Chylous Ascites Associated with Advanced Pancreatic Cancer That Improved with Appropriate Treatment: A Case Report

 , ,
, ,
Abstract
1. Introduction
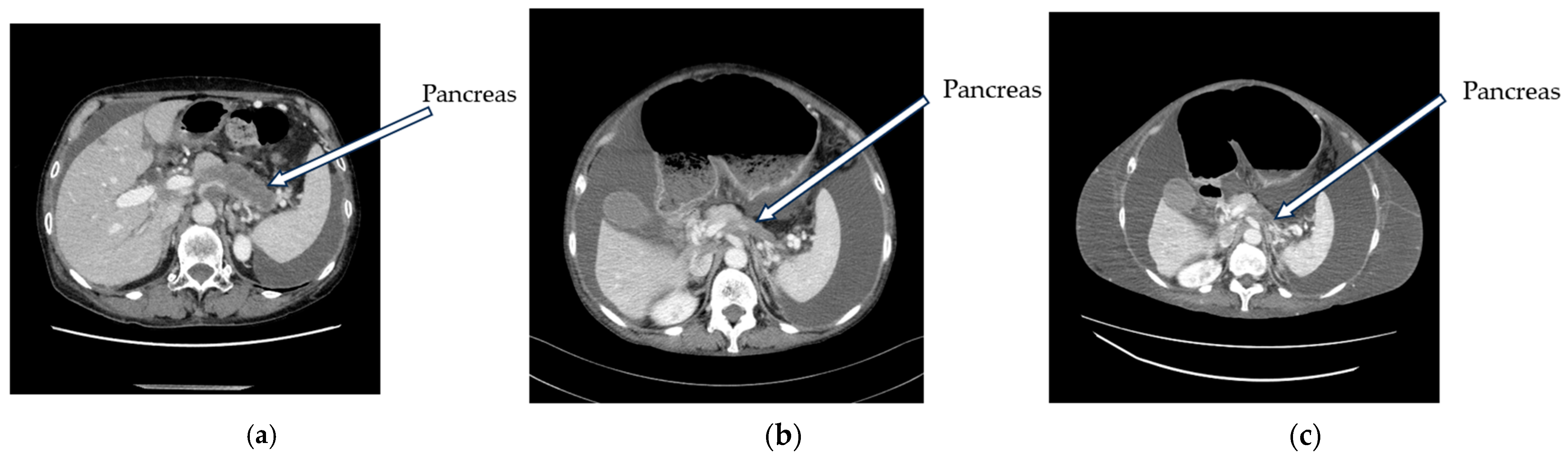
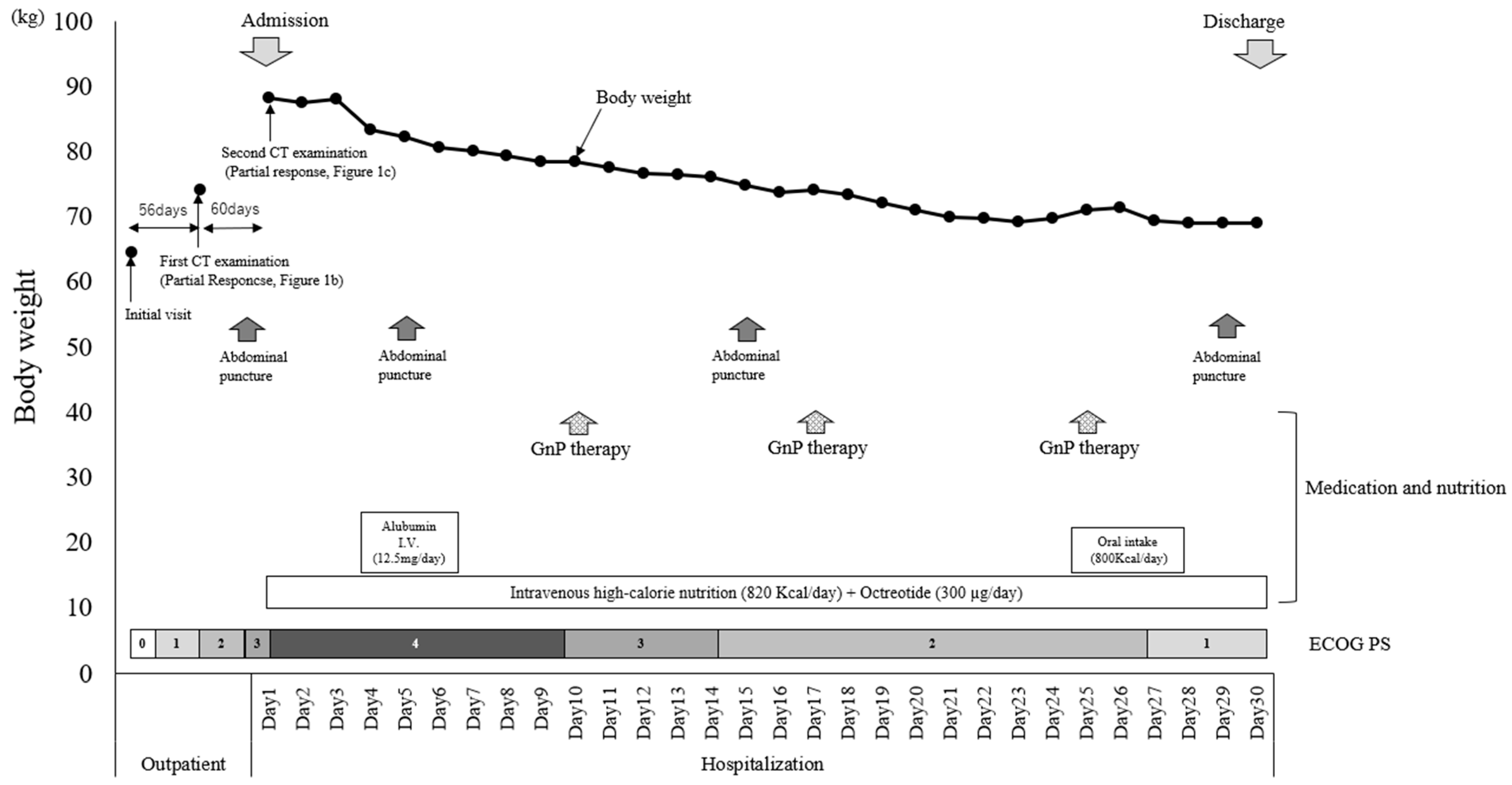
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, J.; Won, J.H. Percutaneous Treatment of Chylous Ascites. Tech. Vasc. Interv. Radiol. 2016, 19, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Satala, C.B.; Bara, T.J.; Jung, I.; Tudorache, V.; Gurzu, S. Chylous Ascites, Unusual Association with Ductal Pancreatic Adenocarcinoma with Plasmacytoid Morphology: A Case Report and Literature Review. Surg. J. 2021, 7, e158–e162. [Google Scholar] [CrossRef] [PubMed]
- Wagayama, H.; Tanaka, T.; Shimomura, M.; Ogura, K.; Shiraki, K. Pancreatic cancer with chylous ascites demonstrated by lymphoscintigraphy: Successful treatment with peritoneovenous shunting. Dig. Dis. Sci. 2002, 47, 1836–1838. [Google Scholar] [CrossRef] [PubMed]
- Fangsaard, P.; Puriwekin, J.; Phattraprayoon, N.; Ungtrakul, T. Unusual Presentation of Bilateral Chylothorax and Chylous Ascites with Pancreatic Adenocarcinoma: A Case Report. Case Rep. Oncol. 2022, 15, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Duletzke, N.T.; Kiraly, L.N.; Martindale, R.G. Chylothorax and chylous ascites: Overview, management, and nutrition. Nutr. Clin. Pract. Off. Publ. Am. Soc. Parenter. Enter. Nutr. 2023, 38, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, R.; Vaziri, H.; Gautam, A.; Ballesteros, E.; Karimeddini, D.; Wu, G.Y. Chylous Ascites: A Review of Pathogenesis, Diagnosis and Treatment. J. Clin. Transl. Hepatol. 2018, 6, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Tulunay, G.; Ureyen, I.; Turan, T.; Karalok, A.; Kavak, D.; Ozgul, N.; Ocalan, R.; Tapisiz, O.L.; Boran, N.; Kose, M.F. Chylous ascites: Analysis of 24 patients. Gynecol. Oncol. 2012, 127, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Assumpcao, L.; Cameron, J.L.; Wolfgang, C.L.; Edil, B.; Choti, M.A.; Herman, J.M.; Geschwind, J.F.; Hong, K.; Georgiades, C.; Schulick, R.D.; et al. Incidence and management of chyle leaks following pancreatic resection: A high volume single-center institutional experience. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2008, 12, 1915–1923. [Google Scholar] [CrossRef] [PubMed]
- Malik, H.Z.; Crozier, J.; Murray, L.; Carter, R. Chyle leakage and early enteral feeding following pancreatico-duodenectomy: Management options. Dig. Surg. 2007, 24, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Kuboki, S.; Shimizu, H.; Yoshidome, H.; Ohtsuka, M.; Kato, A.; Yoshitomi, H.; Furukawa, K.; Miyazaki, M. Chylous ascites after hepatopancreatobiliary surgery. Br. J. Surg. 2013, 100, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.J.; Kim, S.H.; Kwak, J.M.; Kim, J. Incidence and risk factors of chylous ascites after colorectal cancer surgery. Am. J. Surg. 2013, 206, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Aoki, H.; Takakura, N.; Shiozaki, S.; Matsukawa, H. Milk-based test as a preventive method for chylous ascites following pancreatic resection. Dig. Surg. 2010, 27, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Lizaola, B.; Bonder, A.; Trivedi, H.D.; Tapper, E.B.; Cardenas, A. Review article: The diagnostic approach and current management of chylous ascites. Aliment. Pharmacol. Ther. 2017, 46, 816–824. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.H.; Kim, S.G.; Park, K.S.; Ahn, D.J.; Kim, M.K. Chylothorax associated with primary membranous nephropathy: A case report. Ann. Palliat. Med. 2023, 12, 834–842. [Google Scholar] [CrossRef]
- Rashid, R.; Shafi Ahmed, S.; Mahmud, S. Congenital Chylous Ascites: A Rare Cause of Infantile Ascites Treated with MCT-Based Diet and Octreotide. JPGN Rep. 2022, 3, e149. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Pandit, N.; Krishnamurthy, G.; Gupta, R.; Verma, G.R.; Singh, R. Management of chylous ascites following pancreaticobiliary surgery. JGH Open Open Access J. Gastroenterol. Hepatol. 2019, 3, 425–428. [Google Scholar] [CrossRef]
- Bhatia, C.; Pratap, U.; Slavik, Z. Octreotide therapy: A new horizon in treatment of iatrogenic chyloperitoneum. Arch. Dis. Child. 2001, 85, 234–235. [Google Scholar] [CrossRef]
- Tai, E.; Min, A.; Rajan, D.K. A Single-Center Experience with Percutaneous Interventional Management of Refractory Chylous Ascites. Can. Assoc. Radiol. J. J. L’association Can. Des Radiol. 2021, 72, 871–875. [Google Scholar] [CrossRef] [PubMed]
- Yamao, T.; Shimada, Y.; Shirao, K.; Ohtsu, A.; Ikeda, N.; Hyodo, I.; Saito, H.; Iwase, H.; Tsuji, Y.; Tamura, T.; et al. Phase II study of sequential methotrexate and 5-fluorouracil chemotherapy against peritoneally disseminated gastric cancer with malignant ascites: A report from the Gastrointestinal Oncology Study Group of the Japan Clinical Oncology Group, JCOG 9603 Trial. Jpn. J. Clin. Oncol. 2004, 34, 316–322. [Google Scholar] [CrossRef] [PubMed][Green Version]



{kind=link}
{kind=link}
| Outpatient | Hospitalization | |||
|---|---|---|---|---|
| Day 5 | Day 15 | Day 29 | ||
| Glucose (mg/dL) | 133 | 147 | 150 | 152 |
| Total protein (g/dL) | 2.1 | 1.8 | 2.2 | 2.7 |
| LDH (U/L) | 92 | 82 | 95 | 99 |
| Amylase (IU/L) | 18 | 21 | 22 | 27 |
| CEA (ng/nL) | 3.9 | 4.5 | 5.4 | 4.3 |
| Total bilirubin (mg/dL) | 0.2 | 0.2 | 0.3 | 0.2 |
| Triglyceride (mg/dL) | 222 | 181 | 57 | 35 |
| Cytology | Class V |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imai, H.; Saijo, K.; Takenaga, N.; Komine, K.; Ouchi, K.; Kasahara, Y.; Ishikawa, S.; Sasaki, K.; Yoshida, Y.; Shirota, H.; et al. Chylous Ascites Associated with Advanced Pancreatic Cancer That Improved with Appropriate Treatment: A Case Report. Curr. Oncol. 2024, 31, 1477-1482. https://doi.org/10.3390/curroncol31030112
Imai H, Saijo K, Takenaga N, Komine K, Ouchi K, Kasahara Y, Ishikawa S, Sasaki K, Yoshida Y, Shirota H, et al. Chylous Ascites Associated with Advanced Pancreatic Cancer That Improved with Appropriate Treatment: A Case Report. Current Oncology. 2024; 31(3):1477-1482. https://doi.org/10.3390/curroncol31030112
Chicago/Turabian StyleImai, Hiroo, Ken Saijo, Noriko Takenaga, Keigo Komine, Kota Ouchi, Yuki Kasahara, Shiori Ishikawa, Keiju Sasaki, Yuya Yoshida, Hidekazu Shirota, and et al. 2024. "Chylous Ascites Associated with Advanced Pancreatic Cancer That Improved with Appropriate Treatment: A Case Report" Current Oncology 31, no. 3: 1477-1482. https://doi.org/10.3390/curroncol31030112
APA StyleImai, H., Saijo, K., Takenaga, N., Komine, K., Ouchi, K., Kasahara, Y., Ishikawa, S., Sasaki, K., Yoshida, Y., Shirota, H., Takahashi, M., & Ishioka, C. (2024). Chylous Ascites Associated with Advanced Pancreatic Cancer That Improved with Appropriate Treatment: A Case Report. Current Oncology, 31(3), 1477-1482. https://doi.org/10.3390/curroncol31030112