A Rare Case of Complete-Immunotherapy-Responsive Metastatic Non-Small Cell Lung Cancer with Long Lasting Progression-Free Survival: A Case Report

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Case Report
3. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Lung Cancer. Available online: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx (accessed on 6 June 2023).
- Bade, B.C.; Cruz, C.S.D. Lung Cancer 2020: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2020, 41, 1–24. [Google Scholar] [CrossRef]
- Office of the Surgeon General, U.S. Public Health Service. The Health Consequences of Smoking; 72-7516 PNH; National Clearinghouse for Smoking Health: Washington, DC, USA, 1972. [Google Scholar]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424, Erratum in CA Cancer J Clin. 2020, 70, 313. [Google Scholar] [CrossRef]
- Ajrouche, R.; Ielsch, G.; Cléro, E.; Roudier, C.; Gay, D.; Guillevic, J.; Laurier, D.; Le Tertre, A. Quantitative Health Risk Assessment of Indoor Radon: A Systematic Review. Radiat. Prot. Dosim. 2017, 177, 69–77. [Google Scholar] [CrossRef]
- Alberg, A.J.; Brock, M.V.; Ford, J.G.; Samet, J.M.; Spivack, S.D. Epidemiology of lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143 (Suppl. S5), e1S–e29S. [Google Scholar] [CrossRef]
- Gnagnarella, P.; Caini, S.; Maisonneuve, P.; Gandini, S. Carcinogenicity of High Consumption of Meat and Lung Cancer Risk Among Non-Smokers: A Comprehensive Meta-Analysis. Nutr. Cancer 2018, 70, 1–13. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Scagliotti, G.V.; Parikh, P.; Von Pawel, J.; Biesma, B.; Vansteenkiste, J.; Serwatowski, C.M.; Serwatowski, P.; Gatzemeier, U.; Digumarti, R.; Zukin, M.; et al. Phase III Study Comparing Cisplatin Plus Gemcitabine with Cisplatin Plus Pemetrexed in Chemotherapy-Naive Patients with Advanced-Stage Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2008, 26, 3543–3551, Corrected and Republished in J. Clin. Oncol. 2023, 41, 2458–2466. [Google Scholar] [CrossRef]
- AIOM-Linee Guida Nazionali “Neoplasie del Polmone 2016. Available online: https://www.aiom.it/neoplasie-del-polmone-5 (accessed on 30 December 2023).
- Detterbeck, F.C.; Boffa, D.J.; Kim, A.W.; Tanoue, L.T. The Eighth Edition Lung Cancer Stage Classification. Chest 2017, 151, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Kocher, F.; Hilbe, W.; Seeber, A.; Pircher, A.; Schmid, T.; Greil, R.; Auberger, J.; Nevinny-Stickel, M.; Sterlacci, W.; Tzankov, A.; et al. Longitudinal analysis of 2293 NSCLC patients: A comprehensive study from the TYROL registry. Lung Cancer 2015, 87, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Fedewa, S.A. Lung Cancer Screening with Low-Dose Computed Tomography in the United States—2010 to 2015. JAMA Oncol. 2017, 3, 1278–1281. [Google Scholar] [CrossRef]
- National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef] [PubMed]
- Walter, J.E.; Heuvelmans, M.A.; Yousaf-Khan, U.; Dorrius, M.D.; Thunnissen, E.; Schermann, A.; Groen, H.J.; van der Aalst, C.M.; Nackaerts, K.; Vliegenthart, R.; et al. New Subsolid Pulmonary Nodules in Lung Cancer Screening: The NELSON Trial. J. Thorac. Oncol. 2018, 13, 1410–1414. [Google Scholar] [CrossRef]
- Jonas, D.E.; Reuland, D.S.; Reddy, S.M.; Nagle, M.; Clark, S.D.; Weber, R.P.; Enyioha, C.; Malo, T.L.; Brenner, A.T.; Armstrong, C.; et al. Screening for Lung Cancer with Low-Dose Computed Tomography: An Evidence Review for the U.S. Preventive Services Task Force. Rockville (MD): Agency for Healthcare Research and Quality (US); March 2021. (Evidence Synthesis, No. 198). Available online: https://www.ncbi.nlm.nih.gov/books/NBK568573/ (accessed on 25 November 2023).
- Doria-Rose, V.P.; White, M.C.; Klabunde, C.N.; Nadel, M.R.; Richards, T.B.; McNeel, T.S.; Rodriguez, J.L.; Marcus, P.M. Use of Lung Cancer Screening Tests in the United States: Results from the 2010 National Health Interview Survey. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1049–1059. [Google Scholar] [CrossRef] [PubMed]
- Dal Bello, M.G.; Filiberti, R.A.; Alama, A.; Orengo, A.M.; Mussap, M.; Coco, S.; Vanni, I.; Boccardo, S.; Rijavec, E.; Genova, C.; et al. The role of CEA, CYFRA21-1 and NSE in monitoring tumor response to Nivolumab in advanced non-small cell lung cancer (NSCLC) patients. J. Transl. Med. 2019, 17, 74. [Google Scholar] [CrossRef]
- Osmani, L.; Askin, F.; Gabrielson, E.; Li, Q.K. Current WHO guidelines and the critical role of immunohistochemical markers in the subclassification of non-small cell lung carcinoma (NSCLC): Moving from targeted therapy to immunotherapy. Semin. Cancer Biol. 2018, 52, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, H.; Nemoto, Y.; Nakamura, K.; Ikeda, T.; Tachibana, H.; Fukuda, H.; Yoshida, K.; Kobayashi, H.; Iizuka, J.; Shimmura, H.; et al. Prognostic Impact of Early Treatment Interruption of Nivolumab Plus Ipilimumab Due to Immune-Related Adverse Events as First-Line Therapy for Metastatic Renal Cell Carcinoma: A Multi-Institution Retrospective Study. Target. Oncol. 2021, 16, 493–502. [Google Scholar] [CrossRef]
- Kus, T.; Aktas, G. Durable response after interruption of nivolumab in patients with metastatic renal cell carcinoma: Is renal toxicity a marker to predict the benefit of nivolumab? J. Oncol. Pharm. Pract. 2020, 26, 1000–1004. [Google Scholar] [CrossRef]
- Alexander, M.; Kim, S.Y.; Cheng, H. Update 2020: Management of Non-Small Cell Lung Cancer. Lung 2020, 198, 897–907. [Google Scholar] [CrossRef]
- Simeone, J.C.; Nordstrom, B.L.; Patel, K.; Klein, A.B. Treatment patterns and overall survival in metastatic non-small-cell lung cancer in a real-world, US setting. Futur. Oncol. 2019, 15, 3491–3502. [Google Scholar] [CrossRef]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez–Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated Analysis of KEYNOTE-024: Pembrolizumab Versus Platinum-Based Chemotherapy for Advanced Non–Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score of 50% or Greater. J. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gumus, M.; Mazieres, J.; Hermes, B.; Cay Senler, F.; Csoszi, T.; Fulop, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small- Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Mok, T.S.K.; Wu, Y.-L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Wu, Y.; Zhang, L.; Fan, Y.; Zhou, J.; Zhou, Q.; Li, W.; Hu, C.; Chen, G.; Zhang, X.; Zhou, C.; et al. Randomized clinical trial of pembrolizumab vs chemotherapy for previously untreated Chinese patients with PD-L1-positive locally advanced or metastatic non–small-cell lung cancer: KEYNOTE-042 China Study. Int. J. Cancer 2021, 148, 2313–2320. [Google Scholar] [CrossRef]
- Chen, D.; Menon, H.; Verma, V.; Guo, C.; Ramapriyan, R.; Barsoumian, H.; Younes, A.; Hu, Y.; Wasley, M.; Cortez, M.A.; et al. Response and outcomes after anti-CTLA4 versus anti-PD1 combined with stereotactic body radiation therapy for metastatic non-small cell lung cancer: Retrospective analysis of two single-institution prospective trials. J. Immunother. Cancer 2020, 8, e000492, Erratum in J. Immunother. Cancer 2020, 8, e000492corr1. [Google Scholar] [CrossRef] [PubMed]
- Ni, J.; Yang, L.; Zhu, H.; Chu, M.; Zhang, C.; Zhao, W.; Yang, M.; Xu, X.; Zheng, E.; Jiang, X.; et al. A patient with metastatic non-small cell lung cancer who received pembrolizumab monotherapy after stereotactic body radiotherapy had progression-free survival of nearly 5 years: A case report. Ann. Palliat. Med. 2021, 10, 4999–5009. [Google Scholar] [CrossRef] [PubMed]
- Grati, O.T.; Zemoura, L.; Nhy, C.; Daniel, C.; Melaabi, S.; Callens, C.; Villars, M.G.; Bièche, I.; Girard, N. Long response to immune checkpoint inhibitors in metastatic NSCLC despite EGFR germline mutation. A case report. Lung Cancer 2022, 174, 186–187. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.W.; Kwon, J.; Lim, T. Long-Term Response of Pembrolizumab in a Patient with Metastatic Squamous Non-Small Cell Lung Cancer on Hemodialysis: Case Report and Review of the Literature. Medicina 2023, 59, 325. [Google Scholar] [CrossRef]
- Matsuzaki, T.; Iwami, E.; Sasahara, K.; Kuroda, A.; Nakajima, T.; Terashima, T. A case report of metastatic lung adenocarcinoma with long-term survival for over 11 years. Medicine 2019, 98, e14100. [Google Scholar] [CrossRef] [PubMed]
- Baseri, B.; Samra, B.; Tam, E.; Chiu, E.; Leaf, A. An Exceptional Responder to Nivolumab in Metastatic Non-Small-Cell Lung Cancer: A Case Report and Literature Review of Long-Term Survivors. Case Rep. Oncol. Med. 2019, 2019, 1816472. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Pu, Y.; Dai, N.; Wang, D.; Xu, M.M. Complete response of radioresistant brain metastases from non-small cell lung cancer with temozolomide. Medicine 2020, 99, e23592. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Event | Relevant Data |
|---|---|---|
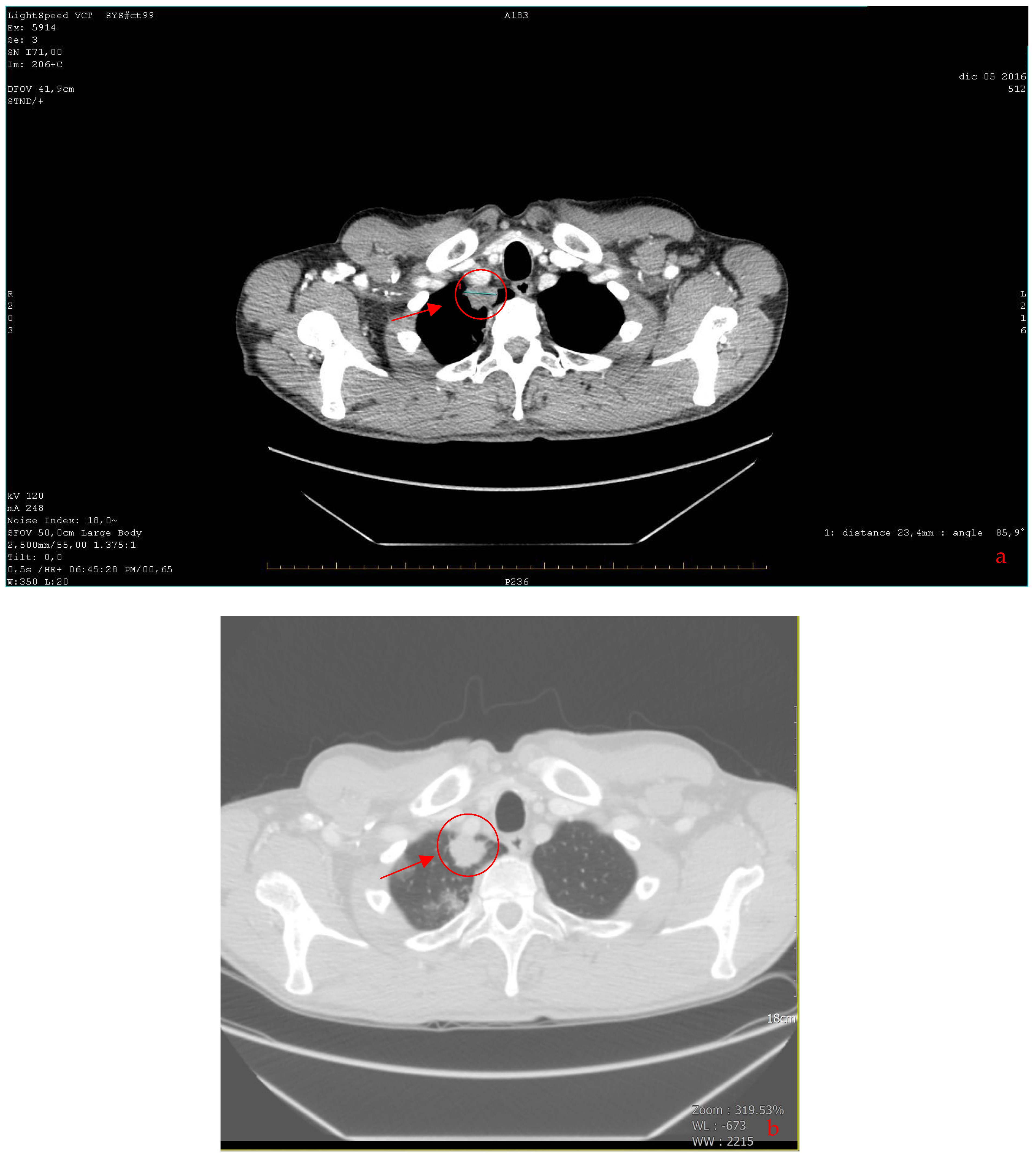
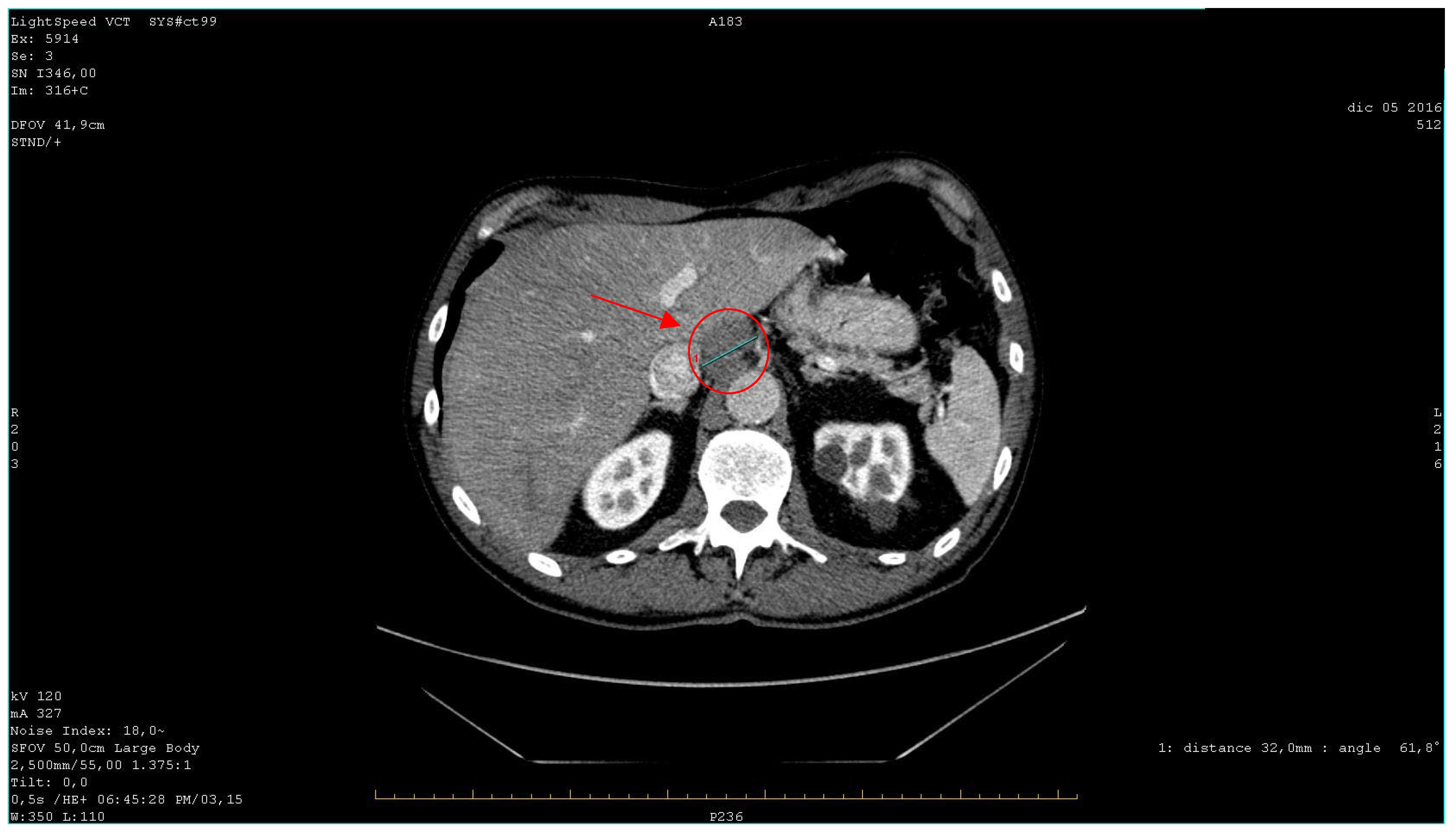
| 2016 | Patient presentation Diagnosis Abdominal ultrasound Total body CT scan | Worsening non-productive night cough, no dyspnea. Metastatic lung cancer. Presence of malignant lymph nodes near the hepatic hilum. Solid nodular- like expansive process in the right upper lobe of the lung and multiple lymphadenopathies in the mediastinum and abdomen. |
| 2016 | US-guided biopsy Immunochemistry EGFR mutation study | Poorly differentiated neoplasm suggestive of primary lung cancer. Positive for CKAE1/AE3, CK7, EMA, focally for TTF1 and p63. Negative for CK5/6, CD56, Chromogranin A, and Synaptophysin. Ki67 value: 50%. Negative result for exons 18, 19, 20, and 21. |
| 2016 | Chemotherapy initiation | Cisplatin (70 mg/m2 dL every 21 days) and gemcitabine (1000 mg/m2, d 1, 8 every 21 days). |
| 2016 | Partial response to therapy | Reduction in the size of the lung tumor and lymphadenopathies. |
| 2017 | Bone scintigraphy | Negative results for skeletal metastases. |
| 2017 | Immunotherapy initiation | Nivolumab (3 mg/kg every two weeks). |
| 2019 | Nivolumab discontinuation | Complete response observed. |
| 2023 | Latest total body CT scan | No evidence of neoplastic disease detected. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Intinis, C.; Izzo, P.; Codacci-Pisanelli, M.; Izzo, L.; Messineo, D.; Sibio, S.; Campagnol, M.; Lai, S.; Molle, M.; Izzo, S. A Rare Case of Complete-Immunotherapy-Responsive Metastatic Non-Small Cell Lung Cancer with Long Lasting Progression-Free Survival: A Case Report. Curr. Oncol. 2024, 31, 723-732. https://doi.org/10.3390/curroncol31020053
De Intinis C, Izzo P, Codacci-Pisanelli M, Izzo L, Messineo D, Sibio S, Campagnol M, Lai S, Molle M, Izzo S. A Rare Case of Complete-Immunotherapy-Responsive Metastatic Non-Small Cell Lung Cancer with Long Lasting Progression-Free Survival: A Case Report. Current Oncology. 2024; 31(2):723-732. https://doi.org/10.3390/curroncol31020053
Chicago/Turabian StyleDe Intinis, Claudia, Paolo Izzo, Massimo Codacci-Pisanelli, Luciano Izzo, Daniela Messineo, Simone Sibio, Monica Campagnol, Silvia Lai, Marcello Molle, and Sara Izzo. 2024. "A Rare Case of Complete-Immunotherapy-Responsive Metastatic Non-Small Cell Lung Cancer with Long Lasting Progression-Free Survival: A Case Report" Current Oncology 31, no. 2: 723-732. https://doi.org/10.3390/curroncol31020053