. Couns. 2019, 28, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Abacan, M.; Alsubaie, L.; Barlow-Stewart, K.; Caanen, B.; Cordier, C.; Courtney, E.; Davoine, E.; Edwards, J.; Elackatt, N.J.; Gardiner, K.; et al. The Global State of the Genetic Counseling Profession. Eur. J. Hum. Genet. 2019, 27, 183–197. [Google Scholar] [CrossRef] [Green Version]
- Akras, Z.; Bungo, B.; Leach, B.H.; Marquard, J.; Ahluwalia, M.; Carraway, H.; Grivas, P.; Sohal, D.P.S.; Funchain, P. Primer on Hereditary Cancer Predisposition Genes Included Within Somatic Next-Generation Sequencing Panels. JCO Precis. Oncol. 2019, 3, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Yap, T.A.; Stadler, Z.K.; Stout, L.A.; Schneider, B.P. Aligning Germline Cancer Predisposition With Tumor-Based Next-Generation Sequencing for Modern Oncology Diagnosis, Interception, and Therapeutic Development. Am. Soc. Clin. Oncol. Educ. Book 2023, 43, e390738. [Google Scholar] [CrossRef]
- Institut National du Cancer. Les Tests de Génétique Somatique 2017. Available online: https://www.e-cancer.fr/Expertises-et-publications/La-plateforme-de-donnees-en-cancerologie (accessed on 4 January 2019).
- Anagnostou, V.; Jones, S.; Lytle, K.; Parpart-Li, S.; Nesselbush, M.; Adleff, V.; Riley, D.; Shukla, M.; Chesnick, B.; Kadan, M.; et al. Personalized Genomic Analyses for Cancer Mutation Discovery and Interpretation. JCO 2015, 33, 1529. [Google Scholar] [CrossRef]
- Bokkers, K.; Vlaming, M.; Engelhardt, E.G.; Zweemer, R.P.; Van Oort, I.M.; Kiemeney, L.A.L.M.; Bleiker, E.M.A.; Ausems, M.G.E.M. The Feasibility of Implementing Mainstream Germline Genetic Testing in Routine Cancer Care—A Systematic Review. Cancers 2022, 14, 1059. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, M.L.; Tomlinson, J.; Pearlman, R.; Abushahin, L.; Aeilts, A.; Chen, H.-Z.; Chen, Y.; Compton, A.; Elkhatib, R.; Geiger, L.; et al. Mainstreaming Germline Genetic Testing for Patients with Pancreatic Cancer Increases Uptake. Fam. Cancer 2023, 22, 91–97. [Google Scholar] [CrossRef]
- Tutika, R.K.; Bennett, J.A.; Abraham, J.; Snape, K.; Tatton-Brown, K.; Kemp, Z.; Copson, E.; Openshaw, M.R. Mainstreaming of Genomics in Oncology: A Nationwide Survey of the Genomics Training Needs of UK Oncologists. Clin. Med. 2023, 23, 9–15. [Google Scholar] [CrossRef]
- Dragojlovic, N.; Borle, K.; Kopac, N.; Ellis, U.; Birch, P.; Adam, S.; Friedman, J.M.; Nisselle, A.; GenCOUNSEL Study; Elliott, A.M.; et al. The Composition and Capacity of the Clinical Genetics Workforce in High-Income Countries: A Scoping Review. Genet. Med. 2020, 22, 1437–1449. [Google Scholar] [CrossRef] [PubMed]
- Sebastian, A.; Carroll, J.C.; Oldfield, L.E.; Mighton, C.; Shickh, S.; Uleryk, E.; Bombard, Y. Effect of Genetics Clinical Decision Support Tools on Health-Care Providers’ Decision Making: A Mixed-Methods Systematic Review. Genet. Med. 2021, 23, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Shickh, S.; Assamad, D.; Luca, S.; Clausen, M.; Somerville, C.; Tafler, A.; Shaw, A.; Hayeems, R.; Bombard, Y. Patient-Facing Digital Tools for Delivering Genetic Services: A Systematic Review. J. Med. Genet. 2023, 60, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hoxhaj, I.; Beccia, F.; Calabrò, G.E.; Boccia, S. A Web Screening on Training Initiatives in Cancer Genomics for Healthcare Professionals. Genes 2022, 13, 430. [Google Scholar] [CrossRef] [PubMed]
- Medendorp, N.M.; Van Den Heuvel, L.M.; Han, P.K.J.; Hillen, M.A.; Smets, E.M.A. Communication Skills Training for Healthcare Professionals in Providing Genetic Counseling: A Scoping Literature Review. Patient Educ. Couns. 2021, 104, 20–32. [Google Scholar] [CrossRef]
- Williams, M.S.; Buchanan, A.H.; Davis, F.D.; Faucett, W.A.; Hallquist, M.L.G.; Leader, J.B.; Martin, C.L.; McCormick, C.Z.; Meyer, M.N.; Murray, M.F.; et al. Patient-Centered Precision Health In A Learning Health Care System: Geisinger’s Genomic Medicine Experience. Health Aff. 2018, 37, 757–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burki, T. UK Explores Whole-Genome Sequencing for Newborn Babies. Lancet 2022, 400, 260–261. [Google Scholar] [CrossRef]
- Kingsmore, S.F.; Smith, L.D.; Kunard, C.M.; Bainbridge, M.; Batalov, S.; Benson, W.; Blincow, E.; Caylor, S.; Chambers, C.; Del Angel, G.; et al. A Genome Sequencing System for Universal Newborn Screening, Diagnosis, and Precision Medicine for Severe Genetic Diseases. Am. J. Hum. Genet. 2022, 109, 1605–1619. [Google Scholar] [CrossRef]
- Stark, Z.; Scott, R.H. Genomic Newborn Screening for Rare Diseases. Nat. Rev. Genet. 2023. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Y.; Poirier, A.; Yong, J.; Garner, R.; Sun, Z.; Than, J.; Brenner, D.R. Long-Term Projections of Cancer Incidence and Mortality in Canada: The OncoSim All Cancers Model. Prev. Med. 2023, 168, 107425. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Canada’s Population Estimates: Record-High Population Growth in 2022. Daily. 2023. Available online: https://www150.statcan.gc.ca/n1/en/daily-quotidien/230322/dq230322f-eng.pdf (accessed on 10 July 2023).
- Caswell-Jin, J.L.; Gupta, T.; Hall, E.; Petrovchich, I.M.; Mills, M.A.; Kingham, K.E.; Koff, R.; Chun, N.M.; Levonian, P.; Lebensohn, A.P.; et al. Racial/Ethnic Differences in Multiple-Gene Sequencing Results for Hereditary Cancer Risk. Genet. Med. 2018, 20, 234–239. [Google Scholar] [CrossRef]
- Lohn, Z.; Fok, A.; Richardson, M.; Derocher, H.; Mung, S.W.; Nuk, J.; Yuson, J.; Jevon, M.; Schrader, K.A.; Sun, S. Large-scale Group Genetic Counseling: Evaluation of a Novel Service Delivery Model in a Canadian Hereditary Cancer Clinic. J. Genet. Couns. 2022, 31, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Birch, P.; Adam, S.; Bansback, N.; Coe, R.R.; Hicklin, J.; Lehman, A.; Li, K.C.; Friedman, J.M. DECIDE: A Decision Support Tool to Facilitate Parents’ Choices Regarding Genome-Wide Sequencing. J. Genet. Counsel. 2016, 25, 1298–1308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, S.; Birch, P.H.; Coe, R.R.; Bansback, N.; Jones, A.L.; Connolly, M.B.; Demos, M.K.; Toyota, E.B.; Farrer, M.J.; Friedman, J.M. Assessing an Interactive Online Tool to Support Parents’ Genomic Testing Decisions. J. Genet. Couns. 2019, 28, 10–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bombard, Y.; Clausen, M.; Shickh, S.; Mighton, C.; Casalino, S.; Kim, T.H.M.; Muir, S.M.; Carlsson, L.; Baxter, N.; Scheer, A.; et al. Effectiveness of the Genomics ADvISER Decision Aid for the Selection of Secondary Findings from Genomic Sequencing: A Randomized Clinical Trial. Genet. Med. 2020, 22, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Nisselle, A.; King, E.; Terrill, B.; Davey, B.; McClaren, B.; Dunlop, K.; Graves, D.; Metcalfe, S.; Gaff, C. Investigating Genomic Medicine Practice and Perceptions amongst Australian Non-Genetics Physicians to Inform Education and Implementation. npj Genom. Med. 2023, 8, 13. [Google Scholar] [CrossRef]
- Husereau, D.; Villalba, E.; Muthu, V.; Mengel, M.; Ivany, C.; Steuten, L.; Spinner, D.S.; Sheffield, B.; Yip, S.; Jacobs, P.; et al. Progress toward Health System Readiness for Genome-Based Testing in Canada. Curr. Oncol. 2023, 30, 5379–5394. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Year | Referrals | Initial Appointments | Results/FU 1 Appointments | GMD DPC-FTEs | GMD Headcount | GC DPC- FTEs | GC Headcount | |
|---|---|---|---|---|---|---|---|---|
| Deterministic projections | ||||||||
| 2020 | 76,710 | 52,331 | 56,961 | 40.7 | 52.7 | 179.2 | 198.0 | |
| 2030 | 125,904 | 86,889 | 93,969 | 69.7 | 90.2 | 295.4 | 326.4 | |
| Probabilistic projections | ||||||||
| 2020 mean (95% CI) | 77,295 (53,748 to 108,468) | 52,708 (35,925 to 74,484) | 57,461 (39,459 to 82,854) | 40.9 (31.4 to 53.8) | 53.0 (40.6 to 69.6) | 180.5 (121.9 to 259.6) | 199.5 (134.7 to 286.9) | |
| 2030 mean (95% CI) | 126,799 (90,847 to 174,801) | 87,457 (61,865 to 1212,329) | 94,722 (66,702 to 133,550) | 70.0 (55.2 to 90.1) | 90.7 (71.4 to 116.6) | 297.4 (206.1 to 420.7) | 328.6 (227.7 to 464.9) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dragojlovic, N.; Borle, K.; Kopac, N.; Nisselle, A.; Nuk, J.; Jevon, M.; Friedman, J.M.; Elliott, A.M.; Lynd, L.D. Workforce Implications of Increased Referrals to Hereditary Cancer Services in Canada: A Scenario-Based Analysis. Curr. Oncol. 2023, 30, 7241-7251. https://doi.org/10.3390/curroncol30080525
Dragojlovic N, Borle K, Kopac N, Nisselle A, Nuk J, Jevon M, Friedman JM, Elliott AM, Lynd LD. Workforce Implications of Increased Referrals to Hereditary Cancer Services in Canada: A Scenario-Based Analysis. Current Oncology. 2023; 30(8):7241-7251. https://doi.org/10.3390/curroncol30080525
Chicago/Turabian StyleDragojlovic, Nick, Kennedy Borle, Nicola Kopac, Amy Nisselle, Jennifer Nuk, Mandy Jevon, Jan M. Friedman, Alison M. Elliott, and Larry D. Lynd. 2023. "Workforce Implications of Increased Referrals to Hereditary Cancer Services in Canada: A Scenario-Based Analysis" Current Oncology 30, no. 8: 7241-7251. https://doi.org/10.3390/curroncol30080525
APA StyleDragojlovic, N., Borle, K., Kopac, N., Nisselle, A., Nuk, J., Jevon, M., Friedman, J. M., Elliott, A. M., & Lynd, L. D. (2023). Workforce Implications of Increased Referrals to Hereditary Cancer Services in Canada: A Scenario-Based Analysis. Current Oncology, 30(8), 7241-7251. https://doi.org/10.3390/curroncol30080525